Past Adoption Experiences
National Research Study on the Service Response to Past Adoption Practices
You are in an archived section of the AIFS website
August 2012
Download Research report
Overview
This report presents the findings of the National Research Study on the Service Response to Past Adoption Practices.
The aim of the study was to strengthen the evidence available to governments to address the current service needs of individuals affected by past adoption practices, including the need for information, counselling and reunion services.
In particular, the study has targeted a wide group of those affected by past practices, including mothers, fathers, adoptees, adoptive parents (and wider family members); and professionals currently working with affected individuals.
Findings from the Senate Inquiry into the Commonwealth Contribution to Former Forced Adoption Policies and Practices were also taken into account.
Key messages
-
The key needs identified by the study included: acknowledgement, recognition and increased community awareness of and education about past adoption practices and their subsequent effects;
-
specialised workforce training and development for health and welfare professionals to appropriately respond to the needs of those affected;
-
review of the current search and contact service systems, with a commitment to develop improved service models;
-
improved access to information through the joining of state and territory databases, governed by a single statutory body
Executive summary
The practices in Australia around the permanent transfer of parental legal rights and responsibilities from a child's birth parent(s) to adoptive parent(s) have varied over time. The Australian Senate noted in their report on the Commonwealth Contribution to Former Forced Adoption Policies and Practices (Senate Community Affairs References Committee, 2012; "the Senate Inquiry") that "adoption as it is now understood is a peculiarly twentieth century phenomenon" (p. 3).
Not only have adoption practices in Australia undergone considerable change, so too have society's responses to pregnancies outside of marriage and single motherhood. Until a range of social, legal and economic changes in the 1970s, unwed (single) women who were pregnant were encouraged - or forced - to "give up" their babies for adoption. The shame and silence that surrounded pregnancy out of wedlock meant that these women were seen as "unfit" mothers. The practices at the time, called "closed adoption", were seen as the solution. "Closed adoption" was where an adopted child's original birth certificate was sealed forever and an amended birth certificate issued that established the child's new identity and relationship with their adoptive family.
Given the prevalence of adoption in Australia in the second half of the twentieth century - particularly in the 1960s and early 1970s - a significant proportion of the population has had some experience of or exposure to issues relating to adoption.
The rationale for conducting the current study - the National Research Study on the Service Response to Past Adoption Practices - is to improve the adequacy of the evidence base for understanding the issues and the needs of those affected.
Despite there being a wealth of primary material, there has been little systematic research on the experience of past adoption practices in Australia. The focus has also been on mothers' experiences of "forced adoption" and the experiences of adoptees, with less focus on fathers, adoptive parents and other family members.
The Department of Families, Housing Community Services and Indigenous Affairs (FaHCSIA) commissioned the Australian Institute of Family Studies (AIFS) to undertake the current study on behalf of the Community and Disability Services Ministers' Conference (CDSMC). It complements the Senate Community Affairs References Committee (2012) inquiry into the Commonwealth Contribution to Former Forced Adoption Policies and Practices. The Senate committee was charged with inquiring into the role, if any, of the Commonwealth Government in forced adoption practices, and its potential role in developing a national framework to address the consequences for mothers, their families and children who were subjected to forced adoption policies. Although our study includes participants with experiences of forced adoption, it includes perspectives from all people potentially affected by past adoption practices (adopted persons, mothers, fathers, adoptive parents, other family members) and service providers, and relates to the full range of adoption circumstances, not just experiences of force/coercion.
Although the Senate Inquiry's terms of reference were focused on the experience of forced adoption and the role of the Commonwealth in these practices, the report of the Senate Inquiry (2012) also provided a number of insights into the experience of trauma, and how those affected can best be served. The report highlighted the "ongoing nature of the trauma caused by forced adoption, and the consequent need for counselling" (p. 219). Due to the complexity of grief, a consistent theme was the need for specific counselling services by well-trained and experienced professionals. In particular, the Senate Inquiry acknowledged that it was "not aware of any research comparing the effectiveness of trauma counselling by trained professionals and the support provided by members of peer support groups" (p. 232). One of the strengths of the current study is its systematic examination of the kinds of support and professional services received by affected individuals, and the identification of those that were seen as being the most helpful.
Aim
The key focus of the study is to improve knowledge about the extent and effects of past adoption practices, and to strengthen the evidence available to governments to address the current needs of individuals affected by past adoption practices, including information, counselling, search and contact services, and other supports.
The main objectives for this study are to:
- examine experiences of past adoption practices as they relate to the current support and service needs of affected individuals;
- consider the extent to which affected individuals have sought support and services, and the types of support and services that have been sought;
- produce best estimates of the number of mothers and children currently living in Australia who were affected by past adoption practices; and
- analyse the findings and present information from the study that could be used in the development of appropriate service responses, including best practice models or practice guidelines for the delivery of supports and services for individuals affected by past adoption practices (such as "what works" to assist with the reunion process).
Method
The methodology of the study was to conduct a series of large-scale quantitative surveys and in-depth qualitative interviews with those affected by closed adoption in Australia, as well as to engage with representative bodies, service providers and relevant professionals, including psychologists, counsellors and social workers.
The study has targeted a wide group of those with past adoption experiences, including: mothers and fathers separated from a child by adoption, children who were adopted, adoptive parents, wider family members (to look at the "ripple effects"), and those servicing their current needs (counsellors, psychiatrists, psychotherapists, psychologists and other professionals).
It has incorporated a mixed-methods approach comprising online surveys and reply-paid hard copy surveys, followed by in-depth interviews and focus groups with a sub-component of the survey respondents. Results were integrated across the two data collection methods, and build on existing research and evidence about the extent and effects of past adoption experiences.
Participants
Survey respondents (n = 1,528) comprised:a
- 823 adopted individuals;
- 505 mothers;
- 94 adoptive parents;
- 94 other family members; and
- 12 fathers.
In addition, we surveyed 58 service providers about their views on the current needs and service provision models for those affected by past adoption practices.
Follow-up individual interviews and focus groups included over 300 participants, in 19 locations, across all states and territories.
Key findings
Most participants in this study were adamant about the need to provide as much information as possible about their past experiences in order for us to adequately understand their current service and support needs. This is reflected in our decision to present the findings using a narrative approach to describe the journeys undertaken by participants, thereby providing appropriate context and meaning to the study's conclusions.
Mothers
The experiences of the mothers who participated in this study would suggest that the long-term effects of past adoption practices cannot be understated. Mothers described a range of areas where practices relating to their experience of adoption continue to affect them now, including:
- the birth process;
- differential treatment from married mothers;
- experiences of abuse or negligence by hospital and/or maternity home staff;
- administration of drugs that impaired their capacity;
- lack of the ability to give or revoke consent;
- not being listened to about their preferences; and
- being made to feel unworthy or incapable of parenting, particularly from authority figures.
These experiences have left many feeling they were the victims of a systematic approach to recruiting "undeserving mothers" for the service of deserving married couples. There were very few birth mothers in the study who felt that the adoption was their choice.
The most commonly identified contributing factors to their child's ultimate adoption were family pressure and/or lack of family support, and mothers often talked about emotions such as grief, loss, shame and secrecy surrounding their experiences.
Mental health and wellbeing measures used in the survey indicate a higher than average likelihood of these mothers suffering from a mental health disorder compared to the general population, with close to one-third of the mothers showing a likelihood of having a severe mental disorder at the time of survey completion.b Mothers rated lower quality of life satisfaction than the Australian norm, and over half had symptoms that indicate the likelihood of having post-traumatic stress disorder. These findings have significant implications for the workforce development requirements of those likely to be in contact with mothers affected by past adoptions, including primary health providers and those working in the mental health field, such as psychologists, psychiatrists and psychotherapists.
Around one-quarter of the mothers said that they had not had any supports to help them deal with the separation from their child, or with the process of search and contact. Mothers identified that the most common form of support they had received in relation to their experiences was from their friends; however, support from professionals/services was also commonly received by mothers, from psychologists or psychiatrists, support groups, social workers or counsellors, and registered search/support organisations. These supports were most commonly viewed as being helpful.
Mothers commonly identified the effective and enabling characteristics of such services as being:
- accessibility;
- affordability;
- flexibility in the modality of services provided;
- sensitivity to the particular needs of mothers separated from children by adoption; and
- staffing by trained professionals with an in-depth understanding and level of experience in trauma and other related issues commonly experienced by the mothers.
The majority of mothers (85%) had had some form of contact with their son/daughter from whom they were separated, and almost two-thirds of these respondents indicated that they had been able to establish an ongoing relationship. For some, their needs had been met simply through the connection with their son/daughter. Qualitative accounts, however, emphasised the difficulties associated with the establishment of new relationships and the need for ongoing assistance for both themselves and their son/daughter to more effectively manage this evolving and complex connection.
Mothers consistently identified six key areas that reflect their current service and support needs:
- validation of their experiences - that what happened to them happened;
- acknowledgement of their experiences through broader community and professional education and awareness;
- restitution through acknowledgement of the truth;
- access to information;
- access to services both for mental and physical health, and for search and contact; and
- a "never again" approach so that society will learn from its mistakes from past practices around closed adoption in Australia.
These themes are consistent with the findings of the Senate Inquiry.
Persons who were adopted
As the largest proportion of participants in this study, the views and experiences of persons who were adopted have provided some key understandings as to their current service and support needs. The findings indicate that the complexities of the issues identified by this respondent group require careful consideration within the context of the service and support options that are currently available. The longer term effects of adoption (both positive and negative) are significant for many adoptees in this study, reflected no more clearly than through their levels of participation in the research.
One of the most significant findings within this respondent group appears to be that, regardless of whether they had a positive or more challenging experience growing up within their adoptive family (roughly equal proportions of each participated in this study), most participants identified issues relating to problems with attachment, identity, abandonment and the parenting of their own children.
Compared to Australian population estimates, adoptees responding to our survey had lower levels of wellbeing and higher levels of psychological distress, and almost 70% of adoptee survey respondents agreed that being adopted had resulted in some level of negative effect on their health, behaviours or wellbeing while growing up. These negative effects included:
- hurt from secrecy and lies surrounding their adoption and subsequent sense of betrayal;
- identity problems;
- feelings of abandonment;
- feeling obligated to show gratitude throughout their lives;
- low levels of self-worth; and
- difficulties in forming attachments to others.
Some of these issues became more poignant when the adoptee had his/her own children, which in itself is an area for consideration in relation to the focus of current support needs.
For those study participants who were subjected to abuse and neglect by their adoptive families, the mental and physical health issues that result from such traumas may require urgent access to intensive, specialised and ongoing supportive interventions.
Seeking information about themselves and family members from whom they were separated was a strong feature in this study for adopted individuals, particularly as this process relates to the formation of identity. Over 60% of participants had had some form of contact with their mother, and 45% of those participants described a relationship that was ongoing; however, only around one-quarter of participants had had contact with their father (around half of whom said they had an ongoing relationship).
Barriers to finding information about families of origin included:
- navigation of complex systems that hold identifying information, particularly for those living in a different state to where they were born;
- costs associated with accessing information;
- inconsistent and sometimes unreliable information provided by departments/institutions;
- feelings of divided loyalties and subsequent guilt for initiating the search process; and
- contact and information vetoes having been placed by birth parents.
Further complexities arise for those who do not discover that they are adopted until late in their lives, as well as for those whose adoptions were not formalised (such as a private arrangement where the child was placed with another family without any legal processes). These individuals are often faced with having absolutely no information about themselves and where they have come from. Late-discovery adoptees may experience significant emotional damage as they find themselves contemplating a life that has been based on lies and deception, no matter how well-intentioned their adoptive families may have been in keeping the adoption secret.
Service utilisation was common among adoptees in the study; in most instances they used psychologists or psychiatrists, adoption support services, or social workers or counsellors. Emotional support was the most frequently sought type of support by adoptees, and more than half of those who had utilised such services had found them to be helpful.
Key service needs identified by adoptees who participated in our study related to the provision of:
- free access to information - original birth certificates and medical/genetic histories (irrespective of contact and information veto status in this instance);
- search and information policies, processes and systems that are uniform across states/territories, preferably managed through a national, centralised system;
- acknowledgement and recognition of the effects of adoption as the living examples of past policies and practices;
- public awareness and education about the effects of adoption, including among broader health and welfare professionals;
- support (and financial assistance) for search and contact, such as Find and Connect services; and
- ongoing counselling and wellbeing support, which recognises that the effects of adoption can be lifelong and may be triggered at any time.
Adopted persons in the study identified the characteristics of services (including those offering search and contact as well as psychological/emotional support) that would enhance their utilisation as being:
- accessibility;
- affordability;
- ease of navigation;
- provision of ongoing (including follow-up) services;
- offering a variety of options to suit differing needs (such as a range of peer support groups and more intensive one-to-one support interventions);
- staffing by professionals with specific training and experience in working with those affected by adoption; and
- availability of mediators/case managers to facilitate the process of search, potential contact and the subsequent outcomes.
Fathers
The limited level of participation by fathers separated from a child by adoption (n = 12) in the current study is in itself, an indication of the need for further and more targeted research with this respondent group. As a particularly hard-to-reach population, specific and assisted recruitment strategies are necessary to further our knowledge and understanding of the broader effects of past adoption practices on fathers, particularly given that the research conducted to date indicates that this group already feels as though they are rarely considered in the broader discourse associated with past adoption practices in Australia (see Coles, 2009; Passmore & Coles, 2008).
Fathers who did participate in the research, however, provided substantial insight into their experiences, which are perhaps reflective of what many other fathers would have also experienced. Unfortunately, such a small number of respondents in this study does not allow us to generalise any of the findings.
These study participants told us that they were never asked or had no rights or say in the decision for their son/daughter to be adopted. However, they said that they had wanted to have a say in what happened with regard to adoption, and many wanted to keep the baby. Very few of them had support at the time of the pregnancy and birth, and very few have had support since.
Most of these fathers had actively sought contact with their child (n = 9), and 10 had had contact (one father was contacted by their child). Of these, most had an ongoing relationship with their son/daughter, which in general appears to have had a positive effect on both themselves and their families.
An interesting and important finding within this sample is that one-third were likely to have a mental health issue, and almost all of them showed some symptoms of post-traumatic stress. This is an area that requires further investigation to establish the ongoing mental health needs of fathers separated from a child by adoption.
Fathers in this study identified their current needs as being centred on:
- having increased information and understanding within the broader community of what happened and why; that is, past adoption practices and fathers' ultimate lack of inclusion/control over any decision-making processes relating to the adoption of their child; and
- the availability of specialised support for all people who have been damaged by what has happened and, specifically, services that are targeted at identifying and encouraging utilisation by fathers who are as yet to speak of their experiences and associated impacts.
Adoptive parents
Many of the comments from the adoptive parents in the study reflect the broader society's attitudes towards adoption in the 1960s and 1970s, which "encouraged" adoption as a way of addressing infertility (Higgins, 2010). Many stated that they were giving a loving home to a child who would have otherwise been left to institutional care, that the adoption of their son or daughter addressed their need and the need of the mother to have someone take her child. In contrast to the mother's experience of the adoption, most adoptive parents were completely satisfied with the adoption process at the time.
Service utilisation was low within this sample, with many more likely to rely upon the support of their spouses and friends for any issues relating to their adoption experience. Mental health and wellbeing measures used in the study show that the adoptive parents who participated are faring well compared to other respondent groups (particularly adoptees and mothers), and these results are within general population norms. However, many of the adopted individuals (and some mothers) who participated in the study indicated that support for the adoptive parents was in fact a current area of need. The areas of support adoptees suggested ranged from acknowledging the grief suffered by adoptive parents as a consequence of their infertility, to developing better strategies for managing the complexities of their child's contact with the families of origin.
Adoptive parents had mixed views about their sons/daughters attempting to make contact with birth parents. The issue of divided loyalties, as it relates to the adoptees' search and contact process, in many ways contrasted with the views held by the adoptive parents. Some adoptive parents felt that their son/daughter's contact with birth family members had contributed to the demise of their relationship with their child, whereas others felt that it had enriched their lives through the expansion of their family unit.
There were few current service needs identified by the adoptive parents in this study. They did not consistently identify needs for themselves, but rather were focused on search and contact services for their sons/daughters, as well as assistance for them in finding out information, such as medical histories.
Other family members
The ripple effects through families are indeed evident from the information provided by the study respondents. A diverse range of relatives completed the survey for those affected by the adoption experiences of a relative (including siblings of the persons adopted, spouses of mothers, and subsequent children of mothers). There was also a range of experiences with the search, contact and reunion with their relative and the family of origin, some of which resulted in a positive effect on relationships, while others were negative.
Although the majority of the relatives had support, most believed that there needs to be facilitated access to support (counselling and therapy) for themselves and their relatives regarding the issues arising from adoption. Other needs include assistance with contact/reconciliation with the "lost" relative, a provision of the facts regarding the adoption, and improved access to information about the family of origin (such as medical histories).
In general, other family members had been adversely affected by the adoption experience (although a few did express positive experiences). Most talked about the ways in which they would benefit from access to support to deal with issues arising from past adoption experiences, including obtaining information, making contact, having peer support, and expanding community awareness, understanding and contrition.
Service providers
The feedback from the service providers corroborated what mothers and adoptees told us about their experiences of accessing services. The predominant issue was that there were not enough services, and when they were available, the professionals were often not knowledgeable about adoption-specific issues. Furthermore, many clients were not aware of the services available, and those who were aware often found that the cost of the services made long-term involvement prohibitive.
The strongest message from the service providers was the need for support for counselling - financial support to assist people affected by past adoption experiences to afford counselling, as well as training support to assist in the development and cost of training counsellors in adoption-specific issues. One respondent suggested implementing a model similar to Find and Connect, which is a service developed to address the needs of people who have been in out-of-home care as children, whether as Forgotten Australiansc or child migrants,d and which has a special search unit for difficult cases.
Respondents supported the development of a system-wide network that can connect clients with services, and support services with other related services. Furthermore, search and reunion organisations advocated for a better relationship with government agencies to assist in the sharing of information.
Strengths and limitations of this study
A significant limitation of the study is that the data were collected from a self-selected sample as there is no identified database or other sampling frame from which to randomly invite people to participate. Therefore, we cannot say with confidence that our findings are representative of all people who have experienced closed adoption in Australia, particularly for the findings about fathers, given the very small numbers (n = 12) who participated in the study.
One of the original aims of the study was to attempt to produce the best possible estimates of the number of parents, adoptees and adoptive parents/family currently living in Australia who are affected by past adoption practices. However, the self-selected sample of study participants and lack of available sources from which to extract such information has prevented us from producing a reliable estimate. From the information that we do have from the Housing, Income and Labour Dynamics in Australia (HILDA) survey, we can conclude that the number of affected people is a significant proportion of the Australian population (around 200,000).
Nevertheless, there are numerous strengths to the present study that mean the data will be a reliable source of information on the experiences and current needs of Australians affected by past adoption practices - most particularly the large number of respondents (n = 1,528), representing a small, but still significant, proportion of Australians currently alive who are likely to have been affected by closed adoption that took place from the mid- to late 20th century.
Our hope is that the rich detail provided of individuals' journeys through the period of closed adoption in Australia, the issues they now face, and how services and supports could be better targeted, is reflective of the variety of perspectives that were shared with us.
Summary of key conclusions
Key needs and priority actions
Across the various respondent groups, despite the range of views and issues raised, there are some important areas where the majority of participants aligned in identifying the needs and priority actions for responding to the ways in which closed adoption has affected their lives. These included:
- acknowledgement and recognition of past adoption practices (including the role of apologies and financial resources to address current service and support needs);
- raising community awareness of and education about past adoption practices and their subsequent effects;
- specialised workforce training and development for primary health carers, mental and broader health and welfare professionals to appropriately respond to the needs of those affected;
- review of the current search and contact service systems, with a commitment to develop improved service models;
- improved access to information through the joining of state and territory databases, governed by a single statutory body;
- improved access to and assistance with costs for mental, behavioural and physical health services; and
- ensuring that lessons from past adoption practices are learned from and translated where appropriate into current child welfare policies, and that adoption-specific services are created or enhanced to respond to the consequences of past practices.
Specific service and support options
Direct services and supports
Direct services and supports relate to a continuum of care that recognises the importance of appropriate and targeted responses at all levels of engagement; from the first point of information-seeking, to the lifelong need by some people to "move in and out of" varying levels of support. The service options identified, based on the experiences and expressed needs of participants in this study, include:
- 24-hour access to advice, support, information and referral services;
- availability of peer support groups, featuring a diversity of options for delivery;
- adoption-specific support services (post-adoption support), offering a "one-stop shop" for accessing information, search, contact and ongoing support/referral to appropriate professionals;
- availability of professional one-to-one support/counselling/therapeutic interventions, delivered by psychiatrists, psychologists, psychotherapists and other professionals who have had specialised training or experience in adoption-related issues, such as trauma, relational interactions, attachment and abandonment;
- priority access to medical, psychiatric and psychological services to address the physical and psychological health consequences of their adoption experience;
- availability of professionals to support other family members; and
- availability of primary and allied health services professionals who are trained to understand the potential effects of adoption on their service users as it relates to accurate and appropriate diagnosis and referral to appropriate support interventions.
Information and resources
Information and resources identified by study respondents that would help facilitate broader public and professional awareness include:
- publications that explain the history of adoption, the common reasons for adoption and the common emotional outcomes;
- a series of short, easy-to-read and well-presented fact sheets on key aspects of the issue (such as the mothers' experiences, the adopted persons' experiences, the adoptive parents experiences, other family members' experiences, how to find information about your birth family, and so on);
- information resources for wider family members, with advice on how to best support their loved one who is affected by adoption;
- a booklet that contains stories of people affected by past adoptions - in their own words - that gives insight into a variety of experiences, and that could be distributed widely in doctors' waiting rooms and the like; and
- a comprehensive website about adoption.
Key features of good practice
Our study suggests that "good practice" should involve implementing improvements to service provision through information delivery, search and contact services, and other professional and informal counselling and supports.
- Good information services (including identifying information and access to personal records):
- are delivered by trained staff;
- are provided through websites, moderated interactive sites ("chat rooms") and/or 24-hour phone lines;
- are provided with sensitivity to the needs of those seeking it (confidentiality, discretion, language used, etc.);
- are relevant to the "stage of the journey" of individuals; and
- have a range of support levels (e.g., access to support person onsite and in follow-up).
- Good search and contact services:
- enable access to counselling and ongoing support during the search and contact journey;
- use an independent mediator to facilitate searching for information and exchanging information; and
- address expectations before contact is made and provide ongoing support afterwards.
- Good professional and informal supports:
- incorporate adoption-related supports into existing services (such as services funded by the Australian Government's Family Support Program, Medicare-funded psychological services or other state/territory-funded programs);
- provide options for both professional and peer supports; and
- address trauma, loss, grief and identity issues.
a Terminology used to describe study participants is discussed in detail in Chapter 2. For the purposes of this report, the terms "mother" and "father" refer to the biological parents except where clarity is needed to distinguish between both sets of parents. In this instance, the terms "birth" and "adoptive" parents are used; however, we acknowledge the sensitivities relating to the use of this language.
b As with all cross-sectional research, our methods do not allow us to determine whether these higher rates of mental health problems can be attributed to their adoption experience, or to other factors.
c Forgotten Australians are adults who spent a period of their childhood or youth in children's homes, orphanages and other forms of out-of-home care, up to 1989. At least 500,000 children grew up or spent long periods in this institutional care system in the 20th century, which was the standard form of out-of-home care in Australia at the time.
d Former child migrants are adults who were sent to Australia as children as part of inter-governmental child migration schemes in the period following World War II (up to the 1970s), and who were subsequently placed in homes, orphanages and other forms of out-of-home care. It is estimated that around 7,000 children were sent to Australia from the United Kingdom and Malta under these schemes, of which about 6,700 were from the United Kingdom.
1. Introduction
"Adoption" is a word that elicits mixed responses from people. The definition of adoption that was relied upon by the Australian Senate's report on the Commonwealth Contribution to Former Forced Adoption Policies and Practices (Senate Community Affairs References Committee, 2012; "the Senate Inquiry"; see pp. 5-6) was that of the New South Wales Law Reform Commission (1993), and is also the definition used in this report:
Adoption is a legal process by which a person becomes, in law, a child of the adopting parents and ceases to be a child of the birth parents. All the legal consequences of parenthood are transferred from the birth parents to the adoptive parents. The adopted child obtains a new birth certificate showing the adopters as the parents, and acquires rights of support and rights of inheritance from the adopting parents. The adopting parents acquire rights to guardianship and custody of the child. Normally the child takes the adopters' surname. The birth parents cease to have any legal obligations towards the child and lose their rights to custody and guardianship. Inheritance rights between the child and the birth parents also disappear. (para. 2.1)
The practices in Australia around the permanent transfer of parental legal rights and responsibilities from a child's birth parent(s) to adoptive parent(s) have varied over time. The Senate Inquiry (2012) noted in their report that "adoption as it is now understood is a peculiarly twentieth century phenomenon" (p. 3).
Not only have adoption practices in Australia undergone considerable change, so too have society's responses to pregnancies outside of marriage and single motherhood. Until a range of social, legal and economic changes in the 1970s, unwed (single) women who were pregnant were expected to "give up" their babies for adoption. The shame and silence that surrounded pregnancy out of wedlock meant that these women were seen as "unfit" mothers. The practices at the time, called "closed adoption", were seen as the solution. "Closed adoption" was where an adopted child's original birth certificate was sealed forever and an amended birth certificate was issued that established the child's new identity and relationship with their adoptive family.1 Mothers were not informed about the adoptive families, and the very fact of their adoption was usually kept secret from the children (see Swain & Howe, 1995); though changes in legislation now allow access to information if no veto from the other party was put in place.
Given the prevalence of adoption in Australia in the second half of the twentieth century - particularly in the 1960s and early 1970s - a significant proportion of the population has had some experience of or exposure to issues relating to adoption. Therefore, it is important to have an adequate evidence base for understanding the issues, and the needs of those affected. However, understanding the true extent of past practices, or its ongoing effects, is problematic. There are no accurate data on the number of Australians who have been affected (Higgins, 2010, 2011a) and there is a wide range of people who may be affected by past adoption practices, including:
- mothers;
- adopted individuals;
- fathers;
- the mothers' and fathers' families;
- subsequent partners of the mothers and fathers;
- subsequent partners and children of adopted individuals;
- siblings;
- adoptive families;2 and
- professionals, such as nursing staff and social workers, involved in the practices of the time.
The range of people involved therefore suggests the potential for wide-ranging impacts, including the possibility of the effects of past adoption practices on these individuals in turn "rippling" through to others, including other children and family members. Furthermore, the effect of past adoption practices affects the next generation - the children of adopted persons. Commentators, professional experts, researchers and parliamentary committees have all accepted that past adoption practices were problematic, had the potential to do damage, and often did.
In its report, the Senate Inquiry noted an earlier review of the available literature regarding past adoption practices that was conducted by the Australian Institute of Family Studies (AIFS; Higgins, 2010). In that report, the conclusion about the state of the evidence base was that:
There is a wealth of material on the topic of past adoption practices, including individual historical records, analyses of historical practices, case studies, expert opinions, parliamentary inquiries, unpublished reports (e.g., university theses), as well as published empirical research studies. They include analyses of both quantitative and qualitative data, gathered through methods such as surveys or interviews.
Despite this breadth of material, there is little reliable empirical research. To have an evidence base on which to build a policy response, research is needed that is representative, and systematically analyses and draws out common themes, or makes relevant comparisons with other groups (e.g., unwed mothers who did not relinquish babies, or married mothers who gave birth at the same time, etc.). (p. 3)
Despite there being a wealth of primary material, there has been little systematic research on the experience of past adoption practices in Australia. The focus has also been on mothers' experiences of forced adoption, with less focus on fathers (where they are aware that they were responsible for a pregnancy, and that the child was adopted), adoptees, adoptive parents, and other family members.
Although Higgins (2010) concluded that there was not a reliable evidence base for understanding the extent of past practices, the number of Australians who were affected, or its long-term effects, key issues evident from the available information included:
- the wide range of people involved, and therefore the wide-ranging impacts and "ripple effects" of adoption beyond mothers and the children who were adopted;
- the role not only of grief and loss, but the usefulness of understanding past adoption practices as "trauma", and seeing the effects through a "trauma lens";
- the ways in which past adoption practices drew together society's responses to illegitimacy, infertility and impoverishment;
- anecdotal evidence of the variability in adoption practices;
- the role of choice and coercion, secrecy and silence, blame and responsibility, the views of broader society, and the attitudes and specific behaviours of organisations and individuals;
- the ongoing effects of past adoption practices, including the process of reunion between mothers and their now adult children, and the degree to which it is seen as a "success" or not; and
- the need for information, counselling and support for those affected by past adoption practices (for a detailed review of the available literature in Australia on the effects of closed adoption, see Higgins, 2010).
As past adoption practices cannot be "undone", one of the steps in the journey for parents and their now adult children separated by adoption is the choice around making contact and potentially being reunited. The existing literature in Australia on this process is mostly from case studies and (auto)biographies, showing a significant variety of pathways and responses. Given this variability of experiences and outcomes, and the absence of any systematic empirical evidence, this is an area where further research would be of particular value. Services attempting to support those affected - including professional counsellors, agencies and support groups - would all benefit from a greater understanding of typical pathways through the contact and reunion process, estimates of the number of reunions that have occurred, the perspectives of those involved, and factors that are associated with positive and negative reunion experiences.
Apart from these issues relating to information, contact and/or reunion, there are other ongoing issues for those affected by past adoption practices, including their sense of self, relationships with others, and experience of mental health problems such as anxiety and depression (Higgins, 2010, 2011a, 2011b).
Although there is a significant body of literature on the experiences of adoptees, little attention has been paid to the specific experiences of adoptees whose parent(s) experienced force or coercion during the adoption. Likewise, there has been little research that separates out experiences from the period of closed adoption from the more recent open adoption paradigm now operating in Australia (see section 2.2).
The current feelings and experiences of adoptive parents from the period of closed adoption have also not been a focus of the empirical literature. For example, there was no focus in the Senate Inquiry (2012) report on adoptive parents, or ways in which adoptive parents think and feel in response to societal shifts in attitudes and support for single parents, and changes in adoptive practices.3
Similarly, the voice of service providers has not been heard, nor their perspectives on the current needs of those affected by past experiences and their professional opinions about what works best in delivering effective services to clients.
1.1 Objectives of this study
On 4 June 2010, the Community and Disability Services Ministers' Conference (CDSMC)4 announced that Ministers had agreed to a joint national research study into "closed adoption" and its effects, to be conducted by the Australian Institute of Family Studies.
The aim of the current study, commissioned by the Department of Families, Housing Community Services and Indigenous Affairs (FaHCSIA) on behalf of CDSMC - the National Research Study on the Service Response to Past Adoption Practices - is to utilise and build on existing research and evidence about the extent and effects of past adoption practices in order to strengthen the evidence available to governments for addressing the current needs of individuals affected by past adoption practices.
The key focus of the study is on current needs for services and supports, and it was designed to produce evidence that can assist with improving service responses to those affected by past practices - including information, counselling, search and contact services and other supports.
In conducting the National Research Study on the Service Response to Past Adoption Practices, AIFS engaged with persons directly affected by past adoption practices, as well as with representative bodies, service providers and relevant professionals.
The main objectives for this study are to:
- examine experiences of past adoption practices as they relate to the current support and service needs of affected individuals;
- consider the extent to which affected individuals have sought support and services, and the types of support and services that have been sought;
- produce best estimates of the number of mothers and children currently living in Australia who were affected by past adoption practices; and
- analyse the findings and present information from the study that could be used in the development of appropriate service responses, including best practice models or practice guidelines for the delivery of supports and services for individuals affected by past adoption practices (such as "what works" to assist with the reunion process).
Our research incorporated a mixed-methods approach comprising online surveys and reply-paid hard-copy surveys, followed by in-depth interviews and focus groups. The results were integrated from across the different elements of the study, utilising and building on existing research and evidence about the extent and effects of past adoption experiences.
The study targeted a wide group of those with past adoption experiences, including: mothers and fathers separated from a child by adoption, individuals who were adopted, adoptive parents, wider family members (to look at "ripple effects"), and those servicing their current needs (counsellors, psychologists and other professionals).
To assist with recruitment, we developed and implemented a recruitment strategy and communications plan, including a study web page with information about the study and through which the online survey was accessed.
This study complements the Senate Inquiry into the role of the Commonwealth in former forced adoptions. The Senate Community Affairs References Committee was charged with examining the role, if any, of the Commonwealth Government in forced adoption practices, and its potential role in developing a national framework to address the consequences for mothers, families and children who were subjected to forced adoption policies. It also complements the work of the History of Adoption Project at Monash University, which is focused on "explaining the historical factors driving the changing place, meaning and significance of adoption", particularly through its collection of oral histories.5
In this report, we:
- analyse information on the long-term effects of past adoption practices as they relate to current support and service needs of affected individuals, including the need for information, counselling and search and contact services;
- examine the extent to which affected individuals have previously sought support and services, and the types of services and support that were sought; and
- analyse the findings and present information from the study that could be used in the development of best-practice models or practice guidelines for the delivery of supports and services for individuals affected by past adoption practices.
1.2 Process
The study commenced with the development of a communications strategy, including the creation of a website and online method for registering interest in participating in the survey. We convened a technical advisory group, and led consultations with stakeholder advisory groups convened by FaHCSIA.
Through the technical advisory group of 10 people - comprising academic experts, representatives from key family support agencies, and representatives of FaHCSIA and the Community and Disability Services Ministers' Advisory Council (CDSMAC) (see Attachment A1 for details) - the Institute ensured that the research was of the highest possible standard for testing the conclusions about the nature of support needed for those affected by past adoption practices. The technical advisory group also provided feedback on this report. The terms of reference for this group are included in Attachment A2.
The value of obtaining input from stakeholder advisory groups representing those affected by past adoption experiences cannot be understated. Our engagement involved consultation with representatives from support groups for mothers, individual mothers, fathers, adopted individuals and adoptive family representatives. One part of this process included conducting two stakeholder advisory group teleconferences, with predominantly mothers separated from children by adoption. Further contact and input was also received from individuals both from these groups and from the wider affected community. The main purpose of this contact was to provide feedback on the proposed content areas for the surveys and assist with recruitment of people into the surveys.
Based on feedback from the technical and stakeholder advisory groups, we refined the content of the online surveys. Approval from the AIFS Human Research Ethics Committee was obtained on 8 July 2011 for both the quantitative and qualitative data collection components for this study.
With input from the technical and stakeholder advisory groups, we developed a list of agencies/individuals to be targeted by the various strategies and implemented an ongoing communication strategy to publicise the study and maximise response rates (see section 3.4 for more detail).
1.3 Terminology
A range of different terms is used in the literature to refer to both adoption practices and those affected by them. In relation to mothers, these include:
- relinquishing mothers;
- parents who relinquished a child to adoption;
- birth mothers;
- biological mothers;
- natural mothers;
- genetic parents;
- adoption of ex-nuptial children;
- mothers affected by past adoption practices;
- mothers of the stolen white generation (analogous to the Stolen Generations of Aboriginal children removed from their parents, which occurred at roughly the same time period) (Cole, 2008);
- real parents (Grafen & Lawson, 1996).
In terms of the process, many affected individuals reject the term "adoption", as their personal experience was one of force, coercion or other illegal behaviour. Terms such as "relinquishment", while occurring often in the early literature, connote a sense of agency and choice that many deny having. Some other terms that have been used in the literature include:
- losing a child to adoption (McGuire, 1998);
- reunited mother of child/ren lost to adoption (Farrar, 1998);
- separation from babies by adoption (Lindsay, 1998); and
- rapid adoption (the practice of telling a single mother her baby was stillborn, and the baby being adopted by a married couple).
It is acknowledged that some of the terms are perceived as being "value-laden", either because of their acceptance of a particular point of view (e.g., "stolen" implies illegal practices), or because their attempt at neutrality (e.g., "relinquishing mothers") potentially hides what are alleged as immoral or illegal practices. For the purposes of the current document, where possible, the terms used by the respondents are used to describe their experiences.
Similarly, there are some sensitivities around the terms used to describe the child who was adopted. These people adopted during the period of closed adoption in Australia are now well into adulthood and are themselves often parents or sometimes even grandparents. Referring to them as "children" is therefore problematic, and many prefer being called a "son/daughter", or simply an "adoptee".
Another term in the literature that is often used is "reunion", referring to the process of a parent and their adopted son or daughter making contact. However, it is important to distinguish between the process of exchanging details, communicating, or even meeting - and the longer term aim of effecting a "reunion"; therefore, it should be seen as a process from making contact through to possible reunion.
1 According to the Australian Institute of Health and Welfare (AIHW; 2012), all states and territories now have a level of "openness" - or the option of openness - in adoption. This can involve gaining access to information or contact between birth and adoptive families. Parties to an adoption can apply for access to information that is either "identifying" or "non-identifying". In some jurisdictions, open adoption is available on request; in others, it is the standard practice for all adoptions (see AIHW, 2012, pp. 70-72).
2 In section 1.3, the issue of terminology is discussed in detail. For the purposes of this report, we try to reflect the language that participants used, as well as terms that the technical advisory group and stakeholder advisory groups identified as being preferable.
3 There was no mention of adoptive families in the motion that established the Senate Inquiry (2012, see p. 1) and, to the best of our knowledge, there is no direct reference in the report to the experiences of adoptive parents and their current needs.
4 CDSMC has since been renamed as the Council of Australian Governments Standing Council on Community, Housing and Disability Services (SCCHDS).
5 See the History of Adoption Project website at <arts.monash.edu.au/historyofadoption>.
2. Background
This chapter provides a summary of the ways in which adoption currently operates in Australia, past adoption practices, and the potential effects that adoption has on those involved. Some of the key legal and policy milestones regarding adoption and single mothers in Australia are outlined in Box 2.1.
Box 2.1 Legal and policy milestones regarding adoption and single mothers in Australia
- Legislation on adoption commenced in Western Australia in 1896, with similar legislation in other jurisdictions following (but not until the 1920s in most instances).
- Before the introduction of state/territory legislation on adoption, "baby farming"* and infanticide were not uncommon.
- Legislative changes that emerged in the 1950s and consolidated in the 1960s enshrined the concept of adoption secrecy and the ideal of having a "clean break" from the birth mother.
- State/territory councils, and eventually a national Council of the Single Mother and Her Children, were established in the early 1970s, which set out to challenge the stigma of adoption and to support single and relinquishing mothers.
- The Commonwealth Government introduced the Supporting Mother's Benefit in 1973, which contributed to a rapid decline in adoptions after a peak in 1971-72.
- The status of "illegitimacy" disappeared in the early 1970s, starting with a Status of Children Act in both Victoria and Tasmania in 1974 (in which the status was changed to "ex-nuptial").
- Abortion became allowable in most states/territory from the early 1970s (the 1969 Menhennitt judgement in Victoria and 1971 Levine judgement in NSW).
- Further legislative reforms started to overturn the blanket of secrecy surrounding adoption (up until changes in the 1980s, information on birth parents was not made available to adopted children/adults).
- Beginning with NSW (in 1976), registers were established for those wishing to make contact (both for parents and adopted children).
- In 1984, Victoria implemented legislation granting adopted persons over 18 the right to access their birth certificate (subject to mandatory counselling). Similar changes followed in other states (e.g., NSW introduced the Adoption Information Act in 1990).
- By the early 1990s, legislative changes in most states/territories ensured that consent for adoption had to come from both birth mothers and fathers.
- The majority of local adoptions (those of children born or permanently residing in Australia) are now "open".
* "Baby farming" refers to the provision of private board and lodging for babies or young children at commercial rates, a practice that has been criticised for being focused on financial gain, including cases of serious neglect and infanticide; however, it was also part of the system for protecting children who were at risk from infanticide or neglect by their family.
Source: Higgins (2011a)
2.1 Current adoption practices in Australia
There are three types of adoption currently operating in Australia:
- Intercountry adoptions are of children from other countries who are usually unknown to the adoptive parent(s). Since 1999-2000, most adoptions in Australia have been intercountry adoptions. In 2010-11, there were 215, representing 56% of all adoptions.
- Local adoptions are those of children born or permanently residing in Australia, but who generally have had no previous contact or relationship with the adoptive parents. In 2010-11, there were 45 local adoptions, representing 12% of all adoptions.
- "Known" child adoptions are of children born or permanently residing in Australia who have a pre-existing relationship with the adoptive parent(s), such as step-parents, other relatives and carers. In 2010-11, there were 124 "known" child adoptions, representing 32% of all adoptions (AIHW, 2012).
Despite the large growth in the number of Australian children in out-of-home care over the last two decades, adoption of these children is rare. This is because there is a strong push for them to be restored to - or maintain active contact with - their parents. In addition, most state/territory child protection statutory authorities have the capacity to: (a) make permanent care orders (which provide security of placement with a foster/kinship carer); and/or (b) have policies relating to the creation of permanency plans6 when there is no foreseeable likelihood of children being able to safely return to the care of their parents. Unlike adoption, these foster/kinship care arrangements do not formally extend past a child turning 18 years of age and the birth certificate is not altered.
2.2 History of adoption
Adoption rates
The first legislation on adoption in Australia was enacted in Western Australia in 1896, with similar legislation following in other jurisdictions, mostly from the 1920s. In the decades prior to the mid-1970s, it was common in Australia for babies of unwed mothers to be adopted. At its peak in 1971-72, there were almost 10,000 adoptions (see Figure 2.1). Since then, rates of adoption dropped significantly, and over the last two decades have remained relatively stable at around 400-600 children per year (e.g., there were 384 adoptions in 2010-11; AIHW, 2012).
Figure 2.1: Number of adoptions in Australia from 1968-69 to 2010-11
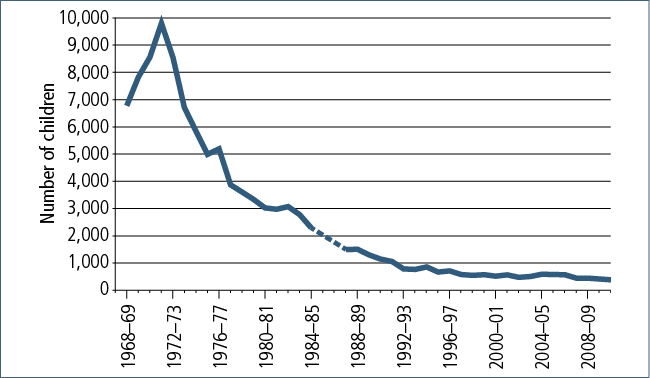
Note: National data were not collected between 1985-86 and 1986-87.
Source: AIHW (2009; 2012)
Similarly, there was a rise in adoptions from the early 1950s, with a peak in 1970-72, and declining rapidly though to the mid-1980s (Figure 2.2).
Figure 2.2: Number of adoptions in Australia from 1951-52 to 1984-85

Note: National data were not collected between 1961-62 and 1968-69
Source: Senate Community Affairs References Committee (2012)
This significant change in adoption rates coincided with a range of legislative, social and economic factors, such as:
- greater social acceptance of raising children outside registered marriage, accompanied by an increasing proportion of children being born outside marriage;7
- increased levels of support being available to lone parents (e.g., the Supporting Mother's Benefit, introduced in 1973) (see Australian Bureau of Statistics [ABS], 1988);
- increased availability and effectiveness of birth control;8 and
- declining birth rates.
Inglis (1984) claimed that more than 250,000 Australian women had "relinquished" a baby for adoption since the late 1920s, but without describing the basis for this calculation. Nonetheless, it is a claim that has been widely cited since.
In any case, what is not known is the proportion of these adoptions that involved force, coercion, or other immoral or illegal behaviours.
Closed adoption
From the mid-20th century, adoption practice in Australia reflected the concept of secrecy and the ideal of having a "clean break" from the birth parents. Closed adoption is where an adopted child's original birth certificate is sealed and an amended birth certificate issued that establishes the child's new identity and relationship with their adoptive family. Legislative changes in the 1960s tightened these secrecy provisions, ensuring that neither party saw each other's names.
The experience of closed adoption included people being subjected to unauthorised separation from their child, which then resulted in what has been called "forced adoption". From the 1940s, adoption advocates saw it as desirable for the child to be separated from the mother as soon as possible, preferably straight after birth.9
From the 1970s, advocacy led to legislative reforms that overturned the secrecy within adoption, such as mothers receiving identifying information. However, it was not until further changes were made in the 1980s (or 1990s in some Australian jurisdictions) that information on (birth) parents was made available to adopted children/adults.
Beginning with NSW in 1976, state/territory-based registers were established for both birth parents and adopted children who wished to make contact. In 1984, Victoria implemented legislation granting adopted persons over the age of 18 the right to access their birth certificate (subject to mandatory counselling). Similar changes followed in other states/territories (e.g., NSW introduced the Adoption Information Act in 1990). Support groups such as Jigsaw, also established their own registers.
Contact/reunion services are now part of the ways in which governments and agencies are trying to address the negative effects of past adoption practices and separation on (birth) parents and children.
Open adoption
The practice of closed adoption changed gradually across each of the states and territories in Australia from the late 1970s through the 1980s and 1990s.
With the implementation of legislative changes, adoption practices shifted away from secrecy. Now, the vast majority (84% in 2010-11) of local adoptions (but not intercountry adoptions) are "open", where the identities of birth parent(s) can be known to adoptees and adoptive families and there are access arrangements. However, the birth certificate is still changed to record the names of the adoptive parents. Among local adoptions, only 16% of birth parents in 2010-11 signed a consent involving no contact or exchange of information with the adoptive family (AIHW, 2012).
Improvements in adoption practices include:
- more accountable processes for obtaining consent from (birth) parents;
- a requirement for consent to be provided by both (birth) parents (or the need for a parent's consent to be dispensed with by a court for a child's adoption to proceed); and
- higher quality assessments and benchmarks for assessing the suitability of prospective adopters.
2.3 Effects of past adoption experiences
There is limited research available in Australia on the issue of adoption practices during and following the period of closed adoption in Australia.
There was a range of people involved, and therefore the impacts and "ripple effects" of adoption reach beyond mothers and the children who were adopted, to include fathers, spouses and other family members. The available information highlights a number of important issues, many of which relate to the experience of trauma.
One issue of particular importance is the trauma of the separation of mother and child, and the resulting experience of grief and loss. Mothers - particularly those who have not had any contact - continue to be traumatised by the thought that their child grew up thinking that they were not wanted. For example, one adoptee, after meeting her mother late in life, said of her mother: "There has hardly been a day in her life that she hasn't wondered where I was or had (I) ever survived" (cited in Swain & Swain, 1992, p. 47). In the words of one mother: "It wasn't the children who were not wanted; mothers weren't wanted because they were unmarried" (cited in Higgins, 2010, p. 13, emphasis added).
As noted by Connor and Higgins (2008), many people who experience potentially overwhelming or horrific life events appear to adapt and survive without developing a psychiatric disorder or other disability. But despite this capacity that humans have, "traumatic experiences" can so profoundly affect people that "the memory of one particular event comes to taint all other experiences" (van der Kolk & McFarlane, 1996, p. 4).
As a diagnostic category, post-traumatic stress disorder (PTSD) "created an organized framework for understanding how people's biology, conceptions of the world, and personalities are shaped by experience" (van der Kolk & McFarlane, 1996, p. 4). PTSD was used as a way of recognising the effects of trauma on the veterans of the Vietnam War, but there is growing recognition that similar stress reactions can be seen in response to other traumatic experiences, including childhood sexual abuse and adult rape.
There are similar parallels in relation to some people's experience of past adoption practices. Much of the research and case studies have focused on the issues of grief and loss experienced by these mothers, but their experiences may be better understood through this lens of "trauma".10 For example, Higgins (2010) noted that issues relating to consent and coercion (including illegal and/or discriminatory actions) point to some of the reasons why trauma may be evident. These issues include:
- administration of high levels of drugs to the mother in the perinatal period (including pain relief medication, sedatives and a hormone that suppresses lactation) that may have affected their capacity to consent;
- not allowing the mother to see the baby (such as active shielding with a sheet or other physical barrier during birth, or removing the baby or the mother from the ward immediately after birth);
- withholding information about the baby (e.g., gender, health information, or even whether the baby was a live birth);
- lying that the baby had died;
- not allowing the mother to hold or feed the baby;
- discouraging the mother from naming the baby;
- discouraging the mother from naming the father;
- bullying behaviour by consent-takers (seen as the "bastions of morality" who are protecting "good families");
- failing to advise the mother of her right to rescind the decision to relinquish, and the effective procedures to do so;
- failing to correctly obtain consent from the mother (e.g., the mother being too young to give consent; interactions with other issues raised above that prevent informed consent; consent being given while under the influence of drugs; mother not being informed of her rights, etc.);
- treating the mothers differently from married women (e.g., social workers and medical/nursing staff making assumptions that all unwed, pregnant mothers' babies would be adopted);
- being abandoned by their own mothers/families;
- the closed nature of past adoption practices (secrecy, and the "clean break" theory);
- the assumption of a married couple's entitlement to a child (adoption was a mechanism for dealing with infertility), with the joint "problem" of illegitimacy and infertility); and
- conducting experiments on newborn babies with drugs, with the children dying or being adopted without any follow-up of these experiments.
The grief and trauma is seen as "unresolvable", due to the silence surrounding closed adoption that prevents the mother from being able to mourn her loss (Goodwach, 2001; Rickarby, 1998). For mothers, the ongoing silence means knowing that their child is out there, wondering how they are, and knowing that there is a possibility of reunion - not the "severed bond" as promised by the clean break theory that shrouded the event in silence (Iwanek, 1997).
In describing the grief and trauma, many authors have drawn on related bodies of research, using infant-mother attachment research to support their contention that separation causes emotional damage to both mother and child (e.g., Cole, 2009). It is somewhat ironic that earlier research in this same field (e.g., Bowlby, 1969) was used to justify the practices of the time (i.e., not allowing the child to bond with the birth mother so as to provide a "clean break" that encourages bonding with the new adoptive parents).
As past adoption practices cannot be "undone", one of the steps in the journey for both parents and adoptees is that of making contact, and potentially being reunited. Given the variability in responses provided in the case study literature, and the absence of any systematic empirical evidence, this is an area where further research would be of particular value. Services attempting to support those affected - including professional counsellors, agencies and support groups - would all benefit from a greater understanding of typical pathways through the reunion process, estimates of the number of reunions that have occurred, the perspectives of those involved, and factors that are associated with positive and negative reunion experiences, and longer term outcomes.
Apart from these issues relating to contact and reunion, there are other ongoing issues for those affected by past adoption practices - particularly for mothers who experienced forced adoption - including problems with:
- personal identity (the concept of "motherhood" and self-identity as a good mother; the concept of family, identity and "belonging");
- relationships with others, including husbands/partners, subsequent children;
- connectedness with others (problematic attachments); and
- ongoing anxiety, depression and trauma (Higgins, 2011a).
The needs identified by writers in this field are consistent with the broader theoretical and empirical literature on other forms of trauma, such as the field of child abuse and neglect or adult sexual assault (Connor & Higgins, 2008; van der Kolk & McFarlane, 1996). As with other groups who have experienced pain and trauma, having society recognise what has occurred (i.e., naming it, and understanding how it occurred and its effects) is an important element in coping with and adjusting to the deep hurt they have experienced (Higgins, 2011a).
There is anecdotal evidence of the variability in adoption practices, ranging from women feeling that they were supported in making an informed decision, to reports of unjust, cruel and unlawful behaviours towards unmarried women during their pregnancy and birth experience.
Past adoption practices continue to affect the daily lives of many people, including the process of making contact between the mothers and fathers and adoptees (their now adult children), and the degree to which contact is seen as a "success" or not, and whether it leads to a long-term reunion.
From these identified issues, it is evident that there is a need for better information, counselling and support for those affected by past adoption practices. Additionally, more research is needed about the current views of fathers (whether they were - or are now - aware that they fathered a child who was adopted), adoptive families and their experiences of closed adoption, as well as the experiences of adoptees (including their perspectives on search and contact services, and their experiences of attempting to find out information and/or make contact).11
In the current study, we aim to address all these aspects, examining the degree to which a wide-ranging sample of Australians affected by past closed adoption practices have experienced different aspects, how this has affected them, and their current service needs. Although we attempt to provide detailed insight into all the specific categories of study participants, the weight of focus has been dependent on the levels of participation within each respondent group.
2.4 Senate Inquiry
The Senate Community Affairs References Committee (2012) concluded that having a range of psychological and psychiatric services was vital to addressing the needs of those affected by former forced adoption practices:
It is clear that there is a real need to make counselling and support services available to all the parties affected by adoption. These services can provide opportunities for people to talk about their experiences to explore inner pain and find a capacity for inner healing, which may help improve their quality of life. (p. 222)
Although the Senate Inquiry's (2012) terms of reference were focused on the experience of forced adoption, and examining the role of the Commonwealth, the report provides a number of insights into the experience of trauma, and how those affected can best be served. The report highlighted the "ongoing nature of the trauma caused by forced adoption, and the consequent need for counselling" (p. 219). Due to the complexity of the grief, a consistent theme was the need for specific counselling services by well-trained and experienced professionals.
The committee also noted the positive benefits of peer support:
Peer support groups play a role in assisting with post adoption support. Some members find validation and acceptance in the company of others with a similar experience, and benefit from "healing" relationships forged within these groups. (p. 231)
Although people who have had a common experience - such as parents and children separated through adoption - can benefit from peer support, there are some serious limitations. Consultations with a range of stakeholders as part of the current study would suggest that there are limits to the ability of peer support groups to adequately address all of the needs of people affected by adoption, with many articulating dissatisfaction with their experience of such groups. The Senate Inquiry (2012) report, for example, provided evidence from one submission that the unresolved trauma from forced adoption can be the very factor that limits the ability of mixed-group peer support processes to be effective:
Many adoptees have left groups because mothers have become frustrated and angry with them, which I believe is the result of the mother's inability to cope with their own unresolved issues of guilt and shame plus fears of possible abuses to their own child. (Ms Kerri Saint, Chair, White Australian Stolen Heritage) (p. 221)
In particular, the Senate Inquiry (2012) acknowledged that it was "not aware of any research comparing the effectiveness of trauma counselling by trained professionals and the support provided by members of peer support groups" (p. 232). One of the benefits of the AIFS study is its systematic examination of all kinds of support and professional services received, and which ones were most helpful.
The Senate Inquiry (2012) identified the role that counselling and peer support groups can provide in assisting with:
- the healing process;
- addressing specific mental health issues; and
- reconnecting with family members, which requires sensitivity, as well as specific knowledge of adoption processes and the experience of attempting to reconnect.
In its report, the Senate Inquiry (2012) emphasised the importance of services being affordable and accessible. It also identified the need for specialist training services for mental health care workers to meet the needs of people affected by past adoption experiences. The committee noted that "counselling to people affected by former forced adoption practices is a niche skill that cannot be developed without adequate exposure or training" (p. 226). Although such work could be carried out by a variety of mental health and social services, the Inquiry also acknowledged that there may be sensitivities among mothers over the role that social services, particularly social welfare agencies and/or religious organisations, had in historic practices.
6 "Permanency planning" refers to making decisions about alternative long-term foster/kinship care placements for children in out-of-home care as early as possible, to avoid the negative consequences of continuing to have failed attempts to restore children with birth parents.
7 The Victorian Council of the Single Mother and Her Children, set up in 1970, and a national equivalent set up in 1973, aimed to challenge the stigma of adoption and provide support to single and "relinquishing" mothers. The status of "illegitimacy" disappeared in the early 1970s, starting in 1974 with a Status of Children Act in both Victoria and Tasmania (in which the status of such births was changed to "ex-nuptial").
8 Abortion also became allowable under some circumstances in most states from the early 1970s; see the 1969 Menhennitt ruling (R v Davidson) in Victoria and the 1971 Levine ruling in NSW.
9 Women's magazines became fierce advocates for adoption, with waiting lists of prospective adoptive parents beginning to emerge in the 1940s and 1950s. As the "demand" for babies from infertile couples outstripped the availability of babies for adoption (though not for babies with disabilities), the pressure to relinquish was particularly high in maternity homes, where matrons and social workers were often personally acquainted with the prospective adoptive parents (see Marshall & McDonald, 2001; Swain & Howe, 1995).
10 Others have also looked at past adoptions through a "rights" lens, which emphasises issues of illegality, unfairness, and differential/prejudicial treatment, and the current "justice" needs of people affected (for example, Murphy, Quartly, & Cuthbert, 2009).
11 Part of the difficulty in assessing the quality of the evidence and drawing together consistent themes or conclusions from the research literature is that in this topic area, where the personal story is the data, it is very easy for (auto)biographies and/or case studies to pose as research. For example, one author who is frequently cited in relation to the experience of adoptees is Nancy Verrier, who outlined her "primal wound" theory about the effect of adoption on children. She presents her arguments using much of the language of academic research (e.g., Verrier, 1998, n. d.). Her arguments are based on a number of recognised theories (mainly psychoanalytic); however, despite articulating a hypothesis, she does not test the hypothesis (e.g., through experimental or observational data). Although often described as a "researcher", what she provides is more accurately described as an autobiographical perspective from an adoptive parent, drawing on research to understand her daughter's experience of adoption.
3. Quantitative survey of persons affected by adoption
3.1 Background
The purpose of the quantitative survey was to try to reach as many people as possible who had personal experiences from the period of closed adoption in Australia, in order to obtain an insight into these experiences. In particular, we were interested in the services and supports that they have accessed as well as their current need for services and support as a result of their experience of adoption.
Conducting a large-scale survey of people with experiences of past adoption practices was met with numerous challenges. The most significant issue was identifying persons who had been affected and inviting them to participate. A list of those affected by past adoption practices from which the sample could be obtained simply does not exist. A multi-level recruitment strategy was therefore developed to promote the study to potential participants in the community. Recruitment strategies were targeted across all Australian state/territories. Further details are given in section 3.4.
3.2 Persons affected by past adoption practices
Researchers have estimated that as many as 1 in 15 Australians are affected by an experience of closed adoption (Winkler, Brown, van Keppel, & Blanchard, 1988). This can include:
- mothers;
- fathers;
- adoptees, their families and children;
- adoptive parents and families; and
- the extended families of all of these people.
Adoption rates peaked in the early 1970s, when traditional societal expectations put pressure on unwed mothers to place their child for adoption. In 1971-72 almost 10,000 children were adopted in Australia, compared to 384 children in 2010-11. Now, more than half of adoptions (56%) are intercountry adoptions, and 19% are step-parent adoptions (AIHW, 2012).
If possible, this study was to produce best estimates of the number of mothers and children currently living in Australia who experienced closed adoption. This is difficult, partly due to the lack of records of people involved, but also due to the fact that no current database or collection on a national basis has this information. National data on adoptions are available from 1968; however, there is nothing systematic prior to that. As part of the research for this study, information has been sought from a variety of sources that include estimates of numbers involved, but we feel that the best estimates are those published by the Senate Inquiry (2012).
One source that provides some information on children who have been adopted is the Housing, Income and Labour Dynamics in Australia (HILDA) survey,12 which is a longitudinal national representative survey of currently around 13,000 respondents. In 2008, respondents were asked questions on the actual relationship of respondents to the persons they thought of as their mother and father, which included "adoptive" as a separate category. In that survey, 171 respondents indicated that they knew they were adopted. Based on these survey data, population estimates indicate that there currently are around 200,000 people aged 15 years and over in Australia who know they were adopted (95% confidence interval is 162,000 to 234,000). About 86% of these are Australian-born. The unweighted figures show 22% of adopted persons were aged under 35 years (many of whom may not have experienced the closed adoption practices of the period up until the mid-1970s and early 1980s, when legislation and practice progressively changed across the eight Australian states and territories), 57% were aged between 35 and 50 years, 15% were aged between 50 and 65 years, and 5% were aged over 65 years.
Although it would be expected the number of mothers of these children who are currently living in Australia would be somewhat less than 200,000, it is likely, when all the people who are closely related to the mothers and the person who was adopted are taken into account, we are talking about a significant proportion of the Australian population who have been affected by adoption. Therefore, one of the aims of this study was to try and attract as many respondents as possible in order to get a sense of the scope of the issues of those affected by past adoption practices.
3.3 Methodology
Survey populations
Separate survey instruments were developed for each of the respondent groups: mothers, fathers, persons who were adopted, adoptive parents and wider family members - (grand)parents, siblings, spouses and others. However, where appropriate, questions were consistent across the surveys to allow for comparisons across as well as within groups. Information about the background and circumstances of participants has also allowed for the different groups within the sample to be identified and compared.
Data collection
The main form of data collection was via an online survey using LimeSurvey software. Alternatively, participants (mothers, persons who were adopted, and adoptive parents) could request that they complete the survey in hard-copy format that they mailed back in a reply-paid envelope. Individuals who were either unable or unwilling to complete the survey via either of these avenues could request a telephone interview, in which a researcher went through the online survey with the respondent over the telephone.
The online survey was activated on 15 August 2011 and was held open until 30 March 2012. Initially it was intended that the data collection would be completed during 2011, but due to the extension of the Senate Inquiry hearing, it was decided to keep our survey open for a month after the Inquiry had released its report (on 29 February 2012) to allow participation by additional respondents who found out about the study through the media interest in the Senate Inquiry's findings.13
Summary of survey content and measures used
The survey included questions on:
- the circumstances (of the mother) at the time of the child's birth (where known);
- some details of the birth (such as use of drugs and contact with baby) - mothers only;
- separation from the child and consent for adoption - mothers and fathers only;
- the adoption process;
- sources of support at the time of pregnancy/birth and/or at time of adoption;
- seeking information and contact, and sources of support at the time of birth and currently;
- involvement with support/advocacy organisations;
- current demographic information for respondent;
- the effects of the events - mothers, fathers only; and
- stressful life events - mothers, fathers, persons who were adopted only.
Respondents were also asked about how they found out about the study.
Three health and wellbeing measures were included in the surveys in order to assist in understanding the effects of the past adoption experiences on the participants.
All respondents were asked to complete the Kessler Psychological Distress Scale (K10), which was used to assess the current mental health of the participants at the time of survey completion. The K10 is commonly used in population surveys and is a simple measure of psychological distress. Appropriate cut-offs for level of distress were developed for the 2001 Victorian Population Health Survey and age-standardised percentages in each level are available from the 2001 National Health survey (NHS). The instrument asks participants how often over the last four weeks they have experienced each of a list of 10 negative states (scored 1-5, with 1 indicating "none of the time" and 5 indicating "all the time"). The total score indicates their levels of distress and consequent likelihood of a mental health disorder. The maximum score is 50, indicating severe distress, and the minimum score is 10, indicating no distress, with in-between scores showing the following:
- less than 20 - likely to be well;
- 20-24 - likely to have a mild mental health disorder;
- 25-29 - likely to have moderate mental health disorder; and
- 30 and over - likely to have a severe mental health disorder.
The K10 is used widely in Australian surveys (such as the Australian Survey of Mental Health and Wellbeing, 1997, and the 2001 Victorian Population Health Survey) and is a good screening tool for identifying mental health disorders. It was also used by the National Transport Commission (2006) to screen for mental health disorders in safety critical workers.14
Mothers, fathers and persons who were adopted who completed their respective surveys were also asked to complete the World Health Organization Quality of Life brief instrument (WHOQOL-BREF).15 This 25-item scale is a shorter form of a quality of life assessment that was developed for use in cross-cultural circumstances. It allows the participant to rate their quality of life over the last two weeks and is used widely internationally and in Australia to provide a comparable measure of physical, mental and social wellbeing. Australian population norms are available.
The WHOQOL-BREF measures an individual's quality of life over four broad domains:
- physical health - comprising the facets of activities of daily living; dependence on medicinal substances and medical aids; energy and fatigue; mobility; pain and discomfort; sleep and rest; and work capacity;
- psychological - comprising the facets of bodily image and appearance; negative feelings; positive feelings; self-esteem; spirituality/religion/personal beliefs; and thinking, learning, memory and concentration;
- social relationships - comprising the facets of personal relationships; social support; and sexual activity; and
- environment - comprising the facets of financial resources; freedom, physical safety and security; health and social care: accessibility and quality; home environment; opportunities for acquiring new information and skills; participation in and opportunities for recreation/leisure activities; physical environment (pollution/noise/traffic/climate); and transport.
Mothers and fathers were also asked to complete the Impact of Event Scale-Revised (IES-R), a self-report measure that assesses subjective distress caused by traumatic events. Respondents are asked to identify a specific stressful life event (in this case, the separation from their child) and then indicate how much they were distressed or bothered during the past seven days by each "difficulty" listed. Items are rated on a five-point scale, ranging for 0 ("not at all") to 4 ("extremely"). A total score (ranging from 0 to 88) is calculated, and the cut-off scores for PTSD are: few or no PTSD symptoms (score under 12), several PTSD symptoms (12-32), likely to have PTSD (33 or more).
In addition to these three measures, mothers, fathers, adoptees and adoptive parents were asked to indicate how satisfied they were with their life in general, using a rating scale ranging from 1 ("completely dissatisfied") to 10 ("completely satisfied"). This was based on the measurement used in the Household, Income and Labour Dynamics in Australia (HILDA) survey.
For mothers who were separated from more than one child by adoption, details were also collected on the birth and adoption of the second child, and supports and services received at the time of the birth/adoption and since.
At both the beginning and end of the online survey, respondents were provided with a link to support services. For those completing the paper survey, a hard-copy list of services was included with the survey package.
Survey testing
Prior to the rollout of each respondent survey version, the online surveys underwent extensive testing by both Institute staff and a number of invited stakeholders. However, once the survey went "live", we were contacted by one stakeholder group with concerns over two of the questions: one related to the order in which response categories were listed for the question about the respondents' preferred terminology for "mother who was separated from her child by adoption"; the other related to the response categories for the question about the timing of the separation (i.e., "How long after birth was the child removed?"), with the stakeholder group wanting the inclusion of the category "immediately".
Changes were made to the survey to address these concerns, so there is a small inconsistency between the original surveys and those completed from 16 September 2011. This is addressed as necessary in our discussion of the results.
Some respondents (fewer than fifty) had some technical difficulties when completing the survey. This was due to "timing out" from the online survey where either the internet connection was too slow or the server capacity was limited.
When this occurred, participants were directed to a web page that provided a phone number for the IT help desk at AIFS who assisted them with identifying and resolving the problem. Participants who experienced these issues were also offered a hard-copy survey or a telephone survey.
Minimising traumatic responses
Given that the actual act of completing the survey may potentially trigger emotional responses from individuals, ethics processes and measures were put in place to try and minimise these effects. These included:
- adding a warning in an introductory page before entering the survey about the potential emotional responses that the questions could trigger;
- encouraging participants to take a break when needed, which was enacted by including an explanation in the introduction on how to save and re-enter the survey;
- providing a list of support agencies and organisations, as well as contact information after the completion of the survey; and
- contacting participants directly when returned hard-copy surveys indicated they had experienced high levels of distress when completing the survey.
Despite these measures, we still received feedback from numerous individuals regarding just how traumatic this process had been for them, although in most instances, they felt it had been cathartic and that it was important nonetheless for their contributions to be made. Senior project staff spent a significant amount of time providing support to participants over the phone and by email throughout the data collection period.
Survey completion time varied depending on the respondent group: it was the longest for mothers and fathers, followed by adoptees, adoptive parents, and finally other family members. Given participants had the option of saving responses and returning at a later time, it is difficult to estimate completion times accurately. Those who completed the hard-copy version of the survey also had varied response times, with many attaching additional written information further explaining their experience, as well as attaching copies of documents relating to their experience of adoption, such as medical records, adoption papers and birth certificates.
3.4 Publicity and promotion
The objective of the communication program was to recruit to the study surveys:
- people affected by adoption - parents, adoptees, adoptive parents, and other family members, including other children, spouses and grandparents; and
- service providers - counsellors, psychologists, psychiatrists, psychotherapists and others working with people affected by past adoption experiences.
Phase 1
Phase 1 commenced as soon as the first survey (for core groups) was live and operating successfully online, on 15 August 2011. It focused primarily on people affected by adoption. There were two purposes to the promotional activity:
- to raise awareness of the purpose of the survey - that is, to understand the current service and support needs of people affected by past adoption practices, including forced adoption; and
- to prompt action - that is, to encourage people to participate in the survey.
It comprised a number of elements to reinforce the key messages and invite action:
- Website - The website provided background information on the survey, contacts for support services and a link to the survey site.
- Direct emails - These went to more than 500 interest groups, advising them of the survey, providing a prepared newsletter-style piece that they were invited to use, and inviting them to link to the Past Adoptions research project website. These interest groups included adoption support groups, family counselling services, mental health services, church and welfare groups and local government authorities.
- Media relations - Background information, website details and an editorial-style media release were provided to:
- 250 grassroots media organisations in regional and remote areas;
- 2 community magazines;
- 11 family and parenting magazines;
- 4 magazines for people interested in researching their genealogy; and
- 7 seniors magazines.
- Radio - Coverage was generated on the ABC Radio's national current affairs program, AM.
- Media background briefing packs - These were distributed to key metropolitan broadcast and telecast media before the pro-adoption National Adoption Awareness Week (6-13 November) to help balance the celebratory style for people with the less successful experiences of adoption.
- Social media - A program that used Twitter (with the hash tag #adoptions) and Facebook ran in September 2011.
- AIFS corporate communications - The survey was publicised through AIFS publications and networks, including:
- the AIFS Family Matters journal, editions 88 (August 2011) and 89 (November 2011);
- four issues of AIFS Alert, an email-style newsletter distributed to around 2,800 subscribers;
- a postcard-sized promotional card, providing contact details for accessing the survey, distributed at AIFS events in September, October and November 2011, and in delegate satchels at a number of conferences in November 2011, including the Family Relationship Services Australia national conference (550 delegates, primarily family counsellors and social workers); the Longitudinal Study of Australian Children & Longitudinal Study of Indigenous Children conference (220 delegates, including researchers and academics from throughout Australia); and the AIHW Australia's Welfare conference (450 delegates from the health and welfare sector).
Phase 2
Phase 2 of the promotional activity aimed to:
- reinforce awareness messages and the invitation to participate - focused on the people affected by adoption; and
- raise awareness of the surveys and invite participation in the service providers survey - focused on the service providers.
The main activity for Phase 2 centred on the service providers survey going live. It comprised a number of elements, again designed to reinforce messages and invite the action of survey participation:
- Social media - A short video by Dr Daryl Higgins (Deputy Director, Research at AIFS) explaining the survey was posted on YouTube, and ongoing Twitter activity on the issue directed people to the surveys.
- Past and Present Adoptions in Australia - This Facts Sheet publication was distributed in hard copy and electronically to media and interest groups, including:
- participants at the AIFS Seminar Series (February and March 2012); and
- at the release of the report from the Senate Inquiry into the Commonwealth's Contribution to Former Forced Adoption Policies and Practices, in Canberra on 29 February 2012.
- Direct contact and support emails - These were directed at service providers and representative bodies.
- Media relations - In preparation for the release of the Senate Inquiry report on 29 February:
- a media backgrounder section, Reporting on Adoption,16 was developed on the AIFS website that provided background information on the issue, links to key resources such as Family Matters articles, the Facts Sheet, the YouTube video, contacts for counselling services, links to the surveys, and links to samples of previous media coverage of the issue; and
- more than 700 media outlets and individuals (parliamentary reporters, regional media and a few specialist publications for seniors, women and families) were contacted, providing the link to the backgrounder and alerting them to the forthcoming release of the report.
3.5 Response
The largest group of respondents were people who had been adopted (54% of all respondents), followed by mothers separated from their child by adoption (33%), adoptive parents (6%), and other family members (6%). Only 12 fathers responded (< 1%) (see Table 3.1). Around a quarter of mothers and adoptive parents who responded to the survey used the paper-and-pencil version, whereas fewer than 10% of adopted persons did so.
Table 3.2 shows the distribution and response rates for the hard-copy surveys. Response to the survey was certainly helped by having other organisations distribute hard copy forms for us. For "other" organisations who distributed hard-copy surveys on our behalf, we can only be certain of the number of copies that we sent to them; the number that they actually gave out may well be less. For those surveys that were sent from AIFS upon request, the response rate was 63% overall.
As mentioned, we asked survey respondents to indicate how they found out about the study (Table 3.3). This helps provide an indication of the success of our communication strategy. Adoption support services provided a lot of assistance in publicising this study via their communication channels, and we know from focus group discussions and comments on the questionnaires that many people who completed the survey also notified others about the survey. AIFS' communication strategies were also successful in getting the survey mentioned across a number of media outlets; in particular, on radio.
| Respondent | Online | Hard copy | Totals | % of all respondents |
|---|---|---|---|---|
| Mother separated from child by adoption | 376 | 129 | 505 | 33.0 |
| Father separated from child by adoption | 12 | 0 | 12 | 0.8 |
| Person who was adopted | 771 | 52 | 823 | 53.9 |
| Adoptive parents | 72 | 22 | 94 | 6.2 |
| Other family members | 94 | 0 | 94 | 6.2 |
| Totals | 1,327 | 203 | 1,528 | 100.0 |
| No. sent a | No. returned | Response rate (%) | |
|---|---|---|---|
| Mother | 380 | 129 | 33.9 |
| AIFS | 61 | 43 | 70.5 |
| Other | 319 | 86 | 27.0 |
| Person who was adopted | 91 | 52 | 57.1 |
| AIFS | 80 | 48 | 60.0 |
| Other | 11 | 4 | 36.4 |
| Adoptive parents (AIFS) | 39 | 22 | 56.4 |
| Totals | 510 | 203 | 39.8 |
Note: a Where "Other" organisations distributed hard-copy forms for us, we can only be certain about the number of copies sent to them by us, not the actual number of forms that the organisations sent to potential survey participants.
| Mother | Adopted person | Adoptive parent | Other a | Total | |
|---|---|---|---|---|---|
| Adoption support service | 178 | 157 | 2 | 8 | 345 |
| Friend/family member | 67 | 155 | 26 | 29 | 277 |
| Newspaper/newsletter | 105 | 154 | 35 | 14 | 308 |
| AIFS website | 59 | 119 | 7 | 17 | 202 |
| Radio | 51 | 165 | 12 | 15 | 243 |
| Website, including social networking | 25 | 103 | 1 | 8 | 137 |
| Told by health/welfare professional | 13 | 26 | 1 | 7 | 47 |
| Television | 20 | 40 | 60 | ||
| Other | 14 | 32 | 2 | 7 | 55 |
| Unsure | 12 | 4 | 16 | ||
| No. of observations | 532 | 963 | 90 | 105 | 1,690 |
Note: Participant could select more than one option. a Includes fathers and other family members.
We were also interested in whether the survey respondents were involved with adoption support organisations (Table 3.4). Around 5% of respondents currently work for a support organisation, and 17% identify as members of these organisations.
| Mother ( n = 505) | Adopted person ( n = 823) | Adoptive parent ( n = 94) | Other a ( n = 106) | Total ( n = 1,528) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | No. | % | No. | % | |
| Work for b | 32 | 6.3 | 34 | 4.1 | 5 | 5.3 | 11 | 10.4 | 82 | 5.4 |
| Member of b | 153 | 30.3 | 92 | 11.2 | 9 | 9.6 | 5 | 4.7 | 259 | 17.0 |
| Neither | 336 | 66.5 | 704 | 85.5 | 80 | 85.1 | 92 | 86.8 | 1213 | 79.3 |
Notes: a Includes fathers and other family members. b Respondents could be both a "member of" and "work for" a support organisation.
3.6 Respondent characteristics
As the quantitative survey is a self-selected sample, from an unknown total population, it does not provide a figure that could be used to estimate the prevalence of mothers, fathers and children who experienced closed adoption. Care therefore needs to be taken in generalising the information obtained. However, given the large number of respondents overall, in conjunction with other information and data sources, the responses to the survey are able to contribute to our understanding of the extent of service needs within these groups. Based on their higher levels of participation in the study, we will provide an overview of the three main respondent groups (mothers, persons who were adopted and adoptive parents) in the following sections.
Mothers
There were 505 mothers who had been separated from their child by adoption who responded to our survey (Table 3.5). Close to 80% of these mothers were aged 55-69 years at the time they completed the survey. Mothers living in all states and territories were represented in the sample.
About half of the mothers were currently married, and one-quarter were divorced. Eighty per cent of the mothers had been born in Australia, and very few identified as Aboriginal or Torres Strait Islander. A small proportion (5%) identified as Forgotten Australians.17
Over half of the mothers were not working, with roughly equal numbers working full-time and part-time. Over 30% had an undergraduate degree or higher qualification.
A very small proportion of mothers who responded to the survey (6%; n = 30) had more than one child adopted; and a few of these had more than two adopted. Although we have collected data for the second child adopted, analysis of these data is outside the scope of the current report, and therefore we have presented findings on the first child who was adopted only.
| Respondent characteristics | Number | Per cent |
|---|---|---|
| Age at time of survey completion | ||
| Under 45 years | 12 | 2.4 |
| 45-49 years | 21 | 4.2 |
| 50-54 years | 50 | 9.9 |
| 55-59 years | 115 | 22.8 |
| 60-64 years | 163 | 32.3 |
| 65-69 years | 109 | 21.6 |
| 70 years and over | 35 | 6.9 |
| No. of observations | 505 | 100.0 |
| Where live | ||
| New South Wales | 117 | 23.2 |
| Victoria | 128 | 25.3 |
| Queensland | 77 | 15.2 |
| South Australia | 65 | 12.9 |
| Western Australia | 37 | 7.3 |
| Tasmania | 17 | 3.4 |
| Northern Territory | 11 | 2.2 |
| Australian Capital Territory | 25 | 5.0 |
| Overseas | 11 | 2.2 |
| Missing | 17 | 3.4 |
| No. of observations | 505 | 100.0 |
| Whether speaks language other than English at home | ||
| Yes | 6 | 1.2 |
| No | 495 | 98.0 |
| Missing | 4 | 0.8 |
| No. of observations | 505 | 100.0 |
| Whether of Aboriginal or Torres Strait Islander descent | ||
| Yes | 9 | 1.8 |
| No | 487 | 96.4 |
| Missing | 9 | 1.8 |
| No. of observations | 505 | 100.0 |
| Whether member of Stolen Generations or Forgotten Australians | ||
| No | 457 | 90.5 |
| Member of Stolen Generation | 5 | 1.0 |
| Forgotten Australian | 23 | 4.6 |
| Both | 5 | 1.0 |
| Missing | 15 | 3.0 |
| No. of observations | 505 | 100.0 |
| Where born | ||
| Australia | 402 | 79.6 |
| Overseas | 90 | 17.8 |
| Missing | 13 | 2.6 |
| No. of observations | 505 | 100.0 |
| Current marital status | ||
| Never been married (single, engaged) | 31 | 6.1 |
| De facto/Same-sex partnership | 25 | 4.9 |
| Married | 261 | 51.7 |
| Separated | 24 | 4.8 |
| Divorced | 125 | 24.8 |
| Widowed | 34 | 6.7 |
| Missing | 5 | 1.0 |
| No. of observations | 505 | 100.0 |
| Current employment status | ||
| Working full-time | 105 | 20.8 |
| Working part-time | 110 | 21.8 |
| Not working | 284 | 56.2 |
| Missing | 6 | 1.2 |
| No. of observations | 505 | 100.0 |
| Current main source of income | ||
| Wages or salary (including self-employed) | 216 | 42.8 |
| Government benefits | 191 | 37.8 |
| Not working | 27 | 5.3 |
| Self-funded retiree/ superannuation | 33 | 6.5 |
| Self-funded and government benefits | 7 | 1.4 |
| Other | 13 | 2.6 |
| Missing | 18 | 3.6 |
| No. of observations | 505 | 100.0 |
| Highest level of education | ||
| Not completed secondary/high school | 84 | 16.6 |
| Secondary/High school | 122 | 24.2 |
| Diploma/Certificate/Trade qualification | 128 | 25.3 |
| Undergraduate degree | 46 | 9.1 |
| Graduate qualification | 58 | 11.5 |
| Postgraduate degree | 61 | 12.1 |
| Missing | 6 | 1.2 |
| No. of observations | 505 | 100.0 |
Note: Percentages may not total exactly 100.0% due to rounding.
Persons who were adopted
There were 823 respondents to the "persons who were adopted" survey, covering a wide range of ages (Table 3.6). The largest group of respondents were aged in their 40s.
About 65% of the respondents were currently married or in a de facto relationship, 16% were divorced or separated, and 14% had never married. Over 90% had been born in Australia, and 3% were of Aboriginal or Torres Strait Islander descent. A small proportion (4%) identified as Forgotten Australians.
Just under a third of the respondents were not working, 40% were working full-time and 28% part-time. Around 30% had an undergraduate degree or higher qualification.
All states and territories were well represented in the sample.
| Respondent characteristics | Number | Per cent |
|---|---|---|
| Age at time of survey completion | ||
| Under 25 years | 10 | 1.2 |
| 25-29 years | 15 | 1.8 |
| 30-34 years | 27 | 3.3 |
| 35-39 years | 94 | 11.4 |
| 40-44 years | 202 | 24.5 |
| 45-49 years | 137 | 16.6 |
| 50-54 years | 92 | 11.2 |
| 55-59 years | 96 | 11.7 |
| 60-64 years | 68 | 8.3 |
| 65-69 years | 50 | 6.1 |
| 70-74 years | 19 | 2.3 |
| 75 years and over | 13 | 1.6 |
| No. of observations | 823 | 100.0 |
| Where live | ||
| New South Wales | 209 | 25.4 |
| Victoria | 202 | 24.5 |
| Queensland | 150 | 18.2 |
| South Australia | 90 | 10.9 |
| Western Australia | 50 | 6.1 |
| Tasmania | 20 | 2.4 |
| Northern Territory | 23 | 2.8 |
| Australian Capital Territory | 59 | 7.2 |
| Overseas | 15 | 1.8 |
| Missing | 5 | 0.6 |
| No. of observations | 823 | 100.0 |
| Whether speaks language other than English at home | ||
| Yes | 22 | 2.7 |
| No | 797 | 96.8 |
| Missing | 4 | 0.5 |
| No. of observations | 823 | 100.0 |
| Whether of Aboriginal or Torres Strait Islander descent | ||
| Yes | 23 | 2.8 |
| No | 787 | 95.6 |
| Missing | 13 | 1.6 |
| No. of observations | 823 | 100.0 |
| Whether member of Stolen Generation or Forgotten Australians | ||
| No | 761 | 92.5 |
| Member of Stolen Generation | 6 | 0.7 |
| Forgotten Australian | 31 | 3.8 |
| Both | 9 | 1.2 |
| Missing | 16 | 1.9 |
| No. of observations | 823 | 100.0 |
| Where born | ||
| Australia | 750 | 91.1 |
| Overseas | 44 | 5.3 |
| Missing | 29 | 3.5 |
| No. of observations | 823 | 100.0 |
| Current marital status | ||
| Never been married (single, engaged) | 116 | 14.2 |
| De facto | 102 | 12.3 |
| Same-sex partnership | 25 | 3.0 |
| Married | 427 | 52.1 |
| Separated | 37 | 4.5 |
| Divorced | 91 | 11.0 |
| Widowed | 21 | 2.6 |
| Missing | 4 | 0.5 |
| No. of observations | 823 | 100.0 |
| Current employment status | ||
| Working full-time | 332 | 40.3 |
| Working part-time | 227 | 27.6 |
| Not working | 260 | 31.6 |
| Missing | 4 | 0.5 |
| No. of observations | 823 | 100.0 |
| Current main source of income | ||
| Wages or salary (including self-employed) | 546 | 66.3 |
| Government benefits | 130 | 15.8 |
| Not working | 28 | 3.4 |
| Self-funded retiree/ superannuation | 0 | 0.0 |
| Other | 113 | 13.7 |
| Missing | 6 | 0.7 |
| No. of observations | 823 | 100.0 |
| Highest level of education | ||
| Not completed secondary/high school | 77 | 9.4 |
| Secondary/High school | 146 | 17.7 |
| Diploma/Certificate/Trade qualification | 248 | 30.1 |
| Undergraduate degree | 96 | 11.7 |
| Graduate qualification | 91 | 11.0 |
| Postgraduate degree | 161 | 19.6 |
| Missing | 4 | 0.5 |
| No. of observations | 823 | 100.0 |
Note: Percentages may not total exactly 100.0% due to rounding.
Adoptive parents
There were 94 adoptive parents who responded to our survey (Table 3.7). The majority of respondents were aged over 60 years when they completed the survey, with a quarter of them aged 75 years and over.
| Respondent characteristics | Number | Per cent |
|---|---|---|
| Age at time of survey completion | ||
| Under 60 years | 9 | 9.6 |
| 60-64 years | 10 | 10.6 |
| 65-69 years | 26 | 27.7 |
| 70-74 years | 24 | 25.5 |
| 75 years and over | 25 | 26.6 |
| No. of observations | 94 | 100.0 |
| Where live | ||
| New South Wales | 22 | 23.4 |
| Victoria | 25 | 26.6 |
| Queensland | 17 | 18.1 |
| South Australia | 9 | 9.6 |
| Western Australia | 8 | 8.5 |
| Tasmania | 1 | 1.1 |
| Australian Capital Territory | 9 | 9.6 |
| Other | 1 | 1.1 |
| Missing | 2 | 2.1 |
| No. of observations | 94 | 100.0 |
| Whether speaks language other than English at home | ||
| Yes | 2 | 2.1 |
| No | 91 | 96.8 |
| Missing | 1 | 1.1 |
| No. of observations | 94 | 100.0 |
| Whether of Aboriginal or Torres Strait Islander descent | ||
| No | 91 | 96.8 |
| Missing | 3 | 3.2 |
| No. of observations | 94 | 100.0 |
| Whether member of Stolen Generations or Forgotten Australians | ||
| No | 90 | 95.7 |
| Member of Stolen Generation | 1 | 1.1 |
| Missing | 3 | 3.2 |
| No. of observations | 94 | 100.0 |
| Where born | ||
| Australia | 71 | 75.5 |
| Overseas | 21 | 22.3 |
| Missing | 2 | 2.1 |
| No. of observations | 94 | 100.0 |
| Current marital status | ||
| Married/ de facto | 63 | 67.0 |
| Separated | 5 | 5.3 |
| Divorced | 9 | 9.6 |
| Widowed | 15 | 16.0 |
| Missing | 2 | 2.1 |
| No. of observations | 94 | 100.0 |
| Current employment status | ||
| Working full-time | 8 | 8.5 |
| Working part-time | 9 | 9.6 |
| Not working | 74 | 78.7 |
| Missing | 3 | 3.2 |
| No. of observations | 94 | 100.0 |
| Current main source of income | ||
| Wages or salary (including self-employed) | 15 | 16.0 |
| Government benefits | 49 | 52.1 |
| Self-funded retiree/ superannuation | 17 | 18.1 |
| Self-funded plus government benefits | 2 | 2.1 |
| Not working | 6 | 6.4 |
| Other | 2 | 2.1 |
| Missing | 3 | 3.2 |
| No. of observations | 94 | 100.0 |
| Highest level of education | ||
| Not completed secondary/high school | 9 | 9.6 |
| Secondary/High school | 34 | 36.2 |
| Diploma/Certificate/Trade qualification | 19 | 20.2 |
| Undergraduate degree | 5 | 5.3 |
| Graduate qualification | 13 | 13.8 |
| Postgraduate degree | 12 | 12.8 |
| Missing | 2 | 2.1 |
| No. of observations | 94 | 100.0 |
Note: Percentages may not total exactly 100.0% due to rounding.
Footnotes
12 The HILDA survey is a household-based panel study that began in 2001. The Wave 1 panel consisting of 7,682 households and 19,914 individuals.
13 Copies of the surveys and other study documentation are available from the authors.
14 For more information on the K10, see: <www.hcp.med.harvard.edu/ncs/k6_scales.php>.
15 For more information on the WHOQOL-BREF see: <www.who.int>.
16 See Reporting on adoption.
17 Forgotten Australians are adults who spent a period of their childhood or youth in children's homes, orphanages and other forms of out-of-home care, up to 1989. At least 500,000 children grew up or spent long periods in this institutional care system in the 20th century, which was the standard form of out-of-home care in Australia at the time.
4. Qualitative data collection from persons affected by adoption
4.1 Background
The survey data were complemented with more detailed information obtained via qualitative methods: open-end responses in the surveys and both focus group discussions and personal interviews. This enabled issues to be explored in more depth and also for discussion to be conducted around suggestions for services and supports to meet current needs.
4.2 Methodology
The interviews and focus groups took a semi-structured approach, with an emphasis on identifying current and past service use as well as current service needs. We did not concentrate on just negative or positive experiences, but sought to include perspectives from people who had experienced a range of events and reactions.
Recruitment
All participants included quantitative data in their survey responses. In addition, they were also asked to express interest in potentially participating in either a follow-up interview or focus group discussion (with separate groups for each respondent group). Due to the high level of interest in participating in the follow-up discussions, it was decided to hold focus groups in the first instance, and only conduct one-to-one interviews upon specific request, either face-to-face or by telephone.
This approach allowed for respondents from different groups and with different experiences to be represented in the follow-up study, as well as reflecting a geographic spread across all states and territories, to the extent that this was practicable.
The process that was followed to arrange the focus groups and interviews was as follows:
- An email was sent to all registered respondents to confirm their continued interest in follow-up participation and to clarify their respondent group, age, preference for interview or focus group, and current location.
- Based on the replies to the initial email, locations were selected across the country, based on the number of people living in particular locations. Those who were living either in or near these locations were sent an email with information on potential dates and times for face-to-face contact.
- Venues were organised based on the participants' capacity to attend a central location and whether they needed out-of-hours sessions.
Response
In relation to the face-to-face consultations, the vast majority of the recruitment for this phase of the study was from the pool of those who had completed the online or hard-copy surveys and had indicated their willingness to potentially be part of a follow-up discussion or interview. A small number of individuals who contacted the Institute in relation to the study or were referred by other participants were also able to attend the groups.
We were overwhelmed by the high proportion of respondents willing to take part in the follow-up interviews/focus groups (70% of all participants). As at February 2012, there had been 881 registrants who had indicated this interest. Follow-up registration was cut off in late January/early February, due to the bulk of the fieldwork activities being conducted across the country throughout February.
After attempting to make contact with these 881 individuals:
- just over 700 people replied to indicate their continued interest in follow-up participation;
- approximately 30 were residing overseas and therefore unable to participate; and
- approximately 150 individuals either did not respond or did not wish to continue in the follow-up component of the study.
Of the 700 individuals who indicated continued interest:
- around 150 people were located in regions that we were unable to accommodate due to either the remoteness of the location or the low numbers of registrants residing in that particular area for us to justify the travel;
- around 550 people were then contacted with details of forthcoming visits to their cities/towns with possible times to meet; and
- around 350 people indicated they would attend a given session, though a number of these failed to attend the relevant session.
We were thus able to meet face-to-face with around 280 individuals who indicated they would be available to attend on the proposed dates - a much higher number than the original 200 individuals that had been planned for in the original study methodology. Table 4.1 shows the locations used, the types of sessions and the number of people who attended.
There were approximately 20 individuals with whom we organised to conduct phone interviews because they were either unable to attend the focus groups in their areas or they were in locations to which we were unable to travel.
A number of individuals contacted us directly who did not feel able to complete the online or hard-copy survey for a variety of reasons, but who still wished to provide information regarding their experiences. All of those who fell into this category (no more than 20) were contacted over the phone or by email and they provided their information through conversation with project staff, by detailed email or by written correspondence sent by post.
Venues
A number of individual agencies provided Institute staff with a venue and catering free-of-charge at which to conduct the qualitative components of the study. Their generosity and willingness to accommodate our needs is greatly appreciated.
A large proportion of the groups and interviews were held in public places, such as a café. These venues were, for the most part, selected based on local participants' knowledge of appropriate locations that would allow for privacy and comfort. Conduct of qualitative interviews in "neutral" settings is a common method of engagement, particularly with vulnerable populations, as it allows for a more relaxed discussion and, hence, is often more conducive to individuals' feelings of safety in their participation. We encountered only two participants who expressed concern regarding this arrangement, and appropriate discussions were held with them to ascertain their willingness to continue participation and what support they may need as a consequence. Both individuals continued their participation in the focus group discussions and at the conclusion of the process remained comfortable with their decision.
| State/territory | Region | Date | Details |
|---|---|---|---|
| Queensland | Toowoomba | November 2011 | 1 interview (adoptee) 1 focus group (adoptees) |
| Brisbane | November 2011 | 4 focus groups (2 adoptees; 2 mothers) | |
| January 2012 | 4 focus groups (2 adoptees; 2 mothers; 1 adoptive parents) | ||
| Gold Coast | February 2012 | 1 interview (adoptee) 1 focus group (adoptee) | |
| New South Wales | Orange | November 2011 | 1 focus group (adoptees) |
| Coffs Harbour | February 2012 | 1 focus group (adoptees) | |
| Maclean | February 2012 | 1 interview (mother) | |
| Wollongong | February 2012 | 2 focus groups (1 adoptees; 1 mothers) | |
| Penrith | February 2012 | 1 focus group (adoptees) 2 interviews (mothers) | |
| Gosford | February 2012 | 2 focus groups (1 adoptees; 1 mothers) | |
| Newcastle | February 2012 | 2 focus groups (1 adoptees; 1 mothers) | |
| Sydney | February 2012 | 8 focus groups (5 adoptees; 3 mothers) 2 interviews (1 father; 1 adoptive parents) | |
| Victoria | Melbourne | October 2011 | 2 focus groups (1 adoptees; 1 mothers) |
| February 2012 | 8 focus groups (4 adoptees; 2 mothers; 1 adoptive parents; 1 fathers) | ||
| March 2012 | 5 focus groups (3 adoptees; 2 mothers) | ||
| Tasmania | Hobart | February 2012 | 2 focus groups (1 adoptees; 1 mothers) |
| South Australia | Adelaide | February 2012 | 5 focus groups (3 adoptees; 2 mothers) 2 interviews (service providers)> |
| Western Australia | Perth | February 2012 | 4 focus groups (2 adoptees; 2 mothers) |
| Mandurah | February 2012 | 1 focus group (adoptees) 2 interviews (1 mothers; 1 adoptive parents) | |
| Albany | February 2012 | 2 focus groups (1 adoptees; 1 adoptive parents) | |
| Northern Territory | Darwin | January 2012 | 1 focus group (mixed) |
| ACT | November 2011 | 2 focus groups (1 adoptees; 1 mothers) 2 interviews (1 adoptee; 1 other family member) |
4.3 Reasons for participation
In the focus group discussions, by way of introduction, participants were asked to reflect on their reasons for taking part and what they were hoping to gain from being involved in the study. This provided some insight into the differing motivations and desires of those who have been touched by adoption. For many, these discussion groups were the first time they had ever met other people who had an adoption story, and in and of itself this was viewed as being of great benefit to participants.
The most common reasons provided in response to the question about participation were to:
- meet other people with shared experiences;
- increase public awareness of the effects of their own experiences;
- broaden the public discussion around adoption;
- highlight the improvements that are needed in the current availability of services, including how and what information is provided to them;
- highlight the gaps in services, information and supports available;
- provide a balanced view point; and
- ensure that history isn't repeated in the current adoption and donor conception environment by increasing awareness of the potential effects that adoption has on all parties involved.
They also expressed the hope that their participation will not have been in vain.
4.4 Recordings and transcription
All focus groups and a number of the interviews were recorded, with the consent of the participants. AIFS researchers undertook transcriptions of the recordings. Qualitative data were coded and thematically analysed according to the respondent group and key research questions. Results from the open-response survey items and focus group discussions were used to both illustrate findings from the quantitative survey as well as quantify majority views held by group participants.
Quotes used throughout the report from study participants have been referenced in two ways. Open-response items from the surveys are identified by a survey identification number followed by the year of response (e.g., "100, 2012"); and quotes from focus group discussions and interviews are referenced by respondent group category and the state from which the participant comes (e.g., "Mother, Qld").
4.5 Service provider survey
In a separate survey, service providers were asked their perspectives on the current needs of those affected by past adoption experiences, and their professional opinions about what works best in delivering effective services to clients. The recruitment strategy and results of service providers' contributions are discussed in detail in Chapter 10.
Given the limited number of participants in the service providers surveys and the small pool of adoption services, we have not included quote attributions for these respondents in order to ensure their confidentiality/anonymity.
5. Mothers separated from children by adoption
5.1 Introduction
The aim of this national research study is to utilise and build on existing research and evidence about the extent and effects of past adoption practices to strengthen the evidence available to governments to address the current needs of those affected. The literature pertaining to the effects of separation from their child for mothers highlights the importance of their stories being told as one means of healing and recovery (Higgins, 2010). By hearing people's stories, their journeys and their perspectives of their adoption experience, it is possible to begin to understand more meaningfully the effects of these experiences as they pertain to what would be effective strategies of support and intervention. These past experiences are therefore a strong focus in the delivery of the study findings.
Accordingly, the results will be presented by first re-visiting mothers' experiences of: pregnancy; birth; the adoption process, including the main reasons for the adoption and process of obtaining consent; and the search and contact process (see Attachment B for detailed data tables). This is followed by an examination of the effects of these experiences on mothers' wellbeing and other aspects of their lives. The chapter finishes with a discussion of mothers' current service and support needs as a result of their experiences.
The information is drawn from the responses of the 505 mothers who took part in the quantitative survey and those respondents who participated in follow-up discussions.
We didn't know what was going to happen. We were women that were left by everybody. (Mother, Qld)
5.2 Pregnancy
As detailed in Chapter 2, there was a steady increase in the number of adoptions in Australia in the late 1960s, peaking in 1971-72, with almost 10,000 adoptions recorded that year. The respondents to the survey reflected this trend, as shown in Figure 5.1. (The data from the study have been scaled up by a factor of 100 in order for the two series to be compared more easily.)
Relationship status
Over 70% of the surveyed mothers indicated that at the time of their pregnancy, they were in a relationship with the father of their child (see Table B1). A further 19% stated that the father was an acquaintance or relative. Only a small minority indicated that the father was previously unknown to them. Many mothers who participated in the focus group discussions said that they planned to marry the father of their child and that, although the pregnancy was unplanned, they were committed to raising the child together:
I was in love (and still am) with my daughter's father and would have loved to have been a family together. That was not to be. (54, 2011)
When he saw me, the fear subsided and we became very very close and very determined to get married and have the baby - to keep the baby. And I thought that was the end of the matter. And that's the story I have lived with for forty-three years. (Mother, WA)
Figure 5.1: Number of adoptions in Australia and trends based on study respondents, 1950 to 1993
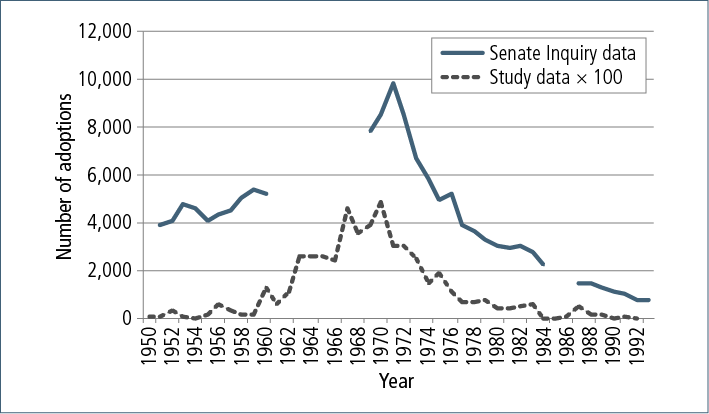
Note: Data from study has been scaled up by a factor of 100 to allow comparison of trends.
Source: Senate Inquiry, 2012; AIFS, 2012
Some mothers did go on to marry the father of their child and had subsequent children together who were not adopted:
My husband is the father of my son. We have been married 42 years. (Mother, WA)
My boyfriend and I wanted to be married and keep our daughter. We did marry two years later. (1276, 2012)
I ended up marrying the father of my adopted son and had three other children. We didn't have any other children for 9 years as we felt such a sadness of losing our son. We weren't given the chance to decide; it was taken from us, and it affected us, and it still does. (1683, 2012)
Many of the fathers who had been acquaintances or comparative strangers were either unable to be informed, or it was inappropriate to inform them of the pregnancy (for example, in the case of women who were pregnant as a result of being sexually assaulted). Survey participants were asked whether their pregnancy was a result of consensual or non-consensual sex (see Table B2). A small proportion of participants declined to answer this question (7%). Although the large majority (82%) of responses indicated the pregnancy was a result of consensual sex, 11% reported conception was the outcome of non-consensual sex. Anecdotal accounts from the focus group discussions ranged from feeling pressured from their boyfriends to have sex but not knowing how to say no to them, through to extreme acts of violence from a stranger, acquaintance or relative.
Place of residence
Although there was parental knowledge of the pregnancy in the majority of cases within this sample, only around one-quarter remained in the family home for the duration of their pregnancy (see Table B2). Almost three-quarters of survey respondents indicated that both their parents were aware of the pregnancy. Where only one parent knew, it was more common for the women to report that their mother - but not their father - knew about the pregnancy. Just 11% of respondents said neither of their parents had any knowledge of their pregnancy.
Over a third of participants spent their pregnancy residing in a maternity home run by a church or charity (see Table B2). A small proportion of mothers (16%) were living independently (working either as domestics for board, or living by themselves as they were gainfully employed). The remainder lived with relatives, friends or the father, or in hostels associated with the hospital, other types of institutions or group houses, or with family friends.
Unmarried mothers homes
I didn't see the other girls for very much interaction. I don't know what I did very much during the day - I was left in a room in the convent and stared out the window most of the time (Mother, NSW)
Focus group participants' experiences of unmarried mothers homes varied; however, the majority of women who had stayed in these homes informed us that they were treated poorly. They viewed this period of time as being a largely negative experience that subsequently affected their view of themselves and their belief in their capacity and right to raise their own children.
A range of factors contributing to this viewpoint are summarised below, illustrated with comments provided by mothers in their responses to open-ended questions in the survey:
- The stigma and shame of their pregnancies:
I was only 17 and society did not accept unwed mothers. (1666, 2012)
I was told, being unmarried, I wasn't fit to be a mother. (1846, 2012)
I was a teenager who felt guilty, ashamed, unsupported and therefore, incapable. (146, 2012)
Shame in my family - religious stigma. (187, 2011)
My father did not want to tell his family. (313, 2012)
Because I was unmarried, it would be awkward to return home carrying such a stigma. (253, 2012)
- The inability to stay in their family home and instead being "sent away":
I was incarcerated into an unmarried mothers home. (187, 2011)
I was sent interstate so as not to disgrace good Catholic relatives. (1835, 2012)
My father registered me at the home while I was 20 years old and still living under his roof. He refused permission for me to marry. (1854, 2012)
- Family rejection, both overtly and covertly:
Parents decided - family shame. (335, 2011)
Parents didn't want someone else's child in their house. (147, 2011)
My family would not allow me to keep my baby. (173, 2012)
I felt I could not shame my mother by asking to keep my baby. (71, 2012)
Catholic parents who were unable to support me because of stigma and shame. (1183, 2012)
- Being isolated from their families, friends and the father of their child, with no visiting rights granted for the duration of their stay:
I wasn't allowed to have visitors apart from my mother and father … They would put us in this little room where we had to sit. And we would sit there and it was pretty horrendous - the shaming. (Mother, NSW)
Being locked up in an institution with no choice, no support, and treated like I was nothing. (739, 2012)
There were accounts of being unable to leave the homes at all unless it was to attend hospital or social work appointments. Mothers frequently described the treatment they received from staff as "cruel" and "judgemental". Attitudes towards the women reflected and sometimes accentuated or became the vehicle for the broader societal view of unmarried mothers, which resulted in feelings of shame, guilt and an unworthiness to raise their child. Certain establishments required residents to undertake manual work tasks such as laundry and cleaning duties right up until the birth of their child:
I was made to work full-time at the hospital for 5 months - in the laundry lifting heavy loads, in the linen repairs, in the kitchens as kitchen hand, and the serveries plating meals for patients. Sometimes on split shifts you would start by 7 am and finish after 7 pm; so exhausted, I had to go up the stairs to bed crawling. I expected I would be paid for this and it might have helped when my baby was born, but I was never paid and my baby was taken … The food and lodging provided was poor and no clothes were provided, despite the need for maternity garments, which I had two of, discarded by others and in poor condition. It was slave labour virtually. We were seen as "sluts" or "fallen women" in need of some redemption. (381, 2012)
At the home we had to work very hard for our keep. We were treated as if we were in gaol. We were constantly told how selfish and bad we were to think about keeping our babies when there were wonderful parents, waiting to adopt them. (1837, 2012)
There was often the requirement to meet with social workers, who consistently applied pressure on the women to accept that the placement of their child for adoption was their only option:
Constant reinforcement by the social worker that it would be wrong for me to keep my baby; that it was best for her - she needed two parents. (1853, 2012)
Told by social worker I had no financial aid and I could not raise a baby. (1145, 2012)
The social worker told me that the baby would be better off with someone who could take care of it better than I could. (352, 2011)
Little - if any - access to information was provided regarding what to expect throughout their pregnancies or the birthing process itself:
And when the child was born, we weren't prepared for anything that was going to happen. You know, you got these pains and you sort of knew you were having a baby. (Mother, Brisbane)
Conversely, a small proportion of study participants regarded the homes as a place of protection from a society that would not accept them; that, in fact, these establishments were the best places for them to be during their pregnancies as they provided a level of comfort through enabling them to be removed from the societal and familial judgements of their situation (i.e., unmarried and pregnant).
Some participants told us that they had relative freedom to leave the premises and receive visitors, and they reflected on the time spent with other residents as being quite positive, as they were able to forge supportive friendships:
My parents sent me there to protect me. I was glad to have the sanctuary and protection of the home. We were treated with respect and dignity and I was able to form good relationships with the other young women. (Mother, ACT)
Another mother described her experience with the staff:
Some staff were really nice. I was allowed to go into the chapel and play the organ, which gave me some solitude and solace. (Mother, NSW)
Remaining in the family home
Those who remained in the family home experienced different challenges to those who were sent to maternity homes or to stay with relatives. However, this group also felt high levels of secrecy and shame, and consequent effects, particularly on their emotional and psychological wellbeing.
Focus group participants spoke of how the belief that they were not good enough and not deserving of the right to parent their own child was reinforced in their own minds during this time. The message that they received from their families was that they were an embarrassment; they were bringing shame on the family, and were regarded as "fallen women" or "damaged goods". Frequent accounts were received of the women essentially being hidden from the community for the duration of their pregnancies, and it was not uncommon for them to be made to hide away (e.g., in their bedrooms, or a cupboard) when visitors came to the family home:
I was kept at home, but had to hide if visitors came. I had to stay inside. Neighbours, nobody was to know that I was pregnant. (Mother, Tasmania)
I was hidden away. If any visitors came to the house I would go into my bedroom, and if someone was going to say hello to me, I was in bed. (Mother, Victoria)
I had to hide in the cupboard if someone came to the door. (Mother, Victoria)
5.3 The time of birth
At the time they gave birth, the average age for the mothers who responded to the survey was 19 years. Almost half of the respondents (48%) were 18 years of age or under (see Table B2). The almost equal proportion of respondents who were aged 19 years and over is an interesting finding in the context of the broader societal assumptions that these women were "teenage mothers", and will be discussed in further detail later in the discussion.
Hospitals were the most common place for survey participants to give birth (89%), with most of the remaining births taking place in a maternity home (8%) (see Table B1). The accounts relating to the treatment received by mothers in this study in the hospitals were often concerning, and we examine some of these experiences in detail in the following sections.
Note: The following accounts contain information that may cause distress to the reader. We advise that those who have been affected by past adoptions or are sensitive to trauma issues may wish to avoid reading them, or ensure that appropriate support is available.
Mistreatment in hospitals
We were labelled as a group called "unmarried mothers". A system was put in place at the hospitals where the married mothers went to the right and were treated with respect, care and nurturing as they prepared for the birth of their child. They were seen by the gynaecologist regularly, they attended prenatal classes, and were shown how to change a nappy, breastfeed, and how to care for their child after it was born. They received all of the other rights and privileges afforded to the "mother-to-be" that we were denied. The unmarried mothers went to the left in the hospitals and were ushered into the social workers office, where they were asked all about their family life. And if there was a hint of a problem with that life, the girls were labelled as social deviants. Severe judgement was handed down. (Mother, NSW)
Overwhelmingly, study participants had negative views concerning their experiences of hospital policies and treatment from individual staff during their labour and in the postnatal period. Both survey and qualitative data provide detailed accounts of cruel and often negligent treatment of many of the mothers who participated in this study. Reports of positive and caring treatment by medical staff were an exception. The Senate Inquiry's (2012) findings reported similar accounts.
Survey respondents were asked whether they felt they had been treated with the same level of care as other mothers giving birth at the same place. Three-quarters of the participants indicated that this had not been the case, and in fact, they felt they had been actively treated with less care because of their marital status, age and social/economic status (Table 5.1).18
| Not at all | A little | Moderately | Mostly | Completely | Missing | No. of observations | |
|---|---|---|---|---|---|---|---|
| Marital status | 2 | 4 | 19 | 47 | 278 | 16 | 366 |
| Age | 41 | 28 | 37 | 61 | 140 | 59 | 366 |
| Social and economic status | 74 | 29 | 25 | 45 | 107 | 86 | 366 |
| Religion | 179 | 19 | 12 | 10 | 21 | 125 | 366 |
| Race/ethnicity | 208 | 4 | 6 | 4 | 12 | 132 | 366 |
| Other | 77 | 3 | 8 | 8 | 45 | 225 | 366 |
Note: Only includes mothers who thought they had been treated with less care than other mothers (n = 366).
I was mutilated by the doctor who stitched the birth tearing. I had stitches designed to increase discomfort. At my request, a nurse removed them. The consultant examined me internally with students - perhaps to teach them how to deter unwed mums. (1540, 2012)
The actual birth was very difficult and I still have some physical problems. I can't help thinking this may have been due to deliberately poor health care. (1097, 2012)
I have gone through my life feeling guilty about my daughter being given up to adoption … If only I was able to have more support instead of being forced … From the time my hands were shackled to the bed to stop me from touching my baby's head while she was being born, and pillows and sheets being put over my face until I was in a drug-enforced sleep to stop me from being a nuisance … Then the memory of waking up in a ward with three other young girls, … all in the same position as me … That room had baby weighing scales in there … The nurses brought babies in there to weigh them … We would all sit up and try and see the babies … We were all told not to bother because the babies weren't ours … I will never ever forget that!!! I couldn't understand why we were in that room … How could another human being be so cruel to another … Such painful memories. (49, 2011)
I will never ever forget being placed in a home in 1966, aged 14, and giving birth at 15. I will never forget how horrific it was to give birth. I was told to shut up and get on with what I was in there for. I was hit by a nurse and told that's what I deserved for playing around. "I bet you think twice next time." Then given a knock-out drug when they took him away. Also being made to breastfeed someone else's baby while I was in the hospital, as some other mothers couldn't feed their babies. As a result of that I couldn't bring myself to breastfeed any of my three children in my marriage. I remember all my check-ups at the hospital, taking a number, having urine, blood and many internal examinations, each time by young interns. Very painful, very intrusive. No privacy. (944, 2012)
Similarly, some mothers recounted experiencing verbally or emotionally abusive behaviour at the time of, or subsequent to, the birth of their babies:
The hospital experience was horrendous, resulting in post-traumatic stress disorder. Because of the fact of being denied the baby, not being given any information about her sex or anything like that … I think it took me three days to find out I'd had a girl. I think if you can try and imagine what that's like. I was put in a ward with mothers and their babies - so everybody else had a baby and I had nothing. And I consider that part of the punishment … The whole hospital experience - I was nothing and no one. I literally think I ceased to exist after I had the baby, because the baby was earmarked for this deserving married couple. (Mother, Tasmania)
To have been treated like an outcast and placed in a maternity ward with seven other new mothers, and have my curtains drawn so I could not be seen by visitors. To be used by medical trainees to prod and poke my private area for their experience and curiosity. Was told I had to cope with hearing other newborn babies cry. (299, 2011)
I told the nun I was scared. Then being told, "Well you should have thought about that nine months ago". I had my child. I had the full sheets up. I heard him crying and he was whipped across the room and off he went. I was taken back to the staging room, where I was left 'til about 10 o'clock in the morning when they remembered that I was there. Then they moved me from there across the main part of the hospital, where I was stuck in a two-bed room with a dying nun. So I had a whole stream of her friends - and them telling me to stop crying. (Mother, WA)
Administration of drugs
Use of drugs prior to, during and post-labour was reported by 63% of survey participants who responded to this question (n = 487) (see Table B3). Almost half of those mothers reported that the types of drugs used affected their capacity to make decisions about their son or daughter, although a similarly large portion (45%) did not believe that the drugs used had this effect. Twenty-nine per cent of mothers who said that they had been administered some form of drug, were unaware what type of drug this was. Eight per cent indicated that they had suffered memory loss or were rendered unconscious as a result of the drugs administered to them, and almost one-third of respondents reported that they had experienced ongoing health effects from the use of the drugs administered at this time. The Senate Inquiry's (2012) findings reported similar accounts.
The most common types of drugs mothers reported being administered were milk suppressants, such as Stilboestrol, barbiturates/sedatives, opioid analgesics, nitrous oxide ("happy gas"), general pain relievers and benzodiazepines. Around 5% also indicated they had been given anti-psychotic drugs.
The nursing staff through the labour and delivery were awful. I am sure that I was drugged because I can remember one of the nurses saying, "Stop all that noise because you are upsetting all the other ladies", and I don't remember making the noise. When she was born, somebody screamed out that I wasn't allowed to see the baby, a mask was plucked on my face, and you were gone. (Mother, Tasmania)
The significance of such incidents for many women in this study was what actually drove them to go back and seek documentation about their time in hospital. The lasting effects were so serious that they wanted to see their records in order to confirm their recollections of the treatment to which they had been subjected.
According to my hospital notes, I was loaded up with enough sleeping tablets to knock out a horse. Plus, a whole lot of other things prior to delivery, including antipsychotics. You tell me, why give me antipsychotics half an hour before delivery? (Mother, WA)
One mother described the lack of use of any drugs to assist with the labour pain:
No drugs were administered. I was left for hours on my own during the last stage of labour and a gas mask was put over my face. I screamed for someone to help me. I was told to stop pushing because [the nurse] didn't want to clean up my mess. (1540, 2012)
Contact with the child
Most respondents (over 70%) stated that their child had been separated from them immediately or within a very short time of the birth. Fewer than 20% were separated within the first week of the birth, and a small proportion of participants said they were either not separated for up to a month or that they had their child with them for over a month (fewer than 10% combined).
Mothers were asked whether or not they had been given the opportunity to see their child after giving birth, and over half of those who responded to this question (n = 487) said that they had not (57%) (see Table B7).
When asked whether or not they had been encouraged to spend any time with their child at the time of the birth, almost two-thirds of women (61%) who responded to this question stated that they had been actively prevented from having any contact with their son or daughter (see Table B7). Just over one-third of respondents (34%) said that they had been advised against having any contact with their son or daughter, and only very few (4%) said that they had actually been encouraged to have contact. A small portion of the study participants (11%) indicated that it had been entirely their decision whether or not to have contact with their son or daughter.19
Those mothers who had had contact with their son or daughter at some point after the birth (n = 209) were asked to describe the nature of this contact (see Table B8). Just over half of these mothers had been able to hold their child (52%) and 21% had been able to feed their child. Fewer women had been able to either nurse or bathe their babies (14% and 9% respectively).
Mothers were also asked whether they had been encouraged to name their son/daughter at the time of the birth (see Table B7). Of the 203 women who responded to this question, just over half said that they had been encouraged to do this; however, they did not always know whether these details had been included on the original birth certificates.
Truth of information
Years later I found out more of the truth: I was lied to, cheated, betrayed, belittled and berated by my parents and church. I was led to believe that I was damaged goods - don't ever tell anyone or you will never find a husband. The secrecy was deadly. (277, 2011)
Many women responding to our survey had been given information or told things about their child at the time of the birth that they later found out to be untrue. The Senate Committee's findings reported similar accounts.
Survey respondents were presented with a series of scenarios in the survey, and were asked to indicate whether they had been given this information, and whether they later discovered this information to be untrue. For example, over one-quarter of mothers had been told their child had already been placed with a new family, and of these mothers, more than two-thirds later found out this was in fact untrue. (This issue will be discussed in more detail later in this chapter, as it relates to obtaining consent.)
My child was stolen from me at birth and I was denied access and information as to her whereabouts or details about her. I was told my baby was gone. I have little recollection of my stay in hospital or even going home. I believed my baby was no longer at the hospital and that they were allowed to take her. And I was made to believe that I was worthless and I deserved to be punished. I believed that I had no rights - indeed, I did not know what rights were. I was just sixteen and a student. My parents were prevented from visiting me and were told I was sedated. It was standard practice to keep family members out of the hospital. (97, 2011)
Similarly, 24% said that they had been told that they were medically or emotionally unfit to make decisions about their child, and more than two-thirds of these mothers later found this to be untrue (see Table B5). Almost half (48%) of the mothers indicated they had been told something else (unspecified) that led them to believe they could not decide their child's future, and 81% of these later found this information to be untrue. Comments provided in the "other" option in the survey indicate that many were referring to being told (or not being told) about any financial assistance that may have been available to them. For example:
I learned some time later (years) that there was some payment available. If there was social support available also, and with a payment, I could've left home … perhaps. (219, 2011)
The last few months of my pregnancy I applied for unemployment benefit. It came to $3 a week. I was never told that I could receive anything after the baby was born. I was made to feel I was cheating the system receiving anything, as obviously I couldn't work as I was pregnant. (321, 2011)
5.4 Main reasons child was adopted
Our treatment as unmarried mothers was not just about social expectations of "these girls", nor was it about applying mild social pressure that is not strictly enforced or put into law. This was about breaking the law, kidnapping babies at birth, drugging young, defenceless girls during and after labour - a premeditated designed system to coerce a young, impressionable person that they were unfit to be a mother during their pregnancy. The visit to the hospital during pregnancy and the conversations with the social workers at the hospitals was designed to convince the girl that the baby she was carrying was not hers. She had no right to it, she was not fit to be a mother and she was asked repeatedly to sign adoption papers before her child was born. (Mother, Brisbane)
Prior knowledge of child being placed for adoption
Consistently, mothers spoke of having no prior knowledge or awareness during their pregnancies that their son or daughter would be placed for adoption. Many talked about how they planned or very much wanted to keep their child. Based on survey responses relating to reasons their child was placed for adoption, a very small number stated that this decision was their own (around 5%).
I knew that I could not care for her in the way in which I felt she deserved. I was very young and had no financial capacity, let alone all of the rest that goes along with bringing up a child. (15, 2011)
Many respondents had been in a stable relationship with the father of their child at the time of pregnancy, and planned to marry him in the future. They had made purchases in preparation for the baby's arrival, such as cots and clothing. Placing their child for adoption had not been an option in their minds:
I had made full arrangements to keep him. I had clothes, cot, pram, high chair, bath, bottles and a bassinette for car travel. (1296, 2012)
My boyfriend [the baby's father] and I discussed getting him back, but we believed it was too late because at Carramar we were always told we only had one month to change our minds. We were both very upset. (1186, 2012)
Both her father and I would have loved to have had the opportunity to love and raise our daughter. He has never had another child. (658, 2012)
When I was leaving, I had made a layette for my child. I was leaving there and went into the office to sign what I had to sign and leave there with my baby. And the baby? Two other people came in and took this baby. (Mother, WA)
Some mothers provided accounts regarding their discovery that their children's birth records showed that they were "marked for adoption", without their knowledge, on admission to the unmarried mothers homes and/or the hospitals where they gave birth. As discussed by the Senate Inquiry (2012) in their final report, "BFA" was the commonly used code marked on the women's files that indicated that their child was a "Baby for Adoption".
File marked BFA and then hospital protocol commenced. (1193, 2012)
I told the social worker that my father and I decided to keep my baby. She said that the baby already had parents waiting. This was four months before the birth. (139, 2011).
The adoption was arranged very early in the pregnancy, and I was then told that it would be unfair to disappoint the prospective adopters. (2041, 2011)
It was more common for study participants to have retrospectively discovered information about their baby being marked for adoption once they had obtained their medical and/or institutional records than for them to have realised this at the time. One mother told us of such an experience after receiving her records in 2009:
And when I got those, I realised that my baby had been marked for adoption one day after I got there. I went there on the 2nd of April and I had my baby on the 29th of September. Some black market kidnapper marked my son for adoption the day after I got there [the unmarried mothers home]. (Mother, NSW)
Some mothers also described how the fact that the baby had been identified for adoption was marked above their beds in the hospital. As they often shared the same ward as married mothers, this added to their sense of shame, as it was not only visible to staff, but to all visitors. One adoptee told us about her own mother's experience of this:
Up above her head was a sign that said, "giving up for adoption", so everyone knew. (Adoptee, NSW)
Based on survey responses and information obtained during focus group discussions, the majority of mothers participating in our study said that at the time of their pregnancy, they had not wanted their son or daughter to be placed for adoption. There were a number of consistent factors contributing to adoption being the eventual outcome (as discussed below), despite it not being the mother's intention. A minority described a fully informed and consensual decision for their child to be adopted, but this was certainly an overall exception to the broader experience of participants.
Two-thirds of mothers in this study said that they had wanted to keep their son or daughter and one-quarter of the sample said that they had been uncertain (see Table B10). Only a small proportion said that they had wanted to place their child for adoption. Almost three-quarters of all respondents believed that if they had had sufficient financial and other support at the time of their pregnancy, they could have kept their baby; however, other respondents (17%) said that they were uncertain as to whether these kinds of support would have made any difference in their decision to place their child for adoption (see Table B10).
Three main reasons for child's adoption
I had nothing to offer her but myself, but [I was told] that was not enough. (1228, 2012)
Survey participants were asked to list the three main reasons for their son or daughter being adopted. Mothers provided 1,373 responses across the three options, which were thematically analysed and grouped by frequency into sub-categories.
The most commonly identified contributing factors to their child's ultimate adoption were:
- family pressure and/or the lack of family support (22%);
- economic factors, including lack of appropriate housing (15%);
- pressure from authority figures (13%);
- the mother's age (9%);
- being an unmarried/single mother (9%); and
- believing or being told there was no other option (7%).
Some descriptive responses also included in less detail that their child had been removed without consent (6%), and a further 6% were either told or they believed that they had been unfit to raise their child. Just 5% stated that it had been their own decision to place their child for adoption, and 5% mentioned that the lack of support from the father had been the main contributing factor in the adoption of their child.
Although the issue of forcible removal did not rate highly in these short-response items, the survey did ask participants specifically to describe their adoption experience as it related to their choice in the adoption of their son/daughter. These results will be discussed later in the chapter in a stand-alone section.
Pressure from others
The pressures placed on mothers by family, social workers, members of a church (commonly Catholic) and the broader society, left many with the understanding that there was no other option than for their child to be placed with a family that was able to provide two parents and all the benefits of a financially stable environment. Respondents described how these messages had been an important contributor to their belief in their lack of capacity to keep their child. Many mothers felt that these messages were "propaganda", intended to influence their belief in themselves and their "decision".
The propaganda fed to you: "Your baby will be better off", "How can you look after a baby?" (1186, 2012)
Although there were only a small number of people who identified stigma as being a reason in itself, most responses reflected the effect of social stigma in the pressures applied by family and others who held positions of authority. For example:
I was from a small country town where my family had their business and a standing in the community. And the stigma of having a baby, not married, as a single mum, was just too much for my mother to cope with. (771, 2012)
Parental influence and lack of support
The shame of illegitimacy and being an unmarried mother was frequently reported as driving the lack of support from parents to keep their children. The family's standing in their local community and church, which would be affected by their daughter's pregnancy, was a common theme reflected by mothers in our study:
My parents had money and were horrified at the thought of an illegitimate child. (1291, 2012)
Catholic parents who were unavailable to support me because of stigma and shame. (1183, 2012)
Family sense of shame and fear of rejection if I kept my baby. (200, 2011)
Forced by parents. I was told to adopt my baby and get on with my life. (1774, 2012)
My parents had decided, against my wishes. (121, 2012)
My mother told me that I had to adopt the baby to someone else who could really care for the baby and provide her with what she needed in life. (658, 2012)
Many mothers reported that their parents also expressed opinions to them that a child would be better off in the long-term if it were raised by a married couple:
I was raised to believe it was the right thing to do [place the child with a married couple]. I didn't have a choice presented. (411, 2012)
I was told that I could not provide for the child as well as the family that would like to adopt him. (1729, 2012)
Other factors contributing to a lack of support from the families included the financial stress that they were already under. Some mothers felt that their family may have been supportive of their daughter keeping their child, but they were not in a position financially to do so. However, it was not always clear that this message was communicated explicitly, or rather that the financial circumstances of the family was well known to the young woman, who then felt that the additional burden of her pregnancy and raising a child would just not be possible:
My parents didn't have any money to help me if I had kept the baby. (930, 2012)
Both sets of parents claimed they could not afford to help assist us to stay together as a family. (1860, 2012)
Unfair to expect parents to raise another child as I would have to go back to work. (1457, 2012)
My parents were poor, working class, so could not support me financially. (1766, 2012)
Some participants described their home environments as being inappropriate for bringing up a child because of existing parental abuse, alcoholism, mental health issues or overcrowding:
As I was part of a large sibling group, with extended family also living in the house, it was thought that a baby would be too unsettling in the home. (21, 2011)
My father refused to have the child in the house. My mother was ill and he was an alcoholic and believed I should have married the father of the child. (1205, 2012)
To prevent him from the abuse I experienced as a child growing up. (219, 2011)
My mother was an alcoholic. (1473, 2012)
Authority figures
The majority of mothers who participated in this study believed that the messages they received from those who were in positions of authority were an attempt to convince them that they had no other option than to place their child for adoption. These communications had been delivered at times of extreme vulnerability. Continued reinforcement of negative messages (e.g., that they were not worthy, capable, or deserving of raising their own child) was one of the issues the mothers discussed most frequently, both within the survey responses and during the focus groups and interviews. Many also said that they had not been presented with any other choice/option for keeping their child:
Absolutely pressured by authorities on an emotionally weakened, frightened 17-year-old girl. (1857, 2012)
No other option given. (34, 2011)
No one would help me keep him. I had a government job, was over 21, but had no support from any suitable family members. (78, 2011)
Coercion by social workers, family. And the general belief that it was the best thing for my child. (239, 2011)
I was convinced I had no other option. (256, 2011)
Many felt that they had been in a "no-win" situation regarding their ultimate decision to raise their children. They had been told that if they chose to keep the child they were being selfish, doing their child a disservice and not giving him/her the best opportunity in life. In addition, they had to face the reality of being stigmatised for being a single mother and their child having the title of "bastard":20
Told over and over by nuns that the only option was two parents. Anything else was selfish. And also told over and over he would be a "bastard". (993, 2012).
I was told that if I loved my baby, I would give it to a married couple who would be able to give him everything that I could not. (71, 2012)
I was told the only way to remove the stigma of "bastard" was allow a married mother and father to raise him. (1819, 2012)
It was expected and assumed automatically by the people I'd approached for help. (439, 2012)
This account provided by a mother in a letter to project staff, is representative of the majority of survey responses, highlighting the way in which mothers were either implicitly or explicitly told they weren't as worthy or capable as a deserving married couple:
We were told that we could not possibly look after a baby all on our own. I was asked if I wanted the best life for my baby and naturally said, "Yes". Then I was asked how I was going to manage, where I would live, who would give me money and I said, "I don't know". I was then told that I was selfish thinking that I could look after my baby, and I was asked to sign the adoption consent so that a "happily married couple, who could offer my baby everything I could not offer him, could look after him". On another day I was told that I could have a child of my own. I did not see a doctor or nurse on these visits and I left depressed and crying. (Mother, NSW)
The frequency of responses in this vein is indicative of the shared experiences by so many who completed the survey:
I was told I didn't love her if I kept her. (1228,2012)
Told it would be harmful to her if I kept her. (1482, 2012)
I was not consulted, but told. (1568, 2012)
Believing: "If you really love your baby, you will give it to a 'real' family". [I was] being told this constantly awaiting labour. (1820, 2012)
Constant reinforcement by social worker that it would be wrong for me to keep my baby; that it was best for her. She needed two parents and I couldn't provide for her. (1853, 2012)
I was told there was no alternative - the professionals told me this. (1857, 2012)
I was told no one would marry me with an illegitimate child. (78, 2011)
Another man would not want me with a child. (147, 2011)
Told I would hate the baby and I was to get back and finish my nurse training. (1194, 2012)
I was told that I had to make up for what I had done; i.e., getting pregnant. (241, 2011)
I was told I had already harmed him enough and if I really loved him, I would give him up. (470, 2012)
Church said it was shameful. (739, 2012)
Social worker advised me that my child would reject me later in life as I wasn't married. (1082, 2012)
Focus group discussions were largely consistent with the survey responses, emphasising the negative messages that these pregnant girls and young women received about themselves, their rights, and their capacity to parent a child:
I was told by the doctor, "You will have other babies. Just get on with your life and forget about it". And I was told things like, "A baby needs two parents, what right do you have to keep your baby?" (Mother, Tasmania)
I had a lot of comments from staff, which I understand now, but didn't understand then. I believed everything they told me then - I was a naïve 18-year-old. I got lots of comments from staff like, "What can you give the baby? How can you look after the baby? No one is going to want to marry you. If you love your baby, you will adopt it". All of these things which I now understand are coercion under duress. And I walked away from all that understanding that I was a very, very bad person. And I was totally ashamed and guilt-ridden. (Mother, Tasmania)
Other methods of pressure were applied, in the form of threatening either to involve welfare authorities or the police if they did not sign a form consenting to the adoption:
Told by welfare she would grow up in an orphanage if I didn't sign the papers. (45, 2012)
I was told I was too young to legally make a decision to keep him. (489, 2012)
The police told me in the hospital ward that I was not allowed to keep my child as I was underage. (1360, 2012)
Once I was put in the home, I told the matron I was leaving to live with my gran and marry. She threatened me with police and welfare. (1854, 2012)
Told my son would be put in a home if I didn't sign the consent. (151, 2011)
Economic pressures
For many women who participated in the study, the lack of financial support or knowledge of what financial benefits might have been available to them were significant factors in the reasons for their child being adopted. This was the second most common reason provided for the ultimate adoption of their child.
Not emotionally or financially ready for children. (548, 2012)
I had no income. (119, 2011)
I had no means of support. (285, 2012)
Financial - I had no way of supporting him and was unaware of financial assistance. (1082, 2012)
Not being told that there was any support available to me at the time. (496, 2012)
They didn't tell me how I could get a pension. (1293, 2012)
Sometimes it was not so much their own view of their economic circumstances and capacity to adequately care for their child, but the external perspective of their families and other authority figures (such as social workers and nursing and maternity home staff) that mothers reported as being a significant influence on their decision:
I was told by the matron of the home that financially I could not look after myself, so I was not capable of handling the situation. (1185, 2012)
I was told by the social worker I had no financial aid and I could not raise a baby. (1145, 2012)
I was told there would be no support from the government. (1181, 2012)
I was told I had no choice with any assistance being available to me from any government department. (1079, 2012)
Many participants expressed their frustration, shock and anger to have learned retrospectively that financial assistance may have been available to them at the time of their child's birth; however, they reported that this information was either not made known to them, or was actively disputed as an option:
I was lied to - told there was no government assistance and that welfare would just take him if I didn't sign. This was lies. In 1975, the Supporting Mother's Benefit was available. Who deemed that I was not worthy of assistance? (1233, 2012)
Angry at the lack of information regarding welfare payments, housing etc. that was available at the time but was never passed on to me. (1266, 2012)
I was very angry at various stages because I had a nice, successful career there, and before long, it was apparent to me that I could have afforded to keep her. And that really pissed me off - that I gave her up. Because I could have made a life for us. And it wouldn't have been a deprived life, it would have been a good life. (Mother, Qld)
Mother's age
As previously mentioned, the most common age for survey respondents at the time of the birth of their baby was 19 years (see Table B2). In addition, almost one-third of the participants were aged 20 years and above, which, in the context of this discussion, is a somewhat interesting finding, given common societal references to "teenage mothers" and the presumption that young, single mothers were incapable of raising a child (e.g., see Swain & Howe, 1995).
Where mothers' responses to the open-ended question about the respondents' main reasons for the adoption related to age, they can be summarised into three key themes:
- the mother's own perception of her capacity to parent;
- the societal view of her capacity to parent; and
- the families' view of her capacity to parent.
Mothers' own perception of capacity to parent
Some mothers held the view that they were too young to be able to raise their child, due to a number or factors. For example, some felt that they were not old enough to do it alone and did not have the maturity to raise a child given their own age:
I was too young to rear a child. (349, 2011)
I was too young to care for him. (657, 2012)
I was too young to bring up a child on my own. (384, 2012)
I believed I was too young to cope with the responsibilities of raising a child as a single mum. (771, 2012)
Didn't believe I was a good mother because I was young and unmarried. (809, 2012)
Societal views of mothers' capacity to parent
Where mothers simply stated their ages - such as "I was 16", "I was 17", or "I was still in school" - these results are a possible indication of the societal view of what you were supposed to do if you were young, unmarried and pregnant;21 it was an assumed course of action:
I was only 17 and society did not accept unwed mothers. (1666, 2012)
We were considered too young to know our own minds. (1860, 2012)
It was automatic … 17 years old and unmarried. (405, 2011)
Too young. Didn't have a choice. (1293, 2012)
I was told I was too young. (167, 2011)
I was underage and not permitted to make decisions. (146, 2012)
I was told I was too young to keep my son. (489,2012)
Too young to assert own wishes. (937, 2012)
I was made to believe I was too young. (1804, 2012)
I was told I was too young legally to make a decision to keep him. (489, 2012)
Families' views on mothers' capacity to parent
Although parental pressure/influence has been discussed earlier in this chapter, many survey respondents provided more specific detail in relation to the significance their age had in their parents' attitudes toward their capacity to keep their child and be an effective parent:
Too young. It was my parents' decision. (204, 2012)
I was told I was too young and incapable of raising a child. (1285, 2012)
I was only 16 years old. My mother would not have me with the child. No other options given. (1779, 2012)
Nuns and some family members said I was too young. (1143, 2012)
Family and environment all pressured that I was too young. (1823, 2012)
Social stigma
The broader societal judgement of unmarried mothers that has already been examined in detail throughout this chapter (and see Higgins, 2010; Swain & Howe, 1995) commonly featured as one of the main reasons identified by participants as contributing to the placement of their child for adoption. This was exemplified by the belief that adoption was their only option, and that many participants subscribed to the messages that they were unfit to be mothers:
The stigma of being an unmarried mother. (910, 2012)
It was socially unacceptable for an unmarried person to have a child - so I got told from day 1. (1266, 2012)
I just knew that that was what happened if you were pregnant and not married. (71, 2012)
It wasn't even something I considered - believed that was the only alternative as I was an unmarried mother. It was just what you did in those days. (1313, 2012)
I wanted to do the right thing by my son, even though I knew it wasn't the right thing for me. (613, 2012)
It was what you did! (1836, 2012)
I thought that it was the thing I had to do to give her the best life. (1530, 2012)
Own choice
Notwithstanding the external pressures (both overt and covert), a small proportion of survey participants (just 5%) said that it was entirely their own decision to place their child for adoption and they felt it was the best course of action for them at the time. However, one mother reflected on the difficulty she had in making the decision to keep or adopt her child:
I didn't know if I would love him or resent him. (1890, 2012)
For some, they felt that they were not ready or mature enough to become a parent; others wanted to focus on their studies and career:
I needed to grow up, leave home, work and become a good teacher before settling down to marriage/children. (1159, 2012)
I was doing my nursing training. (816, 2012)
Education not completed. (1692, 2012)
I wasn't ready emotionally. (780, 2012)
I had no idea how to care for a child. I was still a child myself. (1262, 2012)
I wanted the best for my baby. I felt I could not do that. (1102, 2012)
The importance of their child growing up with two parents was significant in their decision to place their child for adoption for some mothers, who believed that adoption was the best thing for their son or daughter:
I wanted my child to have a father. (56, 2012)
I wanted my baby to have a mother and a father. (1184, 2012)
I believed a family could give my son a better life. (295, 2012)
I realised it was the only way my child could have a good upbringing and education. I was very strong on who I would see as appropriate parents. (448, 2012)
I wanted a better life for my baby than what I could provide as a single mother. (1184, 2012)
I wanted to give my daughter the best opportunities for her life going forward. (1327, 2012)
No support from father of child
Despite the likely viewpoint that would have been held by many at the time, that the fathers "abandoned" the mothers once they became aware of the pregnancy, just 5% of mothers said that this was a contributing factor to their child's ultimate adoption. However, for those mothers who did indicate that there was lack of support from the father of their child, the main explanation was that he had ended the relationship upon discovery of the pregnancy (almost half):
Because my boyfriend had abandoned me. (1040, 2012)
Father would not support me emotionally or financially. (1540, 2012)
No support from father. (1170, 2012)
For others, the relationship had ended prior to the discovery of the pregnancy and the mothers did not want to resume that relationship, or there was pressure applied from the father's family for the child to be placed for adoption:
Son's family insisted. (267, 2011)
Relationship had ended. (142, 2012)
I had split from the father and did not want to resume the relationship. (695, 2012)
For some mothers who stated lack of support from the father of their child as one of the three main reasons for the adoption, the fathers were in fact already married and therefore the scenario of a continuing relationship with the mothers that involved raising a child was not a possibility:
Married man and he was my boss. (1841, 2012)
Forced removal
I never actually said that I wanted to adopt my baby, but it was like you were on a train that had one stop, and the only stop was adoption. That was where the train was going to stop and that was what was going to happen to you. (Mother, Tasmania)
Overt force and coercion was identified as a reason in and of itself by around 5% of mothers in this question as the main reason their child was ultimately adopted; however, the other accounts of pressure, stigma and lack of support (both financial and emotional) were also identified as being forms of coercion and force - just more covert:
Traumatised from baby being taken at birth. Physically, mentally, emotionally overpowered and overwhelmed. Drugged, then shamed into silence, parents prevented from visiting. (97, 2012)
She was taken from a receiving home I had placed her in while I was recovering from mastitis. (51, 2011)
I didn't adopt my daughter - everyone else did. (405, 2011)
Forced signing of papers, and [they] covered sections. (413, 2011)
I was told I couldn't change my mind after I woke up after the birth, when I asked to see my baby and they told me I had previously signed the form to give him up. They said I couldn't be discharged from hospital unless I signed a release form. (271, 2012)
Theft. Stolen at birth. (305, 2012)
I was stood over by the matron and told I must sign a paper that I could not read due to distress and being kept in bed. And I was told to sign as I couldn't be discharged from hospital until I did. (381, 2012)
She was stolen from me. (789, 2012)
I was tricked out of custody. I was told it was permission to have tonsils out by child welfare in 1965. (846, 2012)
She was stolen from the birth table. They covered my face. (1042, 2012)
I never wanted my son adopted. I was taking him home! (1296, 2012)
Provision of consent and further details of the circumstances leading to the adoption of respondent's children will be explored in more depth in the following sections.
5.5 Adoption
Organisation of adoption
The majority of survey respondents indicated that the adoption of their son or daughter was organised through a formal institution (see Table B10). There was more than one agency involved for some study participants. Almost one-third were arranged by the hospital in which the mother gave birth and other common arrangements involved government departments (28%), a church (26%) or the maternity home where they had been living prior to the birth of their child (19%). A small number were organised through a government home for children if the mothers were wards of the state at the time of their pregnancy (4%).
Private adoptions were reported in a smaller number of cases (19%), and were arranged by either the mother's parents, a family GP, a private adoption agency or a family lawyer. Individuals were also identified as organising the adoption; however, it is unclear as to whether they were individuals acting of their own accord, or whether they were attached to a formal institution. These individuals were most commonly identified as being a social worker (19%), with a very small number of participants saying the adoption was arranged by a doctor, member of the clergy or family friend (less than 2% combined).
Fourteen per cent of mothers responding to the survey said that they were unaware of who had organised their son or daughter's adoption, and 20% said that the adoption was arranged by someone other than the options provided in the survey.
Adoption advice and information
Over half of the survey respondents (56%) said that they had not received any information regarding options that may have enabled them to keep their child, particularly any financial support available and the capacity to revoke their consent to adoption (see Table B9). A small proportion (14%) had been told that their consent must be given freely and voluntarily. Very few had been informed about the financial support that was available to them if they kept their child nor told about the possible long-term effects of their child being adopted; nor had they been asked if anyone was pressuring them into placing their child for adoption (2% each). Similarly, very few had been asked if they needed more time to think their decision through (2%).
However, 21% of respondents said that the legal effect of consenting to adopt had been explained to them and another 21% stated that they had been informed that they could revoke their consent in a given timeframe and had been provided with information as to how to do this. Given the accounts of so many of the women in this sample, however, the provision of information regarding revocation of consent may have been used as a form of coercion into convincing mothers to sign the consent form. This will be discussed in more detail in the following sections.
These survey results are consistent with the accounts of focus group participants, who overwhelmingly described not receiving any information of this nature. It was actually common throughout the course of these discussions for participants to be hearing for the first time about government benefits that may have been available to them.
Provision of consent
Nearly 22% of survey respondents said that they recalled freely and voluntarily consenting to their son or daughter's adoption and signed the documents they were given (see Table B9). However, 68% said they recalled signing something, but felt that they didn't have any other choice, and a further 18% said they recalled signing a form but had not fully understood what it was. Some believed the drugs administered to them during labour affected them at the time the process of consent was undertaken (18%), and a few could not recall whether they had signed any documents consenting to the adoption of their son or daughter (9%). However, for those who did recall signing something, the majority of anecdotal accounts indicate that they were generally not shown the paperwork, or the paperwork was partially covered when they were providing their signatures:
I had no idea about signing consent forms. I was led down a corridor. I was told to sit at the table, and there was a GP sitting behind the table and the matron was there. I started to cry and a piece of paper was pushed in front of me and I was told to sign my name. And I just sat there and sobbed and sobbed and sobbed. But nobody really cared about that because all they needed was my signature. I should have been asked if this was what I wanted to do. I had no counselling beforehand. Nobody gave me any options other than adoption. There was never a word mentioned about me keeping my baby. Why would I keep my baby? Because (a) I was a terribly bad person, and (b) there was this deserving married couple who were waiting for my baby. So I signed the forms, and again, nobody took any notice of me. (Mother, Tasmania)
The hospital broke the law when they denied me my child. The hospital broke the law when I was given no options other than adoption. The Adoption Act was contravened, because I was supposed to be given all the options to enable me to make a free and informed choice. I wasn't given that. (Mother, Tasmania)
When asked whether the opinion of the father of their son or daughter had been taken into account in the placement of their child for adoption, over half of the mothers indicated that this had not occurred, with a further 14% of survey respondents indicating that the father of the child was not aware of the pregnancy (see Table B10).
Although laws varied across the states and territories, there was consistency in the fact that consent to adopt could not be taken from a mother within a minimum timeframe after the child's birth (usually between 5 and 7 days). However, we received numerous accounts of these processes not being adhered to by those in charge of obtaining consent:
I signed the adoption papers the day after he was born. (Mother, Tasmania)
The consent - that was shocking. Mum and Dad insist they weren't in the room. That was on the morning of the 4th day. (Mother, NSW)
I left the hospital after three days, but she was taken as soon as she was born. Her adoptive mother had gone into the hospital for a week and seen her and fed her every day for a week before they took her home. It had all been set up and ready to go. (Mother, WA)
Revoking consent
Although there were variations across states and territories as to the length of time during which consent could be revoked, it was usually a 30-day period. Accounts of being informed about the 30-day revocation period were minimal. Over 40% of respondents said that they had been unaware that this was even an option available to them (see Table B9). Just over 20% of respondents indicated that they had attempted to revoke their consent to adoption and have their child returned to them; however, almost all of these attempts were unsuccessful (93%):
I since received my notes from hospital and there is clearly a note in the margin that says "mother is not to speak to anybody without parents present". So they didn't bother to speak to me at all. Except to take me into this room on day 4. "Sign this." "What is it?" "Adoption." "I am not signing it. Not unless I see my child." They brought me in the baby … I suppose it was mine. I got told, "Here is a piece of paper. 30-day revocation period, but you're underage so it doesn't apply to you". I was 15. There was a nun holding [my son], and two or three other gentlemen. Don't ask me who they were. (Mother, WA)
A very small number of survey participants indicated that their child was returned to their custody as a result of revoking their consent (n = 5); however, we were only able to meet face-to-face with one of these mothers in a focus group discussion. Her experience of this process was complex and she informed us that the pressure applied to her at this time to not go ahead with the revocation was immense.
I revoked my consent at 30 days, but I still felt like I was doing the wrong thing. It felt like the wrong thing to do because they kept trying to convince me to adopt. (Mother, NSW)
Some mothers spoke about going home and only then realising that their babies weren't going to be in their care. When they attempted to get their babies back, they were told that it was too late; that the child had already been placed with a family. For many, they later found this information to have been untrue:
They said I had 30 days to decide. They didn't give me any information on how I could actually do something about it if that happened … Then I came to Dad the day before the 30 days was up. And I said, "Dad, please can we go and get him, I want to bring him home". And Dad said, "It's too late - don't be ridiculous, it's too late. The arrangements have all been made". (Mother, NSW)
Survey responses revealed some women being threatened with welfare and/or police involvement when they returned to the hospital to retrieve their son or daughter:
I had doors locked in my face and police were called. (1144, 2012)
I was threatened by police action; that I would be incarcerated. (51, 2012)
I was told by both children's services and hospital there were no records of me having a baby. There was no paperwork and they had never heard of me, and go away or I'd be arrested for being a nuisance. I went to the police and they did nothing. (1296, 2012)
When I tried to leave the home with my baby I was told I had signed him away to new parents. And I was breaking the law and the police would be called if I tried it again. I signed under duress. I can remember crying hysterically and a voice telling me to calm down, it was for the best and that time heals all. (1837, 2012)
The following is an account of one mother's experience that reflects similar stories shared throughout the study. It provides an example of how many women felt that they were systematically "worn down" over extended periods of time, to the point where they did not have the strength to fight against those who held positions of authority. The subsequent use of the 30-day revocation period was presented as a "safe option" for the mothers for the time being, so that they would agree to sign the consent:
It was the day after my 16th birthday, and I was taken to the Salvation Army hospital. I didn't really know all the things that were going on. I actually didn't even acknowledge to myself that I could have been pregnant for a long time. So I was taken up there. I was given work to do. My baby was born. I was going to keep my baby. I loved her right at the beginning and had no intention whatsoever of not having her in my life. I had her for seven days, until my parents told the authorities up there that there was no way I was going to keep her. So that is when the social welfare people started meeting with me every day. And bullying me, telling me some pretty awful things about myself and what would become of her and I etc. And that no man in the future would want me. Some pretty horrible things. So, after that seven days, I was pretty exhausted. Then somebody told me that I would have 30 days to do something about it and get her back. So, as I said, I was pretty exhausted. So I thought, I will sign the papers and then I will go home. I will start feeling stronger, and in a week or so I will come back and get her. And I did that. But nobody would to talk to me. She was gone. (Mother, Tasmania)
There was a minority of study participants who truly believed it was the best thing to do for themselves and the child and who felt completely informed of what they were entering into. But most of them conceded that if they had received the appropriate support, they would not have made the same decision. For some, the adoption was an economic decision as opposed to an emotional one:
I think being brought up in a big family and feeling like I was neglected - I didn't want to do that to her. How was I going to get someone to look after her when I went to work? Where was I going to live? If I stayed at home then they would put the rent up because my mum would have had someone else living with her. It was just impossible. (Mother, WA)
When asked which statement best described their adoption experience, a quarter of survey participants said that their child had been stolen from them; one in five felt that they had lost their child to adoption; and 15% said that their child had been taken from them (see Table B10). Conversely, 21% said that they had given up their child for adoption and 12% said they had surrendered their child.
Even with around one-third of survey respondents describing some level of voluntary relinquishment, four out of five of all mothers who responded to the survey were either completely (67%) or mostly (13%) dissatisfied that their interests had been looked after in the adoption process (see Table B10). Only a few of the mothers had been completely satisfied/mostly satisfied with the adoption process (7%).
Receipt of birth certificates
An area of concern for many study participants was the fact that they had not had any documentation that acknowledged the birth of their son or daughter. Ninety-four per cent of survey respondents said that they had not received a copy of a birth certificate when their child was born, and many were unaware that this had even been an option or a right of theirs (see Table B10). In the majority of instances where a birth certificate had been received (49%), mothers said that the father of their child had not been named on either the birth certificate or birth registration form. Eighteen per cent said the father was named on the birth certificate only and 12% said that the father was named on the birth registration form only. Finally, 9% of mothers said that they either didn't know or couldn't remember if the father of their child was named on the birth certificate.
Some mothers told us that the reason they had not revealed the identity of the father of their child was because they had been concerned/threatened that he would be charged with carnal knowledge. The fear of police involvement was a serious issue for many of these young mothers, as sometimes their boyfriends were adults, and they were below the age of consent. The fear of criminal prosecution - and the attention this would bring to themselves, their boyfriend, and their families - was a legitimate fear, given the laws of consent in place at the time.
The desire to have their child's birth certificate was also identified as being a significant issue for mothers in this study in relation to their current needs; that having this documentation is important as it is recognises that they did in fact give birth to their child and that they are the mother of that child.
5.6 Support during pregnancy, birth and adoption
Survey participants were asked to recall their experiences of any significant issues associated with their physical and/or mental health and wellbeing during their pregnancies. A large majority of the respondents (82%) said that they had suffered significant stress/anxiety, and around two-thirds said they had suffered from depression and/or another mental health issue throughout their pregnancy. Despite this, 43% of respondents said that they had not had any supports available to them throughout the time of their pregnancy and the birth of their child (see Table B11). A very small proportion (1%) said that they had not needed any support.
The remainder of respondents identified their parents, other family members, friends and the father of their child as the most common sources of support (see Table B11). As would be expected, there was very limited professional support either available or utilised; however, a small number of respondents reported receiving support from a social worker or counsellor, a general practitioner, a registered psychologist or psychiatrist, or a support group.
Overall, most of the instances of support given were seen as being either very or somewhat helpful (70%) (Figure 5.2 and Table B12). However, in 13% of cases the "support" was viewed as being very unhelpful. This occurred more often with social workers and counsellors, and with parents.
Figure 5.2: Sources and levels of helpfulness of support given to mothers at time of birth
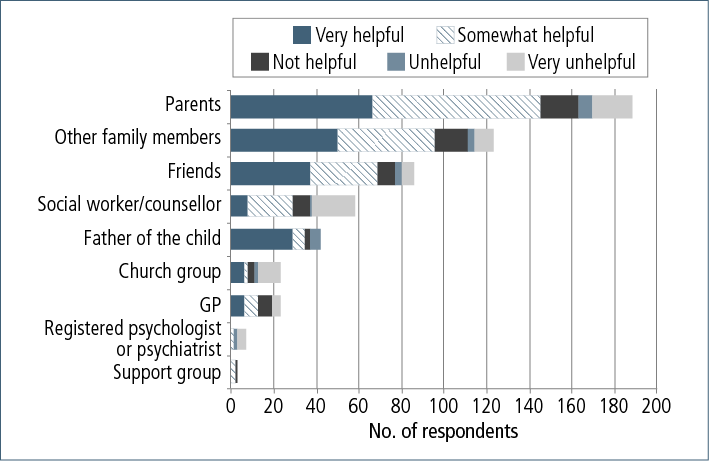
Emotional and financial support were the most common types of support received. Less common types of supports were psychotherapy or counselling, family planning advice and legal support. These various supports came from a range of different sources.
5.7 Search and contact
Although the word "reunion" is generally the standard term that is used to describe both services and the actual act of engaging with lost family members, there has been opposition to its use by many people participating in this study. As one mother who was a victim of forced separation from her child explained:
Reunion? How can you be reunited with someone you never saw in the first place? (Mother, Victoria).
Also, "reunion" implies an emotional (re-)connection, and (re-)establishment of a bond. However, after having made contact, not all parents and their sons or daughters separated by adoption continue to see each other or maintain a close relationship. Accordingly, for the purposes of this discussion, we have used the term "contact" in reference to any communication or connection between those separated from others by adoption, whether or not it has led to a "reunion" or establishment of new and positive connection between parents and their sons or daughters.
Most of the survey respondents (86%) had tried to find information about their child from whom they had been separated and, of these mothers, 88% had actively engaged in a search process (see Table B13). The majority of the survey respondents (85%) had had some form of contact with their son or daughter.
We will now examine participants' experiences of search and contact, beginning with use of services to assist in this process.
Service use
For those mothers who had tried to search for their son or daughter, the most common type of service utilised in the search and contact process was a government department (including the Registrar of Births, Deaths, and Marriages and the Electoral Commission), followed by a non-government organisation (Adoption Jigsaw in most instances) or the institution through which the adoption had been organised. Peer support groups and post-adoption resource centres had also been utilised in the search and contact process.
Mothers were less satisfied with search and contact services than other respondent groups, and felt the frustration of not being entitled to information about their son or daughter due to privacy restrictions such as contact vetoes that are in place across the jurisdictions.22 In addition, there were many impediments to obtaining information from services that were largely focused on accessing records from the time of pregnancy and birth:
Disorganised would be the better word for it. [The application for information] was declined because of the very inexperience of the social worker. (Mother, WA)
Many mothers have been told that their records no longer exist, that there are restrictions on what information can be released or that the records have been destroyed (such as in fires/floods):
I remember when I contacted [church run maternity hospital] I was told my notes didn't exist. I kept phoning up and getting more and more irate. And then I got told they legally have to keep them in [state]. Then there's an apology [from the church], and like magic, that afternoon, I got a call from medical records, and they said they had found them. (Mother, WA)
Mothers often have also had to deal with a high turnover of support workers:
In the adoption field, the turnover of workers is very high, and they are the ones that are supposed to provide the post-reunion counselling. (Mother, Victoria)
The complexities of navigating the varied state/territory government systems if they or their child were living in a different jurisdiction from where their child was born or now lived was also raised as an issue. These sorts of experiences have made some mothers reluctant to re-access search and contact services, such that they have either not continued with their search, or have had to continue the process on their own, through the use of social media and the Internet, or even the employment of private detectives, to try and find information about their child.
Satisfaction was highest with search and contact services when staff appropriately and sensitively managed the process and when the mothers were kept informed of progress regularly. However, we did not get the sense that this level of professionalism was the normal experience for mothers in this study:
I have to say, [at the agency], the only woman I spoke to there - she was fantastic. And she would ring me if nothing was happening for a few weeks. She was totally different from the people who provided the original support. And she followed up. (Mother, Qld)
Despite the high level of search and contact service utilisation by mothers in this study, much of their focus in the discussions we had with them was centred on the actual relationships they have with their son/daughter. Most of the mothers did not wish to describe in any detail their service use at the time of searching; the level of detail in describing their experiences with search and contact services was, for the most part, relatively "surface level", and related to whether or not the service was successful in locating their child or providing information that would enable them to make contact themselves. Given that over two-thirds of mothers' first contact with their son or daughter occurred prior to 2000, this lack of detail is not overly surprising.
Inhibitors to search and contact
Some of the most significant barriers to searching for and possibly making contact with their son or daughter were mothers' own fears and feelings of unworthiness; that they were not deserving of having a relationship with their son or daughter. Some women spoke of the effect that the continued secrecy and shame they carried in relation to their pregnancies and adoption of their child had on their willingness to make contact. Some of those who had carried the secret for their entire lives feared that they would suffer rejection from their partners and other children, friends and family members if they were to now find out they had given birth to a child who had subsequently been adopted.
For those who had not had any contact with their son or daughter (n = 69; 14% of all mothers), 23% stated that the reason was because their child had rejected the possibility of contact and 16% said that there was a veto in place preventing contact (see Table B13). Other common reasons were: that the mother believed it was her son or daughter's choice to have contact and she was waiting for this; that she does have some information about her son or daughter, but they have not yet met or had any communication; and that she is fearful or emotionally vulnerable about the possibility of having contact. Some said that it was simply because they have not been able to find any information about their son or daughter.
5.8 Contact
As previously mentioned, a large majority (n = 427) of mothers who responded to the survey had had some level of contact with their son or daughter (see Table B14). Of these mothers, more than half had had their first contact by the time they were in their mid-forties (see Table B14). Some, however, had to wait until they were over 65 years old before having contact.
In a similar manner, 69% of the adopted individuals had had contact by the time they reached 30 years of age, while a small number (7%) were aged over 50 years before they first had contact (see Table B14).
When asked to describe the type of contact they had with their son or daughter from whom they were separated, almost two-thirds of mothers said they had an ongoing relationship (64%); however, one-quarter of mothers said that although they had met their son or daughter, they did not have an ongoing relationship (see Table B13). A much smaller proportion of respondents said that they had had some form of contact with their son or daughter, but had never met face-to-face (6%).
We also wanted to gain a sense of how making initial contact, or establishing a relationship with their son or daughter had affected the mothers' relationships with others in their lives. According to mothers, their subsequent children, spouses and other family members had mostly experienced positive effects from the contact that they had made with their son or daughter that was adopted (see Table B15). Negative effects were, for the most part, experienced by the mothers' parents.
Whether the mothers who participated in this study had had positive or negative experiences in their contact/relationship with their children is certainly not a black and white picture. The complexities associated with contact and the establishment of a new relationship are significant. In addition, the triggering of trauma-related issues for some mothers as a consequence of making contact with their son or daughter was identified in this study. In both the survey and focus groups, mothers frequently discussed the quality of the relationships with their children from whom they had been separated in terms of how this has affected their current wellbeing. It is therefore an integral part to this broader discussion in terms of current service and support needs.
Positive experiences
I am very fortunate that my son is a big part of my life. He fits in with my family and we see each other often. I believe I am one of the lucky ones. (248, 2012)
For many mothers, making contact - even if a new relationship with their son or daughter has not been established or universally positive - has been fundamental to their capacity to heal and move forward from the debilitating effects of separation by adoption:
Grief and loss do not go away, however after 18 years of contact, the joy my daughter has brought me and my family has filled that empty place. The scars are still there, but I choose to focus on what I have now, rather than what I lost. I make a point of sharing my story. (969, 2012)
I also feel very positive about meeting with my daughter, even though she has now rejected contact, mainly due to the effects upon others within her family who have pressured her to discontinue contact. It has been an insightful journey though difficult, but I would recommend that the journey be taken. It is worth all the risks to at least meet your child, and for me, important to face and understand the terrors of the past. (146, 2011)
I am grateful that my daughter and I have been reunited. The years between her birth and meeting her were difficult, but a great deal of that pain was healed, and overall, I feel that I am probably a better person, and certainly more understanding because of the experience. (205, 2011)
Some mothers discussed the importance of the role of their child's adoptive parents in the successful establishment of a relationship with their child. The removal of any concerns around where their child's loyalties should lie or what role each of the parties play in their son or daughter's life was viewed as being a very important aspect of the relationship they now share:
His adoptive parents were very loving and supportive. They were both very accepting of my husband and I and our children, who were our son's full brother and sister. We felt we were very fortunate in this. His mother and I still communicate on his birthday and at Christmas. (470, 2012)
After the terrible heartbreak at the time, I was so blessed that my daughter's adoptive parents were willing to allow me to keep in touch via the social worker for all the years until we were able to write directly to one another when my daughter turned 18. We then developed a very close relationship with her family, which has enriched all our lives. I am still sorry I couldn't have brought her up, but things have turned out pretty well. (795, 2012)
I have been extremely lucky in that my daughter took steps to find me. And I have been very lucky in that her adoptive parents supported her in trying to find me. I have been very lucky that her adoptive parents and I have endured a lasting friendship and that they have been very generous in sharing her life with me and with that of her siblings. (978, 2012)
Even though many mothers spoke of the positive outcomes of having contact with their son or daughter, they also emphasised that this success has required a lot of commitment from both sides, and that it is an ongoing work in progress. Some participants detailed the intricacies of how their relationships work:
Eight and a half hours later we got off the phone. And that phone call was he to me, me to he. We said never again in our lifetime would anybody, regardless of who they were, ever come between the two of us again; that if we had an issue with one another we were open and honest and talked about it. And that eight-hour phone call of telling him what I expected of him and what he expected of me. (Mother, Qld)
Although we have been reunited for 22 years, it is still a minefield through which we both walk, balancing each others needs and those we love. (95, 2012)
But you are walking on eggshells all the time, and you really have to meet a very high bar of behaviour. Way more than any other mother. (Mother, Qld)
They say that a lot of adoptees act out because they are pushing you. But I don't know if him not calling me for the last month is because he's just a 40-year-old who doesn't like getting on the phone. But you can't push. I'm really scared that I'm going to lose him again. (Mother, Victoria)
Our children started taking on issues about their identity past their teenage [years]. We "received" our children at the point where you would normally be separating from them (early adulthood). So you have to bring your child close and push them away at the same time, because that's the natural process for that age for them. (Mother, Victoria)
Other experiences
For some mothers who participated in the study, the actual experience of having contact with or meeting their son or daughter was a trigger for reactivating the grief, loss and trauma that they had managed to suppress, for the most part, since the initial separation:
I had a massive breakdown when my daughter found me. I understood for the first time what had happened all those years ago and how that led to alcoholism, and finally, sobriety. (419, 2012)
The trauma was compounded for the mothers who discovered that their children went to unloving, unstable or abusive homes. For some mothers, the knowledge that they were forced, coerced or manipulated into being separated from their son or daughter, as adoption was supposed to give them a better life, only to have their child experience hardship, coldness, neglect or even abuse, was a bitter pill to swallow:
The coerced and closed adoption of my daughter led to permanent changes in my own personality and capacity to engage with "normal" life. It also led to a terrible upbringing for my daughter, at the hands of a mentally unstable woman of two other adopted children besides my daughter. By the time I made contact with my daughter she was a drug addict and had spent several periods in juvenile detention and prison. The disastrous effects upon her were a further cause of trauma for me when I learned about them, and when I became aware that I could have kept her and brought her up myself if I had not been denied information about revocation of consent and availability of services. (146, 2012)
I still struggle, as my daughter suffers the effects of an abused childhood, and the effect it has on my three grandsons. (1031, 2012)
Finding my son very troubled - is gut-wrenching - and I feel it is all my fault. (1487, 2012)
I wish more care had been taken in my son's placing. He was given to a woman who was not suitable and he then suffered a childhood of abuse at her hands. I found this the hardest thing to come to terms with. (613, 2012)
Again, the complexities associated with negotiating new roles with each other was raised as a contributing factor to the quality of the relationship between some mothers and their children:
You believe you don't have the right to validate it as a legitimate relationship; that I am allowed to say these things to you, because all this time I've been told I'm not allowed to have you in my life. And you know, you are almost tippy-toeing because you don't want to upset your child and you are scared of fracturing the new relationship - you've only just found each other. This can knock you and make it hard to form a relationship with them. (Mother, Victoria)
Tensions between the adopted individuals, adoptive parents and the mothers has been a common issue raised throughout this study, in terms of the effects such tensions have on the capacity to establish and maintain positive relationships between those who have been separated by adoption. This issue will also be visited throughout the ensuing chapters.
From the information that has been provided to us in this study by some mothers who have experienced these tensions, some common contributing factors appear to be a lack of communication between all parties regarding their respective roles, needs, and how to navigate dynamics between new family members:
She calls me "that woman". But I respect the boundaries and things. But it's not about them, it's about my son. So he is caught in the middle, and I believe most adoptees are in between two families. The fact that she will not acknowledge me means that I tend to give way. (Mother, Victoria)
Even though I have good contact with him, his adoptive parents have never rung me or written to me or asked to see me. I feel like I am still an embarrassment. They didn't want him to invite me to his wedding because they would have to explain who I was. This meant they pretended forever that he was their natural child and they lived a lie. (256, 2012)
I've been told by the adoptive mother that she gave birth in her heart and that she never wanted her daughter to find us. I've been told by my daughter that her adoptive parents don't understand the process I went through to deliver and adopt my baby. As far as they are concerned, they were told to come to Sydney to collect their new baby and the rest was history. They wanted nothing to do with me. To be honest, I'm very disappointed about their attitude toward me and my subsequent children. (1374, 2012)
[At my son's wedding] some people made me feel welcome, some didn't. I know that and I have always said, on those few occasions, my place is not in the front row. I surrendered that to you [adoptive parents] - I am in the back row. And you know he still loves you - just because he found me doesn't mean he doesn't love you. I've always said that you [son] can take whatever you want to do with that family and we can take what's left. (Mother, NSW)
One mother who had been invited to speak to a group of prospective adoptive parents to share her experience of being separated from her daughter gave the following account:
I was trying to get the message through to these prospective adopters that the first separation hurts [for mother and child]. But they are in denial. They don't want to know. One of them came up to me and said, "But didn't you ever think of the gift you were giving?" (Mother, WA).
Unclear messages can also lead to a complete lack of understanding of the feelings/experiences of the other parties:
I've had adoptive parents say, "But you've had other children". So I explain it by saying, "Each child comes into your life and they take a part of your heart. Which one of yours would you want to give away?" (Mother, Victoria).
5.9 Sources of support since separation
Compared to the time of their pregnancy and the birth of their child, fewer than one-quarter of respondents said they had not had any supports to assist them with issues arising from the separation of their son/daughter (or with contact and reunion) (see Table B16). Just 5% said they did not need or want any support.23
Of those who did have support, this was usually provided informally by their friends (31%), which is consistent with the most common source of support at the time of pregnancy and birth, that is, informal support.
Professional/formal supports were, however, utilised by a significant proportion of respondents. Twenty-nine per cent of mothers have engaged with a registered psychologist or psychiatrist; 26% have used a formal support group; social workers or counsellors have been used by 22% of mothers and 19% said they had received support from a registered search/support organisations. Other types of support included support from other family members, from the father of the child, from parents and GPs. The least common type of support was support from a church group.
Emotional support was the most common type of support given (60% of instances), followed by psychotherapy or counselling (25%).
Overall, most of the instances of support given were seen as being either very (48%) or somewhat (36%) helpful (Figure 5.3 and Table B17). In only 5% of instances, the "support" was viewed as being very unhelpful. Support groups were, on whole, the most helpful sources of support, parents among the least.
Figure 5.3: Sources and levels of helpfulness of support given to mothers since separation from child
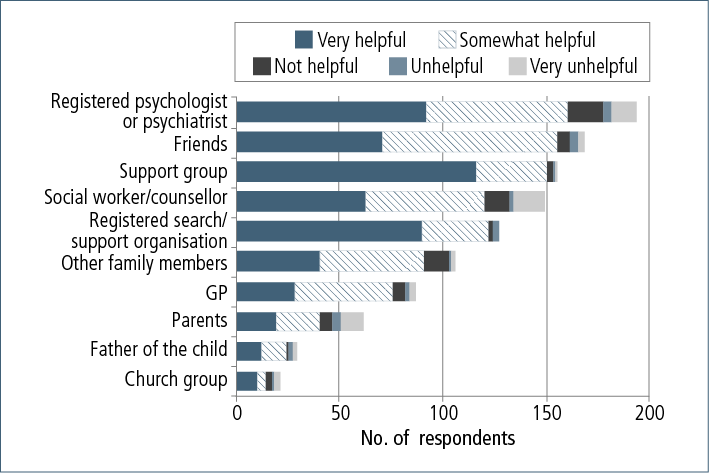
The level of engagement in some kind of formal support since the separation from their child is a significant finding, as it relates to the ongoing effects that this life event has had on mothers. Although we have provided a great level of detail as to what this experience was like for many mothers who participated in the study, the following section focuses on the ways in which these experiences have played out over time.
5.10 Effects of separation
We all survive - I survived … But I don't live. (Mother, WA)
Clearly, the effects of separation have been identified as being significant and widespread:
I am angry at the time of my pregnancy doctors and social workers convinced me that my son would be "better off" in a real family. This was not true. My self-esteem eroded to a point where I believed that to keep my son would be selfish and that if I loved him he needed to be with two legally married people. I also tried to believe it when I was told, "You'll soon get over it", as if giving birth and losing my baby was no more than a dose of the flu. The ripples affect my life and relationships every day. (46, 2011)
Many respondents described the effects of their adoption experience on relationships with their families as being longlasting. It was an assumption in many of the participants' families that the issue was never to be spoken of again, which in turn perpetuated the continued silence, secrecy and shame that the mothers had carried throughout their pregnancies and birth of their child, and had lifelong consequences:
I was told to keep adoption and my daughter a secret. It has caused me to live a double life where I didn't ever tell anyone about my daughter lost to adoption. (88, 2011)
I was told to get over it and get on with my life, and I think that planted a thing in me that you are no good, you don't deserve to be part of the family. You go and do the best you can to go to the places where you are not constantly reminded. So a large part of my life I lived away from my family. (Mother, WA)
Because of my mother's actions of pretending it never happened, and being told I was to never mention it, it made me very angry with her, which I still carry to this day, even though she died three years after I had my baby. (849, 2012)
Being forced to give my son away was the most shattering experience of my life. It has left me with a hatred for my mother and father. It prevented me from ever feeling fit to have other children. (1032, 2012)
I knew I had to do something about it, because at any point, mum and dad were getting frail and I wanted to have a conscious conversation with them. And I knew if I left it too late it would never be resolved. My father displayed similar words and attitudes to what prevailed in the 1970s: "What sort of life would you have had? It was for your benefit. It was a better outcome. It's too late for you to do anything about it now". (Mother, WA)
A smaller number of mothers provided us with accounts where there was admission of guilt or regret later in life from their parents as to the role they had played in the adoption of the mother's child:
So what happened after our babies were gone? Our parents, it really hit them what they were involved in. So instead of being ashamed over us, they became ashamed that they were ashamed. And so they started to make other excuses, like, "She was too young, she was incompetent, she was this and that". [Years later], my father said to me, "I remember the day we took the baby. He was so beautiful. But it was my pride. How bad I felt, how ashamed I felt". (Mother, NSW)
One mother described a poignant moment when her parents were able to take responsibility for their role in the adoption of her son:
I was going to see Mum that morning [of] my first meeting with my son, and she said, "Dad's written this letter he wants you to give him, and he wants you to read it first". And it basically said that I had no choice, that it was completely their decision to have him adopted, and if he wants to place any blame, it's got to be on them. (Mother, Victoria)
5.11 How did these experiences affect the course they then took in life?
The decision in 1975 meant that for the rest of my life I could not admit to my deep desire to have a family of my own. I was desperate to have a baby. I was desperate to find out about the baby I gave away. I always looked for him. I always thought about him and his mother. I broke my heart and I hope I didn't break his. I understood I had no rights, so I tried to move on. I denied myself the experience of motherhood because I had my chance and I made my choice. I had to live with that choice and try to be positive about my later life choices. (343, 2012)
As we have learned through hearing the often challenging and confronting stories of the mothers who participated in this study, their experiences have left many feeling they were the victims of a systematic approach to recruiting "undeserving" mothers to service the "deserving" married couples:
I was never the same again … my emotional health was destroyed from it. (345, 2011)
I have always felt like a second-grade person because of the way I was treated at a most vulnerable time in my life. This allowed me to put up with abuse because I felt I deserved punishment. (1367, 2012)
I think it has stopped me being the person that I could be. (1618, 2012)
I still feel like I am what they told me I was. Dirty, a slut, a whore. You will be back here next year having another baby. (Victoria, 27/10)
For many, the betrayals they reported having experienced from those they trusted - their families, members of a church, hospital staff, social workers - resulted in the inability to trust, form and maintain healthy relationships, and reach their full potential:
I want to go back to then and grow the way I might have grown without this experience. It was like, at the time it happened, my emotional growth stopped. And I chose to stay in the middle, neither having highs nor lows, and stay on that road because that was the least painful. And to be grateful … that I did marry and have children, because I guess I viewed myself as damaged goods. (Mother, Victoria)
My life post-adoption has been a tumultuous journey of alcohol, drugs, depression and anxiety due to my adoption experience. I was made to feel guilty, worthless, unclean and a second-class citizen - not fit to be a mother in society if I placed my baby for adoption, or selfish, cruel and thoughtless if I chose to keep my baby. (444, 2012)
Continued secrecy and capacity to grieve
What can you grieve that you never saw/touched/held? How can you grieve something that you were told to forget as though it never happened? (Mother, Victoria)
The continued silence and shame that so many mothers were left with after their child's adoption made it difficult for them to grieve the loss of their child. Many respondents talked about how, throughout the subsequent years, they carried the weight of their "secret" by themselves, and without the option of openly expressing what they had lived through:
As I have now reunited with my child and have a relationship with him, I can better recognise the feelings I was having during the separation. All those 29 years I was grieving, and there seemed to be no one to understand how I felt … Unrecognised grief affected my life in many ways. (695, 2012)
I have spent years in counselling. I have been diagnosed with PTSD, depression, and complicated grief. I will never fully heal from the grief and trauma of losing my baby the way I did. Shame on the professionals which were supposed to assist me, and instead destroyed the young girl that I was. (1087, 2012)
I felt in retrospect, that in the years between adoption and reunion, that I was emotionally numb, even though I had married and had five other children. It was as though I "woke" from that numbness and started to come alive. (1147,2012)
The suppression of the adoption experience for many years affected all areas of my life. There was not only the loss of my child, but also the loss of trust in any sense of community available to me. I have had to reconcile these two issues first before I have been then able to deal with the huge emotional loss incurred in the experience. (1183, 2012)
The main thing is the shame you were made to feel and having to keep it secret for years, and the affect this has had, [manifesting] in low self-worth, self esteem, etc. (993, 2012)
One mother described how the experience of being separated from her son had such a significant effect on her that she was willing to go to extreme measures to ensure she did not have to go through it again:
It was about 7 months after I had [my son] and he was taken. And I went on holiday with a friend and we hitch-hiked. In those days I was 17. I got raped by the chap who was the driver and didn't say anything to anybody at all and came home. And every night for the next month, in case I was pregnant, I got the biggest knitting needle I could find and used it on myself every single night until I couldn't stand the pain. And I went to work every day, and I don't know when I aborted it or not. If I did, it was in the station toilet. I never told a soul. I got home and said I've got a very heavy period and went to the same doctor who was the one who I told in the first place, and he couldn't look me in the eye. So I'm very lucky that I went on to have two more boys. That's how desperate I was. I had nobody to turn to, not a soul. (Mother, WA)
Subsequent children
Almost all the survey respondents (97%) had been first-time mothers when their child was placed for adoption, and 56% said that their adoption experience either mostly or entirely influenced their ability or their decision to have further children (see Table B21). Some (14%) indicated that the child who had been adopted was the only child they ever gave birth to:
I never married or had other children. My nuclear family have passed on and I now lead a somewhat lonely life. (444, 2012)
The only way I could move on was to suppress any maternal feelings. I was so successful that as a result I do not have any other children. (756, 2012)
My story is a common one for the times. I found from reports that there were other women who did not go on to marry and have more children. It is only now that I am in my 60s that I can see the long-term effects of what happened to me and my family. (1766, 2012)
Some mothers told us how the experience of giving birth to their subsequent children was re-traumatising, or triggered the grief they had not experienced at the time they had been separated from their first child:
I had bad depression and hyper-mania when I had my second child, as I grieved really for the first time - that I found what I had lost, and for the first time felt the overwhelming love I have for my son. I didn't see or hold my adopted son, so I didn't feel anything - no love, no grief, no nothing, just a void. Finding out how a mother feels devastated me. I really grieved then. (256, 2012)
It has negatively impacted all aspects of my life - the way I raised my second child, the man I married. (354, 2011)
When I had my [other] children, I felt as though they were going to be taken from me, even though it didn't make sense. And I feel my mothering experiences were affected. (648, 2012)
Continued guilt and shame
Emotions such as guilt, shame, regret and self-anger permeated the responses from mothers. Sometimes the focus of this was their own lives and the effects they had had; other times, the focus was on the effects they saw on their son or daughter, and wishing they could have avoided the pain:
For my son that is so damaged … you know that primal wound. You think, well no one told me this would happen. But still your heart says, if I hadn't signed the papers, even though I don't remember, it wouldn't have happened. He wouldn't be like this. He would be whole. (Mother, Victoria)
It has and will continue to have a lifelong impact on my life. I have never known what it feels like to be happy or to bond with my children, grandchildren and great grandchildren. It has robbed me of the continuation of my family name and the future generations of my family. It has left me with no faith or trust in God, or the institutions that [were] there to benefit the good of society, and has left [me] with an anger and bitterness that is difficult to resolve. (305, 2012)
It has deeply killed me. Forty-five years I was told to move on with my life, don't discuss any of your past with anyone … Well, I did just that, always feeling very guilty, ashamed, emotionally shattered, so alone, anxious all the time, angry - so very angry. I hate being controlled by anyone. Affected? I am deeply affected by my child's adoption. I will never get over it. I feel sad to know my baby's adoption could have been prevented with help, loving support and loads of compassion. (405, 2011)
I have a huge sense of guilt that my son has got many problems due to him being adopted, and feel sad that I am to blame for this. I feel hate towards the system that told me he would be "better off" with a family, and hate the fact that nobody told me at the time that I would suffer sadness and pain for the rest of my life due to our separation. (56, 2012)
I still believe all those things that I was told about myself. (Mother, Qld)
Effects on relationships
The effects of mothers' experiences of closed adoption can be seen in a range of relationships, including with their parents, partners and subsequent children:
Most of all, I would like to find my self-worth again. I feel I have made choices in life which always reflect on the adoption and that I have chosen partners that are unsuitable for me. I have continually punished myself over the years by lack of self-esteem and have passed this on to my other children, and they have suffered for it. (72, 2012)
I'm trying to make it up to my subsequent children because I wasn't there for them when they were growing up, due to depression. So they all have anxiety disorders to varying degrees … I felt like I let them down. (94, 2012)
I feel sad for my other children that I could not give them everything they should have had from me. When they were little I was always depressed, couldn't cope. I was not always there in body for them. I was always feeling low and worthless. I love my children with my life and we have a relationship that others envy, but part of me was not there. At the time I could never work out what was wrong with me. I now know I was suffering from post-traumatic stress disorder. This is not a clinical evaluation. It has just been proven to me over the years. If not for my other children, I believe I would have taken my life. (988, 2012)
Some mothers are also very protective of their parents, not wanting to hurt them by being seen to blame them for the adoption:
About five years ago, my father said to me one day, "Do you think we did the right thing?" And I said, "It was what happened at the time". And he said, "That didn't answer my question". Because he knew. He's not stupid. But I can't say it, I can't hurt them. They were doing what they thought was best for me, what was best for them and what was best for the baby. (Mother, Victoria)
Life events
Survey participants were asked to indicate on a list of common life events, whether they believed their adoption experience had played any part in contributing to these occurrences (see Table B22). Almost two-thirds indicated that this was true in relation to their marriage, with over one-third specifying that their adoption experience had played some role in their marital separation or divorce. Over half of the sample reported experiencing disruption to either their employment (36%) or their schooling (18%). Almost one-quarter of the sample said they had suffered major personal injury or illness that was in some way attributable to their adoption experience. Conversely, a smaller number indicated that they had experienced outstanding personal achievements that were in some way related to their adoption experiences (16%). Only 11% reported that their experience of adoption had not affected any of the events listed.
Around half of the mothers who participated in this study were engaged in either full- or part-time employment at the time of survey completion (see Tables B23-26), and over one-third indicated that their main source of income was a government benefit. Given that more than half of the mothers who participated in the survey were aged 60 years and over, examining the relationship between their capacity for employment and the effects of the adoption experience is difficult.
As discussed earlier, many women experienced a mistrust of authority as a result of their treatment by authority figures at the time of giving birth. This can have ongoing effects in terms of their capacity to operate in the workplace, and to respond appropriately to authority figures, and organisational structures and requirements:
I find it difficult to make decisions for myself - difficulties in filling in and signing documents, e.g. bank and government docs; extreme difficulty in handling change, especially when it is out of my control; extreme difficulty with bureaucracy and large organisations, such as government, Telstra, banks. (52, 2012)
Engagement in further education was common within the sample, with almost 60% having completed a diploma/certificate/trade qualification, an undergraduate degree, or a graduate/post-graduate qualification (see Tables B23-B26).
Anecdotally however, some mothers indicated that their ability to engage in meaningful employment and/or education had been problematic, and attributed this to the effects of being separated from their son or daughter by adoption:
The emotional stress has compromised my ability to master some of life's demands, particularly work. (1709, 2012)
The pain of it all is exhausting physically and mentally. I no longer work because of my post-reunion outcome. It has nearly killed me. (1843, 2012)
In the survey, mothers reported a number of occasions through the year that were especially difficult for them (see Table B19). Two-thirds of the mothers said that the child's birthday was especially difficult for them, and other difficult occasions include:
- Mothers' Day (60%);
- Christmas (46%);
- their own birthday (23%); and
- Fathers' Day (17%).
Almost half of the mothers said that they were "always" thinking of the son or daughter from whom they had been separated by adoption, and 44% said they "often" thought of them (see Table B18).
Health and wellbeing
Poor mental health has been highlighted as a particularly common issue for the majority of study participants, manifesting in a myriad of ways. Qualitative accounts from both focus groups and survey open-end responses indicate that mental health issues are typical outcomes of past adoption experiences.
A number of measures of wellbeing, detailed in Chapter 3, were included in the survey:
- the shorter version of the World Health Organization Quality of Life instrument (WHOQOL-BREF);
- the Kessler Psychological Distress Scale (K10);
- a life satisfaction scale, based on measure used in the HILDA survey;
- the Impact of Events Scale-Revised (IES-R).
WHOQOL-BREF
For the two single-item measures: "How would you rate your quality of life?", and "How satisfied are you with your health?", higher scores indicate higher levels of wellbeing. Survey respondents rated these items lower than the Australian norms (Table 5.2). This was also the case across the four domains, with only the environment domain being close to the norm.
| Domains | Australian norms | Survey respondents | ||
|---|---|---|---|---|
| Scale score | SD | Scale score | SD | |
| Physical | 80 | 17 | 52 | 13 |
| Psychological | 73 | 14 | 50 | 10 |
| Social relationships | 72 | 19 | 53 | 25 |
| Environment | 75 | 14 | 67 | 20 |
| Overall rating of quality of life | 4.3 | 0.8 | 3.6 | 1.1 |
| Overall satisfaction with life | 3.6 | 0.9 | 3.1 | 1.2 |
Note: SD = standard deviation.
The scores for respondents were examined according to a variety of characteristics (see Table B23), with the following points emerging:
- The relationship between wellbeing and age of respondent appears complex, though for most scales, the older respondents (60+ years) scored slightly higher on the measures of wellbeing than those who are middle-aged (up to 59 years).
- Partnered individuals had higher scores on average than other respondents.
- Those who were workers scored more highly than those not working.
- Higher levels of education are associated with higher scores.
- Generally, the older the age at which the mother gave birth, the higher the scores.
- Whether or not there had been contact with their son or daughter from whom they were separated only had a marginal effect on the scores. However, those who had an ongoing relationship with their son or daughter scored more highly than those who had not.
- Those who were dissatisfied with the adoption process had lower scores than those with higher satisfaction levels.
- Mothers who wanted to keep their child had lower scores than those who had been uncertain or had not wanted to keep the baby, as did those who believed that they could have kept their child with sufficient financial and other support, compared with those who had been unsure or had felt they couldn't.
- Similarly, those who stated their child had been taken or stolen from them had lower scores than mothers who said they had placed or "gave up" their child for adoption.
- Those who had some support at the time of the pregnancy and birth had higher scores on some measures than those who had no support, whereas there was little difference in the scores between those who had and hadn't had support in the years since.
The Kessler Psychological Distress Scale (K10)
As can be seen from Table 5.3, the survey respondents showed much higher levels of psychological distress than those in the 2001 National Health Survey. Particularly of concern is that close to one-third of respondents were likely to have a severe mental disorder.
| NHS female (%) | Survey respondents (%) | |
|---|---|---|
| Likely to be well | 79.6 | 38.5 |
| Likely to have a mild disorder | 10.6 | 15.5 |
| Likely to have a moderate mental disorder | 5.5 | 15.3 |
| Likely to have a severe mental disorder | 4.4 | 30.7 |
Although it is somewhat difficult to disentangle the "cause and effect" of different life events, when these mental health levels were compared across respondent characteristics (Table B24), the following points emerge:
- Levels of psychological distress appear to vary in a complex fashion by age of respondent, though, overall, those who were aged under 60 years at the time of survey completion had higher levels of distress than those who were older.
- Distress levels were lowest for those who were married, particularly compared with those who were widowed, but also compared to those who were single or in other types of relationships.
- Distress levels were highest for those not working and for those with levels of education lower than a graduate or postgraduate qualification.
- Distress levels were much higher for those who had not had contact or had contact but never met with their son/daughter from whom they had been separated, compared to those who had an ongoing relationship.
- Mothers who gave birth before they were 18 years old had much higher distress levels than those who were aged 18 years and over when their child was born.
- Mothers who were more satisfied with the adoption process, those who didn't believe they could have kept their child, and those who felt they had placed or given up their child for adoption, all had lower levels of distress on average.
- Those who were always thinking about their child had higher levels of distress than those who thought of their child less often.
- Those who had had some support during the pregnancy and birth had lower levels of distress than those who had had no support, whereas there was little difference between those who had and hadn't had support since.
Life satisfaction
Only a third of respondents scored their satisfaction with life very highly (8 out of 10 or higher) (see Table B25). A quarter scored their satisfaction level as less than 5 out of 10. The average score for survey respondents was 6.4.
The relationships between life satisfaction and the various respondent characteristics mentioned above show similar patterns to those of the WHOQOL-BREF and K10. Mothers with the lowest average levels of satisfaction include those who had never married (mean score 4.9) and those who felt their child had been stolen from them (4.8). Mothers with the highest average levels of satisfaction included those who were aged 70 years and over at the time the survey was completed (mean 7.4), those who had been satisfied (7.8) or neither satisfied nor dissatisfied with the adoption process (7.6), those who hadn't wanted to keep their baby (7.6), and those who placed their child for adoption (7.7).
Impact of Events Scale-Revised
Mothers were asked a series of questions about the impact their experience of adoption has had on them, with the results providing an indication of whether the respondent was suffering from symptoms related to post-traumatic stress disorder.
Over half of the respondents (57%) received scores that indicated they had many PTSD symptoms (see Table B26). Only one in five had few symptoms of PTSD.
Again, the relationships between various characteristics of the mother and their adoption experience and the Impact of Events Scale were very similar to those found for the other wellbeing measures:
The adoption of my daughter has had a profound and lifelong effect on my health and life. I take anti-depressants and I have been diagnosed with complex post-traumatic stress disorder. (51, 2012)
Physical health issues were also identified as manifesting as a direct result of some participants' adoption experience:
In our histories, these traumas manifest in many ways. We might go [to the GP] because we are feeling depressed. We might go because we have got an unexplained abdominal pain, stomach ulcer, irritable bowel, chronic headaches, insomnia. It's only when you have got a longitudinal relationship with your doctor that some of your story can come out. You are not going to talk about it with a doctor that is only there for five minutes. (Mother, WA)
5.12 Current service and support needs
What we have been able to ascertain from the findings of this study as they relate to the current service and support needs of mothers separated from a child by adoption, is that there has been and still is a clear deficiency in the level of available and affordable psycho-therapeutic options to adequately address the effects of the traumas experienced, not only at the time of the pregnancies and birth of their children, but throughout the subsequent years. The concerningly high levels of psychological distress and likelihood of PTSD-type symptoms in a number of participants - as indicated by the wellbeing measures in the survey and the detailed qualitative accounts - suggest that existing services are not adequately meeting their needs. The ripple effects of their experiences have, in many instances, been profound, as evidenced through the effects on their capacity to form and maintain relationships, their physical health, their engagement in the workforce and their decision and/or ability to have further children.
The effects of past practices have been illustrated in detail in this report in order to demonstrate the level of damage that has been a reality for so many women, and where possible from their accounts, to identify implications for the characteristics of services and responses needed to adequately address their needs.
Box 5.1 Key service system implications
- Mental health professionals - including psychologists, psychiatrists and psychotherapists - will require specialised education and training to respond effectively to the needs of those affected by past adoptions. The two key issues mothers talked about that related to professional education were: (a) knowledge about the events that surrounded closed adoption and the range of experiences that those affected may have encountered; and (b) training in specialist therapeutic skills to address the ongoing effects of trauma, identity issues, negative self-concept, and relationship issues that relate specifically to the adoption experience. This suggests that development of appropriate training modules that are readily accessible to those working in such professions is needed.
- Many current service provision agencies and professions (e.g., church-based agencies, social workers) are strongly associated in the minds of many mothers with their experiences of trauma. Any expansion or creation of new services should be undertaken with sensitivity to this.
- As well as developing a specialist workforce, health and welfare professionals in the broader services would benefit from education about the effects of past adoptions on mothers (including potential physical, social and psychological effects), and training in how to provide appropriate assessment, diagnosis and referral to specialists.
- Post-adoption support services would be obvious places that could act as central points for the provision of information and referral to the broader health and welfare sectors.
- With appropriate resourcing, existing post-adoption services could provide ongoing engagement with those who are at all stages of their adoption journeys. Continuity of care (i.e., not having to repeat one's "story" or build rapport with a new service provider) will play a significant part in the likelihood of those affected feeling adequately supported.
- Addressing current physical and mental health problems that mothers attribute to their past adoption experiences is closely linked to recognising their need for acknowledgement, restitution and positive self-identity.
Mothers' perspectives of their current service and support needs
We are all sitting around this table because we are strong. If we had known back then when we were in that ultimate vulnerable position, where society generally - in other circumstances - protects, nurtures, supports pregnant women … If we had known back then how strong we are today, we would never have given them up. (Mother, WA)
Survey participants were asked to identify the most important thing that would be of benefit to them in their current situations in helping deal with their past adoption experience. Just over 90% of survey respondents (n = 459) answered this question.
There are six key areas that were consistently identified by mothers who participated in this study that reflect their views of their current service and support needs:
- validation;
- acknowledgement through education and awareness;
- restitution through acknowledgement of the truth;
- access to information;
- access to services; and
- a "never again" approach so that society will learn from its mistakes from past practices around closed adoption in Australia.
Importantly, these are consistent with the findings of the Senate Inquiry, which will be included in this discussion.
Validation
Knowing where their thinking came from does not condone their treatment of us. (Mother, NSW)
The information that has been provided by study participants presents an overall message of their need to have their experiences validated. For many, the accounts reported in this study of experiencing broader systemic abuses of power, the use of coercion, abuse (physical, emotional and psychological) and untruths are indeed challenging, but important to hear.
Both survey data and qualitative accounts obtained by participants clearly indicate the desire from mothers separated from their sons or daughters by adoption for their experiences to be validated. The themes of secrecy, shame and broader societal judgements that have been examined earlier in this chapter highlight the ongoing residual effects of the treatment many received from those who they thought would provide them with support and protection.
Some women disclosed how relieved they were to finally know that they weren't the only "bad girl". This study, along with that of the Senate Inquiry (2012), has enabled a sharing of experiences, and through this, they no longer feel alone in their pain.
The power of confirmation in the public arena as to what happened to so many (i.e., the pressures applied to them that made them believe that they were not worthy or capable of motherhood, which often resulted in the forcible removal of their son or daughter), is a message that these mothers communicated as being integral to addressing some of their current needs.
The role of apologies
I would like an apology from someone who represents the system … I believe my child was stolen from me. I believe I was coerced into giving up my child. I know I was given no option. "Sorry" for telling me I wasn't good enough to look after my own child and then giving my child to an abusive mother. "Sorry" for treating me roughly at the hospital, for ignoring my needs and making me feel dirty; for not giving me a birth certificate; for the closed adoption system which kept me from knowing if my child was OK; for keeping the silence for years; … for stealing my child; for dividing the world into bad mothers (unmarried) and good mothers (married). An apology would be an acknowledgement that this terrible thing happened to me. I have been so numb it has taken 40 years for me to even begin to feel … I have spent my life pretending I'm OK, but I'm not. I'm confused, enraged, guilty, grief-stricken. (259, 2012)
In their final report, the Senate Community Affairs References Committee (2012) made recommendation for a national apology to mothers, fathers, adoptees and other family members who are victims of forced adoption, contingent on such an apology following strict guidelines for its delivery (Recommendations 1-7).
Although we did not include a specific question in the survey about whether an apology was warranted or needed, we found a range of views were spontaneously expressed by participants regarding apologies for past adoption practices in Australia. The subject was frequently raised and debated in the focus group discussions held across the country. In addition, around 17% of mothers specifically mentioned the need for an apology in their survey responses.
Participants from most respondent groups in this study supported the sentiments of an apology on the whole; however, the majority view held was that apologies are only appropriate when they are followed by tangible actions that address the harms experienced - both past and ongoing. That is why mothers spent much of the time in the focus groups wanting to tell their individual stories, and to have acknowledged the harms that they have experienced, and current difficulties they encounter. A small number of participants specified that they were seeking financial redress, particularly for the treatment they received from particular institutions, such as the mothers' homes and the hospitals in which they gave birth. For these mothers, they saw financial compensation as appropriate when:
- the traumas suffered and ongoing effects had affected their capacity to earn an income;
- there were physical injuries that were a direct result of negligent medical treatment; and/or
- there are enduring psychological impacts that have required a lifetime of psychiatric/medical intervention.
However, it was more common for respondents in our study to view the benefit of financial compensation being in the form of having subsidised access to psychological services (including trained, specialist psychiatrists, psychologists, and other mental health service providers) for as long as they require it. The issue of distance and costs associated with regular face-to-face contact was identified as being a significant barrier to establishing and maintaining relationships with their children, so there was also a proportion of participants who would like funds to be available to assist them with the costs of travel to see their son or daughter several times a year.
What do respondents expect an apology to achieve?
Participants mostly raised the issue of an apology in relation to the Senate Inquiry, which ran from November 2010 and delivered its report in February 2012. As this period coincided with fieldwork for the current study, an apology was often "top-of-mind" for participants as they were responding to our survey or participating in the focus groups and interviews.
In the first instance, an apology was seen as recognising the mothers' experiences as being valid. Apologies can also be an active way for those involved to take responsibility (individually or on behalf of an institution) for the part they played. Mothers talked about the way in which such an apology would demonstrate a level of accountability for the injustices they have suffered.
Broadcasting the apologies in the public arena was viewed as creating an opportunity to enable a conversation to start within the broader community, so that the continued silence and shame that is carried by so many respondents from our study can be alleviated through an opportunity for dialogue and acknowledgement. Some viewed the importance of this broader public acknowledgement as being integral to altering the perception of what has been the common and long-held view of "relinquishing" mothers:
They still see you as a 16-year-old. (Mother, Qld)
The most profound thing that happened to me was learning about the [WA] adoption apology, and realising that I wasn't a bad person, after all these years. (648, 2012)
Apologies can also provide the opportunity for the sons/daughters who were adopted to have a better understanding of the circumstances surrounding their placement with a new family. This was a strongly held view by many mothers who participated in this study. This shifts the focus away from individual behaviour (e.g., a son or daughter who may wonder, "Why did my mother give me up for adoption?") to systemic influences and the responsibility of society, family, institutions and professionals from the time.
However, in this discussion, it is also important to highlight the perspectives of those who feel that apologies may have adverse effects. As one mother said:
If they say what they did was wrong, then it means I made the wrong choice and I don't think I could live with that … I don't want them to say sorry, because it negates what I did. (Mother, ACT)
Who should provide an apology and what should be said?
The view of the majority of mothers in this study who saw the role of an apology as being integral to their capacity to heal, was that it is not the responsibility of just one group, institution or government; it was seen as the role of all who had some involvement in the practices that saw the coercion and/or forcible removal of children from their mothers.
Although there were hundreds of specific statements that were provided in this study by the mothers as to what they would like to have acknowledged in the form of a public apology, a smaller number of quotes have been selected that encompass the broader sentiments of the sample:
An apology that acknowledges that the law was broken. An apology that acknowledges that the hospital staff acted unlawfully and unethically and denied me my legal rights. An apology that does not skirt around the issues because of fear of having to pay compensation for the severe mental health damages mothers suffered as a result of adoption practices. An apology that does not fob us off with references to "social mores of the time", "in hindsight", "mothers may have been damaged". Social mores were not above the law. We were damaged by the way we were treated. I want the general public to know that I loved my baby. That I did not give her away because she was unwanted. (1087, 2012)
A sincere apology to me, my family and my daughter from all sectors involved in past adoption practices for their part in ostracising us from society and not providing any pre- or post-adoption support to us. (444, 2012)
A public apology that young women like me were mistreated, misinformed, left without support or any real options by the government of the day, the churches, and often the parents and family, because of the conservative beliefs that were prevalent at the time. (495, 2012)
Acknowledgement through education and awareness
For many women of my generation who lost children to adoption, keeping quiet about it was the only option. Most of us were "sent away", and many stayed away and smothered our memories; we simply had no choice. There was no one to listen. It is difficult to reach a certain age and to realise there is an opportunity to speak. Many of us have become accustomed to silence and have learned, somehow, to live with the loss. (43, 2012)
Awareness and education of the broader community
Almost one in three survey respondents (30%) indicated that there is a need for broader community awareness about what happened and how it has affected those involved over time. Many participants expressed a concern that it will be difficult to achieve effective service and support outcomes while there is limited understanding in the broader societal discourse of these issues.
Education and awareness can be a powerful method of validating people's experiences and providing a way for other parties in the adoption circle24 to be made aware of these experiences from different points of view. This approach may also work to enable the issues associated with adoption to be heard throughout the wider community:
The education and empathy of the wider community of the effects of the loss of my only child. To understand that I was not a "bad girl" and that giving up my son was not "my choice". (71, 2012)
Education of professionals
Part of the message of not repeating the mistakes of the past, as well as providing sensitive and appropriate professional services to address the current needs of those affected by past adoption experiences is that the history of closed adoption in Australia - and the issues faced by those who were caught up in events of the past - needs to be made known widely to professionals currently being trained in Australia:
You have this era where young doctors, mental health professionals, nurses are coming through where [intercountry] adoption is so normal, who aren't aware of the history because it has never been written and never put on the public record for what the truth was. (Mother, WA)
Mothers often expressed frustration with their experiences of counsellors and other professionals who were not aware or were dismissive of the effects that separation by adoption had had on their lives. Survey data show that those who have accessed formal forms of support from professionals have found them to be largely ineffective:
Wider community [education] would especially include those working in psychological professions, who too often see adoption as just a tick in a box and so do not recognise the possible long-term impact of separation loss. Imagine a [birth] mother after 20 or 30 years of silence tentatively speaking of the loss of her child for the first time, expressing her grief, shame and guilt, only to feel unheard. (71, 2012)
I think there is much ambivalence, even today, towards women like myself and our experience and the impact it had on the rest of our lives. It never goes away. The pain of loss, the guilt at being so helpless and ignorant of our rights. That needs to be put right. (381, 2012)
Respondents felt that the issues that mothers present with to mental health professionals may be symptomatic of trauma associated with their adoption experience. The shame and secrecy of her experience, as well as the presence of unrecognised trauma, may affect the accuracy of diagnosis and referral to appropriate treatment interventions. Similarly, presentation to GPs with both physical and mental health issues requires further exploration by the health professional in order to determine whether symptoms may be attributed to an adoption-related experience, and therefore an increased likelihood of providing an appropriate referral/choice of a suitable course of treatment.
Restitution through acknowledgement of the truth
As highlighted in the introduction to this chapter, the significance of having one's story told can be a powerful tool in the process of healing. Having discussed the roles that broader community awareness and formal apologies can play in meeting their current needs, mothers also told us that it was just as important for the words they wanted to say to their then infant children to be communicated to them now in adulthood. Mothers saw it as critical that their now adult sons and daughters hear their pleas to those in positions of authority, including their families, for recognition of the wrongs they suffered, their love for their son or daughter, their powerlessness to control what had happened, and the importance that their son or daughter has in their memories and in their lives today.
Study participants described some of the messages that they would like to be communicated specifically to their sons/daughters:
- You were always loved.
- Becoming pregnant may not have been planned, but you were always wanted.
- Even if you don't want to know me, I want you to know that this was not my decision.
- I had no choice.
For example, one mother said:
I want to be seen for who I am, not to continue to be judged for what I had no control over. (Mother, ACT)
Access to information
Study participants discussed on several levels their capacity to access information. Firstly, it was about the need for them to know what happened at the time of the birth; to have the information on adoption documentation verified and corrected where necessary; to correct the untruths (e.g., names, details about them, etc.); and to have their names put on the original birth certificates.
Second, it was about accessing medical/hospital records that detail the process of obtaining consent and any drugs that were administered to them.
Finally, it was also about accessing information that will assist in the process of search and contact. A national system was viewed by those affected as being highly desirable. Many noted that the barriers presented when attempting to navigate an often complex and bureaucratic system across states and territories affected the likelihood of having successful contact and subsequent healing.
Access to services
So it's been 30 odd years for me. You can cruise along for years, and then something happens in your life and you [realise] this is about that - I need to talk to somebody about that. And you need to have access to that particular experienced counselling when you need it. (Mother, Qld)
Almost one-third of survey respondents said they wanted access to funded or subsidised support. This is consistent with the focus group discussion findings as well as those of the Senate Inquiry (2012). The range of support needs identified by study participants is vast; however, the consistent message was that services need to be accessible, affordable and delivered by professionals with specific knowledge/expertise in adoption-related issues.
Thematic analysis of the data revealed significant need in the following areas:
- mental health issues that have manifested as a result of their experiences;
- trauma-related issues;
- grief and loss support; and
- support throughout the search and contact process, including the availability of assistance to deal with the outcomes of the process, both positive and negative:
What I need is to deal with the guilt of giving my son away and not helping him grow up knowing who he is … To actually forgive myself for giving him up. To find the father of my son and tell him we have a son who wants to know him. For my children to forgive me for not telling them they had a brother until later in life, after I found my son. (72, 2012)
To be allowed to grieve without feeling guilty and for professional people to acknowledge this grief. (56, 2012)
A "never again" approach
I think for every woman who stands up and steps forward, I understand the amount of courage that takes. And many stand alone. I hope that out of this, what happens is not the same, where women go on the journey alone; that there is somebody with them they can turn to, someone who can hold their hand and say "You are OK". (Mother, Victoria)
During the focus group discussions, participants were asked what they hoped to achieve through taking part in the study. For many, it was about simply providing information that they hoped could be helpful; others were interested in meeting women with shared experiences; but for many, it was about having a voice. They wanted to contribute to making changes to current practices through revealing the realities of their own situations and experiences. As one participant articulated:
My participation is so that our pain and suffering has not been in vain, and the hope that our participation in this study will not have been in vain. (Mother, Victoria)
There will always be children in need of parents. But it's not about parents in need of children. When you put the emphasis where it belongs, sure, but it should never be about parents needing children. (Mother, WA).
Another mother wrote to us after completing the survey and expressed her hope for what this study may be able achieve:
I do not envy your efforts to support the truth of what happened, and it is in your power to let this atrocity be left unresolved. Or, you can be the hero who fights for the truth and justice of a group of people who have been severely wronged. (Mother, NSW)
5.13 Summary
The majority of mothers who participated in the current study had been - at the time of their pregnancy - in a relationship with the father of their child, and their parents had been aware of the pregnancy; however, few remained living in the family home until the birth of their baby.
Experiences of unmarried mothers' homes had been largely negative, with reports of verbal abuse and the requirement to perform manual labour tasks, often right up to the time of birth. Many mothers described how they felt shamed and punished. Conversely, some saw this as a relatively positive time, with friendships forged with other residents, and treatment from staff described as warm and supportive. However, limited information had been provided to prepare them for what to expect when giving birth.
The birth experience was described overwhelmingly as negative. Mothers focused on the poor treatment by staff from the homes and hospitals, including: being left alone, being verbally abused, being given drugs that impaired their capacity to make informed decisions about their own and their child's wellbeing, being denied pain relief, the use of pillows and sheets to shield their view of the baby, being ostracised from other mothers in hospital and being treated poorly/insensitively if in the same ward as married women (e.g., being denied access to their babies while married mothers were nursing and spending time with their newborns in the bed next to them).
There were reports of many mothers having had no intention of adopting out their child.
In the maternity homes and hospitals, mothers reported threats and the reinforcement of the message that they were not deserving or capable of raising the child on their own and that they were selfish for not giving the baby to a married couple. To a young vulnerable mother, the power of messages from authority figures, such as "If you loved your child, you would give him to a real family", is significant. Such messages were reinforced by the pressures applied by their families as well as the social stigma attached to illegitimacy and single motherhood.
Few mothers described having knowledge at the time of their rights regarding consent or revocation of consent; and when they made attempts to revoke consent, they were met with untruths and/or threats.
The long-term effects of the closed adoption experience have manifested themselves in poorer physical and psychological health for the mothers, compared to the larger Australian population.
On an emotional level, the mothers described having difficulties with issues of trust and feelings of self-worth. Some reported an inability or lack of desire to have further children, based on their adoption experience.
Search and contact processes have been complex for many, yet relatively easy for others. Mothers described the complex issues involved in maintaining a functioning relationship with their adult child who was adopted, including distance, dual relationships for the adoptee (with their adoptive families), and the complexity of their son/daughter's understanding of the situation that surrounded their adoption.
The key current needs that were identified by mothers in this study included the need for validation (through mechanisms such as apologies), acknowledgement through education and awareness and retelling the untruths, access to information, access to support and ensuring that we learn the lessons of the past and that the harms associated with closed adoption should never happen again.
18 The high level of missing responses for these questions made these data somewhat difficult to analyse. One could assume that most people who did not give a response, did so because this was not a factor for them; however, many mothers selected the "not at all" option. It is clear that many mothers believed that the main reason for them receiving a lower level of care during the birth was their unmarried status, followed by their (young) age, and in some cases their social and economic status. What can also be deduced is that few respondents believed that race/ethnicity and religion played a factor in the type of treatment they received at the time of birth.
19 Mothers were able to provide more than one response to this question to describe their experiences of advice given regarding contact with their child at the time of birth.
20 The term "illegitimate" was altered to "ex-nuptial", firstly through the Status of Children Act in Victoria and Tasmania, and with other states/territories subsequently effecting similar changes. Prior to this, children born outside of registered marriage were legally referred to as "bastards".
21 Such responses were categorised as being societal viewpoints of age, as the additional information provided in individual responses indicated the societal pressures that applied, based on age, marital status and associated stigma.
22 With the legislative changes across the states/territories that moved from closed adoption to greater openness in adoption practices, came first the capacity for parents and adoptees to search and make contact through a third party. Although there are state/territory differences, in general, both parties are able to place a veto on making contact, in which case their details cannot be passed on. (For further information, see AIHW, 2012; Higgins, 2012).
23 It is likely that for many women their husband has been a source of support, and may well be the most common source. However, we did not specifically ask about spouses as a source of support in this set of questions. A few women did list their husband as a source of support under "other", but we believe this underestimates the level of support from spouses.
24 We use the term "adoption circle" in reference to all those affected by adoption in preference to the more commonly known "adoption triangle", as we feel it is more inclusive of all those affected by adoption, such as wider family members.
6. Fathers separated from children by adoption
As the NSW Legislative Council Standing Committee on Social Issues (2000), articulated in their report on adoption practices 1950-98:
The fathers were disregarded and very little was done to consult or involve them during the birth and in the postnatal period … this failure to acknowledge fathers was wrong and caused long-term harm to those involved. The failure to record the birth father's name … has also caused pain and suffering to them and to other people, including adoptees. (p. 119)
Participation in this study by fathers separated from a child by adoption was limited, perhaps a reflection of the sentiments of the NSW Parliamentary Committee, in that fathers were often not an active "part of the equation" of adoption. The challenges associated with recruitment of this respondent group were multiple, yet not unexpected. We were only able to meet face-to-face with three fathers, and just 12 completed the online survey. However, for those who did participate, they were able to provide us with a rich and often frank picture of what it has meant for them to be separated from a child by adoption, and the journeys they have travelled in the subsequent years.
6.1 Respondent characteristics
Twelve fathers who had been separated from their child by adoption responded to the online survey, and just three of these fathers participated in the qualitative interviews:
- All were in the age bracket 58-70 years bar one, who was considerably younger.
- Two-thirds were born in Australia.
- All had been married, but three were now divorced or widowed.
- A third were working full-time, a third part-time and a third were not working.
- Five had university qualifications, four had a diploma/certificate/trade qualification and the remaining two had completed high school.
- They were from a range of states/territories.
They had found out about the study via:
- an adoption support service (n = 3);
- a friend/family member (n = 4);
- a newspaper (n = 1);
- a health/welfare professional (n = 1);
- the radio (n = 2); and
- other (not specified) (n = 1).
6.2 Pregnancy, birth and separation
The pregnancy
Almost all of the fathers knew about the pregnancy at the time, with one finding out when the child was born, and one finding out later. The fathers had a variety of reactions:
Regret … guilt … Wanted to marry, and be a father to my child. (178, 2011)
I was confused and angry. The pregnancy was not supposed to happen; she was on the pill. But I accepted her claim that the baby was mine, reluctantly, under the circumstances. When it became a reality, I wanted to be involved. (Father, Victoria)
I was only 17 … so I had no position or say. I was quite immature at that age, as most of my friends were. (Father, 17)
I was fearful and confused, afraid of the shame my family would endure if the secret got out. (Father, NSW)
Happiness and yet apprehension. (Father, Victoria)
It was a very traumatic time for both the mother and me. We were very young and did not handle it well. (148, 2012)
I wanted to marry the child's mother, but was threatened with carnal knowledge and imprisonment if I did not stand back … We later married, and have two more children. (1790, 2012)
For only two respondents, the pregnant woman had been their girlfriend; for seven respondents, she had been an acquaintance. Only in one case had she been previously unknown to them.
Half of the fathers had maintained frequent contact with the mother of their child during their pregnancy; the others had little or no contact.
Most of the fathers who responded to our survey said that their parents had been informed. Only four fathers said their parents had not known about the pregnancy.
As presented in section 5.4, mothers were asked to identify the three main reasons their child had been adopted. Contrary to the public perception that the fathers must have deserted or abandoned the women upon discovering they were pregnant, mothers in this study gave lack of support or "abandonment" by the fathers as only the 9th most common factor directly contributing to their child's adoption.
The child's birth
According to the fathers, eight of their adopted children were girls and four were boys. At the time their children were born:
- a third of the fathers were aged 17-19 years;
- a third were aged 20-22 years; and
- a third were aged 24-32 years.25
Seven of the children were born during the period 1970-74, with three born in the decade before, and two afterwards. Eleven of the children were born in Australia, across five different states/territories.
Contact with child at time of birth
Three-quarters of the mothers were immediately separated from their baby, with only one mother retaining contact for more than a day.
Four of the fathers saw their child, but only one saw the child more than once. Three of the fathers were able to hold their child.
Birth certificate
In only two cases was the father named on the birth certificate, but in three cases the father had since arranged to have his name added retrospectively. In one case, the father was named on the birth registration form only. Common procedures for obtaining information to be included on the birth certificates was largely placed on the mothers, and the majority of mothers who participated in this study stated that the fathers had not been named. The reasons behind this were varied; however, many mothers said that they had not realised that it was an option to have the fathers included.
This issue has been examined in other discussions relating to fathers separated from children by adoption, and its significance in terms of the effects this has had on reinforcing the notion that fathers had abandoned responsibility. As Coles (2004) asserted:
Not only does this procedure dishonour the role of birth fathers played in conceiving their child, but it also leaves the lingering impression that the father did not care enough about his child to insist that his name be recorded on the original birth certificate. This perception may be picked up later by the searching adopted person, when they discover a birth certificate with but one name, that of the birth mother. It is no wonder then that so many adoptees are apprehensive about finding their birth father. (p. 105)
Adoption experience
Like the majority of the mothers we heard from, the fathers responding to our survey were very unhappy about the adoption process:
- seven of the fathers had wanted to keep the child and the remaining five had been uncertain;
- three fathers said their opinion had been taken into consideration before the child was adopted;
- nine of the fathers were completely dissatisfied; and
- none of them were satisfied that their interests had been looked after throughout the adoption process.
In relation to wanting to keep the child, fathers stated:
Once I was told about the pregnancy I wanted to be involved, either in marriage, or any other way possible, including financial support and contact. Every offer was refused point blank. (178, 2012)
Hindsight does not really help. At the time, shock was clouding any judgement or logic. Now, I would say yes. (Father, NSW)
It was expected in those times that if parents were not a couple they should not keep children. (148, 2012)
I was stunned by the mother's decision [to have the baby adopted], but acquiesced thinking, wrongly, it was the supportive thing to do. (1728, 2012)
Nine of the fathers believed that if they had had sufficient financial and other support, they may have been able to keep their child. The remaining three said that maybe they could have. One father stated that he and the mother could have kept the child even without additional financial support, and another said that he would have kept the child anyway, if given the opportunity.
The most common reason given for why their child was adopted was that the father was never asked/had no rights or say/mother decided on her own (n = 11). As one father described, there was an inevitability, almost, about the outcome:
I just knew that it was going to happen. The thing is, the boy was not part of the journey. He wasn't part of the decision process, he wasn't part of the good or the bad. He wasn't part of the decision process. He didn't even know the process to make a decision, to object, to say anything. You just weren't any part of the process. (Father, NSW)
Other common reasons provided by participants were:
- their parents decided (n = 5);
- there was no support available (n = 4); and
- they were too young (n = 3).
One father described in an interview the feeling at the time that the systemic pressures placed on young people in their positions was somewhat of a "losing battle":
There was a system in place within the church, government and hospitals, that was highly structured, … like it is a predator. It had a predatory feel about it, because it was just out there and the eyes are looking at it [the child]. And it goes, "That's it!" And I would have thought that once they had their eyes on a target, with a view of vulnerability, age, time, the whole lot. And this is the problem - the girls at the time had to handle it and I don't think they stood a chance. There was a big force in action. (Father, NSW)
There were a variety of outcomes for the subsequent relationship with the mother of their child, including the following:
- Two of the fathers married the mother of their child, and are still married.
- Two fathers continued a relationship for a while after the adoption, before splitting up.
- Three fathers were forbidden to have contact with the mother.
- In two cases, the relationship was destroyed by the pregnancy/adoption process.
Past use of services and supports
Fathers received very little support at the time of the pregnancy, birth and separation. Six fathers reported having had no support at this time, and one indicated that he had not needed any support. As one father articulated in a group discussion:
There was a lack of permission to grieve. You weren't entitled to do that. (Father, Victoria)
Of the remaining five fathers, one mentioned two sources of support and the others just mentioned one source, not all of which they found helpful:
- one received emotional support from their parents that was somewhat helpful:
My mum always reminded me each year on her birthday. She would always remind me in a good way. (Father, NSW)
- one received "other" support from their parents that was in fact unhelpful;
- two received emotional support from friends that was somewhat helpful; and
- one received some support from their mother, not their father, and saw a social worker on the day that he held his daughter, which he considered equivalent to almost no support.
6.3 Search and contact
Search
Nine of the fathers had tried to find information about their son/daughter, including trying to search for them. Half of the fathers used contact services (two fathers used two services, and one father used three services):
- Three fathers used the relevant government agencies.
- Two fathers used agencies responsible for organising the adoption.
- Agencies used by one person each included the Registrar of Births, Deaths and Marriages; a solicitor; and the newspaper births and deaths section.
Three fathers reported that the services they used were helpful because they gave information that helped locate their son/daughter.
One father who participated in a face-to-face discussion, told us about his journey of searching for his son, which involved making contact with the mother of his child in the first instance. He explained that the first thing he needed to do was apologise to her for letting her down at the time of the birth/subsequent adoption:
I ended up turning up at her work, and we spent 4-5 hours together talking it through. It was a very powerful experience - forgiveness, ownership, etc. I felt like a new person after doing that. (Father, Victoria)
Ten of the fathers have had contact with their son/daughter (four with sons, six with daughters):
- three when the son/daughter was aged 18-22 years;
- three when the son/daughter was aged 25-30 years; and
- four when the son/daughter was aged over 35 years.
For four fathers, this contact was 15-20 years ago, for three fathers it was 5-10 years ago, and for the remaining two fathers it was 3-4 years ago.
Seven of the fathers indicated that the outcome of contact with their son/daughter was that they have been able to establish an ongoing relationship with them. One father has contact about once a year, and the other two fathers do not have an ongoing relationship.
The relationship with my daughter is one of the beautiful pieces of my life. My wife is godmother to her son, I am a grandfather and my son has a sister. (Father, NSW)
My daughter finding me, after 36 years of separation, with [agency] help, has been the best thing ever in my life. The emotions of found are just as powerful as those of loss. It has affected me profoundly. (148, 2012)
What impact did it have on me? It enriched my life. It completed a circle that I would have gone to the grave worrying about. Not about her, but worrying about [if I hadn't found her]. (Father, NSW)
One father, whose relationship with his daughter is now fractured, shared how this has affected him.
I actually "lost" my daughter twice, once at birth and then after reunion. That is doubly hard to deal with. She has forbidden all contact. I saw her and the children at least twice a year around birthdays and Christmas for nearly three years. I thought it was a good relationship, but she had a confrontation with her adoptive mother about me and changed her mind. I don't think she had told her. Immediately after that, I got an email telling me she wanted no further contact. Now I have no relationship at all. Her brother, also adopted, was banished from the family for seeking information on his birth parents. There has been no contact with his adoptive mother for maybe fifteen years. (178, 2012)
Another told us of how challenging and drawn-out the process of searching for his daughter had been, and some of the barriers that he came up against throughout this time:
I tried for over 30 years to find out about our daughter … I wrote many respectful letters and made many polite enquiries without success, … asked them if I could be put on the list of parents who would welcome contact. As my name was not on the birth certificate, I was told this was impossible without the birth mother's consent … I was contacted by [agency], who replied to a letter I had sent in the 1970s, saying the child wanted to meet me. This came out of the blue, and we wrote to each other for about a year and then met. We have continuing contact. (148, 2012)
Effect of contact on relationships
The contact between the fathers in this study and their son/daughter has had a positive effect in most cases on their relationships with their spouse, their other children and other family members (see Table 6.1). The impact was less positive on average with their parents. For one father, contact with his child had very negative impacts with all his other relationships.
| Effect | Spouse | Other children | Parents | Other family members |
|---|---|---|---|---|
| Very positive | 4 | 3 | 2 | 2 |
| Positive | 5 | 6 | 2 | 6 |
| None | 2 | 1 | ||
| Negative | 1 | |||
| Very negative | 1 | 1 | 3 | 1 |
Note: Only includes fathers who had had contact with their son/daughter (n = 10).
6.4 Services and supports used since separation
Six of the fathers had not used any services or had any supports since being separated from their son/daughter. Of the other six fathers, one father had accessed many sources of support, one had accessed two sources, and the remaining fathers had just used one form of support.
The father who used multiple forms of support did so because his wife - the mother of their child who was adopted - was suffering health issues. However, some of the sources of support he described as being not helpful, in particular:
- the psychologist/psychiatrist and GP; and
- the registered search organisation because the couple met their son/daughter's parents, rather than son/daughter.
However, his parents were very helpful and the support group that they eventually found was very helpful and was the beginning of the road to recovery.
The sources of support for the other fathers were:
- a support group providing emotional support that was very helpful (n = 2);
- visits to a registered search organisation that proved somewhat helpful (n = 2);
- friends, who in one case provided very helpful emotional support, but in another case were not helpful.
6.5 Effects over time
In this study, fathers were asked how often they had thought about their son/daughter from whom they were separated, both in the years following the adoption, as well as currently.
Then
Seven of the fathers often thought about their son/daughter at the time of separation, three were always thinking of them, and two sometimes thought of them.
In the 12 months following separation:
- ten of the fathers recalled experiencing a sense of loss for their child; and
- six fathers recalled experiencing a sense of loss for the mother of their child.
Now
Now, nine of the fathers always think of their son/daughter, and two think of them often.
Some fathers described feelings of guilt in the subsequent years following the adoption of their child:
I felt I had been the guilty party, and carried it as a burden over decades. I felt I could share it with no one and it was a silent subject in my family. Meeting our daughter and being open about it has been very good. (148, 2012)
I regret not arguing for keeping our daughter at the time of her birth. Her absence from our family leaves a hole in my heart. I wish we could be reunited. (1728, 2012)
The impact of the adoption on my daughter is my greatest concern. We were led to believe that she would have a better life, that she would be happy. This was not the case. I feel a great deal of shame and guilt for what I have put her through. I feel the loss almost every day, even with regular contact. (481, 2012)
Life events
Fathers were asked about whether they find any times of the year that are particularly difficult for them in relation to thinking of their son/daughter. The most common times of year that were identified as being hard for fathers in this study are:
- child's birthday (n = 7);
- Christmas (n = 6);
- Mother's Day (n = 2);
- own birthday (n = 1);
- holidays (n = 1);
- working with people the same age as son/daughter (n = 1); and
- grandchildren's birthdays (n = 1).
One father spoke of how difficult he finds it not having contact with his grandchildren:
I only hope that if I live long enough (80 or thereabouts) that I can have contact with my grandchildren when they turn 18 … I am left with a feeling of intense sorrow - that is the only word to describe what I feel. (178, 2012)
Other children
All except one of the men had fathered other children, and all had only had one child from whom they were separated by adoption. In all cases, it was their firstborn child who had been adopted.
There was considerable variation in the extent to which their adoption experience influenced their decision to have further children:
- five said "not at all" or "a little";
- four said "moderately"; and
- three said "mostly" or "entirely".
Fathers' health and wellbeing
Based on their responses to the K10 measure, one-third of the fathers were likely to have poor mental health at the time of survey completion. Almost all of them showed some symptoms of post-traumatic stress (64% with severe PTSD symptoms and 37% likely to have PTSD).
When asked how satisfied they were with their life, on a score from 1 to 10 (with 10 as the highest level of satisfaction), two-thirds of them rated their satisfaction as 7-9, and one-third as 4-5. These respondents had lower levels of life satisfaction when compared with men of the same age who completed Wave 8 of the HILDA survey.26 In HILDA, 86% of men aged 58-70 rated their life satisfaction as 7-10.
6.6 What would help now
Most of the fathers wrote about how the experience of adoption has affected them and what would be of assistance to them currently.
Education and awareness
Some fathers identified broader understanding from the community as being of extreme importance to them for their current and future wellbeing. This involves making people aware of what the adoption climate of the day had been like and how this had affected their capacity to be involved in the decision-making process about their child's future. Acknowledgement of the result of trauma that occurs from the separation of family was also viewed as being of importance:
More information about the adoption and the processes involved at the time. (481,2012)
Understanding why it was so controlled by other people, including the church, and the fact that the male just did not exist in the adoption process. (627, 2012)
Someone to admit that the mainstream Christian churches, government, medical profession and legal profession - that they were all in cahoots to rob people like us of their children. (1078, 2012)
Some fathers said that some kind of acknowledgement from those involved in past adoption practices was perhaps even more important for the mothers and adoptees:
Adoption is a very bad experience and its mental health impacts on natural mothers is catastrophic. This must be recognised … and the need for Australian laws to acknowledge the fact that family is the core component of any society, and states and governments must protect that unit. (156, 2012)
Understanding from their children
A common theme for fathers in this study was their desire for their son/daughter from whom they were separated to understand the circumstances surrounding their adoption, such as the fathers' lack of choice in the decision-making process at the time. This would be of assistance to them currently:
The only thing that would help me is my daughter changing her mind about having contact with me. (178, 2012)
Being able to talk about it with my adopted daughter, telling her the story of it. But she does not want to hear it. (1728, 2012)
Helping my son understand the situation we were in. (1790, 2012)
I would like to see the Hollywood charade of adoption - which is portrayed as caring for children - portrayed more accurately as baby theft. Inter-country adoptions are far more repugnant to me, as I see it as a way of exploiting whole underprivileged groups in order to take their children, instead of providing them with the funds that they need to live together as natural families. (156, 2012)
Access to support
The concern from some of the fathers as to the limited availability of supports for themselves and others was raised as an issue in terms of current service and support needs. Given the very low numbers of fathers participating in the study, there was some discussion around the need for very targeted advertising/campaigning for men, who may have never been able to speak of their experiences with anyone to this point in time:
The other thing is, males don't want to talk about it. Whether a male wants to talk about it, you almost need to talk a different language to them sometimes. But it's all about the same thing. (Father, NSW)
One father, whose story has been very positive in terms of the relationship he has with his daughter, felt that it was imperative that other fathers hear about his experience, so that it can perhaps encourage them to go on the journey of search and contact; that the benefits of what he has now have not come without hard work but the challenges they have faced have indeed been worth the effort:
A lot went into it, it didn't just arrive. There are some deep scars to carry and wounds. And to fix them and come back - it was a full-blown story. But the one thing that I would like to come out of this is, if other people who have fear in their soul could take the story and take the risk of going to find their journey … But in their case, give them structure along the way that can help them. I would love that, it would make more sense than what happened to them. (Father, NSW)
Fathers who participated in face-to-face discussions spoke in more detail about the need for the availability of "funded, professional counselling by qualified counsellors who have an understanding of adoption issues".
As one participant described:
where a trained person that has empathy, that has the strength, that understands the process, that can evaluate the person, that can give them a path that is not like a rigid path, because otherwise if they don't walk that path they think they are not going to get there. If they are given a general path and milestones to reach, and every time you reach a milestone you can sit and look back on the alley from where you have come from, and the whole time, you can still see the peak. (Father, NSW)
Acknowledgement of fathers' experiences
Other researchers have acknowledged that birth fathers' experiences and perspectives are often ignored in relation to adoption and the effects of past adoption practices (Clapton, 2007; Passmore & Coles, 2008). It is only in the last 15-20 years that there has been any research attention on the experience of fathers who have had a child adopted, mainly in the context of closed adoption in Australia.
Passmore and Coles (2008) outlined a range of reasons for the lack of representation of birth fathers in the research and public dialogue relating to past adoption practices, including:
- the fathers' names were often not recorded on the birth certificates;
- they may not have been informed of their paternity;
- there are stereotypical views of birth fathers being sexually exploitative; and
- they have experienced shame and guilt over abandoning the mother.
Recognition of these factors may influence birth fathers to acknowledge their experiences, researchers and practitioners to focus attention, sons/daughters to be interested in making contact, and the general population to change their views of this aspect of the adoption process.
These studies show that, just as with birth mothers, fathers also experienced parental pressure (Clapton, 2007). Another significant theme is the issue of exclusion from the arrangements and decisions. Passmore and Coles (2008) documented in their study of 27 birth fathers that there was an inverse relationship between agreement with the decision to "relinquish" and fathers' current sense of hope, and their perceptions of the effects of the event on their current life. Effects were noted in areas such as current emotions, personal identity and personal relationships (e.g., with their current spouse, including cases where they had kept their experience a secret). Most of Passmore and Coles' sample had made contact and/or experienced a reunion, some of which had not been very positive. Many described conflicting feelings, drawing a distinction between what Clapton (2007) referred to as: "being a father, but not a 'dad'" (p. 66). However, the primary reasons reported by fathers for wanting contact were "altruistic" (Passmore & Coles, 2008). Based on a small sample of birth fathers, Passmore and Coles (2012) identified a range of contexts and characteristics of more and less satisfying reunions. Lower satisfaction was associated with a mismatch between the needs of birth fathers and their sons/daughters, and where they reported having difficulty developing a relationship.
Clayton (2007) came to the conclusion that there were more similarities than differences in the experiences of birth mothers and birth fathers. He concluded that, "there can be an enduring psychological/attachment bond between the child and their biological father that is of significance both to the child and the father, whether the father is present, absent or indeed has never been known to the child" (p. 69).
Box 6.1 Key service system implications
Fathers' accounts suggest areas of improved service provision relate to:
- inclusion of their names on birth certificates;
- access to "search and contact" services;
- advice and assistance with managing ongoing contact with son/daughter, including assistance with helping sons/daughters understand why they were adopted, and that it wasn't necessarily the fathers' choice;
- funded, professional counselling by qualified counsellors who have an understanding of adoption issues and its effects (including post-traumatic stress);
- coordination of peer supports for fathers who have been damaged by their experience of adoption; and
- increased societal awareness and understanding of what happened and why, and acknowledgement of the injustice of past practices.
6.7 Summary
Although very few fathers completed the online survey, their experiences reflect what many of the mothers who also participated in the study have told us.
These fathers wanted to have a say in what happened with regard to adoption, and many wanted to keep the baby. Very few of them had support at the time of the pregnancy and birth, and very few have had support since. And of those who sought support, in general the support agencies provided better assistance than the medical profession.
Almost all of these men went on to have other children. Most of these fathers sought contact with their son/daughter, and most now have that contact, which in general appears to have had a positive effect on the fathers and their families.
Their current needs relate to wanting increased societal awareness and understanding of what happened and why, and the provision of individual psychological and peer supports for people who have been damaged by what has happened. Around one-third of fathers in this study were likely to have poor mental health and almost all of them showed some symptoms of post-traumatic stress.
25 The father's age at time of the child's birth was estimated by calculating the father's year of birth (from his current age, given in the questionnaire from the year 2011), and then subtracting the child's year of birth from the father's year of birth.
26 This is the dataset that contains information on whether the respondent had been adopted.
7. Persons who were adopted
The closed records adoption system was a violation of the human right to know oneself. To be given an entirely fictional identity was a further cruelty. To have birth rights stripped away is utterly immoral and wrong. (53, 2012)
For many adopted individuals who participated in this study, the experience of closed adoption is best described as a lifelong journey of discovery. The complexities within the experiences shared with us by 823 adopted individuals (54% of all survey participants) across the country, reinforces the need to delve deeply into the information that was provided. As the embodiment of the consequences of the closed adoption system in Australia, the adoptees participating in the study overwhelmingly expressed the view that their collective voices - as varied as they are - must be listened to carefully.
Adoptees responding to our survey were not asked to identify their gender; however, it is likely that there are gender differences in areas such as the effects of their adoption, as well as the experience of contact.
7.1 Terminology and language
As for mothers who are separated from children by adoption, the issue of terminology and the language that is used in reference to individuals who were adopted was a frequent point of focus in the discussions with this respondent group. Similarly, the report from the Senate Inquiry (2012) acknowledged the sensitivities in the broader public discourse in relation to common terminologies.
Some participants expressed dissatisfaction with the use at all of the word "adoption" in this study, as they said their own placements were a result of forced adoption and/or that no formal/legal record of their adoption actually exists (i.e., their adoptions were privately arranged). Many adoptees also do not appreciated being referred to as "children". Therefore, in this report, we use terms such as "adoptee", "persons who were adopted", or "adopted individuals" to describe participants who were adopted as children during the period of closed adoption in Australia.
7.2 Respondents
Adopted individuals participating in the current study represent a very broad range of ages. Some insightful viewpoints were shared across generations, particularly in the focus group discussions.
The quantitative survey results (mainly item frequencies) for adopted individuals are provided in Attachment C. The following discussion of the highlights from both the quantitative and qualitative research draws upon these data, with references provided to the relevant detailed tables as appropriate.
7.3 Family of origin
About half of the survey respondents were born in the 15-year period between 1960-1974, with only 9% born after that time (see Figure 7.1 and Table C1).
Figure 7.1: Distribution of adopted respondents, by year of birth
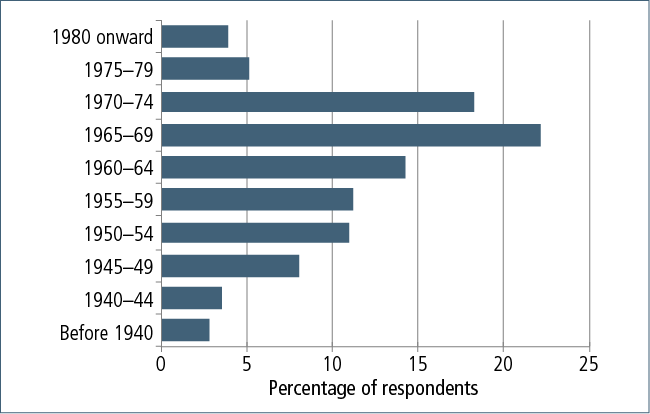
Respondents' places of birth were spread across all states and territories in Australia, with the majority having been born in either Victoria or New South Wales (30% each) (see Table C1). South Australia and Queensland were each the states of birth for 13% of respondents and 6% were born in Western Australia. There were very few participants who had been born in Tasmania or either of the two territories (fewer than 4%). Five per cent had been born overseas.
Over 80% of respondents had been born in a capital city, and 80% had been born in a hospital (see Table C1). Most of the remainder had been born in either a maternity home or church home (9% and 7% respectively).
About one in ten survey participants indicated that they had lived with their mother or other family member before being adopted by another family.
7.4 Adoptive family
Many respondents (43%) were the only children in their adoptive families who were adopted (see Table C2). A similar proportion (45%) grew up in a family with one other sibling who was also adopted. We did not specifically ask survey respondents whether there were other children in their adoptive family who were the biological children of the adoptive parents; however, short-response items in the survey and focus group discussions revealed this to be the case for many study participants:
I think it was talked about when I arrived home, as my older brother was also adopted. It was always talked about openly. (241, 2012)
My brothers were also adopted and we were all incredibly different looking. It was just a part of our life. (567, 2012)
My two siblings were not adopted, so I was not sure what this meant in terms of my future - how secure my position was in the family. (463, 2012)
The news came in the same year my sister was born, who was a natural birth for my parents. (532, 2012)
When adoptees found out they had been adopted
Many of the respondents found out they had been adopted when they were quite young, with more than half knowing by the time they were 5 years old (see Figure 7.2 and Table C2).
Figure 7.2: Age when adoptees found out they had been adopted

Sixty-eight per cent of respondents said that their adoptive parents told them about their adoption (see Table C2). Another 17% had known they were adopted from a young age, but could not recall how they found out. Others found out by accident (8%), were told by another family member (5%) or found out in some other way (8%). A very small number (less than 1%) found out when contacted by their (birth) parent(s).
Reaction to finding out
Because some respondents were told at a very young age that they were adopted, they were unable to recall their reactions to finding out (i.e., they had "always known"). Others told us they simply had no recollection of how they felt when they were told or found out they were adopted.
For those respondents who recalled their reaction (n = 683), the information they provided us ranged from very positive through to significantly more negative (particularly for those who found out later in life). Positive and negative reactions were of almost equal proportions in the responses we received in the survey. Just fewer than half the respondents said that finding out they were adopted was never an issue for them, and a very small number had a positive reaction and/or were relieved to find out they were adopted because of the very negative experiences they had growing up in their adoptive families (such as abuse). Knowing that they weren't biologically related seemed to be of some comfort to them.
Numerous respondents spoke about being given a special book that explained what adoption meant and that they were "specially chosen" by their adoptive parents. For some, being told about the day they were picked up was regarded as a favourite story in their childhood:
My parents had purchased a book called Mr Fairweather and His Family, and read it with me and told me I was like the boy in the book. (41, 2012)
It was a bedtime story, and it seemed like a nice story to me. (216, 2012)
I grew up always knowing I was adopted. I felt chosen and loved by my birth mother - because she gave me up - and then chosen and loved by my adoptive parents. Mum and dad told me that they went into a room with lots of babies and they chose me. (570, 2012)
I have always known that I was adopted. The judge who signed my adoption orders gave my parents a lecture on making sure that they told me. They even had story books about families adopting. (676, 2012)
It was a story my mother told me. Like a bedtime story. (895, 2012)
Special. My parents told me they had gone to the hospital and looked at all the babies and couldn't find one. They had asked the matron if this was all the babies and she said there was one more that was ill. They wanted to see that baby [me]. When they went into the room I was crying, but I stopped when I saw them and smiled, and they knew that they had to take me home. (611, 2012)
A number of participants told us they felt lucky that they had two mothers - that their (birth) mother loved them so much that she wanted them to have a wonderful life with their adoptive parents:
My parents always spoke to me about it from a very young age. I felt proud about it. My mum described it as "the greatest gift of love and unselfishness" another person could give - when they couldn't provide the life they wanted for their baby. She made it clear it was an act of love to be given up for adoption and chosen. (620, 2012)
My parents always told me my birth mother loved me but couldn't look after me, so she unselfishly gave me up for adoption so I could have a better life. (311, 2012)
However, of those who could recall their reaction, just over half had a negative response to the information. For many, it instilled a fear that they could be given away or sent back at any time, and there were frequent descriptions using words such as "shocked", "devastated", "confused", "didn't understand", "sad" and "angry":
Always bothered me. Sad, confused, angry. (50, 2012)
Scared - I thought they were taking me away to a home. (1242, 2012)
I was more concerned about my feelings of despair and when someone was coming to take me back to the orphanage. (1411, 2012)
Initially numb, then confused, then disappointed, and finally embarrassed. (140, 2012)
I can say that I often had feelings of insecurity as a child because I always felt that my relationship with my adoptive parents was not permanent and that I could be given up at any time. (96, 2012)
Startled, embarrassed, hurt. It explained a lot. (262, 2012)
I was relieved. My most important thought, which I still remember absolutely, "I will not inherit her wickedness". And somehow I knew I was not going to be like her in adulthood, and that one day I could "get away". (1292, 2012)
Eleven per cent of respondents did not find out they had been adopted until they were 21 years of age or older (see Table C2), and described the effect of this discovery at the time, as well as throughout the subsequent years:
Shocked, disbelieving, foolish, sense of self identity shattered. (435, 2012)
When I found out I was adopted, it came completely out of the blue as a note on a birthday card sent from an aunt [by marriage], telling me that although I was adopted, I would always be her nephew. From this point, my life was shattered; the life I had been living up till now was a complete lie. (131, 2012)
I had just told my parents that I was leaving home and my father said, "I suppose you know you're adopted". (40, 2012)
It was as if my history was no longer mine. All that I knew was no longer true. I sought counselling, which helped somewhat. (316, 2011)
As if I had been hit between the eyes with a Mac truck. It meant that my entire life up to the age of 49 was a lie. It was also badly managed by the department. It took approximately a year to begin to come to terms with it. During this time, I discovered that there was nothing in Australia to support people who find out later in life. It is a very different experience of adoption to knowing when you were a child. (1391, 2012)
Even though I didn't know I was adopted, the fact impacted on me because my parents tried to hide it from everyone. This led to them avoiding most members of the extended family. (40, 2012)
Late discovery adoptees have a unique level of complexity to their stories, and some of these issues will be discussed in greater detail later in this chapter.
Family discussion
Although not specifically asked in the survey, in response to a number of the free-text response items, some participants mentioned how their adoption had been discussed within their family while growing up. For many, it was a very open topic and this normalised their experience of being adopted:
It was always talked about. (338, 2012)
They [adoptive parents] introduced the theme of adoption in a conversational way, so I just grew up knowing about it and it felt quite normal. (890, 2012)
It was an ongoing conversation my whole life and my parents were very open about it. (698, 2012)
I do not recall ever being told. I just always knew, as it was freely discussed within my family. (727, 2012)
It was part of my story, told to me as a very young child. It was never a secret within my family or outside of it. (728, 2012)
I can't ever remember being told for the first time. My parents made it very clear that my brother and I were adopted and that it was OK to talk about it and ask questions. (959, 2012)
However, others who knew from a young age that they had been adopted reported that there was an expectation that it would not be discussed, or that it had to be kept a secret outside of the immediate family:
I was made to feel special - most parents just have children, but I had been chosen. I was asked to keep it private, so it was a mixed message. I didn't realise until I was older that my parents were probably embarrassed at their inability to have children and they felt it reflected on them. Whereas when I was younger, I thought it reflected on me. I associated shame with keeping it quiet. (1410, 2012)
I didn't understand it, though I was told not to tell anyone about it. So that made me feel that it wasn't something good. (1646, 2012)
This type of experience was also regularly discussed in the focus groups:
I assume they told me I was adopted when I was very young as I've always known, but it wasn't a topic we talked about at home. And when things came on TV [about adoption], I just felt bad for them and bad for me. (Adoptee, Victoria)
I was told that I was adopted but then never felt comfortable discussing it. It was sort of like, "Let's just pretend you're not adopted". (Adoptee, Victoria)
I was pretty much not allowed to discuss adoption when I was growing up, as my adoptive mother would get upset and cry. (Adoptee, NSW)
I don't remember being told. I always knew, but it wasn't discussed. If I did bring it up, there was usually a guilt trip from mum to let me know I shouldn't be talking about it. (Adoptee, Victoria)
I think I would have been in complete denial about having any problems about being adopted if it wasn't for my best girlfriend growing up who was also adopted [inter-country adoption]. So she always had major identity issues, but was always allowed to talk about it. They were always talking about adoption in the house because her older brother was also adopted. Because I spent so much time at their house, I think that helped me in a way process my own adoption stuff without having to talk about it at home. (Adoptee, Victoria)
For a smaller number of study participants, their adoptive parents still perpetuated the façade that their children had been born to them, which has had ramifications for how these participants currently view themselves and their relationship with their adoptive parents. As two focus group participants shared:
I feel like I'm cheating on my parents even just being here today. I'm cheating on them right now. (Adoptee, Victoria)
It's difficult, because it's secret. I've had to keep a whole other part of my life completely secret from my parents. I was very angry and still am angry with mum and dad. For their secrecy and the inability to put us first basically. (Adoptee, Victoria)
There appears to be an association between the age at which study participants found out about their adoption and how openly adoption was discussed, and their levels of wellbeing, both growing up and now. That is, the earlier they knew and the more openly and freely discussed adoption was as a topic within the adopted family, the higher the level of wellbeing of the adoptee. These links are examined later in the chapter when we discuss participants' wellbeing.
7.5 Circumstances of adoption
Survey respondents were asked whether they were aware of the reasons that led to their being placed for adoption, and if so, to describe these reasons to the best of their knowledge and understanding. Respondents were not specifically asked to identify where they obtained this information (whether from their adoptive parents, their family of origin or elsewhere); however, we assume that the responses are based on information from a mixture of sources.
Seventy-nine per cent of those who responded to this question (n = 813) said that they had an awareness of the circumstances that led to their adoption (see Table C2). For these, the most commonly reported reasons were:
- family pressure for their mother to place them for adoption (31%);
- stigma attached to being an unmarried mother (27%);
- their mother's age (26%);
- their mother had wanted a better life for them, which she felt she was unable to provide (10%);
- their mother could not afford to care for them (10%);
- the pregnancy was a result of an extramarital affair and there was no option for their mother to keep them (10%);
- no support from their father (7%);
- the pressure of social stigma was too much (7%); and/or
- their mother "did not want them" (7%).
Other reasons included general lack of support (6%); pressures applied by others in positions of authority, such as hospital staff or members of a church (6%); their mother felt they had no choice (5%); or the home environment was unsuitable, unstable or unsafe due to family violence, drug or alcohol abuse or mental health issues (4%). Another 4% said that they were placed for adoption as the pregnancy was a result of rape and/or incest, and 3% understood that their mothers had been victims of forced adoptions. Just 1% described their mother's decision to place them for adoption as being her own informed choice.
Qualitative accounts in the focus group discussions provided some further insight into the understandings that participants had about the reason for them being adopted:
So they all met together and then they all had a meeting about the fact that she was pregnant. Her mum went nuts, they went to the church for some advice. The church gave them a list of the maternity homes, and she was locked up in the home for nine months and had no contact with the family at all. She said after she gave birth to me, she wasn't allowed to see me, but snuck into the nursery. She went into that room and they gave her the adoption papers to sign and, "Do you understand what these mean?" And she said, "No, I don't understand what these mean". But they badgered her until she signed. (Adoptee, Qld)
Focus group discussions also provided us with information on the reasons for their adoptive parents adopting them. The most commonly talked about reasons were infertility, wanting a child to balance the gender of their existing biological child(ren), or to save their marriage. Some participants told us that their adoptions had occurred very rapidly:
My adoptive parents have three sons naturally and mum kept talking about wanting a girl for many years. So they applied to adopt a baby girl. In 1972, because so many babies were being given up to adoption, basically seven weeks later, they got a call that I was available. (Adoptee, Victoria)
I was adopted to save a marriage, but the marriage broke up when I was five … So for me then, it was my mother was 29 and made to believe she couldn't rear me, but I ended up five years later being reared by a man who was rearing two other adopted children on his own in the 60s. My [adoptive] mother had bipolar and she had the boyfriends. So I couldn't have friends when I lived with her because my mother was the "slut of the street" … and when I lived with my father, I couldn't have friends because he was a man rearing children on his own … And because of the society view - it views you in your education, your standing in the community. (Adoptee, Qld)
My adoptive parents had three biological sons before deciding to adopt a girl. (Adoptee, NSW)
I was never good enough for my adoptive family as I was a replacement for an older child who died suddenly. (320, 2012)
7.6 Childhood experiences
Relationship with adoptive parents
In the initial version of the survey, which went live in August 2011, the question about adoptee's views of their relationship to their adoptive parents was asked about both parents in a single question (n = 140) (see Table C11). After revisions to the survey instrument, which was released in December 2011, respondents (n = 683) were asked their views about each adoptive parent separately.
Overall, respondents to the question about both adoptive parents described the relationship with them as being either good or very good when growing up (54%). For those who responded about their adoptive parents individually, 26% had a poor or very poor relationship with their mother, and 18% had a poor or very poor relationship with their father when growing up.
Focus group discussions showed a broad range of perspectives regarding the quality of relationships with their adoptive parents and other family members while growing up, from extremely positive and loving, to the adoptees being subjected to physical, emotional and/or sexual abuse. These experiences will now be discussed.
Positive experiences
For many study participants, on average, their adoption provided them with affirming experiences throughout their childhood as well as now (see Table C11). For some, their reasons for participating in this study were to communicate how positively they viewed their experiences growing up, and the normality of simply being in a family that is supportive and loving, regardless of how it originated:
I have had a wonderful experience of adoption. My parents were very open about the adoption and always framed it for my brother and I in a positive way. I believe that adoptive parents play a vital part in helping an adopted child to develop a positive identity and self-image. One that encompasses both their birth heritage and their adoptive family. My family is just as real as any other family, and the bond is just as strong, regardless of the lack of biological ties. (698, 2012)
I wanted to complete this survey to show that adoption can have a positive impact on a person's life and does not necessarily have negative consequences or lead to difficult emotional issues. (727, 2012)
It has only ever been positive for my family, which I know is a rarity. My birth parents married a few years after having me, so I have three siblings as well as the brother I grew up with. My birth father always calls my adoptive father on Father's Day. My children have extra grandparents, cousins, aunts and uncles and great grandparents. It has been readily accepted by all concerned and, despite a few hurdles early on, it has been a positive experience. I like to think that I am loved by two different families who, together, become my one big family. (18, 2012)
I grew up feeling extremely special and very much wanted and needed. (64, 2011)
It hasn't affected me like so many other people it has. I have had an awesome and supportive upbringing. I have a close family and very supportive friends. Yet there are others out there who haven't had this. (73, 2011)
I'm a very lucky person. I have been loved and treasured all my life by my parents, grandparents, aunts/uncles, etc. I've never felt not wanted - only loved. (85, 2011)
I have no negative issues from being adopted. I was raised in a very loving environment so I was very appreciative then and now. (303, 2011)
However, it should also be noted that there is a distinction between having had a positive experience of childhood and whether or not study participants experienced any negative effects as a consequence of being adopted. The two are not mutually exclusive. This subject is discussed in more detail in section 7.7.
Negative experiences
Just over half of the adoptees reported a wide range of negative experiences, including being treated differently and feeling different to the adoptive parent's biological children, never feeling wanted, and living with secrecy and lies and even abuse:
I never felt that they accepted me for being different. I wonder if unconsciously I was trying to fit in for a while. I think I'd given up myself in order to belong. We had to go our own ways, or I had to give up a big part of myself to be part of the family. I wish I'd been stronger and gone, "Stuff you, this is how I am". (Adoptee, Victoria)
I never received a cent from those two. I asked for help once, never got it. I was never treated like a daughter. (Adoptee, Qld)
I'd had a great upbringing and good school etc., but to me, it's not about that. It's more about the feeling that I didn't belong. It didn't matter if I went to a private school or whatever, because I still didn't belong … So in some ways, I would have preferred to stay with my natural parents and deal with whatever life they gave me. (Adoptee, Victoria)
I felt different from my brother and sisters who had not been adopted. I felt as though I was welcomed, but didn't really belong. (834, 2012)
This treatment extended to attitudes from the extended family members of some participants:
My grandfather said, ever since I was a tot, "You are not blood. You will get nothing, but I will look after you until you go into the workforce or whatever you want to do". (Adoptee, Qld)
There were parts of the family where we were treated differently because we weren't blood. (Adoptee, Victoria)
There was a difference, however, between feeling lucky or special and being told they were lucky or special, which for many study participants subsequently led to feelings of needing to be grateful for something:
People would come up to me and say, "You don't know how lucky you are". Lucky that what? They put some clothes on my back? (Adoptee, Victoria)
We were told by my adoptive parents that we were special - I did not feel special, I felt different. (679, 2012)
The conflicting messages, where people are saying you are so lucky to be adopted into this great family, that had me think, well what was so bad about those people, and therefore what's wrong with me because I'm a part of them? (Adoptee, Victoria)
I always knew, but when I was young, I didn't really understand what it meant. I remember being told constantly that I should feel very lucky. (558, 2012)
I always remember feeling like I was acquired, like one acquires something they want. With that comes the feeling that you are expected to "be" something particular for the person who selected you. (1063, 2012)
Participants spoke about the stigma associated with being adopted. Comments were made such as "coming from tainted/bad blood", or being "painted with the same brush as your mother":
If I ever did anything wrong, it was because I was adopted and had "bad blood". It was brought up all the time on family outings, in front of the neighbours and relatives. (1662, 2012)
I have always not felt part of my family, as my brother was their blood and I wasn't. (182, 2012)
I was a little young to fully understand, but there was a stigma with this in the 70s, which made me sad. (1485, 2012)
I was getting chastised one time and was crying for my "mum". [A woman] said, "[name] isn't your mother, you're illegitimate. Your mother was no good and you'll turn out no good too". (1763, 2012)
Then the kids started to bully me and make fun of me and so I actually turned around and said that I had lied [about being adopted] - I just did it because I was wanting attention … That sense of shame that something was wrong. (Adoptee, Victoria)
I lived my life being told that God didn't want me because my natural mother was unmarried. These people were extremely religious. I was made to live my childhood praying and asking God for forgiveness for being conceived, and constantly told that he wouldn't forgive me anyway. (1771, 2012)
The names I was called and the way I was treated at school - it is a real surprise I didn't become extremely violent. (Adoptee, SA)
I told my best friend and she told other people, and I remember feeling ashamed and felt I had to hide the fact that I was adopted. (1680, 2012)
I was devastated that what the other kids at school were saying about me was true. I felt that I didn't belong to anyone. (1744, 2012)
Of particular concern is that quite a number of participants reported suffering abuse in the adoptive family environment.
Note: The following accounts contain information that may cause distress to the reader. We advise that those who have been affected by past adoptions or are sensitive to trauma issues may wish to avoid reading them, or ensure that appropriate support is available.
Adoption has been the single most damaging event in my life. It robbed me of the knowledge of who I am, leaving me to live in a limbo of disconnectedness - a place of not belonging, adopted into a dysfunctional family where fear and abuse were the only parenting skills used. I was passed into institutions as a flawed and failed human being. With no follow-up on adoptions into my family, the abuse went undetected and any aberrations in behaviour were seen to be the child's fault. (16, 2011)
What more information do you want? I was socially, sexually, legally, medically, physically, psychologically and financially abused. I was left with nothing. Not even clothes or a home to live in. I had no education and I had to fend for myself. Had I been left in the hands of my adopting family or the hands of the government, I would have died a long time ago. (35, 2011)
I was told by my adoptive parents that I was someone else's rubbish. (134, 2011)
In my experience, my adopted parents should never have passed the psychological test, if they even had it back then. I was told over and over that they should have left us in the orphanage, that I was "A wog or a coon" and I didn't belong to them. I was kicked out of home at 15 and told to go live in the gutter where I belong. (189, 2011)
There have been many times where I wished that I had been aborted rather than adopted. Not to sound dramatic, yet the experience has diminished my faith in both biological responsibility and adoption screening of potential adoptive parents. The adopted child is left to carry this burden. (314, 2011)
I was stolen from my mother who was unwell. I was given to people who wanted a daughter not a son, but were made to take me and wait two years to adopt a daughter. I was not wanted and was severely abused, unloved and disinherited. (359, 2011)
Some respondents who had not been placed with a family but remained in the care of the state reported that they had been subjected to medical experimentation, while others believed that they had been included in activities related to eugenics:
Orphaned boys were seen to be second class and government advocated to punish them. I was punished and tortured in a eugenics program by government. (14, 2011)
Many of those who had experienced abuse and neglect within their adoptive families felt that the issue of how their parents had been screened prior to adopting, as well as the lack of follow-up or monitoring by those who had organised their adoption, was of particular concern:
I strongly believe that more care should have been taken in the process - more home visits and involvement. Had that happened, then I strongly believe I would have been or should have been removed from that house. They adopted because back then, couples "had to have a child" and she had already had two miscarriages. [My mother] got a child for all the wrong reasons and was not able to provide. (51, 2012)
Where was the government's responsibility to ensure that the parents you were going to were safe? (Adoptee, NSW)
There couldn't have been any background checking, because there were quite a lot of longstanding issues before I was adopted into my family. (Adoptee, Qld)
My adoptive parents were shocking. My adoptive mum had a long history of mental illness and alcoholism. And they split up a year or two after me being adopted to them. And then I went through a series of foster homes, things like that. And I sort of shake my head and think: how the hell - who the hell - was making these decisions? (Adoptee, Qld)
Although a significant proportion of adoptees responding to our survey described positive personal experiences from the closed adoption period, this does not in any way minimise the significant number of adoptees who reported that their experience had been negative, and whose descriptions provide evidence of a range of ways in which closed adoption and the way it was practised in Australia until the late 1970s and early 1980s caused harm, distress and other ongoing effects. These effects are discussed in further detail below.
7.7 Effects of childhood experiences of adoption
The comparisons that come out whether people are better off adopted; I think that's a useless argument and I don't see any point in it. The issues are there. There are issues with being adopted. Whether we would have been better off or not is really beside the point, because you can't really understate the emotional ramifications that are lifelong for all parties. (Adoptee, Queensland)
The information presented thus far from study participants shows a relatively equal mix of positive and negative experiences. There are complexities across and within these experiences. Similar to mothers who participated in the study, people who were adopted were keen to reflect on their past experiences in detail in order for us to gain an understanding of how these experiences have played out over the course of their lives.
When asked whether they believed being adopted had had any effect on their health, behaviours or wellbeing while growing up, 69% of adoptee survey respondents agreed (see Table C2). (Six per cent did not know they were adopted until they were an adult, so could not respond to this question.)
The following section presents information on the effects of their childhood experiences of adoption. Firstly, we examine some common themes that emerged in both the survey results and focus group discussions, which related to issues of secrecy and lies, identity, abandonment, worthiness and attachment. These issues were described not only by those with negative experiences of growing up as an adopted child; challenges with identity and belonging were frequently presented by study participants, regardless of whether they had a "textbook perfect" upbringing, a relatively "normal" upbringing, or whether they had been subject to varying levels of abuse and neglect within their adoptive families.
Secrecy and lies
One of the most common themes to emerge from adoptees in relation to the effects of their adoption was the issue of the secrecy and lies that have been told over the years, with much of this still happening. Even though many knew from an early age that they had been adopted, they were often not allowed to talk about it or, if they did, their adoptive parents were elusive with the details. Some were even told that their mother was dead, which was later found out to be untrue:
That secrecy has continued. That sense of shame that something was wrong [with people knowing]. (Adoptee, Victoria)
I had been told, and believed growing up, that my birth mother had died during birth. I have since found out that was not the case and that she was only a teenager who was forced to give me up. (767, 2012)
Respondents said that they need to know the truth, and that they have been hurt by the dishonesty. They have felt cheated and invalidated; for example, some found out years later that others knew of their adoption when they didn't - a number mentioned that "everyone" appeared to know except them. This veil of secrecy has led to a loss of trust, a need for acceptance and fear of rejection:
I think the biggest thing for me was finding out how many people had known. As in: all of my extended family, in-laws that came into the family were always told, my husband was told. I was never to be told. (Adoptee, Victoria)
Every child I grew up with in my life, went to school with - and some of them are still my best friends - every single one of them knew I was adopted. Every single one. And they were under dire threats from their parents that if they let me know they would be in so much trouble. (Adoptee, Qld).
Some respondents who attended the focus groups said that participation in the current study was the first time they had discussed their adoption with anyone, and many appreciated the opportunity to speak with others who had had the experience of being adopted:
I have no real complaints about how I was treated by my adoptive parents. But I don't like some of the processes involved with this. I don't like the lying, and I don't like the fact that I don't trust any human being because I don't know who has got a hidden agenda or who knows something that I don't know. (Adoptee, SA)
That's where I find being adopted the worst thing. Because we spend our lives lying to each other and everyone around us. But we trust this piece of paper that someone wrote in two seconds, and basically in a lot of cases, they [mothers] didn't write it. When I first saw my piece of paper, it told me my father was four years older than he was and he had a different name, and all these things that weren't true. So we base everything and say, "Well, that piece of paper is going to be the truth", when actually, nothing has been the truth. (Adoptee, SA)
It's getting harder when you get older, because when you grow up you are told to lie in a way. I feel like I was brought up to lie about everything. I had a very good upbringing, but they didn't want to know really what I felt. So I gave them what they wanted to hear. (Adoptee, SA)
I wasn't allowed to talk about it, so it was completely closed and I had to pretend I was theirs. They pretended if we met anybody. I mean, their friends knew, but never once was it said out loud. (Adoptee, SA)
I felt different growing up and was ashamed of being adopted. My parents were trying to protect me and strongly suggested that I kept my adoption a secret. This had a big effect on my confidence. (40, 2011)
Identity
Two of the key themes also to emerge were issues relating to identity and belonging; that everyone has the right to know who they are and where they come from. Not having information about themselves was an issue for many, as was feeling like no one else understood what it was like to be adopted (particularly if they had not had the opportunity to discuss this with anyone else). The added complexity of knowing how to tell their own children who they are was also raised as an issue relating to identity for many in this respondent group:
I do believe it is the sense of belonging that has been a void. You do not always look like your adoptive parents. I would also not like to be the dirty little secret in my biological mother's life. By not acknowledging my birth to my siblings, I feel there is a certain shame about that time in her life. (596, 2012)
I had to pretend I was something I wasn't. I think that's really unfair, no matter how well you get on with your parents and your siblings. I love them, they were my parents, they were lovely to me. But I was always upset with them because I was a lie. I still have to lie today. (Adoptee, SA)
There were various reports of feeling different (e.g., "not feeling like I fit", "I was different to everyone and couldn't make sense of myself within that [family] unit"), and wanting or needing to feel a sense of "belonging somewhere in the world - making sense of where I fit":
I just need to accept that as an adoptee, I am a mixture of my birth parents and my adoptive parents. I have genetic, emotional and personality traits from my birth mother and have learned personality traits from my adoptive parents. Unfortunately, that makes me feel that I don't really fit with either parents and I just have to accept that. (218, 2012)
The feeling of not really belonging. (138, 2012)
I felt I didn't belong. My parents didn't understand me as I was so different - the way I thought. They just thought they would teach me to be like them, and I was different. I lacked self-esteem when I was young and didn't know why, and never felt I fitted in with school friends. (114, 2012)
I thought I was different to other kids. I worried that I had an intellectual disability and that was why I was adopted out. I didn't feel like I belonged to my extended family on my maternal side. I didn't look like anyone in the family, so I often felt alone, not part of something bigger. (152, 2012)
Some felt they were cut off from identification with any group in society:
We are not validated as people. We were given up because our mothers had to because of society's wishes. And we were adopted for a purpose, to fulfil a need in that family. And then if we didn't perform? You were discarded. (Adoptee, Qld)
I always felt different and alienated from everybody else … because they weren't adopted. (288, 2012)
I always felt that I lived a side-saddle life - not quite belonging anywhere, with few rights to access things I saw others access. (267, 2012)
Others had less of an issue with their sense of personal identity:
Being adopted is just a part of me that other people find interesting, but it is not who I am. (168, 2012)
The effects also varied according to when respondents found out that they were adopted:
And I think it's a human right for everyone. Everyone should have the right to know who they are. I think every person should be told they are adopted from a very early age. Because hearing these stories and hearing stories from late discovery adoptees - the lies and deceit. (Adoptee, Victoria)
Because I have always known, I believe that this has made me better adjusted, and it is others [who weren't told at a young age] that have trouble dealing with adoption. (297, 2012)
For late discovery adoptees in particular, the issue of identity was significant, as many felt that everything they had known about themselves to that point in time was untrue:
Absolutely let down. I had led a lie for my first 24 years of my life. Upon disclosure, a big black hole opened up for me - "Who was I really?" (1053, 2012)
Although I did not know I was adopted, I always felt different from the rest of the family. I did not think or behave within the norm for that family. I felt I did not belong and was constantly confused about the way I was treated by my parents. Greater expectations placed on me than my brothers. (401, 2012)
I felt my life had been a lie. (131, 2012)
Devastated. My whole life was a lie. I never got over it. (1138, 2012)
Abandonment
A number of participants reported feelings of abandonment ("I wasn't wanted") and the confusion of rationalising in their head that their mother didn't have a choice, but in their heart not being able to believe it ("She could have tried harder to keep me"). Some felt that if they had more information on the circumstances of their adoption, then it might lessen the feelings of abandonment:
I need help dealing with the issue of feeling abandoned by people. I have a low self-esteem because of this and I feel angry because I am stuck in this thought pattern. (255, 2012)
As an adopted person, you grow up with a feeling of insecurity and abandonment. As an adult, you can rationalise, but as a child you can't and you don't understand. (316, 2012)
I had always been told as a child it meant that I was special. As such, I felt privileged. As I grew older, this turned to feelings of rejection, as I could not understand why my mother "would not want me". (821, 2012)
I imagine most adoptees would feel some sense of rejection, even if they were able to understand the mothers' reason for letting them go. (1138, 2012)
Adoptees also talked about the "ever-present fear" of being sent back or given away ("If I don't behave, I'll be abandoned again"):
Children discarded by their own mothers, unlovable, unwanted … Believing we are less than deserving of respect, love, safety and truth, we play the game of fitting in to survive. We adapt to our new environment, pretending everything is OK for fear of being abandoned and rejected yet again. (Adoptee, Qld)
I often felt terror and feeling abandoned when left alone. (147, 2012)
Some participants spoke about how not knowing what happened to them between the time they were born and when they were placed with their adoptive parents plays on their minds:
She wasn't allowed to hold me or anything … I was in hospital I think for a couple of months because I was underweight. That's a period of my life that I'm really worried about. Having had children myself, I'm so attentive to them when they cry and when you breastfeed them. I sort of think, well two months in a hospital - who was really there? (Adoptee, Victoria)
Gratitude
A commonly reported experience reported by adoptees in this study, was the feeling that they had to show gratitude/appreciation to their adoptive parents for "taking them". This often resulted in over-achievement and over-compliance:
I've always felt my entire life indebted to them; that I owe them a debt. And therefore, if anything's ever happened to my parents, I've been the one to support them … I just feel constantly that I have to give, I have to give back. (Adoptee, Victoria)
I thought I should be grateful of having parents who loved and looked after me, therefore I never liked to ask for anything and tried to be very good and keep out of trouble. (610, 2012)
I tried overly hard to please my adoptive parents. I built a strong imaginary world that I lived in a lot, and built barriers between me and others. I was independent, strong-willed and didn't ever want to rely on any one else. I didn't want anyone to see me as weak. And took rejection (even that everyday rejection in the school yard) very badly. I was hurt a lot and although I appeared to be confident and happy, I was often sad, and was very happy to stay away from other kids and read books. (354, 2012)
I felt unsure of my position in my family - felt I had to "earn" my place in my family, felt an obligation in fact for my life and that I somehow had to be grateful for my very existence and justify being here. I had to be grateful for my life and the sacrifice others had made in order to adopt me. (463, 2012)
I have a strong desire to achieve. I feel I always need to prove myself to be good enough. (288, 2012)
Although being told you were special/chosen was in many ways a wonderful experience for participants ("We chose you because you were the one that smiled"), this often led to pressure associated with needing to uphold a certain level of behaviour ("I always felt I had to be happy"):
Feeling of inadequacy and of needing to be grateful someone had taken me, and had better be good and nice and likable. (357, 2012)
As previously mentioned, others, when talking to the adopted individual about their circumstance, often used the term "lucky". Many respondents felt this was a misnomer:
The terminology that people used for children, as being "We saved you". An adopted child's self-esteem is already low … You have a parent who says, "I saved you; you owe me". And now I am going to do something to you in a way that is morally wrong. The whole terminology leaves you already set up to be abused, whether it's by the [adoptive] parent, or by your spouse, or by your workplace or whatever. Because you see yourself somewhere else down the rung, and that you owe society just to breathe. (Adoptee, Queensland)
Many respondents questioned whether the adoption was done in the best interests of the child:
I remember yelling at someone saying, "Well I am just a parcel! No one asked me do you want to be given away? What's the right thing for me?" They talk about it being the best thing for the child, but that's bullshit. (Adoptee, SA)
It's a right to a healthy upbringing, not a privilege because we're adopted! (Adoptee, Queensland)
Worthiness
The flow-on effects of feeling like the "forever grateful adoptee" or being "unwanted" manifested themselves through many participants having difficulties throughout their lives with feeling worthy of anything good. This has affected many areas of their lives, including their relationships and career:
If only I could feel worthy … I am respected at work and loved by my husband and children, but I still feel like I belong on a scrapheap and one day everyone will realise that. (351, 2012)
What I need now is to find the courage to be the person who was "discarded" and honour myself as this; to "accept" myself and find a way to shake off the shame and the fear of being misunderstood. (573, 2012)
My biggest issue that has resulted from being adopted is a low self-worth. If I wasn't worthy of being kept and loved by my birth mother, then what am I worthy of? This affects me every day; I don't deserve to look nice, have clothes that fit. (241, 2012)
When I was a teenager, I sought out the different side of life - the bad boys, the bad lifestyle, the drugs, the alcohol, the running amok. Not caring about what people thought because you don't feel like you fit into society. So I felt like I didn't have to act like I was in society. I didn't care about people because they didn't care about me. (Adoptee, NSW)
The desire to prove myself worthy all the time. (451, 2012)
Attachment
Attachment issues were common for study participants as a result of their adoption experience. Issues with attachment had an effect on some adopted individuals' childhood relationships - never getting close and trying to avoid being too clingy - as well as later on in life, such as their capacity to bond with their own children:
I intensely feared rejection and abandonment. I constantly needed reassurance that I was loved. I intensely feared making mistakes, any mistakes, to the point where it limited my ability to achieve. I had extreme difficulty making friends. I didn't trust people not to desert me. (704, 2012)
I have always expected a lot from my friendships. If they didn't give me as much as I was giving them, then I'd let them go. (Adoptee, Victoria).
I have been diagnosed with an attachment disorder. For me to try and navigate life, it's extremely difficult because I don't make attachments. I don't see love the way other people see love. For me, it's important that the government see that these are the ramifications and there are people who are out there that really need support. (Adoptee, NSW)
I didn't really bond at all with my own children. (Adoptee, WA)
I'm not sure if I'm properly connected in any of my relationships. (Adoptee, WA)
7.8 Support when growing up
Almost 39% of survey respondents said that they had not had any support relating to their adoption experience when growing up (see Figure 7.3 and Table C3). A further 14% said that they had not wanted or needed any support.
Figure 7.3: Sources of support when adoptee was growing up
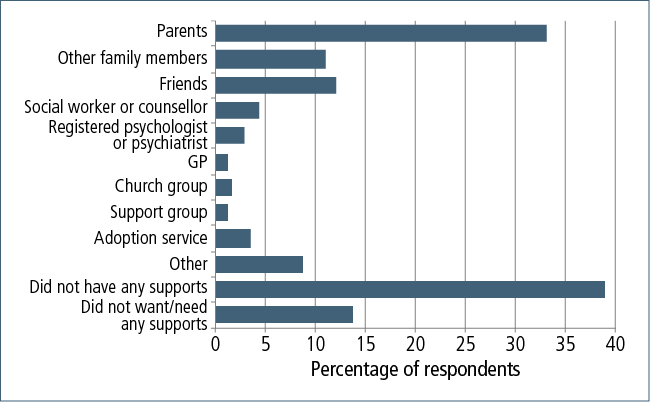
Parents had been the most common source of support, with a third of respondents turning to their adoptive parents for support. About one in ten respondents had received support from friends, and a similar number from other family members.
Emotional support was the most common form of support received overall, with almost half of the instances of support being of this nature (see Table C4). The other common form of support was general support and information (37%).
Well over half the instances of support were described as having been very helpful, with a further third somewhat helpful (see Table C4). Only a small number reported that the support they received had been unhelpful or very unhelpful (5%).
There can be many ways in which lack of appropriate and accessible support throughout the lifelong journey affects adoptees, as discussed below.
7.9 Effects over time
It's huge and I think we need to have a voice and say, "This is what it did to us". (Adoptee, WA)
Many of the effects experienced by survey respondents during their childhood have carried over into adulthood. Even though a large proportion of respondents had very positive experiences of growing up, they often still faced challenges with their identity, a sense of belonging/"fitting in" and attachment issues.
Relationships
I've not had my own family - I'm sitting in a goldfish bowl. (Adoptee WA)
Many respondents referred to the effects of being adopted on their capacity to establish and maintain meaningful relationships with partners, parents and their own children. The effects of feelings of abandonment, rejection and worthlessness compounded into more complex issues when trying to navigate their relationships:
There is no doubt that forced adoptions and unethical practices did occur, and I cannot imagine the loss that the mothers felt. Many went on to marry and have other children and, while that child could never be replaced, formed a family unit. However, for me, I lost my identity, have felt detached all my life, have great difficulty forming relationships, experienced family rejection - from those who believed that adopted children were not "true" relatives, and then by my birth family - believed that my mother was a terrible wayward woman and so on … I have struggled with many acceptance issues throughout my life time. (Adoptee, Perth)
I continue to this day to question my self-worth and don't believe anyone will love me unconditionally. I have a "hurt them before they hurt you" mentality. I suffered many more abandonments post-adoption. (Adoptee, Victoria)
Feelings of not belonging and not being good enough. Difficulties in relationships and trust issues. (143, 2012)
Some participants talked about the complexities of adoption and how it affects their partners:
I think he struggles a little bit with it. He's got a big family and I was always a part of that family. But for him to be a part of my family, he's not sure how to fit. And he feels quite threatened. (Adoptee, Qld)
Because he doesn't understand my perspective because he has had this beautiful life with two fantastic parents. But [my adoption] is still affecting me to this very moment. He doesn't see that, he just thinks, "You're adopted, you had a good family, get over it". (Adoptee, NSW)
One participant who is both an adoptee and a mother forced to relinquish her own son as a teenager, described her adoptive mother's reaction to her own reunion with her son:
When my own son came back into my life, my adoptive mother said to her natural son, "Why do I have to meet him? He's not my grandson". And if he is not her grandson, then what am I? I am not her daughter. (Adoptee and mother, Qld)
Having children
Almost half of the respondents said that their adoption experience in no way affected their decision to have children, and a further 15% said that it only had a small effect (see Table C2). In contrast, just over one-quarter of respondents (26%) said that their adoption experience had either completely or mostly influenced their decision to have children. Respondents were not asked whether the influence was positive or negative.
Although a large proportion of respondents said that their decision to have children was not influenced at that time by their adoption experience, many did report the subsequent effects that they experienced once they had children.
During discussions, some respondents noted that they were worried about their capacity to bond with their own children, or of being overprotective. They noted that there are ripple effects on their own children - "it does not stop with us". Others felt that their own experience had led them to be very open with their own children:
I feel my own personal experiences as an adopted child has been of great benefit to my own children, who have grown up with a much better sense of self because I have ensured that they have access to information about their biological parents and family, and we can talk very openly about our experiences and feelings. (114, 2012)
I know [the effect of adoption] manifests a lot more clearly then, when you have your first kid. When I had my own child it was ridiculous because it was your first blood. And that's undeniable. If people were ever in doubt what adopted people feel, they just have to analyse what adopted people feel when they see their first child. It's not tangible - it's not necessarily something that can be seen - but it is no less important. (Adoptee, SA)
I had two boys first and that was hard enough looking at your own flesh and blood for the first time. But when I had a girl, I just went mad. I wouldn't let her out of my house. The hospital would go mad with me because I wouldn't let her out of my sight because I was sure someone was going to steal her. (Adoptee, SA)
Normalisation
Dealing with societal attitudes of curiosity, pity and awkwardness is something else many respondents mentioned experiencing, both while growing up as well as throughout adulthood. This has been described by some as an incredibly frustrating "burden" they have had to carry throughout their lifetime:
You just want to be like everyone else, but you never felt that way. Our view of ourselves is that we're not normal. I've always felt like I was not normal, there was something wrong with me. I don't fit into society, I don't fit into family. I just don't fit. (Adoptee, NSW)
Most people say when you tell them, "Oh, but you're OK aren't you? Aren't you traumatised?" They all look at me like there should be something wrong with you. People expect you to have some sort of mental problem if you're adopted. (Adoptee, Victoria)
I would really like to be able to say that if I'm just out at dinner or whatever, and someone says something about family, that I can just say XYZ about my adoptive parents. I would like to be able to put that on the table without people saying anything that's either positive or negative, one way or the other. (Adoptee, Victoria)
I find myself having to manage their reaction, their response. (Adoptee, Victoria)
I had this thing the other day at work discussing the family tree at the lunch table. It's just like I wanted to crawl up on the table or run away and hide. No one asked me about my family tree. (Adoptee, NSW)
I came along today and I guess I didn't realise I would be meeting up with people. Which is nice, because you always feel in a separate class. People still look at you - their eyes go all concerned when you say that you are adopted. So it's nice to meet people. (Adoptee, Qld)
Life events
As one of the ways to gain an overall sense of the effects that adoption has had throughout their lives, respondents were asked whether they believed their adoption experience had played any part in contributing to a series of common life events.
Fewer than one-third (29%) said that none of the items listed had been affected by their experience of adoption (see Figure 7.4 and Table C14). However, 38% indicated that their adoption experience had affected their marriage, and nearly a quarter (22%) said that their experience had played some role in their experience of separation or divorce. Disruption to employment and schooling was also commonly reported (22% and 20% respectively).
Figure 7.4: Whether adoption experience affected adoptees' experience of life events
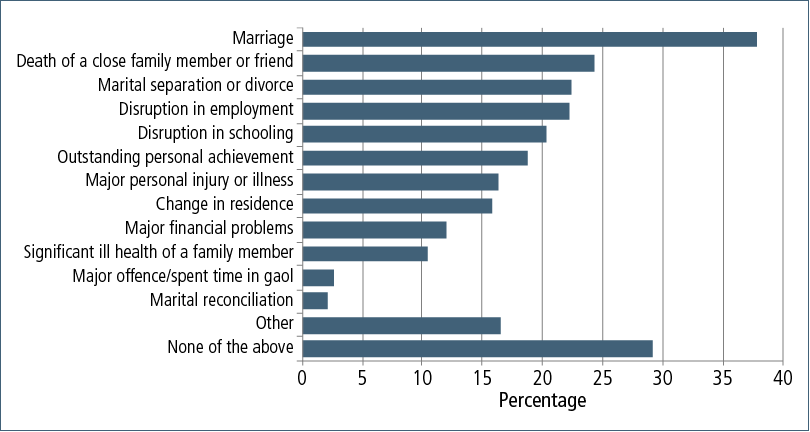
Wellbeing
Pretty much every aspect of my life is coloured in some way by adoption, simply by virtue of the fact that it has made me the person that I am. In terms of mental health, being reunited with some of my natural family has definitely helped me consolidate who I am as a person, relieved some of the cognitive dissonance. But I am still left with the scars that are inevitably left by being given away by your mother. I still fear abandonment by friends and my partner. Even though intellectually I know that they love me, I always dwell on little things that I have done that might drive them away. I have crippling bouts of depression when I just can't seem to leave the house. If I force myself to attend a function that I have been dreading, I will get a massive headache or feel nauseous. But since my reunion, I find that once I get to the function I am usually OK. (Adoptee, Victoria)
A number of measures of wellbeing were included in the survey, as described in section 3.3:
- the shorter version of the World Health Organization Quality of Life instrument (WHOQOL-BREF);
- the Kessler Psychological Distress Scale (K10); and
- a life satisfaction scale, based on the one used in the HILDA survey.
WHOQOL-BREF
For the two single-item measures: "How would you rate your quality of life?" and "How satisfied are you with your health?", higher scores indicate higher levels of wellbeing. Overall, survey respondents rated these items only slightly lower than the Australian norms (Table 7.1). However, across the four domains, only the environment domain had respondents scoring similarly to the norms. For the other three domains, the scores were significantly lower.
| Domains | Australian norms | Survey respondents | ||
|---|---|---|---|---|
| Scale score | SD | Scale score | SD | |
| Physical | 80 | 17 | 56 | 13 |
| Psychological | 73 | 14 | 51 | 9 |
| Social relationships | 72 | 19 | 59 | 24 |
| Environment | 75 | 14 | 72 | 19 |
| Overall rating of quality of life | 4.3 | 0.8 | 4.1 | 1.0 |
| Overall satisfaction with life | 3.6 | 0.9 | 3.5 | 1.2 |
Note: SD = standard deviation.
In Table C15, the scores for respondents with a variety of characteristics are examined. The following points emerge:
- Partnered individuals (married and de facto/same-sex) had slightly higher scores on average than other respondents.
- Full-time workers scored a little higher than part-time workers, who in turn scored higher than those not working.
- Higher levels of education were associated with higher scores.
- Generally, the older the age at which the person found out he/she was adopted, the lower the scores.
- Those who believed that being adopted had not affected their wellbeing while growing up had scores that, compared with other characteristics that were examined, were considerably higher than those who felt their wellbeing had been affected.
- Those who had had some support for their adoption experience while growing up had higher scores than those who had no support, whereas those who had had support since becoming an adult, scored slightly lower on average than those who had not had support.
The Kessler Psychological Distress Scale (K10)
As can be seen from Table 7.2, the survey respondents show much higher levels of psychological distress than those in the 2001 National Health Survey. Of particular concern is that close to one in five respondents was likely to have had a severe mental disorder at the time of survey completion.
| NHS male (%) | NHS female (%) | Adopted persons (%) | |
|---|---|---|---|
| Likely to be well | 85.6 | 79.6 | 54.1 |
| Likely to have a mild disorder | 8.3 | 10.6 | 17.4 |
| Likely to have a moderate mental disorder | 3.1 | 5.5 | 10.3 |
| Likely to have a severe mental disorder | 2.7 | 4.4 | 17.9 |
When these levels are compared across characteristics (see Table C16), the following points emerge:
- Levels of psychological distress appear to vary according to the age of the respondent.
- Distress levels were highest for those who had never married or were separated/divorced.
- Distress levels were highest for those not working and for those with lower levels of education.
- Distress levels were slightly higher for those who had had contact with birth family members.
- Those who believed that being adopted had not affected their wellbeing while growing up had distress levels that, compared with other characteristics that were examined, were considerably lower than for those who felt their wellbeing had been affected - so low, in fact, that they were very close to the NHS norms.
- Those who had had some support for their adoption experience while growing up had lower levels of distress than those who had had no support, whereas those who had had support since becoming an adult, had higher levels of distress on average than those who had not had support.
Life satisfaction
Around half the respondents scored their satisfaction with life very highly (8 out of 10 or higher) (see Table C17). However, 16% scored their satisfaction level as less than 5 out of 10.
The relationship between life satisfaction and the various respondent characteristics mentioned above showed similar patterns to those of the WHOQOL and K10.
Comparison with HILDA respondents is broadly possible, although the HILDA measure of life satisfaction has the scale ranging from 0 to 10.
Table 7.3 shows that our survey respondents rated their life satisfaction slightly lower than respondents in the HILDA survey. The difference at the high scoring end is mitigated to some extent by the fact that the HILDA scale has 11 points, rather than 10. However, there were considerably more respondents to our survey who rated their life satisfaction at very low levels.
| Score (weighted HILDA data) | HILDA a | AIFS study | |
|---|---|---|---|
| Adopted (%) | Not adopted (%) | Adopted (%) | |
| 0-4 (low) | 3 | 2 | 16 |
| 5-7 (moderate) | 36 | 31 | 34 |
| 8-10 (high life satisfaction) | 61 | 67 | 50 |
| Total percentage | 100 | 100 | 100 |
| No. of observations | 148 | 12,537 | 825 |
Note: a Data from Wave 8 of HILDA was used because this is the dataset that contains information on whether the respondent had been adopted.
7.10 Seeking information
A significant component of the study centred on people's experience of seeking information about themselves and family members from whom they were separated, as well as the process of search, contact and the subsequent establishment of new relationships (if this eventuated as a result of contact).
For many of the adopted individuals who participated in this study, this process related to formation of their identity, and search and contact experiences were identified as being some of the most significant in their adoption stories.
Almost nine in ten survey respondents indicated that they had tried to find information about their family of origin, even though just over half of them were worried that their adoptive parents would think they were being disloyal by doing so (see Table C5). In discussions, participants mentioned feeling guilty about their natural curiosity about their family of origin. About one in ten indicated that they waited until their adoptive parents had passed away before seeking any information, mainly because they were concerned for their parents and their reaction.
When asked how their adoptive parents reacted when told about their intention to search for information about their birth family, 20% of respondents said they did not tell them. Those who told their parents described the most common reactions to be: supportive (34%); anxious (24%); and actively encouraging (14%).
The complexities associated with this process for many of the adoptees in this study were substantial. The issue of divided loyalty being a factor in the original search process often did not subside once contact had been made and a relationship with birth family members established. We will have further discussion in relation to divided loyalties later in the chapter.
Barriers
Respondents identified a number of barriers to their attempts to search for information about both themselves and their family of origin, and to making contact.
Cost
The cost of accessing their records was one of the main issues participants raised as being a barrier to obtaining their personal information and that of their family. Fees associated with the search, sending of documents and other information have put considerable stress on many adoptees who participated in this study, and they expressed their frustrations with this issue:
Why should I have to pay for something that is my right to know? (Adoptee, Qld)
Access to my information is my right, not my privilege. I should not have to pay for that. (Adoptee, NSW)
I feel that I should be able to have all information about my birth, including my original birth certificate, without going to counselling or paying any money. (188, 2012)
I want easy, low cost access to information. (122, 2011)
I would also feel a lot happier if adopted people's records and information were available to them free of charge. That I had to pay for my own information disgusts me. (1682, 2012)
The cost of information … it was just all too hard. It was expensive, it was time consuming, it was stressful. There were just too many closed doors. (Adoptee, Qld)
I forked out my extra $100 on top of the 30 odd dollars for the birth certificate - just simply because I was adopted. (Adoptee, NSW)
Contact and information vetoes
Contact and information vetoes were an issue of contention on a number of levels within this respondent group. These issues mainly emerged during focus group discussions and included:
- frustration with birth mothers having contact vetoes and therefore adoptees not being able to access medical histories for their mother or father;
- the threat of legal/criminal action if they breached the veto;
- concern that vetoes are not effective given the current levels of accessibility to personal information on the Internet; and
- vetoes having sometimes been signed by the adoptive parents, not by the adopted individual, or there was no signature required when filling out the veto.
Generally your birth mother does not wish to be identified. The state government gives her absolute power over your life, because she not only blocks her identification, she also blocks the birth father's identification and any siblings identification … You're just as much a victim and just as much a human being as she is. What makes her better than me, in terms of being able to know who I am? (Adoptee, SA)
It's our children that suffer. My daughter and grandkids will never truly know their family tree either, or if there is any medical problems in the family. We don't get to know that. (Adoptee, NSW)
Inaccessibility of information
There were many issues associated with the difficulty of accessing information, such as the navigation of complicated systems and dealing with departmental staff. Study participants reflected that the current system often doesn't provide easy access to information, commenting on the ways in which it fails to take into account the significance of the information that is being provided to those who are seeking it. Respondents noted a lack of sensitivity to the effects that receiving this information may have:
Negotiation with governments and negotiating systems is not easy. And they re-traumatise people, I think, in having to get through what can be a difficult system, when people are already traumatised. The system needs to be made easier for people to use, and provided by the people who have the skills to help people get through it. (Adoptee, Qld)
Access to information, records and an original birth certificate without having to jump through hoops. You just give up sometimes, which probably isn't helpful for your psyche. (547, 2012)
A well-informed public service system would avoid the suspicion directed towards you when you present a Schedule 6 rather than a birth certificate as proof of identity. I had difficulty enrolling in teacher's college, applying for a bank account, bank loan, driver's license, passport and any other activity that required a birth certificate. (452, 2012)
Some phrased this in terms of human rights:
I want the restoration of my human right to full disclosure regarding who I am and how I got here. (53, 2012)
I feel that adopted children aren't given the same rights as biological children, and this is unjust. (107, 2012)
I would like to be able to access my genealogy and family history, and have the right to the base information that I believe is a child's right to have. (110, 2012)
For others, they expressed their frustration with having no information about their fathers, as fathers were often not included on their birth certificates. For some, their mothers either don't know who their father is, or refuse to disclose that information:
Information my mother has given me is unreliable and possibly incorrect. I just wish women were required to name a father back then, as it leaves me wondering about all sorts of scenarios. (113, 2012)
I would dearly love to find my birth father because recently I have become disabled and they are talking genetics. Unfortunately, my birth mother is not willing to help me do this. (48, 2012)
A couple of years later, I wrote a letter saying this is my birth right to have this information. In the same way you thought finding me was bigger than you, well this is bigger than me. (Adoptee, Victoria)
One area of particular concern raised by this respondent group, was the discovery that some of the information contained in their documentation is inaccurate. This has had a significant effect on them, as they no longer know what information about themselves and their family members they can trust:
I was OK with being adopted until I got my freedom of information stuff. To find out that your birth certificates were forged … She didn't sign [the consent], but whoever it was who signed, forged the paperwork and basically they covered their tracks by putting into Births, Death and Marriages with my mother's name - middle name first, first name second, with spelling mistakes in both. My mum wouldn't sign, she refused to sign, because I was born with a medical condition [and deferred adoption]. In the end they came in to her and said, "Because you didn't sign, we couldn't give your child an operation and he's died". For me, I don't believe the information anymore. I look at it and think, is this real or is it just forged like the rest of it? (Adoptee, NSW)
I would also like to be able to access my genealogy and family history and have the same right to the base information that I believe is a child's right to have. The law should not deny me or protect those who created what turns out to be a lie. In other words, the history I was raised with turns out not to be my history, but an adopted history. (110, 2012)
Facts about the circumstances of my adoption rather than the built narrative that I am given by family. Each story is presented as a fact, but is contradicting of other versions. (332, 2012)
We also received accounts from participants regarding the lack of professionalism of some staff, particularly those whose roles included the provision of information at the Registrars of Births, Deaths and Marriages. These negative experiences ranged from staff lacking sensitivity in the provision of information, to breaches of confidentiality. For example:
- forwarding a letter from a birth mother when the adoptee's name was not yet on the contact register;
- sending a letter informing adoptees of their adoption without knowing whether they were already aware of it; and
- making phone contact at the workplace to advise about the existence of half-siblings.
Enablers to search and contact
Of those who had tried to find information, nine out of ten had received information, and just over half had made use of a contact/reunion service (see Table C5). A further 52 respondents (7%) said they would have made use of such services, had they known these existed.
When asked what were the most helpful things about the search and contact services they utilised, respondents identified a number of key areas:
- Accessibility of information:
The social worker giving me all the paperwork from my adoption. (131, 2011)
Access to the Salvation Army Family Tracing Unit database. (195, 2011)
DoCS [departmental] and hospital records. (314, 2011)
Turnaround time was quick and my entire birth file and adoption records were obtained. Also very helpful tips about conducting a search. (41, 2012)
Search and retrieval of information. (354, 2012)
- Active assistance in search/contact process provided by departments/agencies involved:
The person from [agency], who acted as an intermediary and arranged contact with my birth mother. (53, 2011)
Having someone else do the search for me, as I found it a bit overwhelming. (62, 2011)
That it was an independent third party government service, removed from church/welfare services. (40, 2011)
Everything! Search, contact, mediation, support groups, literature, advocacy. (169, 2011)
Ability for others not involved emotionally to contact and mediate on your behalf. (50, 2012)
Using them as a mediator service so that my birth family members had time to evaluate the situation prior to having contact directly with me. (118, 2012)
Support, outsourcing the search and thus removing myself from discovering possible rejection of my enquiry. (189, 2012).
My case worker helped me every step of the way. (304, 2012)
- Helpful/useful information provided by departments/agencies involved:
Providing information, my legal status/rights and helping me through the stages of the process. (113, 2011)
To know the best way to make contact/how to make the approach. (85, 2011)
Got some basic information from [service] about how to write letters. When I found my real parent's information, got help with the search. (173, 2011)
Information, support, methodical supervised process for reunion. (194, 2011)
People who understood importance of family connection and who were informed about adoption issues. (57, 2012)
Great advice and information when preparing me for contact. (141, 2012)
- Ongoing support from agencies:
They would be there to support me if it didn't work out. (73, 2011)
Checking I was in the "right place" and clear about why I was doing it. (87, 2011)
The social worker listened to me when I found the reunion very emotional and overwhelming. (270, 2011)
Post-reunion counselling. I found all the information myself and met my birth family without any support or reunion services. (166, 2011)
Counselling and just knowing they were there. (238, 2011)
Pre- and post-reunion counselling. (298, 2011)
Support and understanding. (138, 2012)
Emotional support. They liaised between me and my birth mother when we did make contact. (316, 2012)
As is evident in the information provided by adoptees in the study in relation to their use of search and contact services, there is a marked difference in their experience when compared with mothers in the study. The adoptees group were able to reflect in detail the characteristics of what was most helpful to them, as well as what they would have liked to have experienced differently.
7.11 Making contact
Contact with mothers
Sixty-three per cent of respondents had had contact with their (birth) mother (see Table C6). Of those who had not had contact (305 respondents), the most common reason was because their mother had passed away (28%). Other reasons provided for this contact not having been established were:
- the respondent simply had not wanted to establish contact with their mother (16%);
- they had some information, but had never met nor had any communication (13%);
- they had not been able to find any information or their mother had rejected the possibility of having any contact/relationship with them (12% each);
- the respondent had simply not been ready to have contact at this time (8%);
- they believed it was their mother's choice to have contact and they were waiting for her to do so (6%); and
- their mother had a veto on contact in pace (6%).
For those who had had contact (n = 518), almost all contact has been since 1985, with contact occurring at a range of ages, but mostly when the adoptees were in their 20s and 30s.
Of those who had had contact, 54% of respondents who answered this question (n = 439) indicated that they had an ongoing relationship with their mother, 33% said that they had met but they did not have an ongoing relationship, and 13% had never met face-to-face.
Contact with fathers
Fewer respondents had had contact with their fathers than with their mothers - just 26% compared with 63% (see Table C7).
For those who hadn't had contact (n = 613; 75% of total adoptee respondents), the most common reasons given were:
- the respondent had not been able to find any information about their father (42%);
- their father had passed away (16%);
- the respondent had simply not wanted to establish contact with their father (13%);
- they had some information, but had never met nor had any communication (10%).
A small number of respondents who had not had contact with their fathers stated that they were not ready for contact (4%), the father had rejected the possibility of contact/relationship (4%) or they believe it was their father's choice to make contact (3%). Fewer than 1% of respondents said that there was a contact veto in place.
For those who had had contact (n = 210), almost all contact had been since 1985, with contact occurring at a range of ages, but mostly when the adoptees had been in their 20s and 30s. More than half indicated that they had an ongoing relationship, and 33% said that they had met but they did not have an ongoing relationship.
Contact with other family members
Almost two-thirds of respondents had had some form of contact with other members of their birth family (n = 532) (see Table C8). For those who hadn't had contact (n = 291), the most common reasons were:
- the respondent had not been able to find any information (28%); and
- the respondent had simply not wanted to establish contact (21%).
- Of those who had had contact with other family members, 63% indicated that they had an ongoing relationship, and 30% said that they had met but they did not have an ongoing relationship.
As can be seen from Figure 7.5, first contact with other birth family members tended to occur after first contact with mothers.
Figure 7.5: Age of adopted person when first had contact with birth family, by mothers, fathers and other family members
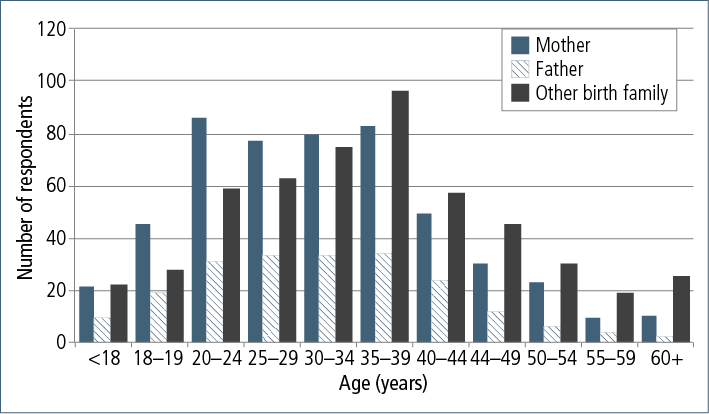
7.12 Effects of contact
Regardless of whether adoptees' contact with their birth families had resulted in positive or negative outcomes for participants in this study, the information shared with us provides a complex picture of how these relationships are developed, maintained and often fragmented from the time of discovery and through subsequent years.
Positive experiences of contact
A number of respondents provided positive accounts of their contact with their broader birth families:
I grew up feeling like an imposter, needing to be extra good to ensure that I would fit in and not be rejected. Only through meeting my natural family members did I learn about other parts of who I am. Only then I became able to make my own choices more freely. (101 2012)
I feel blessed to have had such positive contact with my birth family, especially considering I felt like I didn't really belong in my adoptive family through adolescence. I now have a close and ongoing relationship with my extended birth family, who all accepted me with open arms when my birth mother first introduced me to them. My life has been enriched by the addition of all my birth family. My relationship with my birth mother in particular has taught me a lot more about myself. (185, 2011)
I feel extremely lucky to have been placed in such an awesome family. I feel equally blessed that I was able to meet my birth mother and family to gain a bit more understanding of where they came from. (175, 2012)
Well, losing my adopted mother was the worst thing (other than becoming disabled) that has ever happened to me, as I was only 19 at the time. But thankfully I had found my birth mother (and her family) in the months preceding my adopted mum's death, so they could meet (and she met my birth grandma too) and I had someone to turn to when she died. Mostly it has been a positive experience finding my birth mother. (48, 2012)
I feel complete now I have found my birth mother. The hole in my heart is filled. I don't have a close relationship with my birth mother, but speak on the phone monthly. Have only seen her once in the last year, but I am OK with that. This experience has actually brought me a lot closer to my adoptive mother, and I am so appreciative to her for all that she has provided for me. It took finding my birth mother to realise this. For what my life could of been like with my birth mother, I had a very good childhood. (65, 2012)
I've had a wonderful adopted family and am very lucky to have strong relationships with both biological parents (who are thrilled to be grandparents). (214, 2012)
However, study participants also identified some of the challenges arising from having contact, particularly the complexities of negotiating newly established relationships with members of their family of origin, such as managing expectations as well as being able to convey one's own needs and wants within the context of the new relationship:
One of the reasons that my biological mother and I don't have a relationship anymore is that I don't think she ever got over the guilt of "giving me up" and she always expected me to be angry about it. I have never felt anger about it. Whilst I didn't have a good relationship with my adoptive mother, I don't blame that on adoption. (Adoptee, NSW)
They welcomed me with open arms and for a while we enjoyed a relationship, but I think coming to grips with who my mother was paired with, how demanding she is, I pulled back. And I know it upset them, but I had to do what was right for me and my own family. (175, 2012)
Going through reunion was like having a mental illness. I had an emotional breakdown from it all. It's a complicated relationship and all the relationships - birth and adoptive - are complicated. After 10 years of reunion, I finally found a psychologist that understood the issues and this made a big difference. It's a shame the media portrays it as a good thing and a "selfless" thing for adoptive parents to do. I feel that I was never good enough or acceptable, never what my parents wanted and also not what my birth mother wanted. She doesn't like the way I'm different to her. She expected me to make up for her loss and pretend nothing happened (that we weren't separated). I couldn't, I was so depressed and emotionally upset. The invalidation of my deep feelings by society and my families is as hard as the trauma of the separation and reunion. When I had a breakdown, I couldn't accept my own feelings as valid. My therapist said the feelings were normal in the circumstance. I didn't know to expect an emotional reaction like that. I wish more people understood how painful adoption is, and recognised it as separation and loss, not just adoption (gain), and no different than the non-adoption experience. My reunion experience brought all the underlying emotions to the surface. I have been working through these feelings for 20 years. (227, 2011)
The adoption must have been very hard for my biological mother. She was pressured into the decision. Had she kept me I would have been raised in a loving happy family with many older siblings. For me, contact was about curiosity, but for her it was a very emotional reunion and the answer to many questions. We only had three contacts within a short time. I distanced myself from her, as she wanted to absorb me into her family. She has memories of the birth, I do not. (283, 2012)
I am lucky to have such an extended family, and to have a good relationship with all of them. My birth parents are now more like friends than parents. We socialise together and travel together often. The only thing I'm sorry about is the effect the adoption had on my birth mother. She suffered many years of guilt before we met. My birth father was also adopted. He tried to contact his family after meeting me, but it wasn't very successful. I know a little about my paternal grandmother, but nothing about my paternal grandfather. (311, 2012)
Effects on other family members
In general, respondents' contact with birth families had either a positive or no impact on their other close relatives (see Figure 7.6 and Table C9). Although still in the minority, the relatives whom adoptees most often identified as being affected negatively were their adoptive parents, with the respondent's own children being the least likely to be identified as negatively affected by the adoptee's adoption experience.
Figure 7.6: Effects of contact with birth family on other family members
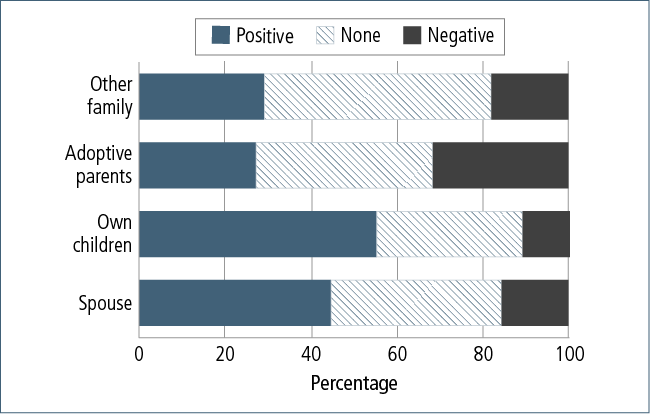
Divided loyalties
The issue of divided loyalties was a complex topic within both the focus group discussions and the open-response items in the survey. Probably more than any other respondent group in the study, adopted individuals appear to have been the "gatekeepers" of other people's needs/expectations in the adoption circle. The effect of this position/role was clearly stated, and remains one of the most significant issues associated with their adoption experience for many participants in this study. A relatively significant proportion of study participants said that they had in fact waited until the death of their adoptive parents before they contemplated searching for their family of origin, either out of respect to their adoptive parents and/or because they did not want to upset them:
When the adoption laws changed and they opened up and you could find [your family], I think it troubled my mum badly, and I had to actually counsel her that "I'm OK. It's OK, I won't be doing this, don't worry". So it affected her more I think. (Adoptee, Victoria)
She actually developed Alzheimer's; that's when I started investigating. Because I would not do it while my adoptive mum felt so threatened. (Adoptee, Queensland)
Another participant gave a more detailed account of how this issue has played out in her life. She said:
I get really upset about the guilt that everyone feels. My natural grandmother sought me out just as the laws changed … And I was pretty young and my adoptive family, as you can imagine, were pretty distressed about that happening at 16. And they felt, had made me feel guilty about having a relationship with them. I've tried to be really strong and not feel guilty about it, [but] that's been a kind of constant battle. My adoptive mother is very threatened by anyone from that family. When I was pregnant with my first child, on Mother's Day, I kind of said to mum, "Look, you know I want my children to have a relationship with [name] and everyone else in that family, it's very important to me. And it doesn't mean that [my children] are not going to have a relationship with you and they are not going to lose you. But you know, you're going to need to deal with this". That was really tough, you know. She was crying and carrying on. I guess I've been very lucky that I have a really supportive partner who's kind of a very level-headed person and he's constantly going, "No, this is right. I'm involved now, these are my children. We're not going to have the guilt and issues that have affected you affect the kids". I didn't expect it. To feel guilt all the time, and responsibility. (Adoptee, Victoria)
Of the 710 participants who responded to the question of whether they had ever experienced a sense of divided loyalty between their adoptive and birth families, 36% said this was not something they had felt (see Table C5). However, anecdotal accounts of the internal conflict over loyalty were common in focus group discussions with adoptees.
When I met my natural family, I got severely scolded by one of my adoptive brothers for hurting my adoptive mum's feelings, and I don't think he has ever really forgiven me for wanting to know them. (Adoptee, NSW)
It is your own guilt as well that I find really difficult. It is about trying to find out, and saying, I actually do have two [sets of] parents. Not just the person who brought me up, but also the person that gave birth to me, and they are just as important. And the guilt of knowing that they are just as important … That guilt is just horrible really. (Adoptee, SA)
One focus group participant spoke about how she has kept her relationship with her birth family completely secret from her adoptive parents, as she finds it too difficult to deal with their reactions:
That family is secret to my adoptive family, so my parents don't know and they never will. It's too difficult. It doesn't benefit anybody, particularly [adoptive] mum and dad. Because of that whole "We're your parents" sort of thing, and I'm just not going to buy into it. It's difficult because it's secret. I've had to keep a whole other part of my life completely secret from my parents. (Adoptee, Victoria)
7.13 Support received as an adult
Eleven per cent of respondents said that since becoming an adult, they did not want or need any support in relation to their experiences of adoption (see Figure 7.7 and Table C12). A further 4% did not have any supports.
Informal supports were again the major source of support identified by adoptees in the study, with over one-third of respondents seeking help from friends, and adoptive parents being the main source of support for around 20%. However, there has been quite high use of formalised/professional supports, with about one-quarter of respondents seeking help from a registered psychologist or psychiatrist, almost that many seeking help from an adoption support service, and more than one in five seeing a social worker or counsellor.
In their survey responses, the 823 adopted individuals collectively identified around 1,800 instances where they received support as an adult (twice the amount received while growing up), with most support being emotional (close to 60%) and psychotherapy or counselling (around a quarter) (see Table C13).
Almost half of the respondents who received support indicated the support had been very helpful, and somewhat helpful in a further 40% of instances (see Table C13). Only 5% said it had been unhelpful or very unhelpful.
The higher use of professional services for counselling/psychotherapeutic support would indicate that the effects of adoption have been significant for the adoptees participating in this study. The information provided in the qualitative components of the study support this notion; in fact, for many adoptees in these discussions, this was one of the most essential areas where they felt the current options for addressing the effects of their adoption experience were inadequate or inaccessible in the long-term due to the high associated costs of such services.
The results of the K10 measurement for this respondent group shows much higher than average scores in the likelihood of having either a moderate or severe mental disorder compared with the general population (see Table C16). And although just over half of participants in this respondent group (54.3%) were likely to be well (i.e., not likely to have a mental disorder), there was still a significant subgroup with higher levels of support need for whom clinical services would be beneficial.
Figure 7.7: Sources of support received by adoptees as adults, by type of support
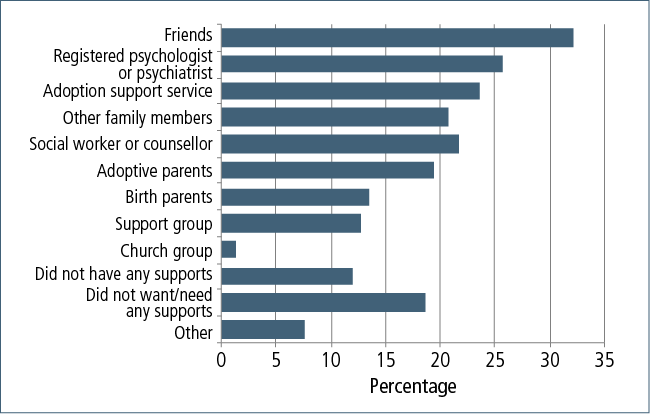
7.14 Current service and support needs
We are the children of the failed experiment that is adoption. (47, 2011)
I feel like I am the result of a failed social experiment. (219, 2012)
Adopted individuals in this study frequently told us that they feel as though they are the forgotten part of the equation in the broader adoption discussion; yet they are, in reality, living examples of how past practices have played out, and they want to have this information shared with the broader community.
It was clear to us in the collection of their information throughout the course of this study, that:
- adopted individuals have some very specific and particular needs;
- for many, their adoption experience has often significantly affected their capacity to function fully, both socially and emotionally;
- the effects of identity, attachment and abandonment issues have been an incredible burden to both themselves and their other family members, such as spouses and their own children; and
- the inaccessibility of their own information as this relates to the formation of their identity and sense of "place" in the world, as well as broader implications on their own and future generations' health, has been largely misunderstood/not acknowledged in the wider focus of the adoption discussion.
Despite the breadth of adoption experiences and associated effects, many adoptees in this study have felt that currently, health and other service professionals lack an understanding and awareness of adoption-related issues and are subsequently ill-equipped to provide effective support interventions.
Box 7.1 Key service system implications
- Addressing the variability between state and territory-based systems and laws regarding adoptees' access to information would be of significant benefit. The difficulties in navigating often complex systems, along with the associated costs, has been identified as a barrier to the formation of sense of self and identity, as well obtaining potentially life-saving information regarding medical histories. The centralisation of all state and territory databases would be the most efficient way of addressing this issue.
- Reviewing and potentially harmonising state and territory laws relating to contact and information vetoes was seen as a high priority. Currently, vetoes are seen by many adoptees to deny them access to medical/genetic information that they regard as their right, and differences in state/territory laws also create difficulties for situations where the two parties live in two different jurisdictions, or a different jurisdiction from where the adoption occurred. Harmonisation would still need to take into account the needs of those adoptees and birth family member(s) who do not wish to be personally identified in the information provided.
- Mental health professionals, including psychologists, psychiatrists and psychotherapists, will require specialised education and training to respond effectively to the needs of those affected by past adoptions. Key issues adoptees talked about that related to professional education were: (a) knowledge about the range of experiences that those affected may have encountered, including abuse and neglect and late discovery of adoption; and (b) training in specialist therapeutic skills to address the ongoing effects of identity issues and negative self-concept, and relationships that relate specifically to the adoption experience. This suggests that development of appropriate training modules that are readily accessible to those working in such professions is needed.
- As well as developing a specialist workforce, health and welfare professionals in the broader system would benefit from education about the effects of past adoptions on adoptees, and the potential physical, social and psychological effects. They would also benefit from training in how to provide appropriate assessment, diagnosis and referral to specialists.
- With appropriate resourcing, existing post-adoption services could provide ongoing engagement throughout the adoption journey. Continuity of care (i.e., not having to repeat one's "story", and build rapport with a new service provider) will play a significant part in the likelihood of those affected feeling adequately supported.
Adoptees' perspectives of most important benefit
All survey respondents were asked about the single most important thing that would be of benefit to them now in helping them deal with their past adoption experience. This topic was explored further in the focus group discussions.
These discussions identified several areas that study participants commonly said would be of use to them.
Information
The only way that we are ever going to pass the issues that we face is if the veil of secrecy is lifted. That there is acknowledgement of the impacts of past adoption experiences on us - on adopted children. And the state laws are repealed and federal laws are put in place that lift the veil of secrecy and allow adult people to deal with the situation. (Adoptee, SA)
A clear need was evident from the discussion for (identifiable) information to be provided on adoptees' mothers and fathers, their medical history, what the process was for screening and selecting prospective adoptive parents, and how true their adoption story is.
One of the most common issues to emerge was knowledge (or lack thereof) about their biological family's medical history and their own medical history at the time of birth. Respondents strongly expressed their rights to their genetic identity - not just for themselves, but also for their children and grandchildren. Many were fed up with always having to explain to medical practitioners about the absence of medical history information.
In addition, some respondents talked about the risk of incestuous relationships occurring if details about one's birth family are not known.
Some respondents expressed frustration with the veto system:
I find it disgusting and think we have moved forward as a society enough that we should allow adults to deal with adult situations. And time is running out for me. My mother is 60 now and she just reinstated her veto last year. So there's another five years I have to wait. And it's not about meeting her as such, it is about having the lineage. (Adoptee, SA)
Respondents also wanted easier processes for obtaining documents such as birth certificates and passports, and mentioned the indignity of procedures for obtaining such documents that they have had to, and still have to, follow. The need for a national approach, and government officials who have training in how to deal with adopted individuals, was expressed by a number of focus group participants.
Acknowledgement/recognition
As with many of the mothers, a common theme emerging from surveys and focus groups with adoptees was the importance of society recognising what has gone on, and acknowledgement of its effects on individuals:
To bring to the awareness the ongoing challenges experienced by abused adoptees and their families, such as mental health issues, physical disabilities, substance abuse, family and relationship breakdown, parenting, criminal and problems of reunion etc. (Adoptee, Qld)
Acknowledgement that the effects of adoption are lifelong and significant. Access to specialist support. Assistance to heal (Adoptee, WA)
Another very common theme was respondents' desire for there to be wider recognition of the situation of persons who have been adopted, with apologies being noted as one avenue for this:
Acknowledgment of the wrongs done to the victims of the adoption boom era. Acknowledgement of adult adoptees' right to feel anger for what was done to them in the name of bad public policy. (704, 2012)
Truth, recognition and apology from our government. Adoptees that were given to families and subsequently abused are seeking better services for pain, suffering, grief and trauma. We are seeking an apology not only for being taken from our mothers and family, but for the lack of screening of potential adoptive parents that should have protected us from perceived harm. As an adoptee who suffered abuse, to the extent of torture, I need immediate help with trained and qualified persons with experience in the areas of torture. This is a specialised service and not available to adoptees. Financial assistance to such services and a change to allied health plan, which only allows a small number of visits to much needed support from a trusted and trained social worker. Adoptees like myself seek the same type of apology as given to the Stolen Generation and Forgotten Australians and believe a watering down of any such apology will only result in continued pain and suffering, and even death. We require an equal voice with our mothers and ask that we be consulted more readily on past and present adoption issues. I ask that our needs and concerns be urgently addressed and that all stakeholders, self-help groups and organisations more readily support and encourage the voice of adoptees. That these organisations earnestly seek to overthrow perceived myths and perceptions about adoption, and that many adoptees have been unable achieve healthy relationships with adoptive parents, resulting in many suffering lifelong traumas. (50, 2012)
Some adopted persons noted the lack of a language to use to describe adoption to their own children. They felt that this could be made easier through greater public recognition of what has happened.
I guess my biggest issue right now is that my kids are coming to an age where I guess they need to know. But how do I explain it to them? (Adoptee, Victoria)
The issue of compensation came up more frequently among persons who were adopted than other respondent groups:
Will money ever compensate for the fact that I will always be torn, always be between two worlds, never fit in and always feel insecure and have no confidence and feel I am betraying one parent with another? Money will do one thing. Pay for the psychiatrist bills. Thanks for that. I will never fulfil my own potential, due to my own insecurity, but at least I have been to the right school. I am scared of having children and hate the whole adoption process. (97, 2012)
A class action involving compensation for people like us - whose lives have been blighted by our lack of adequate social skills and ongoing psychological suffering - would also help. (265, 2012)
I have suffered significantly from these matters, and if there are any illegalities or gross negligence, then I wish to seek advice with regard to legal compensation. (369, 2012)
Public awareness and education
Respondents expressed a strong need to stop the secrecy that still continues in many families today. They commented that increased awareness can enable people to understand that adoption can be a contributing factor to mental health and wellbeing issues:
More openness and social education as to the realities and widespread extent and repercussions of these policies that were carried out here in Australia. Created by and backed by and carried out by both state and church, in the most cruel manner. The trading of humans at a social/class/status level. Admit what happened, in it's entire ugliness and why, and to what extent. Acknowledge the high level of pain, suffering, permanent scaring and, sadly, suicide this policy has and continues to cause. (219, 2012)
To create a dialogue, to hear more accounts of others' stories about the experience and their emotional reactions, to have access to research. I would also hope that adoption is no longer viewed as a convenient "birth control measure" by the wider community and that the long-term effects on everyone involved are considered, measured and taken seriously in making future policy on this issue. (558, 2012)
I think any public discussion which openly discusses and acknowledges the difficulties of the issue and validates the complex experiences of all parties is a positive step. It was only in the past ten years when I read a book on the adoption experience that I realised for the first time that my mixture of feelings and emotions was actually pretty typical for an adopted person. (288, 2012)
Some more information from adopted children. The loudest voices and agenda setting comes from relinquishing and adoptive parents. I have a number of adopted friends and all feel unable to be truthful for fear of hurting both sets of mothers/parents. It is a taboo area for discussion. My sister and I will not be able to publicly voice our experiences truthfully until our parents are deceased. In the meantime we will toe the adoption party line … that we are very grateful. (371, 2012)
It is all too late for me. But I would like the negative side of adoption for adoptees to come out publicly so that we can stop pretending that it is a good practice. It is good for adoptive parents and, perhaps, natural mothers who for their own reasons choose not to keep their child. But for adoptees, we have largely had to remain silent until we are in a room on our own. If we say what we really think, we run the risk of being rejected by our adoptive parents and being seen as ungrateful. On the occasions when we do try and speak about how we feel, we are often interrupted mid-sentence by natural mothers telling us why they did what they did. (417, 2012)
Current adoptions and donor conception
Part of this discussion also centred on many participants' concerns regarding the current adoption and donor conception environment in Australia. It was a regular topic of discussion in both the focus groups and in some of the open-ended sections of the survey, and those adoptees who held views on the subject were extremely firm in their opinions that these issues be part of the discussion in this study. They felt that as they are the living result of past practices, they are in a better position than most to comment on current policy and practices in Australia. We will therefore present this information in the study participant's own words:
Recently in the paper you see adoption rights - and I think, "Ooh, adoption rights" … And then you realise it is not about the rights of adoptees. It's about the rights of others to adopt. I feel really angry about the whole donor sperm thing - anything about manipulating a baby who has no say. It's not just adoption, it's all these issues. (Adoptee, Victoria)
Future adoptions, surrogacy, IVF, etc. be focused around the child and not just that of the parent. It always seems as though that is the voiceless person in the debate and where the impact appears perpetually underrated. (Adoptee, NSW)
Education of the population to know that adopting out your child is not always the best thing. The best is for children to have their own mothers bring them up and it would be better to support them. I resent the idea that the adopting parents are wonderful, when they are having their needs met, but not the child they are adopting. (114, 2012)
I think the concern I have is about displacing people's pain. It's about saying, we can't have children, so you've had a child, and we're in a better situation. Now if that person is willingly giving up their child for their life and future options and where they are at in their life right now, it is a conscious choice, powerfully made, that they would rather make and not have a child at this point in time, then that's an absolute gift for that couple. But where coercion is part of it, it's about actually saying, well we are more deserving than you and your pain is less of a consequence than our pain of not having a child. That's really concerning for me. (Adoptee, Victoria)
I don't think I could adopt because I know the wound is there. To be real with that child, you are facing a very big, overwhelming wound. I'm very clear about my opinion of adoption - it should be about the best interests of the child. The whole adoption industry is about supplying couples with children. I was reading the recommendations of the Senate Inquiry and what I was disappointed about was, for me, it's too late. I've learnt to deal with it myself. For me, a sort of recommendation that would absolve things would be a change in current practices. I think the underlying root of the problem is the baby-supply industry. The same issues are coming up with donor conception, surrogacy, "selling" children on the Internet, especially in America. The same issues are popping up and they're being repeated. To me it means nothing, because I'm seeing the same thing again. I'll never know who my father is and I'm seeing these people being put in similar situations where they'll never know who their father is. They're told, but you've been given life, you're better off because we want you. It's about the needs of the parents, not the child. (Adoptee, Victoria)
Support for search and contact
Respondents indicated that support is needed for searching, contact and navigation of new (and existing) relationships. Help is needed with:
- the process of searching;
- accessing information (from birth mothers and government/adoption agencies); and
- addressing the effects of contact (managing new relationships, having divided loyalties, experiencing rejection for a second time).
Focus group participants suggested that counselling should be offered at all stages of seeking information and making contact, and that mediators should be available to assist all parties involved:
System in which information is exchanged in a timely fashion, and support given to all parties to encourage family connections. (57, 2012)
Now, I am going okay, but I think others definitely need ongoing counselling and support as they make the journey of search and contact. I know that is what I needed, and probably from time to time still need. Resolving the residual inner issues is as important as the physical search for "family". Unless you can simultaneously address the impacts and damage caused by closed adoption, then the quality of the reunion (if it occurs) will be affected. Adopted people also need assistance on how to juggle the competing needs, expectations, demands of the adoptive and birth parents and their/your families along this journey. For me the lifelong feeling of being in no man's land was exacerbated as I tried to balance (almost guiltily) the desire to connect with the guilt of doing so (and upsetting my adoptive parents). Intellectually, I knew what I was doing and intended to do, but emotionally and in reality, it was much tougher. I was lucky. I regard the effects of my adoption experience as a black cloud hanging over me, but for many it's a gaping, raw wound. (88, 2012)
Support for wellbeing
A very strong theme to emerge for adoptees was the need for appropriate, affordable counselling and support, which should be available whenever trigger events happen, not just as a one-off service. A range of options is needed so that the most appropriate form for a particular individual can be selected. Not everyone saw cognitive behaviour therapy or other structured psychological interventions as the solution for all. It seems that cognitive behaviour therapy was one of the most commonly identified interventions received by those accessing services, but people found it had limited utility in addressing their particular needs. A number of participants suggest that other modalities can be more effective, and that research is needed as to which techniques will work best for whom:
Assistance in the form of counselling services for those adult adoptees who need it. Assistance - real assistance - in the sometimes extremely difficult task of searching, particularly in circumstances where an adoptee's health is being affected by lack of genetic medical knowledge. (704, 2012)
Free weekly counselling from a professional with deep knowledge of adoption issues. (74, 2012)
A support group in my area. (81, 2012)
The periodic availability of a support group or even online support group. (96, 2012)
Specialised counselling to help manage, understand and deal with the separation and abandonment issues I try and manage as an adult. (108, 2012)
A support group for folk with similar stories. (122, 2012)
7.15 Summary
It is clear from the accounts of adopted individuals that they have rarely felt that their experiences have been validated or viewed as being of any real importance - that the effect that their adoption has had on their lives (both positive and negative) has not been included in the nation's broader discourse around adoption. Many stated that they never felt that they could talk about their experience because no one ever recognised or acknowledged their loss (of identity, of family, of history, etc.).
Issues of identity, attachment and abandonment among adoptees do not appear to be solely dependent on whether or not a positive and loving environment was provided by the adoptive parents. Rather, it is likely that those who have experienced adoption as an open discussion, who were encouraged to search, and were given a positive view of their birth mother, have fewer experiences that play out negatively throughout their lives.
Adoptees in this study showed a higher than average likelihood of having a mental health disorder than the general population, and qualitative accounts of mental health and wellbeing support these findings. The most important issue is having access to appropriate and specialised counselling and support that is both affordable and ongoing. This includes support to address the complexities of navigating both existing and new relationships following contact with birth family members. In addition, assistance with their own parenting was identified as a current need, with many participants saying this life event was the trigger for some of the issues associated with their adoption experience and subsequently affected their own parenting.
As is evident from the information provided by study participants, the issues of seeking information about themselves and their birth families, and the subsequent process of search and contact, significantly contributed to both past experiences of adoption and its current effects. A strong theme from adoptees participating in the current study was that access to information about themselves and the medical histories of their birth family was a "right" not a "privilege", and they called for the processes associated with obtaining such information to be reviewed as a matter of priority.
8. Adoptive parents
Adoptive parents were able to participate in the study by completing an online questionnaire or a hard-copy survey, with almost a quarter of the adoptive parents completing the hard-copy survey. Some adoptive parents were also involved in follow-up focus groups; however, the majority of information was gathered from the surveys and supplemented by the information gathered from the face-to-face meetings.
There were 94 adoptive parents who responded, with over two-thirds being over the age of 65 years.
8.1 Time of adoption
When recruiting participants to complete this survey, we emphasised that the survey was for parents who adopted their children during the period of "closed adoptions". The survey questions asked whether the adoptive parents had adopted multiple children and what was the perceived level of success of their search and contact experience (if any), and its effects on various relationships.
Characteristics of children adopted
Of the adoptive parents surveyed, 57 had adopted a boy, and 36 had adopted a girl as their first adopted child. The majority of the children adopted were born between 1965 and 1974 (see Figure 8.1 and Table D1).
Figure 8.1: Year of birth of adopted child, by gender
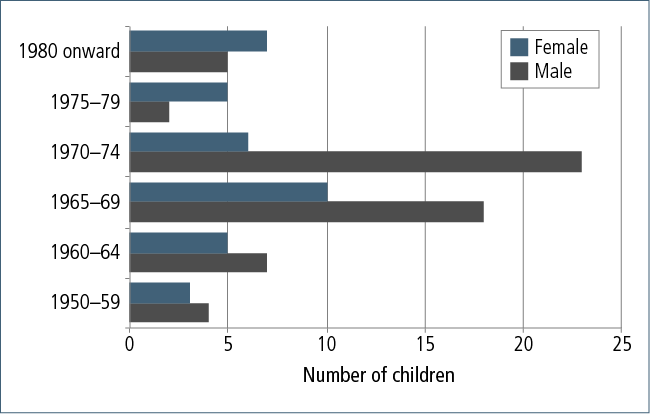
Over half of the children had been adopted by the time they were six weeks old, but there were a few who were not adopted until they were much older (see Figure 8.2 and Table D1).
Figure 8.2: Age of child when adopted
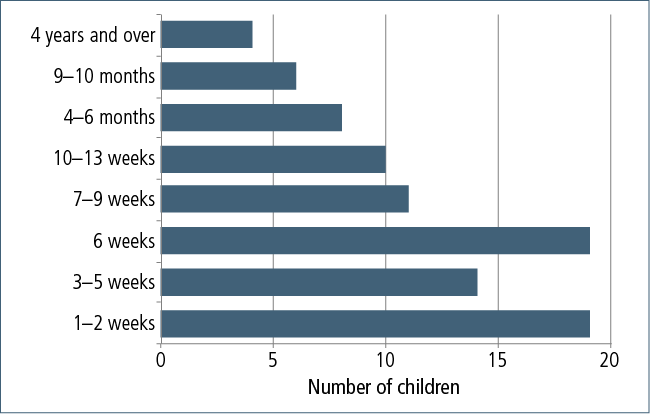
Over half of the participants had been living in Victoria and New South Wales at the time of the adoption, with a small number adopted while they had been overseas (see Figure 8.3 and Table D1).
Figure 8.3: Place of residence at time of adoption
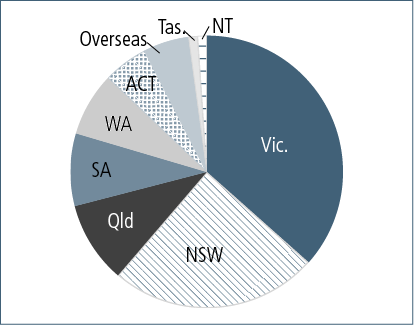
Reasons for adoption
We decided to adopt when I was unable to conceive. (Adoptive parent, WA)
Three-quarters of the respondents stated that the main reason for adopting was their inability to conceive or carry a child full-term (see Table D1). However, another common reason for adoption was a preference to adopt to ensure the gender of their next child, or because they wanted to adopt a child with special needs.
Forty per cent of the adoptive parents had adopted just one child, with 44% adopting two children and 10% adopting three or four (see Table D1).
Further adoptions
We had already decided on two children. (Adoptive parent, Queensland)
Many of the adoptive parents had decided on the number of children they wanted to adopt before the first adoption. Often the gender of the child affected the decision to adopt a further child. Some did not adopt further because they had subsequent biological children, while others no longer fulfilled the age requirements to adopt or had medical reasons for not adopting.
For those who felt that the experience of the first adoption did influence their decision to adopt more children, the reasons were often because they were:
- pleased with the outcome and eager to expand on their family;
- encouraged by the adoption agency to apply for another child; and
- unhappy with the process and decided not to reapply.
Organisation of the adoption
Advertisements were seeking homes for babies unable to be placed. (58, 2012)
The large majority of adoptions were organised by institutions: half by a government adoption agency, close to a quarter by a church, and one in five via a hospital (see Table D4). A small number were organised through a maternity home or home for children. Ten per cent of the adoptions involved private agencies, of which some involved the family lawyer or a private adoption agency. Social workers, family friends and other individuals were also involved in the adoption process.
More than eighty per cent of adoptive parents were completely or mostly satisfied with the adoption process. Only a very small number were dissatisfied (see Table D4).
Problems with the adoption process
Despite the fact that our daughter was an abandoned infant, and moving to a country town where we, as parents, had no extended family, there was no counselling, no advice, no support, no encouragement - only criticism from the Department of Youth and Community Services. (Adoptive parent, WA)
Although a large majority of the adoptive parents did not experience any problems during the adoption process, there was a small portion of respondents who did (see Table D4). These problems were:
- administration of relevant paperwork;
- length of time taken to adopt (either too quickly, or they had to wait too long):
To know that with a little more than one day's preparation and finding you are to be the first-time parents of a child who was a state ward, should never have happened, especially when there was no ongoing support! (392, 2012)
We had no warning that he was available. We'd been waiting approximately nine months but then it just happened. There was no viewing or anything, we were just given him. There was no transitional information or discussion or anything. (Adoptive parent, Qld)
- lack of follow-up and support:
I feel that we were not mature enough. (Adoptive parent, WA)
- management of the screening process:
They would pop out to the house at any time. One of them was making snide comments about there being no carpet, dogs etc. They had no understanding of our living situation at the time. They went to our [biological] daughter's school, which we had no knowledge of until a teacher told us. There was no support - it was more like an interrogation. (Adoptive parent, Queensland)
- no counselling about the issues relating to adoption:
As an adoptive parent, the experience was mostly positive, but there were times when we felt like we were just babysitters and we weren't really valued as valid parents. (Adoptive parent, NSW)
I would like to think that adoption processes are handled differently, with more importance give to adoptive parents' concerns. To be told [in my forties] that my concerns about my son's behavioural problems were unfounded, and that adoptive parents look for imaginary things because the adoptive child behaves differently from the birth children, was to me insulting and degrading. Consequently [our son] is now a 41-year-old welfare patient, still living with us. (1421, 2012)
- mother changing her mind about the adoption:
The mother had three months to change her mind. It was really stressful. (Adoptive parent, Queensland)
- changes in legislation over the period of time of seeking adoption.
Support at time of adoption
The social worker at the Women's Hospital took us through the whole process in a supportive way. (Adoptive parent, NSW)
About three-quarters of respondents received some type of support during the adoption process (see Figure 8.4 and Table D2). The main source of support for adoptive parents was their spouse, with friends, parents and social workers or counsellors also common forms of support.
Emotional support was by far the most common type of support received, with this representing around 60% of all instances of support (see Figure 8.5 and Table D3). Some adoptive parents also benefited from financial support (28 instances), legal support (21 instances), family planning advice (18 instances) and psychotherapy of counselling (18 instances). The vast majority of support was found to be helpful, with fewer than five per cent of cases being unhelpful.
Some families received information from social workers that gave recommendations on how and when to tell the child about the adoption, as well as explanations of what to expect with the adoption process. In regards to the assistance from the social worker, one respondent commented:
[S/he] tried to explain what our feelings would be and how we should feel about adoption. Very positive all the way. (Adoptive parent, Queensland)
Figure 8.4: Sources of support given to adoptive parents at the time of adoption

Figure 8.5: Emotional support provided to adoptive parents at time of adoption
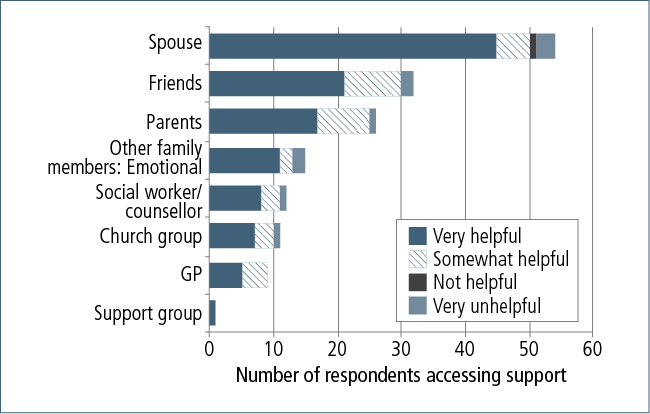
8.2 Disclosure of adoption to children
Every Sunday evening before bed, we told them the story of their adoption and how we had longed to have a child and God provided them for us. There was never any problem with speaking about their adoption to them at any time, and there is still no problem speaking to them about it. (192, 2012)
A large majority of adoptive parents told their children about the adoption before they started school (see Table D5). Many stated that the child "always knew", and it was common for the story of the adoption to be told "as if it was another fairy story". Most believed that their child had "no issues" about their adoption:
He always knew. It wasn't an issue. (644, 2012)
Told at an early age and totally accepting. (199, 2012)
They knew from the word go and no reaction. (1115, 2012)
Some of the children had a positive reaction to finding out about their adoption:
Very accepting when told about his adoption. He felt very special. (1409, 2012)
It was always accepted as being special to him. (1054, 2012)
My daughter used to tell people who picked on her that she was specially chosen. (794, 2012)
However, some adoptive parents believed that their children were too young to understand the implications of the adoption until later years:
They had always known, as [their] reaction didn't act in until adolescence, when they fully understood the implications. (1295, 2012)
They registered no surprise or understanding until they were about 7 years old. (808, 2012)
It was hard to judge, as the context needed to be in line with his development. I think the realisation of the concept of adoption comes at a much later development stage. (1098, 2012)
A few reported that their child had a difficult time when they found out about the adoption, describing their son/daughters' reactions in a variety of ways, such as:
Broken-hearted. (Adoptive parent, NSW)
Upset/sleepwalking and crying. (1776, 2012)
Gradual process of acceptance. (952, 2012)
Many of the adoptive parents stated that they believed it was appropriate to tell the child as early as possible, and to try to associate the adoption with positive messages of hugs, kisses and being "specially chosen":
We celebrated birthdays and adoption days. Therefore they always knew and that it was a cause for celebration. (416, 2012)
8.3 Contact with family of origin
We understood that his search was natural. (1218, 2012)
More than two-thirds of the sons and daughters of the respondents had tried to find out information about their family of origin (see Table D5). Of these, over half said they encouraged and/or supported their search for information (n = 37), and a further 11 respondents were not concerned about the search. Only 9 actively disliked the fact that their son or daughter was searching for information.
Contact/reunion services used
The majority of adoptees who searched for members of their family of origin used a contact/reunion service (see Table D5). This included search and reunion organisations, government departments and direct contact with individuals or agencies involved in the adoption.
Only two of the respondents indicated that the reunion service supported them by providing information about how they might feel about the possibility of their son or daughter being in contact with their family of origin. Both found this information helpful.
Contact with family
At first I was hurt, but I have overcome this and am very happy for my daughter. (598, 2012)
Well over half of the respondents had sons/daughters who had contact with members of their family of origin (n = 55) (see Table D5). The main reason for not having contact was that their son or daughter had not wanted contact.
About half of the sons and daughters who made contact did so in the 1980s (see Table D5). The most common age at which they first had contact was in their early twenties (see Figure 8.6 and Table D5).
Based on the knowledge of the adoptive parents, the majority of adoptees who did make contact established an ongoing relationship (n = 26), while some had met but did not have an ongoing relationship (n = 17), and a few had yet to meet (n = 3) (see Table D5).
Figure 8.6: Age of son/daughter at first contact with family of origin
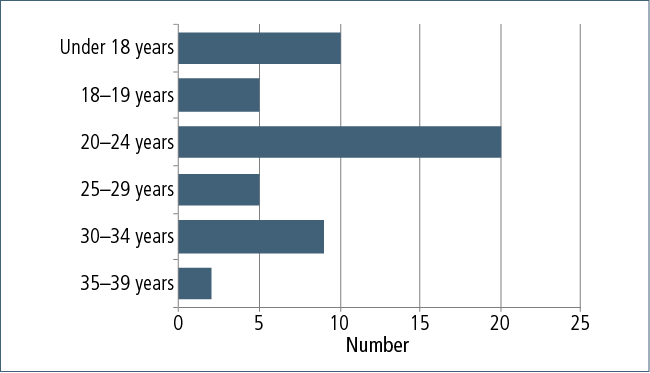
Adoptive parents' response to contact
Not happy, as we had been led to believe these details would be kept "closed". Contact was made for both my children by the birth mothers through the department. (794, 2012)
Adoptive parents reported a variety of reactions to the contact with their child's family of origin. There were common feelings of anxiety and apprehension, joy and sadness (particularly when the contact did not result in a positive outcome). Many recognised their son or daughter's need to know, especially with regard to their medical history. Adoptive parents talked about their reactions to adoptees making contact:
Very elated and proud to present her to her birth family and so they were able to see what a lovely person she had grown into. And to allow her to get answers we were unable to give. (1408, 2012)
Uncertain of emotional consequences, but very understanding and supportive. (953, 2012)
Concern that we would lose her … Jigsaw rep. gave us a lady's phone number and I had to make that call to tell her we had raised her ex-baby. One of the hardest things I have had to do. (1772, 2012)
We were unaware that our daughter had contacted her biological mother through Jigsaw being created by government. Unfortunately, we were completely unaware for over 12 months that she had been seeing her biological mother and father … Both of us took this news very badly, made worse by the length of time before we were told. (1773, 2012)
Effect of contact on relationships
We encouraged our daughter to accept the contact from her biological mother (in 1991). She [that mother] did not go on with face-to-face contact, and we believe that has unsettled our daughter in some respects. (Adoptive parent, Victoria)
Few adoptive parents reported that the contact resulted in negative effects on their son or daughters' relationships with other key people in their lives (see Figure 8.7 and Table D6). In fact, around half of the adoptive parents stated that this contact had had a positive effect on their own relationship with their son or daughter, and well over half felt that the contact had had a positive effect on the relationship between their son or daughter and their own children.
Figure 8.7: Effect of contact with family of origin on son/daughters' relationships
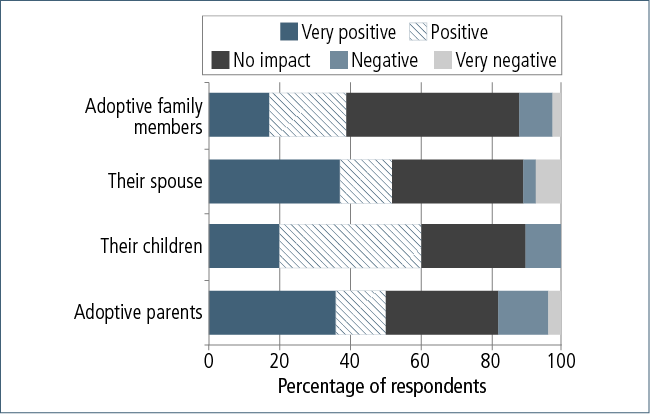
8.4 Effects of adoption
Effects of the adoption on child
I believe his adoption has been a very difficult aspect of his life. We cannot recall any warning about psychological issues, particularly not attachment disorder, which means we would have sought counselling earlier. (Adoptive parent, WA)
Just over half of the respondents (n = 50) did not believe the adoption had any effect on the health and wellbeing of their son or daughter (see Table D4). However, many of respondents did believe there was a link, of which the most common reported were:
- mental health problems (including depression, autism/Asperger's syndrome and personality disorders);
- low self-esteem;
- attachment issues;
- feelings of rejection;
- abuse of drugs;
- negative behaviours (shoplifting, stealing, "inappropriate sexual behaviour"); and
- embarrassment about the adoption.
Some adoptive parents commented that it would have been useful to have known the medical history of the birth family in order to better respond to the needs of their children. Other comments on the health effects of the adoption on their son or daughter include:
He always wanted to be seen as the unwanted one and would get extremely angry and frustrated when we tried to reason with him … As a young person, I always had in mind adopting children who would live happily ever after, but sadly so many of them have some sad stories to tell. (1420, 2012)
The lack of more detailed information concerning the birth mother and father with respect to health and personality profiles and their family backgrounds has made it very difficult for us to respond to the many issues which are ongoing. (1770, 2012)
Distracted by wanting to know and meet his biological family. Not being able to apply himself to study/projects and persevere to the end. Poor decision-making, inconsistent, unsure of himself, low self-esteem. (233, 2012)
Over the past four years I have read a lot of literature on the subject, so I understand there are real adoption issues. But I hasten to add, I feel sometimes that too much of an issue could be made of this at times. I really do understand as I get older how important it is to belong to a family. Before her "crisis", I considered her part of our families, of course, but now after reading literature I realise that adopted children feel different and not part of the extended family. I understand this could be a lonely feeling. I do think though that some professionals could exaggerate the effect of adoption, which could do more harm than good. I have come to terms with everything over the past year or so and it has been a difficult period, like grieving, I suppose. (1767, 2012)
Attitudes toward family of origin
Certainly, the challenges that are faced in the formation of a new family unit are complex, including the respective parents feelings toward one another. This was at times an emotive topic for some study participants who have experienced both positive and negative feelings about their child's family of origin.
A number of participants told us of their concern for the mothers of their children and sympathy for the difficult decision that she would have had to make at the time. Others wanted to be able to tell the mothers that their child is okay:
I felt blessed to be an adoptive parent. Feel only thanks to the mum who gave her up for adoption. I myself was an unmarried mum, who had an option to give my baby up for adoption or to keep my baby. I chose to keep my baby, but know the decision was not an easy one to make. We all make decisions in life that at the time seem to be the right ones for our position at the time. (1046, 2012)
I would like to be able to get a message to the birth mothers to tell them that their children are healthy and working in jobs that they enjoy. (334, 2012)
A number of adoptive parents who participated in the study were open about some of the more challenging feelings that they have at times experienced toward the families of origin:
I was amused at my only negative reaction recently, when the birth mother mentioned that she was taking the opportunity of spending more time with her grandchildren in a shared holiday. I thought, "They are my grandchildren!" (Adoptive parent, Queensland)
For the natural family to disappear. (239, 2012)
I would like my four adopted children to explain to me why they transferred their allegiance from me to their respective birth mothers. (546, 2012)
Support for dealing with issues arising from adoption
We have been very fortunate in not having experiences that required support. (Adoptive parent, NSW)
Half of the adoptive parents participating in the survey had support to assist them in dealing with issues arising from adoption (see Table D8). Almost a third did not want or need any supports and the rest did not have any supports at all.
Of the respondents that did have supports, the most common source of support was spousal support, followed by support from friends (see Figure 8.8 and Table D9).
Of those who had no support to help work through the issues, one commented:
I had very little support, and have now established (with others) an organisation to support others in the same predicament. (797, 2012)
The most common type of support received by the adoptive parents to assist with issues arising from adoption was emotional support. One respondent stated that "encouragement" was a better way to describe the type of emotional support received. A small portion of the participants mentioned receiving other forms of support: psychotherapy or counselling (n = 10), financial (n = 10) and legal (n = 3).
Figure 8.8: Sources and helpfulness of support given to adoptive parents at time of adoption

8.5 Adoptive parents' health and wellbeing
The vast majority of adoptive parents who responded to the survey were likely to be well, based on their responses to the K10 measure. Only a handful of respondents were likely to have moderate or severe psychological distress. These results corresponded to the general population norms.
In response to the question about their overall satisfaction with life, the average response was 8 out of 10, similar to the results from the HILDA survey for respondents aged 65 years and over.
8.6 What would help now
Access to medical information
Having access to their child's family of origin's health history to address medical issues arising with their son or daughter and their children was one of the most recurring needs of the participants of the survey. Many had sons/daughters with medical issues that they believe could have been better addressed if their medical history was at hand.
To know a little more about the medical history of our daughter's natural parents, as we know that the condition of asthma has been passed on to her children and grandchildren, and we suspect that problems coping with some of the aspects of mental health difficulties have also passed on to at least two of her children. (1021, 2012)
I think a medical history of the parents, if at all possible, should be supplied when you are adopting a child, as it would be so helpful to know some details as health problems arise with the children you have adopted which could be inherited. (595, 2012)
I would like to contact my son's birth family for medical reasons. His three children need to be aware of any health issues which may be inherited. Whilst he was ill, I had his permission to try to contact them through DHS, but did not succeed. I have tried since his death, but still have had no success. (Adoptive parent, Victoria)
We would like to know a lot more about our son's father, as we have been told that our son's Asperger's comes from the male side of the family. His dad was unnamed. We know a little about his mother and her family and who she married and where she lives and that her father died of a heart problem, but we believed that we are not allowed to contact her. We would like to know a lot more about our two children's parents and their families for any health problems. (1115, 2012)
Death of a child
For a small number of adoptive parents who participated in the study, their adopted son/daughter had passed away. They spoke about the fact that they have no way of making contact with the birth families to let them know of the death if their son/daughter had not made contact:
Our second daughter passed away year 2001 from breast cancer, she never wanted any contact with her natural parents, she was the fifth child and never shown any emotion what so ever about her natural parents or brothers and sisters. Both my husband and other daughter would like to contact them or members of her family to give photos of her and talk about the joy she gave us and our family we will never have peace till we know her natural Mother knows about her and the life she had. (1407, 2012)
Awareness of positive adoption stories
Many respondents believed that the media "focuses too much on the birth mother's loss" and does not accurately reflect the positive stories of adoptive families. This was explained to have a detrimental impact on the adoptive parents and their sons/daughters. Some respondents stated that they would like this imbalance to be addressed and increase the awareness of more successful adoption stories:
We resent the relentless publicity about forced adoptions, which were the exception, because the authorities, for the anguish they continue to feel [sic]. This is very disturbing to adoptive children and grandchildren. (Adoptive parent, Victoria)
I am afraid that the very negative publicity about adoption is colouring people's experiences and that there is too little attention paid to the many positive adoption stories … I feel it is very important, for the wellbeing of adopted children, including adult ones, that some balance is introduced into the public discussion of this issue. (246, 2012)
It would be helpful for our daughter, and therefore for me as her adoptive mother, to hear many more adoption success stories in the public domain. There is a gross over-representation of difficult adoption stories in the media. (709, 2012)
Assistance with search and reunion
Some adoptive parents stated that they would like assistance with making contact with the family of origin because they believed it would be helpful to their son or daughter. Others wanted contact with the family to share information and to show gratitude for being given the opportunity to parent the child:
The process for a child to get information and perhaps re-establish some connection with a birth parent needs to be better supported and facilitated. It was so difficult to see our son make such an effort to find his birth mum, and then for it to be such a trauma in taking the next steps. (Adoptive parent, WA)
What would benefit me? To know that my son and I could work together to find his mother, to help him connect, to know that you can love as many people in your life as you want. (Adoptive parent, NSW)
Counselling and support
A few respondents suggested the need for counselling and support, whether from professionals or support groups. They identified needs such as:
The need to talk to people in the same situation. Fortunately, I have friends from the support group I attended and helped to run, so can always talk to them. (797, 2012)
To have someone I could talk to about how I feel and to reassure me that I am doing all I can to help my children and grandchildren now, without interfering. To be able to know what - when there are problems - are a result of "adoption" and what are just normal life problems. Only others involved in adoption can really understand. (1295, 2012)
I wasn't able to find any support groups that helped with the adoption experience. For the last two and a half years I have been seeing a counsellor on a regular basis. She has been wonderful, but is not specifically trained in matters of adoption. I am afraid that this support will someday end and I feel that I will need ongoing support, as I feel very alone in this. (1406, 2012)
Information about the effects of adoption
Adoptive parents reported that they had had little information on the effects of adoption during the time they were raising their son or daughter. They believed that access to better information would have assisted them in dealing with some of the issues that arose from the adoption:
More material on the market or available in bookshops on the emotional impact of adoption on the adopted child. By this, I mean the effects of separation from the birth mother on adopted children. There is still little available. We got the greatest help from a simple photocopied booklet entitled, The Primal Wound: Legacy of the Adopted Child, written by Nancy Verrier in California in 1991. This box has to include the lack of medical history of the adopted child. Neither he nor we had any provided and this son died a few months ago. (1007, 2012)
How to help my daughter overcome her unwarranted fear of being less loved. (1090, 2012)
For our son to communicate with us honestly, without feeling he has to please us or win approval. (233, 2011)
Wish I had been directed to literature regarding what the adopted child is really going through, as we had no idea. Looking back we just had our heads in the clouds with so much going on in the little ones' minds that we were completely unaware of. (1767, 2012)
While I now believe that being an adopted person necessarily always carries with it some degree of loss and grief, and a need to come to terms with things that biological children don't need to, I believe it can, on balance, be a very positive life experience, leading to a fully realised and successful adult life. More awareness of this more subtle understanding in the wider community would greatly help the adopted child as she grows, and therefore support adoptive families as a whole. (Adoptive parent, Victoria)
Knowing adoptive families realise the importance of their "new" children having contact with their original families. (255, 2011)
Too late for support
Some adoptive parents stated that there is nothing that can be done now to support their needs, or that they no longer have any issues relating to adoption that can be addressed:
Too late, and would not advise anyone to adopt on our experiences. (Adoptive parent, Victoria)
Don't feel that I need anything right now, but at the time more communication would have been helpful. (Adoptive parent, WA)
I have dealt with anything that troubled me many years ago. (1645, 2012)
I have no issues that I need to deal with regarding my adoption experience. It was, and is, one of the best thing we ever did. (1235, 2012)
There is nothing now. It is all in the past. We overcame any difficulties and got on with life. (807, 2012)
Effects of political/media attention
Many of the adoptive parents found the current political and media interest in past adoption practices were biased and had a negative effect on their wellbeing and the wellbeing of their children. Some of the comments mentioned were:
The most important thing for me would be for people to stop making this whole thing such a big issue. At the time that we adopted our children, there were laws regarding adoption and we did nothing to go against these laws. All of the things that are happening, such as the Senate Inquiry being held now, are hurting us, because we have done nothing wrong, and yet we feel that we are being shown up to be people who physically "stole" these children from their mothers. The three mothers that are the birth mothers of our children, were not mistreated. We have assurances from the society who handled all of this and cared for these girls, and it was family pressure that made them give their children up for adoption. We have been assured under oath that the society and the hospital who cared for these girls never maltreated them. We actually knew of the home where these girls were cared for pre-birth, and they were given love and care and support for free, and helped so much because of their situation. We cannot understand why all of these situations are put together into one big heap, and folk are being told they have mistreated girls and stolen their children, when in fact this did not happen. Why aren't genuine people given the opportunity to speak up about their experiences instead of a small group being chosen to put down people who tried to help them. Don't these birth mothers realise that in most cases, the alternative from adoption was to have their child institutionalised? Would this have been better than having a loving caring family environment to grow up in? Families did not want these girls to go home to them with a baby for the family to care for. Why aren't these facts spoken about? (192, 2012)
Adoptive parents are often shown in the media in a negative light, with the focus being on the mother who "lost" her child. At the time of the adoption of our children, it was pre- the pill, and there was little help for single mothers. And as a consequence, there were many children available for adoption. It seemed to us that by adopting we were not only answering our own need to be parents, but also keeping at least two children out of institutional care. Although my children have had contact with their birth mothers (in each case the father is now deceased), I have told them it is up to them how much contact they have, but would prefer if they kept that a separate part of their lives. It was very difficult having a birth mother wanting to contact when my children reached 21 years of age. I did meet my son's mother, who said I had "done a good job". As it was never a "job" to me, it was not easy to take, but I suppose she meant well. I therefore think that support for adoptive parents when their adult children first have contact with birth parents would be helpful, because they are emotionally affected by this also. (794, 2012)
Box 8.1 Key service system implications
Adoptive parents talked about the need for ongoing support at the time of the adoption, so were less focused on current service needs. Their accounts suggest areas of improvement to current service provision relate to:
- managing contact with birth parents;
- managing their own emotions when children decide to seek information or make contact with birth parents;
- assistance with medical information/family history for their son/daughter;
- public awareness of adoption issues to be balanced with positive stories, and reflecting the motivations of adoptive parents (e.g., many assumed they were doing a service by keeping a baby out of institutional care); and
- some (limited) need for peer support or professional counselling services for themselves, but more so for their sons/daughters (especially during the search/contact process).
8.7 Final comments from adoptive parents
Clearly, there are multiple complexities surrounding the experiences of adoptive parents, and the information we received from study participants was perhaps more divergent within this group than within any of the other respondent groups. For example, they experienced emotions relating to the role they play in their children's lives, the effects of their child's contact with families of origin, and dealing with their own struggles relating to not feeling like their son/daughter was ever really "theirs". Some of these sentiments are highlighted in the following reflections:
Our adoption experience was very positive. I can't think of anything that I'd change … My sister also adopted a child, but under quite different circumstances, here in Australia. That was also a very positive and wonderful thing for them, with the child also having a re-connection with both her parents when she grew up. Perhaps it is the family culture that makes the difference. (161, 2012)
All past experiences have been positive. We have three wonderful children who have accepted the fact that they were adopted and have always considered us as their parents and have not had issues relating to adoption. Our daughter has had a successful relationship with her birth mother, as do we. Our two sons have no desire to contact their birth parents, although we have assured them that they have our full support if they wish to do so. (953, 2012)
Knowing my son is at peace and happy. I don't think this will ever happen because of the way contact was made. (Adoptive parent, NSW)
My two adopted children have grown up as normal adults and have never shown any sign of problems regarding adoption. (Adoptive parent, Victoria)
That one's own children are not replaceable … even the ones who were never born. It's just not what I imagined or wanted - to feel like a babysitter. (364, 2011)
I am not a mother. These are not my children. I do love them but I wish they had really been mine. (Adoptive parent, Queensland)
8.8 Summary
Wellbeing measures completed by adoptive parents indicate that the respondents to our survey had a healthier mental wellbeing than adoptees or mothers, which was supported by the qualitative accounts. Adoptive parents often did not identify any issues within their family that have arisen from the adoption experience. However, those who did identify issues past and present believed that it was too late to address any issues now or that whatever concerns they may have had had already been addressed.
Many of the comments from the adoptive parents reflect the broader society's attitudes towards adoption in the 1960s and 1970s, which "encouraged" adoption as a way of addressing infertility (Higgins, 2010). Many stated that they were giving a loving home to a child who would have otherwise been left to institutional care, and that the adoption of their son or daughter addressed their own needs and the need of the mother to have someone take her child. However, in contrast to the mothers' experiences of the adoption, most adoptive parents were completely satisfied with the process.
Most of the respondents saw adoption as a way to attain their ideal family. Children were often chosen based on gender, and the number of children they intended to adopt was decided before the first adoption. On the occasions when the adoptive parents conceived a child after they had adopted, they no longer adopted any more children.
The experiences of raising an adopted child ranged from being the best thing in their lives to being the greatest sadness of their life. Many expressed feeling blessed for the opportunity to parent a child. Although some had issues related to the adoption, few mentioned counselling and support as a preferred way of addressing them. They were more inclined to rely on their spouse and friends for emotional support instead. It was also quite common for adoptive parents to rely on church groups for support and acceptance as a family unit.
Most of the adoptive parents surveyed had told their son or daughter about the adoption at a very young age. This may reflect some bias in the respondent sample, as those with positive attitudes and more open communication with their adopted son or daughter may have been more motivated to complete the survey. Some commented that they had been advised by the social worker or adoption agency on how and what to tell the child. It was a common theme to tell the child that they were "specially chosen". The implications of this were discussed in Chapter 7.
Many of the adoptive parents were encouraging and supportive of their son or daughter's search for their family of origin. However, some felt threatened or hurt when the adopted person decided to search. Some of the comments from the survey reflect an underlying suggestion of an "us or them" mentality, and this is supported by what was found from the surveyed adoptees and mothers.
A small number of respondents also expressed concern that the media is biased in favour of mothers and that the reflection of mothers having their babies "stolen" from them was not a true depiction of what had happened to the best of their knowledge. It was reported by some adoptive parents that there was too much negative publicity about adoption that was detrimental to their own mental health and that of their sons/daughters and grandchildren. Addressing this imbalance was a concern raised by some of the adoptive parents.
The main areas of current support needs identified were:
- access to medical information for their son or daughter; and
- support for them and their son or daughter during their son or daughter's search and contact process and beyond.
In conclusion, most adoptive parents believed that the adoption experience had been a positive force in their life such that their children were well-adjusted and that issues that had arisen had already been addressed (with the exception of access to medical records).
9. Other family members
9.1 Respondent characteristics
Responses were received from 94 other family members to the online survey. Table 9.1 shows how these respondents were related to people directly affected by past adoption practices.
There were four survey streams that respondents could follow:
- grandparent of child who was separated from birth parents (1 respondent);
- spouse of a birth parent (4);
- spouse of a person who was adopted (15); and
- other family members (75).
Most respondents were either:
- child of a person who was separated from another child by adoption (22 respondents);
- sibling of a person who was adopted (18);
- spouse of a person who was adopted (15); or
- sibling of a person separated from their child by adoption (12).
| Spouse/ partner | Child | Siblings | Parent | Other | Total | |
|---|---|---|---|---|---|---|
| Person who was adopted | 15 | 3 | 18 | 1 a | 6 | 43 |
| Person separated from child by adoption | 4 | 22 | 12 | 1 | 3 | 44 |
| Adoptive parent | 0 | 5 | 1 | 2 b | 0 | 8 |
| Total | 19 | 30 | 31 | 4 | 11 | 95 |
Notes: a Parents of a person who was adopted were asked a very reduced set of questions (ideally this person should either have answered the birth parents survey or the adoptive parents survey). b Parents of adoptive parents were asked a very reduced set of questions.
A number of the respondents mentioned that the person they were related to who had been affected by adoption was also intending to respond to the survey. A small number of these respondents also participated in the qualitative interviews.
The respondents found out about the study via:
- friend/family member (25 respondents);
- AIFS website (17);
- radio (13);
- newspaper and newsletters (13);
- website advertisement, Internet (8);
- health/welfare professional (6);
- adoption support service (5);
- Facebook, Twitter (3);
- workplace emails (3);
- TV (2);
- poster/flyer at medical clinic (1); and
- other (not specified) (4).
9.2 Search and contact
About two-thirds of the respondents' relatives had sought information about their birth relative, with just over half of their relatives making use of contact/reunion services (see Table 9.2). Fifty-six per cent of their relatives had had contact with the birth relative.
| Yes | No | Unknown | Total | |
|---|---|---|---|---|
| Whether relative tried to find information about birth family | 64 | 23 | 5 | 92 |
| Whether reunion service used | 35 | 19 | 10 | 64 |
| Whether has had contact | 56 | 31 | 5 | 92 |
9.3 Effect of contact on relationships
There were very mixed effects on other family members of the contact between the respondent's relative and the birth relative from whom they had been separated from by adoption. Table 9.3 combines the responses from: respondents who are the spouse of either a person separated from a child by adoption or a person who was adopted, and respondents who are related in some other way to a person separated from another by adoption.
| Effect | Spouse | Other children | Parents | Other family members | Total |
|---|---|---|---|---|---|
| Number | |||||
| Very positive | 4 | 4 | 3 | 10 | 21 |
| Positive | 12 | 16 | 4 | 24 | 56 |
| None | 14 | 9 | 9 | 24 | 56 |
| Negative | 6 | 8 | 10 | 15 | 39 |
| Very negative | 5 | 5 | 5 | 7 | 22 |
| Not applicable | 10 | 10 | 18 | 12 | 50 |
| Total | 51 | 52 | 49 | 92 a | 244 |
| Per cent (excluding not applicable) | |||||
| Very positive | 10 | 10 | 10 | 13 | 11 |
| Positive | 29 | 38 | 13 | 30 | 29 |
| None | 34 | 21 | 29 | 30 | 29 |
| Negative | 15 | 19 | 32 | 19 | 20 |
| Very negative | 12 | 12 | 16 | 9 | 11 |
| Total | 100 | 100 | 100 | 100 | 100 |
Note: a This total is higher than for the other categories, as it includes two sets of responses from the "other family members survey" - once in relation to the effect on themselves, and once for its effect on other family members.
9.4 Services and supports used since separation
Most (61) of the respondents had used some form of services or support to help with issues associated with the adoption experience of their relative. Twenty respondents said they had no need of any support, and 15 said that they did not have any support.
The most common sources of support were:
- other family members (28 respondents);
- friends (22);
- parents (12);
- social worker or counsellor (11);
- psychologist or psychiatrist (11);
- GP (8); and
- adoption support service (7).
The most common form of support received was emotional, followed by psychotherapy or counselling. Most of the support received had been helpful. There were only a few instances where respondents said the support had not been helpful or even unhelpful. However, in general, support from family or friends was more likely to be helpful than support from professionals.
Table 9.4 shows the most common types of support offered and how helpful they were.
| Source | Emotional | Psychotherapy or counselling | Other forms of support not listed | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Very helpful | Somewhat helpful | Not helpful/ unhelpful | Very helpful | Somewhat helpful | Not helpful/ unhelpful | Very helpful | Somewhat helpful | Not helpful/ unhelpful | |
| Other family members | 13 | 13 | 1 | 1 | 2 | 2 | 1 | ||
| Friends | 12 | 9 | 1 | 2 | |||||
| Parents | 6 | 5 | |||||||
| Social worker or counsellor | 1 | 4 | 1 | 2 | 1 | 1 | 1 | ||
| Psychologist or psychiatrist | 5 | 2 | 5 | 1 | 1 | ||||
| GP | 2 | 1 | 1 | 2 | 1 | 1 | 1 | ||
| Adoption Support Service | 2 | 1 | 1 | 1 | 1 | 1 | |||
| Support group | 2 | 1 | |||||||
Other help received included financial support: from parents (n = 1), other family member (n = 2), social worker (n = 1), and adoption support service (n = 1). In all cases, the support had been very helpful. There was also one instance were a friend provided very helpful legal advice, and one instance where an adoption support service provided somewhat helpful legal advice.
9.5 What would help now
I don't hold any grudge towards the government or people of the time. It was how it was. But when it becomes apparent that a significant amount of people have been adversely affected, a genuine response and remedial processes need to be investigated and implemented. You hear so much about the birth mother, and adopted children; less about the birth fathers, or subsequent children. Whatever is implemented needs to address the continuing impact for this situation. (147, 2012)
Many respondents provided long responses to the question that asked what is the single most important thing that would be of benefit to them in helping deal with their past adoption experience.
The most common themes were:
- providing support for people affected - more so for those affected directly, but also in some cases for themselves (17 respondents);
- having contact/reconciling with "lost" relative (12);
- knowing the truth about what happened at the time of the child's adoption - both in general and for their particular relative (11); and
- having access to information about the relative (such as medical history) or to locate the relative (9).
Other matters mentioned included having a public apology (4), contact with others with shared experiences (4), a national approach/register (3), financial assistance (3), and understanding and forgiveness (2).
A few stated that they did not need help, or that nothing could help now (9 respondents).
Only a few respondents stated that their experience had been a positive one:
There hasn't been any problems dealing with the adoption. My sister (who was adopted out) and her family have become a part of our family and us a part of theirs. In fact, my sister's adoptive mum is currently in respite at the same nursing home in which my sister's birth mother (my mum) is a permanent resident, and the "mum's" check on each other, basically on a daily basis! And we all check on the both of them! (77, 2012)
I believe the adoption experience was a positive one for my brother, myself and our parents. My mother acted upon the belief that the facts of my brother's adoption should be known to both my brother and myself at age-appropriate times and in age-appropriate ways. We did not discuss the issue with anyone outside the family, but I do not remember this as posing any particular problems. I believe that we grew up as a pretty average family, and any problems that arose were just those of normal family life and were not related to the fact that my brother was adopted. My brother did tell me that he had made no effort to find out anything about his birth mother as he couldn't really see the point. (102, 2012)
Support
The following are some of the statements made by respondents about the kinds of support that they saw as appropriate:
More services for families dealing with family members who were adopted. My mother suffers from severe trauma and cannot deal with relationships, including husband, children. (80, 2012)
A massive amount of therapy, perhaps cognitive behaviour therapy. But what would really help is if professional psychologists would publicly discuss the damaging and destructive effect of adoptive children on the natural children of a family. The problem is widely known in psychology, but the general public is unaware of how families are destroyed by adoption. (81, 2012)
For my mum to be able to get the help she needs to open up and talk about what happened to her, and the effect it has had on those around her. She is simply unable to talk at all about it and bottles it up, and then explodes unexpectedly, but not about what happened; it is usually something very insignificant, and directed always at me. (147,2012)
My sister was tortured by the whole experience of losing her son. It was so wonderful to see her reunite with him. The problem as I see it now, there were no guidelines in place for either herself or her son. It seemed like, once they met up, they went through a torrent of highs and lows, and there was no network of support for either to fall back on. During her bouts of depression, we tried to encourage her to seek the professional help we knew we couldn't give, but each time she was given a different case worker and had to go through the painful process of retelling her story. Each time, I believe she told less and less of the truth of how she was really feeling. (111,2012)
Having contact
The following are some of the statements made by respondents about wanting contact between adoptees and other birth family members:
To find my granddaughter to complete our family and let her know how much she is loved, especially by her mum. And not a day goes by we don't think of her, and every birthday I ring my daughter and say happy birthday. (97,2012)
I have found out my nephew's name now, but would love to meet him or have some photos of him from birth to now. My brother died shortly after his birth and took the adoption very hard. It is very hard knowing that you have a person out there that belonged to the brother you lost at a young age himself. My nephew is living memory of my brother. (121, 2012)
What hurts deeply is that my husband has to live until the day he dies knowing that maybe he does have someone out there who is related to him. But it's a secret never to be told. That's worse than being told you have no other relatives. A secret harasses a human being because they never get an answer. Plus, my husband thinks somewhere out there, there might be an old man who sometimes thinks about that son he never met, and knows that he will die never knowing anything about him. It's not fair to anybody if they don't get a choice about contact. (131, 2012)
After seeing a variety of TV programs recently about the way babies were taken from unmarried mothers in the 1960s and into the 80s, my husband is now considering trying to find his birth mother. My husband's birth certificate has his adoptive parents' names on it and we don't know where to start. A clear process on how to register to find birth mothers would be helpful. (154, 2012)
I am sad to see my spouse missing out on his biological family. He has siblings and parents alive, but the parents feel it is too long to now introduce him to the others. He felt abandoned, even though he grew up in a most loving home and adored his adoptive parents. Now he feels rejected again … My children also are missing out on their heritage, even though they love and adore their adoptive relatives. (106, 2012)
Knowing the truth
A strong theme in the responses from other family members is the journey of discovery and the need to find out about the "truth" relating to past events. The following are some of the statements made by respondents about knowing the truth:
I don't feel that I personally need anything, but by going through a reunion of my wife and her son, and having other children who were not aware of the adoption, it has opened my eyes to the problems associated with adoption for all concerned. I feel that the subject of adoption needs to be talked about more openly, with better services for birth mothers, adoptees and family. This is needed to help heal all the emotional baggage that has been carried around by all parties. (132, 2012)
Knowing the facts of my mother's experience. (30, 2012)
To know why my cousin was abandoned by the birth mother and her family. (52, 2012)
To know some answers as to why my sister made the decisions she did, and whether either of our parents were aware. (53, 2012)
Access to information
Inadequate information about adoption, and the process of making contact between biological family and adoptees was often mentioned by other family members. The following are some of the statements made by respondents about having access to information:
I know others who have felt really bad because they do not know their biological inheritance/family/history, etc. Just knowing mine makes me understand totally how much they feel is missing, regardless of their type of upbringing. I would just like him not to feel this way, for his biological family to be known to him … Where we come from is incredibly important, but doesn't stop us going forward to other places. (106, 2012)
Adequate and easy access to information, especially how to support my mother/other family members affected. (95, 2012)
Having information about my adopted niece. Tried to find out (with my sisters permission) but run into too many dead ends. (129, 2012)
Apology and understanding
Although the survey did not specifically ask respondents whether they thought there should be a public apology, a number of family members spontaneously identified the need for an apology, an increased community awareness and understanding of the issues relating to past adoption practices, and the current experiences of those affected:
My mum (and I) would probably like some sort of apology, similar to that obtained by state parliament here in WA, but for NSW where the adoption took place. And also from the Catholic adoption agency/church. (142, 2012)
A better understanding by the community of the damage caused by adoption and the lifelong issues faced by all affected by adoption. (124, 2012)
There has always been a person missing in our family. I know the past can't be changed, but perhaps those who were adopted might have a better understanding when there is more public discussion and disclosure of the circumstances at that time. (129, 2012)
My mother died in December 2010. All her children, including the adopted child, supported her in her illness. My mother had low self-esteem and suffered from anxiety, which I believe was a result of the shame she was encouraged to feel. She was forced to surrender her child. She was not able to hold or see her child. It is important to me that this wrong be recognised and that an apology be given to all women who have suffered. (146, 2012)
Contact with others
Another important theme from family members was feeling "alone" in their experience, and wanting to have peer support from others in a similar situation. This was identified as an important area where services would be of benefit:
The most important thing that would be of benefit to me now in helping me deal with my past adoption experience would be to find others that are in a similar position to myself. It would help to know that the support services that are there to support people affected by adoption look behind the "adoptee" and focus on others like myself that have been affected greatly by the experience. This has not been a positive thing for me … I feel like I was the one that was adopted!!!! (88, 2012)
He needs like-minded people to speak with. If he found out about [an adoption support group] he might be open to it. I don't think he's ever talked to anybody ever about it. (28, 2012)
Making contact with other people whose mothers adopted children out prior to their father coming on the scene and having other children. Being able to talk to other children of biological mothers who have not coped well. Talking about how their problems affected our lives so badly. (36, 2012)
Box 9.1 Key service system implications
Other family members who completed surveys or participated in focus groups talked about the need for ongoing support for themselves, as well as their family members. Their accounts suggest areas of improvement to current service provision relate to:
- support to help them deal with traumatised family members;
- wanting help and direct support for their family member affected by adoption; and
- public acknowledgement of (including an apology for) past experiences and its effects to create awareness and greater openness.
9.6 Final comments from family members
Many respondents chose to write some final comments about their experience. The words most commonly written in these comments were about their experience of adoption being destructive or devastating for their family:
- "secrets can destroy individuals"; (27, 2012)
- "it has effectively destroyed our family"; (40, 2012)
- "it destroyed me"; (81, 2012) and
- "has been a devastating experience". (32, 2012)
Many comments reflected the pain that had been suffered by many of those affected, and the ripple effects through family and friends were evident:
Until I was 27 years of age, I did not know I had another sister. My mum was forced (by her parents) to put the child up for adoption as she was unmarried. It is now too painful for mum to establish a relationship with her adopted daughter, as she was forced to give her up, and [she wants to] block the pain of this from her memory. I feel for both my adopted sister and my mum, but there is nothing I can do. (20, 2012)
The biggest impact on me is watching my mother suffer since I can first recall. This has been a lifelong emotional rollercoaster for her/us. (30, 2012)
Giving away her first-born ruined my mother's life, and so that affected my life when I was growing up, as our household was never a normal one into which I could invite friends because I never knew what condition I would find my mother in when I arrived home. (38, 2012)
My mother "adopted" another female child while she was pregnant with me. My mother subsequently gave birth to another daughter after me. My mother rejected her own baby in favour of the stranger's child. My father had to provide for another man's child and endure his wife's rejection of their first baby. A truly horrible situation, but I have found out that it is not unique. There is no data about families that consist of adopted and natural children. All the research focuses on the adopted child - there is no research on the natural child. The natural children are the powerless victims. (81, 2012)
He suffered badly all his life if adoption ever came up while his adopted mum was alive. She would sternly issue threats of being disowned if he ever tried to contact his birth mother. (131, 2012)
I am the child of parents who adopted a baby boy in the 1960s. My adopted brother has never fully come to terms with being adopted and it caused massive stress in his teenage years, in particular for him and our family. My parents nearly divorced because of it and I felt neglected with all the dramas around him. (150, 2012)
One mother whose daughter had been separated from a child by adoption provided an emotional account of the longlasting effects of her role in the adoption of her grandchild:
At my stage of life, 85, there is no benefit. All the damage has been done. Up until recently, I lived with the knowledge that this was all my fault, with the decisions my husband and I had made. Even though my daughter had three wonderful children, a marriage and a career, the thought was always there of a great loss that she had to endure. The not knowing, the secrecy, the bureaucracy, the heartache, the blame, the stigma. It has been a large source of grief and heartache to myself knowing that you had failed your child in their eyes. My daughter could not forgive me, as her daughter could not forgive "that woman who gave me away". So the need for more counselling, not only for girls in that situation, but for parents, is paramount to stop the blaming game. Only through hindsight can things change for the betterment of all. The most important thing that would benefit everyone - mother, child, parents, all that were touched by this experience - is forgiveness. How do you achieve that? Only God knows. It is all too late for the government or whoever to say "sorry". (39, 2012)
Some mentioned feelings of loneliness through lack of understanding from others:
I would have to say it is very lonely having had a mother who was forced to give up a child. You cannot talk about it, and mostly people do not understand anyway, if you do. (36, 2012)
My cousin is trying to contact her birth mother. In the last few years, both her adoptive parents have passed away and she is feeling isolated and alone. She is not really close to most of her family due to some rebellious behaviour during her teens after she found out she was adopted. She had issues with alcohol and binge drinking; no criminal or drug issues. (52, 2012)
My sister's life is becoming quite isolated because of fears and anxieties and loss of friends because of the unreliability of her behaviour. 62, 2012)
One person felt that it may have been better if her husband had never found out that he was adopted:
Since my spouse found out the true story of his past he has felt his life to that point was a lie … An attempt to reunify them was made by his mother's psychiatrist, who was treating her for anxiety and depression. He was inappropriate and damaging and he only stopped pursuing my spouse when I threatened to report him … [My spouse] has become more reclusive, more dependent on me and more remote from me. He tried counselling a couple of times but found it unhelpful. I honestly believe it would have been better for him, and his mother and for me if he had never found out about his true background. (18, 2011)
However, most people indicated that it was important to know the truth. The following sums up the importance of a biological family for many:
Family don't always turn out to be your best friends in the world, but you are always connected by the sharing of personality traits, behavioural traits, phrases you use, the way you stand or even the expressions on your face. You belong to a group and even when you are alone you are not alone. You are connected to someone who's very much like you in various ways. (131, 2012)
9.7 Summary
The ripple effects through family are very evident from the information provided by respondents. There was a diversity of relatives who completed the survey for those affected by the adoption experiences of a relative (including siblings of persons adopted, spouses of mothers, and subsequent children mothers). There was also a range of experiences with the search/reunion and contact of their relative and the family of origin, some of which resulted in positive effects on relationships, while others were negative.
Although the majority had support, most believed that there needs to be a facilitated access to support (counselling and therapy) for themselves and their relatives regarding the issues arising from the adoption. Other needs included assistance with the contact and reconciliation with the "lost" relative, a provision of the facts regarding the adoption, and improved access to information about the family of origin (such as medical history). Additionally, there was a sentiment for the delivery of an apology to those affected by past adoption experiences from the agencies involved in the adoption practices.
In general, other family members had been adversely affected by the adoption experience (although a few did express positive experiences). Most talked about the ways in which they would benefit from access to support to deal with issues arising from past adoption experiences, including information, making contact, peer support, community awareness, understanding, and contrition.
10. Service providers
Another major component of the study was to collect information from professionals (such as psychologists and counsellors) who work with people affected by their experience of adoption. They were asked about the effect of these experiences on clients and the needs of those who have been adversely affected. Information was also obtained on the types of services offered and, where possible, details obtained on usage.
Although the information collected from service system professionals is not intended to provide an audit of services available to people affected by their experience of adoption, it provides sufficient information to understand the amount, nature and type of services available. In addition, the insight of professionals working in the field into the effects that past adoption practices have had on clients, and what the needs of those who have been adversely affected are, has helped in framing appropriate best practice models.
10.1 Design
An online survey (using LimeSurvey) was developed for two target groups:
- managers of organisations that provide adoption-specific services; and
- general providers of adoption-specific support and services.
The main aim of the managers survey was to collect information about the types of services currently provided by organisations, client profiles, the perceived needs of clients, and how these needs could best be met.
The general service providers survey sought information from counsellors, social workers and other health and welfare professionals who provide services to individuals who have been affected by adoption. The survey included questions on:
- characteristics of respondent - age, gender, field of qualification, years of experience;
- client needs - perceived needs (such as counselling, search and reunion services, or mediation services) and changes in demand; and
- professional training - types of training undertaken, benefits of training and methods of assessing benefits of the training.
Both surveys included a mix of closed and open-ended questions.
10.2 Communication strategy
The service providers surveys were the final surveys to be launched for the Past Adoptions Experiences project, in early November 2011. There was some awareness in the service provider community of the research project into the service needs of people affected by past adoption practices through the publicity generated for the surveys of persons affected. Many agencies had already been asked to publicise the survey for individuals who had been affected by past adoption practices, and other health professionals had received promotional emails or information via newsletters. At this point, the communication strategy focused on raising awareness of the survey among service providers, as well as reinforcing the awareness messages and the invitation to participate among the general population. The strategies employed are described in section 3.4.
The first phase of the service providers survey communication strategy involved sending regular email to a wide audience of professionals and key interest groups, informing them of the study and including a link to the online survey. Organisations approached included:
- Commonwealth Government: National Health and Medical Research Council, Australian Research Council, Centrelink Media Unit, Medicare Australia;
- state and local government: Australian Local Government Association, Adoption Information Unit (NSW), Family Records and Inter-Country Services, Department of Human Services (Victoria), Adoption and Permanent Care Unit (ACT), Queensland Health Mental Health Services;
- child welfare organisations and peak bodies: Families Australia, Australian Research Alliance for Children and Youth (ARACY), Australian Childhood Foundation, National Association for Prevention of Child Abuse and Neglect (NAPCAN), Association of Child Welfare Agencies (NSW), Victorian Centre for Excellence in Child and Family Welfare, and individual agencies such as Barnardos, Benevolent Society, Anglicare, CatholicCare, UnitingCare/Wesley;
- networks and agencies for seniors: Council on the Ageing (COTA), Australian Seniors Computer Clubs Association, Older Persons Electronic Network, Aged and Community Services (WA), Grandparents Australia Inc., Association of Independent Retirees, Meals on Wheels;
- adoption-specific services: Relationships Australia (SA), Origins, Jigsaw, Victorian Adoption Network for Information and Self Help (VANISH), Association of Relinquishing Mothers (ARMS), Post-Adoption Resource Centre, Adoption Research & Counselling Service (ARCS);
- non-government organisations: Red Cross, Mission Australia, Lifeline Australia, The Smith Family, Benevolent Society, St Vincent De Paul;
- health and social welfare organisations: Mental Health Council of Australia, Australian Healthcare Association, Australian Psychology Society, IHealthCare, The Royal Australian and New Zealand College of Psychiatrists Health Insight, Drug & Alcohol Services (SA), Alcohol Education & Rehabilitation Foundation Ltd, Australian National Council on Drugs;
- parenting organisations: Parenting Research Centre;
- women's organisations: National Council of Women of Australia, National Foundation of Australian Women, National Council of Single Mothers and Their Children; and
- radio: AusRadioStations, ABC Radio National, local ABC radio (Melbourne, Canberra, and Sydney).
Unfortunately there was limited response to this first phase, so a targeted follow-up was undertaken.
One of the challenges faced was the lack of a database of professionals or agencies who work with those affected by adoption. This was later re-enforced as being a service system failure in survey responses from the service professionals themselves, as well as from mothers and adoptees who found the service system difficult to navigate. For the second phase, a database of organisations and agencies working with people affected by adoption was developed, as a starting point for targeted recruitment.
The second phase of the communication strategy involved making contact with organisations by telephone. It appeared that although many of the professionals working within the agencies were aware of the study, they had not completed the survey. The contact person was encouraged to complete the managers survey on behalf of the organisations, to ask professionals within their agency to reply to the general service providers survey, and to disseminate the link to the survey through their networks.
10.3 Response
As can be seen from the figure below, the targeted follow-up was very successful in improving the response to both surveys (Figure 10.1). At the end of the survey period, 15 responses from managers and 46 responses from general service providers had been received. Almost all of the key service provider agencies responded to the managers survey.27
Figure 10.1: Responses to service provider surveys, Phases 1 and 2
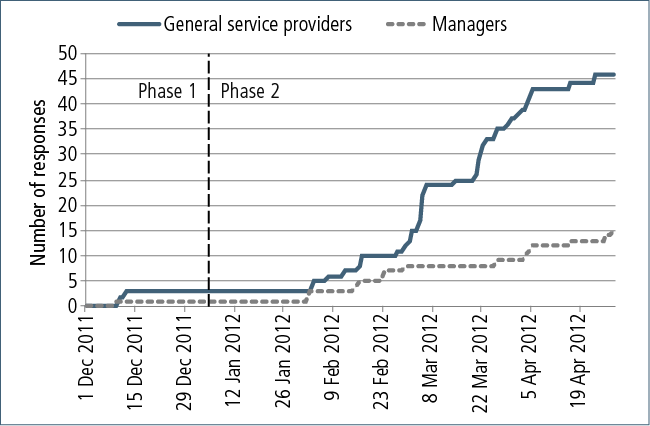
10.4 Managers survey
Services
There were 15 completed responses from managers in organisations that work with people affected by adoption: 5 government and 10 non-government.
In general, the non-government agencies were small, with all bar one having fewer than 20 paid staff. Three of them had paid staff only, four had a mix of paid staff and volunteers, and three had volunteers only.
Almost all of the organisations offered adoption-specific counselling and support (n = 13) and search and reunion services (n = 12). Other services offered included information and referral (n = 9), adoption advocacy (n = 7), general counselling and support (n = 5) and mental health services (n = 2).
According to the managers, the service most used by clients was specialised counselling services. Seven had clients who used medical or mental health services, and two had clients who were accessing services for alcohol and other drug support. When respondents were offered an opportunity to elaborate further or suggest other services that their clients used, services mentioned included support groups and search and mediation services.
Professionals employed by these agencies included:
- social workers (n = 13);
- generalist counsellors (n = 5);
- psychologists (n = 3); and
- mental health workers (n = 2).
Although two-thirds of respondents believed that there had been no real change in the demand for services over recent years, the remaining third said they were experiencing an increase in demand. None of the managers thought that the demand for the services was decreasing.
Clients
Almost all organisations offered their services to all people affected by adoption; that is, to mothers (n = 14), fathers (n = 13), individuals who had been adopted (n = 13), adoptive parents (n = 14) and other family members (n = 13). Two respondents also commented that they provided services to people separated from families by foster care arrangements.
Most of the organisations (n = 11) always asked their clients whether they had had a past adoption experience, and only one organisation never asked.
A large majority of the organisations (n = 13) collected some type of information about their service users. Most (n = 10) knew the number of times their clients had used the service, more than half (n = 8) collected information on the types of services used and the demographic of their clients, but fewer than half (n = 6) knew the length of time their clients had been engaged in support or the types of referrals made or given to their clients. Two of the organisations mentioned collecting data on the number of attendees at support groups and on the clients' experiences of adoption.
It would be useful to obtain this information from the relevant agencies when further developing best practice models.
All respondents had some clients who found their services through their own research. The other common ways in which clients found services were: from other clients (n = 14); other word of mouth (n = 11); or referrals from another related agency (n = 14), generalist welfare services (n = 11), another section of the agency (n = 7), or a medical specialist (n = 6).
Referrals
General services are very poorly informed about the impacts of adoption, and generally shared the same myths and misunderstandings about adoption as the general public, but give these misunderstandings an air of professional certitude. (Manager)
There were divergent views about the capacity of existing systems to effectively meet the needs of people affected by past adoptions. Only one respondent strongly believed in the capacity of existing referral networks to be helpful in relation to appropriately addressing the effects of past adoption experiences. Three respondents mostly agreed, four neither agreed nor disagreed, another three mostly disagreed and one respondent strongly disagreed.
In general, services to which managers provided client referrals included: adoption agencies, adoption support services, mental health and counselling services, and search and reunion organisations. Referrals were for: search and reunion support, counselling support, accessing records and information, and mediation services
In terms of referrals received from other agencies, most were either from government adoption information services, other adoption agencies or counselling services. The types of support sought from these referrals included: support (searching support, parenting support, support groups); information (such as access to records); assistance with search, reunion and mediation services; counselling; and networking.
Managers also indicated that there are gaps in the current referral system. This was more acute in remote and rural communities, but also viewed as being insufficient in metropolitan areas. In one state there is a complete absence of a specialist adoption service dealing with contact and reunion. Other concerns identified were:
- lack of information about the effects of adoption;
- absence of services and other resources to draw upon;
- access to affordable services; and
- insufficient awareness of adoption issues within the mental health community and among "younger" counsellors.
Training
Two-thirds of the organisations that responded to the survey had most or all of their staff trained to work with people who had past adoption experiences. Only two organisations had no trained staff, another two had some trained staff, while one organisation stated that staff had generalist knowledge that could be applied to a variety of client needs.
Three-quarters of respondents (n = 12) stated that they would be supportive of the development of a training package to enhance the skills and knowledge of the workforce, while three were unsure about their support for such an initiative.
When prompted to propose ideas as to what the training package should include, some key areas suggested were:
- the historical and social context of adoption;
- information about the effects of adoption experiences, including inter-generational effects, bonding, attachment and identity;
- awareness about search, reunion, mediation and making contact, including the potential effects of negative outcomes of such processes;
- specialist training in counselling for grief, loss, bereavement and trauma.
Respondents were also asked to suggest any services that they were aware of that offered an effective model of care for people affected by their experiences of past adoptions. Services that were specifically mentioned included:
- Adoption Research and Counselling Service (Western Australia);
- Adoption Jigsaw (Western Australia);
- Post Adoption Resourse Centre (New South Wales);
- Post Adoption Support Queensland (Queensland);
- Post Adoption Support Service (South Australia); and
- VANISH Inc. (Victoria).
There was no indication as to what made these services effective. Further investigation into the services would provide insight into existing best practice models.
Client needs
Managers perceived the needs of their clients as falling broadly into four key areas:
- awareness - both clients and the general public need to have a greater awareness of the issues relating to adoption and to acknowledge such issues;
- access to information - clients need access to information about the adoption, whether about the relinquished child, the birth family or medical information;
- counselling support - clients need support through mental health services in dealing with adoption related issues such as loss, grief and trauma; and
- search, reunion and mediation support - clients need to be assisted in the search process and subsequent contact, and for mediation services to be available when needed.
There was a variety of reasons that managers identified as preventing these needs being addressed:
- lack of understanding - lack of general awareness about issues related to adoption, including in schools;
- inadequate training - poor levels of training within and outside the adoption sector;
- clients' own perceptions - clients may be unable to identify their own needs, often believing that information is the solution;
- cost of services - often prohibitive;
- knowledge of services - clients are often unaware of the existences of services that could assist them, or they do not value the services available due to lack of understanding of the complexity of adoption issues;
- geographical distances - services are beyond the reach of clients who live in remote and rural areas; and
- restricted access to information - legislation prevents ease of access.
Addressing client needs
Common strategies to address client needs that were identified by respondents to the managers survey were:
- more training and tertiary courses for professionals - better professional development and training in adoption-related issues, including education at the tertiary education level for a range of welfare professionals;
- enriched public awareness and information - among both the professional community and the general public. A "concerted effort" is needed so that the "lifelong impacts of adoption" can be addressed; for example by increasing promotional material, with information about adoption issues and relevant services being made available to people affected by past adoption experiences;
- improved funding - for specialised adoption services, and to assist people on a fixed or low income who struggle to afford the costs of adoption-related services;
- better networking between agencies - to facilitate communication between services;
- investment in counselling services - encompassing all aspects of investment: funding to support ongoing or intermittent counselling, training more counsellors, and publicising the availability of these services; and
- mandatory interviews - one respondent urged for the return of the "mandatory interview", with the aim of providing those receiving information about their adoption with non-therapeutic counselling.
Further comments
Respondents were invited to make additional comments about service provision for people affected by past adoption practices:
There are limited services offered to young children to explore their birth story/adoption questions or even support for new adoptive parents. Limited services for birth parents to access after their child has been placed and counselling has finished with the adoption agency.
Adoption is a serious and complex issue, and when undertaken, care should be taken to fully support all those it impacts through a full life journey - not just at the point of adoption.
We have a lot of specialist knowledge in agencies already established, the issue is insufficient funding.
Those of us involved in search need access to records along the lines of the Special Search Service in NSW. We waste a great deal of time and therefore cost and emotional angst trying to locate people because we can only access records in the public arena.
Many of the members of ARMS (Vic.) have died without being able to find out about the welfare of their child or to contact that child. Therefore there is urgency about setting up the training proposed in this survey.
These comments highlight the complexity of the issues, the perception of inadequate funding, and the urgency of the needs of those affected by their experiences of past adoptions.
10.5 General service providers survey
Respondent characteristics
Of the 46 respondents to the general service providers survey, 41 were female and 5 were male. Respondents were aged 25 years and over, with almost half aged 55 years and over (Figure 10.2). The majority of respondents had a postgraduate qualification, with only a small number not holding a higher education degree of some kind (Figure 10.3).
Figure 10.2: Age distribution and gender of general service provider survey respondents
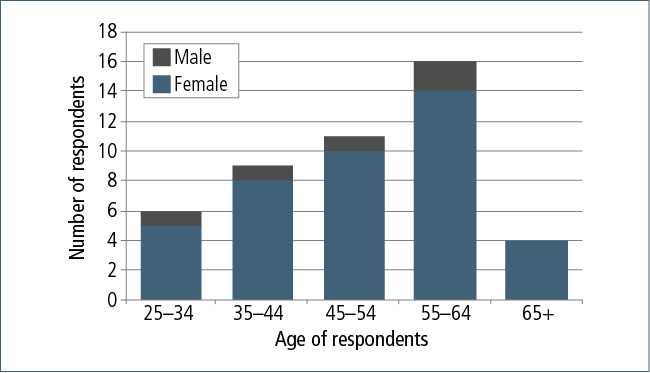
Figure 10.3: Postgraduate qualifications of general service provider survey respondents

Most of the respondents had qualifications in psychology (n = 17), social work (n = 15) or counselling (n = 15). Other fields of qualification were: social science (n = 7), mental health (n = 5), nursing (n = 3), education (n = 3), alcohol and other drug support (n = 3), and community services (n = 2). There was also one medical practitioner (GP or other), one psychiatrist and one criminologist among the respondents.
Services
The most common services provided were: counselling (psychologist, psychiatrist and other), search and reunion services, general information, referral, and mental health services (Figure 10.4). The majority of respondents had more than six years of experience, with only a few having less than two years' experience and none having less than one year of experience.
Figure 10.4: Types of services provided and years of working experience of general service provider survey respondents
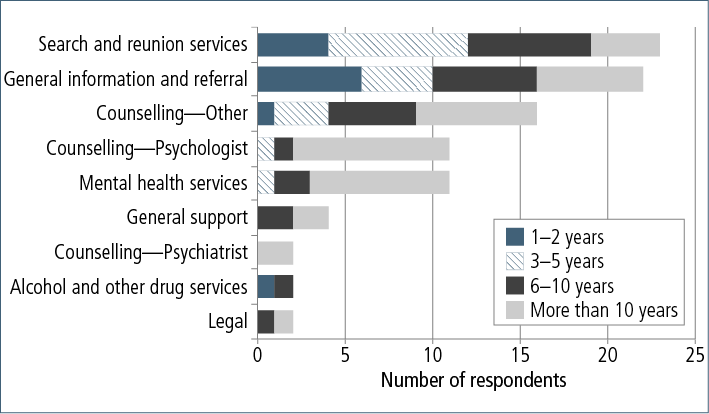
Other services offered include:
- advocacy/awareness raising;
- social research projects;
- consultation regarding legislation and policy;
- parenting support;
- family mediation; and
- release and restriction of adoption records to people affected by past adoption.
Clients
The majority of respondents provided their services to mothers separated from a child by adoption (n = 40) and adoptees (n = 40). A smaller number had other family members (n = 31), fathers (n = 28) and adoptive parents (n = 28) as service users. Other types of clients included people separated from families due to foster care arrangements, Forgotten Australians, prospective adoptive parents, and the broader community in general.
Most respondents (n = 16) had more adoptees as clients than any other group, with a smaller number of respondents (n = 6) with more mothers as clients. The other respondents either stated that the types of clients they had fluctuated or did not select a group. Organisations that only saw mothers were likely to be peer-based support networks. It was noted by some that there was a noticeably smaller portion of fathers, adoptive parents and other groups accessing services.
Twenty of the respondents worked only with people affected by past adoption experiences. Of the respondents who worked with other clients, nine stated that it was standard practice to ask if the client had any past adoption experiences; however, the majority (n = 15) only asked this question if the client mentioned it in the course of their interaction.
The following are some of the statements made by respondents regarding the demographic of their clients:
I would see more adoptees than relinquishing mothers, but that is nothing to do with my role as a service provider. More to do with age, as older people are reluctant to seek psychological services and/or would be referred to aged care services in the particular set-up I work in.
Relinquishing mothers are increasing lately. Previously it was more adoptees. Rarely do adoptive parents contact us.
Predominantly users of services are adoptees and birth mothers.
Equally adoptees and birth mothers. A lesser percentage of birth fathers, spouses of adoptees and adoptive parents.
Birth fathers always seem to be the "also rans" or the faceless group. Raising their profile is important.
Yes, adoptees are referred to me more often than relinquishing parents. Adoptive parents rarely access my services.
There are variances between the groups accessing the agencies in the types of services they are accessing and the length of time clients are in need of such services. Reasons for accessing the service and pathways of referral were also varied; however, survey respondents identified some trends among the client groups:
Our clients all report trauma related to being separated from their birth families, community and culture.
I tend to find adoptees access services more than relinquishing mothers, but relinquishing mothers require a lot more support when they do access it.
In my experience, there are more adoptees seeking support than relinquishing parents, although they do not always seek support for their adoption - it can be for other issues.
Unfortunately, unacknowledged birth fathers and non-adopted siblings have more difficulties in accessing information and services.
A minority of respondents were not aware of any particular service users who were accessing support in relation to their past adoption experiences any more or less than others.
One service provider commented on the role of media and its effects on the types of clients they saw. The participants cited research that indicated a link between an increase in relinquishing fathers accessing support and media coverage given to that particular group.
Awareness of services
Only a small number of respondents believed that their clients were well or very well informed about the services offered (Figure 10.5). The majority of clients were either somewhat or not very informed of services available to them.
Figure 10.5: Clients' level of awareness of services available
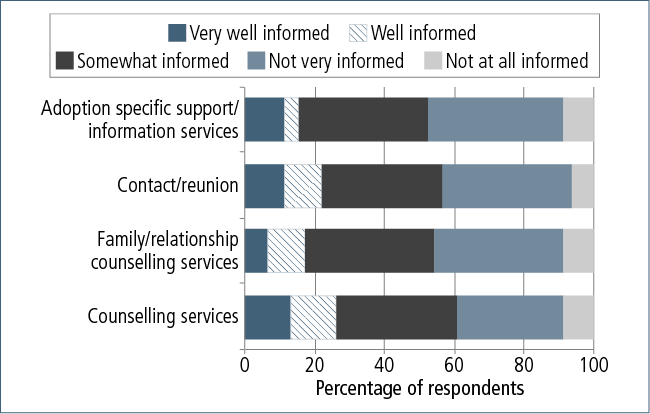
Client needs
Counselling and support
Someone to talk to who understands what they are feeling. Many ask about counsellors, but it is very hard to find any who have appropriate understanding of adoption issues.
A large portion of respondents believe that their clients are in need of counselling and support services; however, the current availability of such services was considered to be inadequate and too costly. Survey respondents were for the most part supportive of the provision of funding to make counselling more affordable to clients:
Access to support and counselling by workers who understand the field well.
The Medicare ten-session scheme is not adequate or effective in my view, and some independent research into this is required.
Informed counselling, freely available.
It was also considered imperative that the counsellors who provided the support were well trained in assisting people with past adoption experiences to deal with issues such as:
- grief and loss;
- identity;
- shame;
- trauma;
- excess feelings of guilt;
- rejection;
- emotions of anger/hurt;
- difficulty in maintaining friendships or close relationships with family (attachment issues);
- anxiety; and
- self-confidence issues.
Search, contact and mediation support
Respondents noted that clients needed support with search, contact and mediation services. This included assistance with the contact phase, mediating between families, and informing their own families of their adoption experience (mothers) or their intent to find their birth families (adopted individuals). Intermediary and mediation services are needed for clients who require assistance during the reunion process in managing the contact with the birth family.
Access to information
Another common response to the question of identifying the main needs of clients concerned access to information and records. This included information about the family of origin, wellbeing of the child, and medical records:
They need to know their identity and where they have come from. Including any medical information.
Accessing adoption records and identifying information about biological family.
For people to find out all information about their adoption, including birth fathers' names and people's details. It would then be up to the individual if they want contact, but they need to know their history and identity.
Awareness and validation
Respondents believed clients needed more public awareness about and validation of their experiences. The word "validation" was used frequently to express this need:
The relinquishing mothers' stories need to be heard and validated. The children's losses need to be heard and understood.
To feel validated and supported.
Validation of their experience.
Validation of experience. Connecting with others who understand.
For awareness of adoption and how many people have been affected by adoption. To be discovered in society so that they can now speak out … To be heard and to be able to speak about their loss.
Opportunity to have their stories heard and experiences validated.
One respondent summarised their perception of clients' needs as follows:
Varies … Their needs from us are to feel understood and heard, which they report is not usually their experience in attending generalist services. Needs include: being able to integrate their adoption experience so that it no longer dominates their lives and prevents them from functioning to their full potential; being able to prepare for contact with birth family; managing contact with birth family; managing triggers and other trauma responses; creation of a coherent narrative around their experience; replacing maladaptive behaviours with more adaptive ones; creating and maintaining healthy relationships; validation; space and support to grieve losses; the list goes on and on …
Barriers
What seems to be affecting the needs of people affected by adoption from being addressed is the lack acknowledgement by the federal and state government agencies of the true impact of adoption, even though they claim this is well understood.
Although some respondents believed that there were no issues preventing the clients' needs from being addressed, most believed that there were obstacles. The most common challenges were:
- availability - insufficient services in regional and metropolitan areas and a lack of counsellors trained in understanding issues stemming from past adoption experiences;
- financial - inhibitive costs for client, and a lack of funding for agencies providing services to expand and promote their services;
- client's non-compliance - clients deciding not to access support, or not accessing appropriate support (due to guilt, fear previous communications);
- access to information - challenges with locating birth families, privacy laws too stringent, lack of uniformity of access policies of Registrars of Birth, Deaths and Marriage, delays in accessing documents and information, and the government policy of "user pays" for information;
- inter-agency networking - no unified process pulling the different but related needs into one place, a poor integrated broad-based service, with an inadequate referral network, and lack of knowledge of services:
In relation to information, the process can be confusing and you are required to contact various organisations
- misinformation from media - television programs such as Find My Family encourage an inaccurate perception of adoption issues; and
- insufficient awareness - clients unaware that the issues they face are "common issues", and lack of awareness in the general community and therefore scarce resources to support people who need the services.
Addressing client needs
The most common suggestion was subsidising the cost of counselling. Other suggestions included:
- encouraging publicity and awareness of the past practices of adoption as well as the availability of services for those in need to improve the general public's understanding and help strip the associated shame and stigma. Suggestions for how to achieve this include:
- interviews/discussions in the media;
- educating teachers, hospital staff, allied health practitioners, mental health workers, counsellors, social workers, ministers of religion and so on; and
- government awareness campaigns;
- improving education and training of professionals (such as counsellors, social workers, mental health professionals) who work with people affected by past adoption practices. Suggestions for how this could be achieved were by:
- including adoption as a topic in social work training curricula;
- publishing good practice guidelines;
- funding conferences for national post-adoption workers;
- disseminating information and research; and
- conducting research into topics of adoption (especially longitudinal studies).
- promoting inter-agency networking to improve the liaison between organisations, agencies and state and territory government agencies around best practice issues. Suggestions for how to achieve this include:
- developing a practitioner network similar to the Mental Health Practitioner Network; and
- standardising legislation across jurisdictions;
- facilitating access to information for individuals (and agencies representing them) who are seeking information about their birth family. Suggestions for how to achieve this include:
- developing consistent access policies from the Registrars of Births, Deaths and Marriages across all states;
- digitising records and housing a searchable database in each state;
- simplifying the process of accessing information;
- waiving fees for accessing records; and
- reviewing privacy laws in the context of adoption;
- increasing funding to facilitate access to services for clients and to fund training and self-help initiatives; and
- providing access to specialist counselling services for all people affected by their experiences of past adoption, in a format similar to the Find and Connect service for people who have been in out-of-home care as children, whether as Forgotten Australians or former child migrants28 (see <www.findandconnect.gov.au>).
Knowledge and skills
All respondents (n = 46) felt either very confident or confident working with clients who had experiences of past adoption. None of the respondents to the survey felt unconfident working with that client group.
The large majority (n = 38) felt either confident or very confident referring their clients to appropriate support services. Only a few (n = 8) did not feel confident in this referral process.
The respondents rated their knowledge of issues arising from past adoption experiences as at least moderate, with most rating their knowledge as very high (n = 20) or high (n = 14).
Training
No formal training, but 16 years on-the-job training working at Adoption Jigsaw and first-hand experience as a birth mother in [sic] reunion with my son for 20 years. This is invaluable, because as pioneers in this experience, we have had little formal guidance to assist us.
Well over half of respondents (n = 28) had received training or attended continuing education relating specifically to issues associated with adoption. Reasons for not having training included:
- not aware of suitable training (n = 15);
- could not afford training (n = 3);
- no support from workplace to attend training (n = 2); and
- no time for training (n = 1).
Some participants found that their own personal adoption experiences provided them with sufficient knowledge.
Other types of training that respondents found useful in assisting people affected by experiences of adoption included programs on:
- grief and loss;
- family formation;
- child development;
- general and specific counselling; and
- attachment theory.
A few respondents (n = 2) increased their knowledge through reading books on issues relating to adoption.
Training outcomes
Training increased my knowledge and ability to be sensitive to all parties affected by adoption.
Respondents found that the adoption-specific training was helpful in:
- understanding the personal lived experiences of those affected by past adoption, and the involvement of adoptees, adoptive parents, or relinquishing mothers themselves, independently or within the "adoption triangle", was found to be helpful;
- learning about other adoption services in order to make positive referrals;
- informing on the results of research from both national and international speakers, and the practice tools arising from the research in relation to adoption;
- improving understanding of the psychological issues associated with adoption and search - including grief, loss and trauma - for both those directly affected by adoption and their wider families; and
- providing a greater knowledge of applicable legislation relating to adoption and how it might affect the clients' search for their birth family.
All respondents believed that the training provided them with a positive outcome. Respondents found that the training:
- was relevant to their current work (n = 26);
- increased their knowledge relating to the effects of past adoption practices (n = 22);
- increased their confidence in responding to the needs of clients (n = 22);
- increased their knowledge of other services (n = 15); and
- increased their confidence in being able to refer their clients to appropriate services (n = 15).
One respondent commented that the training was helpful in:
Fitting personal stories of people who are parties to an adoption to theory and practice, e.g. stories of disclosure or non-disclosure of their adoption status to an adopted child by the adoptive parents, and how this fits with identity formation, the development of family scripts.
Half of those who attended training mentioned that evaluation forms, client feedback and attainment of client goals were used to assess the benefits of the training.
Future training
Most respondents (n = 35) wanted further training in matters concerning past adoption experiences. As mentioned earlier, some participants found that their own personal adoption experiences provided them with the knowledge they needed and therefore they did not feel the need for further training.
The types of training that would be most useful to the respondents were:
- counselling skills in issues specific to adoption, such as trauma, grief, loss, identity issues, attachment theory and other potential issues that are common in adoptees;
- training in reconciliation, intermediary services to provide assistance in the search and reunion process:
Supports required with reconnection. Importance of making it meaningful and not rushing it. Supports for someone coping with someone that does not want to reconnect.
- information on legislation affecting issues of adoption, such as access to records.
It seems evident from other respondents that training packages on these subjects have been developed.
Further comments
Respondents provided some additional insights relating to the issues of past adoption and the service needs of those affected:
It is really important that some consideration is given to the online world of adoption and its potential and risks. I am a member of twenty Facebook groups for adoptees and I am constantly sharing information and support through these and other online forums. Some central online repository for information is necessary for Australia where latest research, statistics, service provider information, search information etc. etc. can be obtained. The lack of services in this regard pushed people to search for help online. I have seen (and personally experienced) that adoptees in particular respond well to other adoptees, who they see as the only people in the word who understand them.
It would be wonderful to have more adoption-specific services to rural and remote areas.
Adoption is a complex social structure. Many people experience it positively, but those who have been traumatised by their experience are often very isolated and overwhelmed by grief and loss. It is important that these traumatic experiences are addressed retrospectively for those affected. It is also important to ensure that these traumas do not continue into the future.
I also believe that public education in relation to reunions is essential. People often expect quick and happy results when searching and reuniting with their families. I would like to see people educated about how reunions should be taken slowly, and that the desired outcomes are not necessarily always achieved.
There are long-term and wide-ranging impacts of past adoption practices that require ongoing support. Recognition of this via funding of services would be extremely beneficial to this client group.
The government should consider that although protection policies are a thing of the past, the removal of Aboriginal children (by DOCS or similar) and their placement within non-Aboriginal families continues unabated. This will result in ongoing need for services such as Link-Up until these practices stop.
This is a very specialised area of client group, and people's experiences are many and varied. Counsellors need to be sensitive to varying client experiences.
Also, for society to be told that reunions can and do work, as I have had many. But unfortunately, the way society is, they only dwell on the negative, and that can be why many people chose not to reunite - because they have heard the stories about ones that have not gone well. This can be due to the people themselves, but others don't think that far unfortunately.
Adoption impacted on a very large number of people in the past. It was probably overused. I suspect the backlash has been too much and it is now probably under-used.
An integrated model of service that includes the self-help model.
I would also like to see more publicity around the findings of the Senate Inquiry. Firstly so that adoptees understand that they were not unwanted babies. Secondly to let the many women who have never been able to talk about or share their past trauma of losing their child to adoption, know that there are support groups and welcome places for them.
Box 10.1: Key service system implications
The most common suggestions by respondents for enhancing the services provided by the support system were:
- improving access to information and awareness on:
- services operating and a referral list of trained colleagues;
- available training;
- developments within the adoption community; and
- best practice and procedure;
- increasing funding for:
- employing more caseworkers, researchers administration support and staff;
- subsidising counselling and other relevant services for people affected by adoption;
- allowing professionals more time to work with clients;
- promoting the services offered by agencies;
- arranging training, seminars and workshops; and
- research into issues relating to adoption and the various healing modalities that can be employed to assist the professionals providing support;
- providing materials to share with clients on adoption-related issues:
Materials and resources to share with people affected by adoption, from simple fact sheets with information about which agencies offer which services in each state, to material describing the impact of adoption and sharing stories about reunion, healing journeys.
Other suggestions for improving the services provided included:
- offering online support services to provide access to clients in rural and remote areas;
- encouraging face-to-face interactions with clients when providing adoption information, allowing counsellors who have established a relationship with their client to pass on sensitive information;
- providing external clinical supervision and support;
- promoting awareness by government and other relevant agencies about past adoption practices; and
- enhanced cooperation between various agencies to provide support for people affected by past adoption experiences.
10.6 Summary
The feedback from the service providers corroborated what persons affected by adoption told us about their experiences of accessing services: that there were not enough services, the professionals were often not knowledgeable on adoption-specific issues, there was a lack of awareness of the services, and the cost of services made long-term involvement prohibitive.
The service providers involved in the survey were mostly highly qualified professionals with many years of experience working with people affected by adoption. They had very similar perceptions of the service system, its strengths and its weaknesses. Although many of the service providers involved in the study had had training of some sort and were confident in addressing the needs of their clients, most felt the need for further training.
A strong message from the service providers was the need for financial support for counselling, both for the development and conduct of training in adoption-specific issues, and to assist people affected by past adoption experiences to access counselling. One suggestion was for a service implementing a model similar to Find and Connect, a service developed to address the needs of people who have been in out-of-home care as children.
Another recurring theme from service providers was a need for more awareness around the issues stemming from past adoption experiences, and more promotion of the services available. Respondents advocated for public awareness campaigns involving the media, government agencies and other relevant organisations. As with the mothers, service providers believed that validating the experiences of those affected by past experiences of adoption was fundamental, and a first step to addressing the stigma associated with adoption.
Many respondents were also mindful of the need to address the inadequate availability of information on adoption-related issues, both for organisations about best practice models and for clients themselves. Respondents advocated for the facilitation of access to information, and wanted increased funding for search, contact and reunion services, training and inter-agency cooperation.
Respondents supported the development of a system-wide network that can connect clients with services, and support services with other related services. Furthermore, search and reunion organisations advocated for a better relationship with government agencies, to assist in the sharing of information.
In developing models for best practice, detailed examination of successful training referred to by respondents could be conducted to determine the key features of its success.
27 Given the limited number of participants in the service providers surveys and the small pool of adoption services, we have not included quote attributions to ensure confidentiality/anonymity of the participant.
28 Former child migrants are adults who were sent to Australia as children as part of inter-governmental child migration schemes in the period following World War II (up to the 1970s), and who were subsequently placed in homes, orphanages and other forms of out-of-home care. It is estimated that around 7,000 children were sent to Australia from the United Kingdom and Malta under these schemes, of which about 6,700 were from the United Kingdom.
11. Discussion
The aim of the National Research Study on the Service Response to Past Adoption Practices was to utilise and build on existing research and evidence about the extent and effects of past adoption practices, in order to strengthen the evidence available to governments to address the current needs of those affected.
The aims of the study were to:
- identify the long-term effects of past adoption practices as they relate to current support and service needs of affected individuals, including the need for information, counselling and reunion services, based on analysis of the information provided by study participants;
- identify the extent to which affected individuals have previously sought support and services, and the types of services and support which were sought; and
- present findings based on the analysis of the information from the study that could be used in the development of best practice models or practice guidelines for the delivery of supports and services for individuals affected by past adoption practices.
In order to conduct this research study, the Institute developed and carried out quantitative surveys, and follow-up focus group discussions and interviews, targeting a wide group of those with experience of past practices relating to closed adoption in Australia, including: mothers and fathers separated from a child by adoption, adopted individuals, adoptive parents, wider family members (to look at "ripple effects"), and those servicing current needs (counsellors, psychologists and other professionals). The survey questions and the topics used to guide focus group discussions built on existing research and evidence about the extent and impact of past adoption experiences.
For such a study, the recruitment of relevant sections of Australian society that are not readily identifiable, due to the sensitive and private nature of the issues, was in itself a substantial task. Yet, we were able to reach over 1,500 individuals - a significant result in itself.
The willingness of people to share their stories and accounts is evident in the fact that over two-thirds of the survey participants wanted to tell us more by taking part in the follow-up component of the study. While our focus was on current needs, service usage and possible service response improvements, participants wanted to tell us what adoption has meant for them - including both positive and negative perspectives - in order to paint the whole picture. Many talked about how their participation in this study was an opportunity for their voices to be heard and their journeys to be shared with the broader Australian community. Taking part in a study that is one-of-a-kind at this point in Australia's history has been described by some as a lifelong dream, as they never thought they would get their chance to tell what it has been like for them. In a sense, this means that one of the most important service responses is to create opportunities for those affected by past adoption practices to be heard - to tell their story and have their experience validated. This would seem to be in line with the needs and expectations of other groups who have been affected collectively by past practices (such as care leavers, former child migrants, and the Stolen Generations).
Project staff could not have anticipated the journey that they also have taken through conducting this research. People's willingness to share some of the most intimate parts of their lives, and their thoughts, feelings, hopes and aspirations for the future, has been a humbling experience. As researchers, the privileged position we have held, with people placing their trust in us to tell of their experiences to the broader community, has been nothing less than overwhelming.
The participants in this study asserted their positions clearly in relation to how the effects of past adoption practices have played out in their lives; how they are currently trying to deal with these issues, and what their current needs. What we have discovered is that although every person's experience is, of course, unique, there are some fundamental and core issues that are shared - issues that don't discriminate according to respondent group.
11.1 Why participate?
Persons who were adopted
A common theme underlying adoptee's stated motivations for taking part in the study was that they simply wanted to tell their stories and dispel some of the myths surrounding what it means to be adopted. For many of the adoptees who participated in the focus group discussions, it was also one of the first opportunities for them to actually come together with other adopted individuals, while others participated in the hope that the provision of information about their own experiences would be of benefit for future policy and practices in relation to the current adoption and donor conception environment in Australia. Some talked explicitly about their participation in the research project being a way of passing on the message that they wanted governments to be doing more for adoptees in relation to issues such as inaccessibility of information and the poor availability of appropriate support services. Some also hoped for a change in media portrayals or other public perceptions of adoptees.
The key areas of service provision need identified by adoptees were:
- access to their own information, such as original birth certificates (preferably through a national, centralised system) and medical histories of their family of origin, regardless of contact/information vetos;
- opportunities to tell their story to increase public and service professional awareness of their particular experiences and subsequent needs;
- connecting with other adoptees as a means of validating and normalising of experience;
- access to Find and Connect-style services staffed by trained and experienced professionals;
- supportive counselling to assist with responses to making contact, trying to establish a relationship with families of origin, and navigating the complexities of such newly established relationships;
- ongoing counselling provided by trained professionals that targets the specific needs of adoptees, including issues associated with identity, attachment and abandonment; and
- further consultation with adoptees as a group by governments in relation to current adoption policies and practices in Australia (including intercountry adoptions) and anonymous donor conceptions.
Mothers
Similarly to adopted individuals, many of the mothers who participated in the study were interested in having their stories told. They wanted the broader community to know what it was like for them to be young, unmarried and pregnant through a period of time in Australia's history when the stigma of such a situation was so powerful that they had few viable options for keeping their children.
Many of the mothers described how their participation in the survey and/or focus groups was a validating experience. The issue of wanting to change public perceptions about mothers who have been separated from a child through adoption was a consistent theme. It relates to the overall message of wanting to tell their stories and wanting to be heard. They also wanted the lessons learned from past practices to inform future policy development.
The depth of feeling around the importance of improved services was articulated well by one mother:
The first question I have is, why now? I mean, look at the age of the women sitting in this room. No one has ever asked me what services I might need. And I have been involved in support groups for 30 years almost. And that's the first question, and it has been asked. And if it's going to be taken on, then that's terrific. (Mother, Qld)
The key areas of service provision need identified by mothers were:
- access to appropriate and targeted mental and (to a lesser degree) physical health services to deal with the consequences of trauma and other ongoing effects of their adoption experiences;
- opportunities to tell their story and connect with others affected by past adoptions;
- access to Find and Connect-style services;
- access to targeted and specialised counselling to assist with responses to making contact or trying to establish a relationship with their son/daughter from whom they were separated by adoption; and
- access to their information from the time of their child's birth, including hospital/maternity home records, and original birth certificates.
Fathers
We only had limited participation in the study from fathers who were separated from their son/daughter by adoption. In some ways, this is understandable, as mothers may not have told the child's father that she was pregnant at the time; however, we also know from the mothers who responded that a significant proportion were in a relationship at the time of their pregnancy, which suggests that there is still a significant number of males in Australia who might reasonably know that they are a father of a child who was adopted (see Passmore & Coles, 2008). Despite the small number of fathers participating, the messages from them were powerful, and were given in the hope that their stories would broaden the awareness of other fathers in the community.
One father - who was extremely successful in making contact and subsequently developing a relationship with his daughter - was hopeful of being able to provide a "light" for others who may have not been as fortunate as him in their adoption journey:
A lot went into it, it didn't just arrive. There are some very deep scars to carry, and wounds, and fix them and come back. But the one thing that I would like to come out of it is, other people that have fear in their soul, could take our story and take the risk of going on their own journey … By hearing a story like ours that can maybe go out and touch people's hearts, it's doing two things: it's the social acceptance of it; and more subtly for the person who is afraid that they can identify with what is being said. If you're afraid of making contact, then maybe thinking about it in a way - that there is something that you can add to their lives that has real meaning and importance. And when you add it to their lives, you are adding it to your life as well. (Father, NSW)
The key areas of service provision need identified by fathers were:
- opportunities for their voices to be heard about their experiences, given the often overlooked/neglected recognition of their place in the adoption circle;
- opportunities to connect and engage with other fathers;
- establishment and promotion of support groups for fathers in order to encourage engagement;
- supportive counselling to assist with responses to making contact or trying to establish a relationship with their son/daughter from whom they were separated by adoption;
- Find and Connect-style services; and
- retrospective inclusion of their names on their child's original birth certificate.
Adoptive parents
The motivations for participation in this study were varied among the adoptive parents, and perhaps more divergent than within any other respondent group. Consistent with the other groups, adoptive parents wanted to have their experiences of past practices shared with the broader community to ensure a balanced viewpoint is presented. Some participants were concerned that given the current focus on forced adoptions as a result of the Senate Inquiry, that adoptive parents would be "tarnished with the same brush" as those professionals who were involved in the organisation of the adoption/forced removal of babies from their (birth) parents, or that all adoptions from this period of time would subsequently be viewed by the broader community as being "bad". Some of those adoptive parents reflected that such a focus could indeed be damaging to not only themselves, but their adoptive children, through the questioning of the legitimacy and/or legality of their adoptions.
Conversely, other adoptive parents who participated in the study expressed their concerns about the negative effects of adoption on their children (such as behavioural, identity and attachment issues), as well as how distressing they had found it to learn of some of the practices of the past and the treatment of (birth) mothers. They wanted to participate to show their support and sympathy for those mothers and fathers who had been adversely affected by the policies and practices of the time they were adopting their children.
There were few current service needs identified by the adoptive parents in this study. They did not consistently identify needs for themselves, but rather were focused on search and contact services for their sons/daughters, as well as assistance for them in finding out information, such as medical histories. They were more likely to focus on the time of their child(ren)'s adoption, in that very little support/guidance was provided to them about what to expect as new parents, nor the possible challenges their adopted children may face as a consequence of their adoption. However, some adoptive parents did identify that the option of speaking with other adoptive parents about their experiences, challenges, and successes would be of benefit - if not for themselves, then for those who have faced or are currently facing more difficult situations than their own.
Other family members
The ripple effects through family members are indeed evident from the information provided by these respondents, and indeed, from their level of participation (being the same total as that of adoptive parents who completed the survey). There was a diversity of relatives who completed the survey for those affected by the adoption experiences of a relative (including siblings and spouses of persons adopted, spouses of mothers, and subsequent children of mothers).
Participation in the study was largely viewed by other family members as an opportunity to share how past adoption practices have affected not only on themselves, but also their relatives (although many focused on the needs of their loved one and how they would be best placed to provide support).
Most other family members believed that there needs to be facilitated access to support (counselling and therapy) for themselves and their relatives regarding the issues arising from the adoption. Other needs included assistance with the contact/reconciliation with the "lost" relative, provision of the facts regarding the adoption and improved access to information about the family of origin (such as medical history), having access to peer support groups; raising community awareness and understanding, public acknowledgement, apologies and contrition for those adversely affected.
11.2 Effects of past adoption practices
Participants provided an immense amount of information through both the survey and the follow-up discussions regarding their experiences of the past, as they felt it was integral to the identification of what they are in need of now and into the future. As one participant said:
Without understanding the past, how can we hope to appropriately inform the right actions going forward? (Mother, WA)
In the previous chapters, we have shown that there is a number of common threads that run throughout the various respondent groups in terms of how their past adoption experiences have affected both themselves and, in many instances, those around them; such ripple effects have also highlighted a more general lack of understanding and awareness in the broader community as to what it means to be affected by an experience from the period of closed adoption in Australia, and how to respond accordingly.
In this discussion, we will firstly revisit these effects as they relate to the current service and support needs of study participants. For those who have shared their accounts of more positive and fulfilling experiences of adoption and what has "worked" for them in their journeys, these characteristics will be explored in more detail in the final section of this chapter, where we examine potential models of service and support as reflected in the information obtained in the study as a whole.
Mothers
As described by one mother who took part in this study, the effects of past adoptions for many are "intangible", as well as far-reaching and long-lasting. The common practices around adoption that were viewed by the broader society at the time as a means to provide a solution to both illegitimacy and infertility, were seen by many mothers who participated in the current study as systemic abuses and the betrayal of trust by those who had a duty to care and protect. Part of the service response expected by mothers with this view was the acknowledgement of this by relevant authorities, as well as assistance with finding out more about their history, such as hospital records (including any drugs that were administered) and details of the adoption consent process.
Many of the mothers described how the reasoning used at the time to justify adoption was focused directly around the perception that they were unable to care for their child because of their age, inexperience, lack of financial stability and lack of family support. In counterpoint to this, the responses from mothers to the survey showed that many had been working (such as nurses or teachers), had been financially stable, educated, and had not been teenagers (the majority of respondents were over 19 at the time of the birth). This suggests that the impetus for adoption was more strongly based on social stigma and the needs of infertile married couples (the "deserving"), as opposed to the actual capacity of the young women to parent effectively as a single mother or, with the father, as an unmarried couple. One of the issues that mothers discussed the most frequently was the ways in which institutions and individuals continued to reinforce messages such as their lack of worth or that they were not capable or deserving of raising their own child. Mothers also emphasised how these messages have manifested as beliefs about themselves to the present day. For many, this is 40 years of negative self-assessment that has been internalised.
The effects of adoption experiences on life events for many mothers have been significant, particularly in the areas of engaging in meaningful relationships and social functioning. For others, they have been able to excel in certain areas, particularly academically, despite the trauma so many endured (or indeed, because of it). This would suggest that psychological services are needed to address self-concept, and the ways in which these experiences that occurred at an early and formative stage in their adult development have affected the mothers' sense of self, relationships with others, and engagement with the outside world.
Wellbeing
Quality of life is defined as "individuals' perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns" (World Health Organization, 1997, p. 1). In the survey, the WHOQOL-BREF was used as a measure of an individual's quality of life over four broad domains: physical health, psychological, social relationships and environment (access to resources). Mothers recorded lower than average scores in the psychological, social relationships and physical wellbeing domains.
Respondents were also asked about how satisfied they were overall with their life on a scale of 1 to 10. The average score for mothers was 6.4, which is lower compared with general population data as reported in the HILDA survey, where the mean rescaled value for persons aged 35 years and over was 7.2.29
Both the survey open response items and focus group discussions were consistent in their messages in relation to current service needs, whereby many mothers said they are in urgent need of support to address these wellbeing needs. When asked what would be of most help to them now in dealing with their issues associated with past adoptions, psychological assistance was identified as the second most common response (having their experiences validated and acknowledged was the first).
The K10 mental health measure used in the survey indicated mid- to high-levels of current distress or likelihood of having a mental health disorder among the mothers who participated in our study. While being mindful that the K10 is an indicator of likelihood of having a mental disorder and applies to the previous four weeks of an individual's life at the time of completion, almost half of mothers participating in our study may currently have a moderate or severe mental health issue.30 This presents some significant challenges in terms of the service delivery needs of this group - in terms of addressing their mental health issues and providing other information and supports in a way that is sensitive to the variety of mental health challenges that service users might have.
Mothers' age at the time of birth appears to have had some effect on how likely survey respondents were to be currently suffering psychological distress. Well over half of the women who gave birth before they were 18 years old were likely to have had either a moderate or severe mental health issue at the time of survey completion (rates were even higher for those who had been aged 15 years or younger at the birth), compared with around one-third of mothers who gave birth when they were 20 years and older.
Mothers' perspectives of the adoption process were also associated with current levels of psychological distress. About two-thirds of women who said that they had either placed or gave up their child for adoption were likely to be well, compared with one in five mothers who said that their child had been taken or stolen from them. In addition, mothers who had had some support at the time of the pregnancy and birth were doing slightly better than those who had not had any supports at the time.
Trauma
The detailed accounts of extremely distressing treatment suffered by so many of the mothers who took part in this study are consistent with the findings of the Senate Inquiry, and hence it is appropriate in this discussion to highlight the more intensive levels of intervention that are needed by some who reported that they are still living with paralysing trauma-related symptoms in their day-to-day lives.
Mothers scored very high on the Impact of Events Scale, which is an indicator of post-traumatic stress disorder. Well over half were likely to meet the diagnostic criteria for PTSD based on their responses at the time of completion of the survey.
Qualitative accounts of experiences of pregnancy, birth, the process of obtaining consent and the ultimate adoption of their child were for the most part negative and have had broader implications for the mothers' wellbeing over time regarding:
- the decision and/or capacity to have more children;
- the capacity to form and maintain stable relationships; and
- the capacity to engage fully in social contexts.
The ability to make fully informed decisions regarding the adoption of their child and the emotional, physical and psychological effects directly relating to informed consent triggered the need for many mothers in this study to seek information from their records to confirm their experiences.
Some participants identified the administration of drugs during and immediately after the birth as a continuing issue for their capacity to come to terms with their experience, as it directly relates to whether there could have been informed consent. Whether or not some of these drugs were standard administration for all mothers in the hospitals, is not the point of focus. As one mother articulated:
It may have been true that similar drugs were also given to married mothers, but they weren't then asked to sign a legal document. (Mother, Victoria)
There was strong endorsement of the need for counselling/psychological intervention and support, and the low levels of mothers' wellbeing found in this study support these accounts, and is also consistent with the findings of the Senate Inquiry, as presented in Recommendation 8 of their final report.
Fathers
The limited participation in the study by fathers makes it difficult to draw conclusions that could be considered representative of this population. There is therefore a need for further investigation into this group, with targeted and coordinated recruitment strategies.
The fathers who did participate in this study expressed concern about the lack of support options available to them, as well as concern for the fathers who would have never engaged in a discussion about their experiences. In addition, they spoke about how the lack of choice and control in the decisions that were made at the time of their child's adoption is being perpetuated today, as they felt that they have little voice in the broader public discussion around past adoptions. These results show consistency with the findings of previous small-scale research that has focused directly on fathers, such as that conducted by Clapton (2007) and Passmore and Coles (2008).
The fathers' experiences reflect what many of the mothers who also participated in the study told us: they had wanted to have a say in what happened with regard to the adoption, and many had wanted to keep the baby. Very few of them had had support at the time of the pregnancy and birth, and very few have had support since.
Their current needs centre on an increased awareness and understanding of what happened and why, and a broader understanding from the community as to what the adoption climate of the day was and how this affected their capacity to be involved in the decision-making process about their child's future. Fathers also saw it as important to acknowledge the trauma that occurred from the separation of family.
Persons who were adopted
I guess we want our story to be told, because it's all so "Shhhh, we don't talk about adoption". We are not possessions. (Adoptee, Qld)
Many adopted individuals who took part in this study stated that they have rarely felt that their experiences have been validated or viewed as being of any real consequence, and that the effects of their adoption on their lives (both positive and negative) have, for the most part, not been included in the nation's broader discourse to this point in time.
Some participants described feeling as though they are the forgotten part of the equation. Nevertheless, they felt that they are the living result of how past practices have played out, and therefore want to have the accounts of their experiences, both positive and negative, shared with the broader community.
The feelings of silence and secrecy and the stigma attached to adoption led to many of these study participants feeling like they have been unable to talk about their experiences, because no one ever recognised or acknowledged their loss of their family of origin and sense of identification with their biological kin. Although many have gained richly from their upbringing within their adoptive family, there was still a view held that they have not been provided with the opportunity to have a voice.
Mental health and wellbeing
As with mothers, adopted individuals who responded to the survey had lower ratings than average on three of the four domains for the WHOQOL-BREF measure, and close to 30% were, at the time of the survey, suffering moderate or severe levels of psychological distress (compared with around 10% of the general population). Their overall satisfaction with life was also lower than average population results.
There was some evidence that the adopted individuals in the survey who had had more support when growing up were faring slightly better now.
Qualitative accounts suggest that adopted individuals are facing multiple issues, and having had a positive experience growing up with their adoptive families has not necessarily meant that they have not faced any issues in relation to their adoption. In fact, there was an overwhelming amount of information provided to us as to how their adoption experience has affected many areas of their lives, such as self-identity, family and other intimate relationships, parenting behaviours (including confidence, and questioning their own adequacy as a parent), and issues with abandonment and attachment (or "bonding"). Having their own children has also been a trigger for many participants as to what adoption has meant for them and how it has affected their lives.
Continued secrecy and shame
Negative feelings by some study participants about their adoption experience have been compounded by feeling ostracised from a community who perceived adoption as being something to be ashamed of - that there was and to some degree still is a stigma attached to adoption. These messages have come in myriad forms, such as people's general reactions to hearing that someone is adopted (for example, a "pitying" attitude or displaying an intense curiosity), or the more overt discrepancies in rights to information about oneself that the rest of the community take for granted. An overarching theme was that for many, there is a lack of normalisation, as an adopted individual should be able to speak of their experiences without the need to worry about managing others' reactions.
Some participants also spoke about the effects of secrecy, stigma and shame on their adoptive parents as well as families of origin, and how this has filtered through to ultimately become their own burden to bear. For some, they carry the weight of their mothers having never disclosed that she ever gave birth to them; similarly, many felt the weight of adoptive parents' expectations, who have treated the adoption of their children as something to remain discreet about or entirely hidden.
For many late-discovery adoptees who participated in this study, it has been a matter of "rebuilding a life that has felt like a lie". The effects of non-disclosure of their adoption by their adoptive families have been profound.
Information
For the most part, persons who were adopted who participated in the study considered information about themselves as being of extreme importance, as it is related to issues of identity that everyone else takes for granted. As is evident from the amount of information provided by study participants, the issues of seeking information about oneself and one's family of origin and the subsequent process of search and contact are significant contributors to both past and current experiences of adoption and its associated effects.
Many study participants also reflected that the current system does not provide for ease of access to information; it fails to reflect the significance of the information that is being provided to those who are seeking it. A number of respondents noted a lack of sensitivity to the effect that receiving this information may have coming from those who are in the position of providing it to them.
The main issue for adopted persons in this study in relation to gaining access to their own information is that it should not be viewed as a privilege, but rather as a right. This includes information about the details of their birth and subsequent adoption, as well as their genetic and medical histories. Being able to have access to information that the rest of the community takes for granted (such as original birth certificates) was a central issue for many adoptees. They talked about the absence of choice that they had in their adoption and so were questioning why they have to bear the burden of fighting for information that belongs to them, such as an original birth certificate. A critical element of the service response to adoptees is assistance with obtaining information to support their search for their real legal identity, genealogy (including their father's name), and medical history.
Late-discovery adoptees have faced an added complexity of accessing information, given that for many, both sets of parents have passed away. Many of the mothers kept the birth a secret for their entire life. Similarly, for those whose adoptions were privately arranged, they have had little to no availability of information regarding their family histories.
For some participants, they have suffered extreme distress by discovering the inaccuracies contained in some of their "original" documentation. Many described how they had been lied to about the circumstances of their adoption, or given incorrect information about their birth family:
For me, I don't even believe the information anymore. I look at it and think, "Is this real, or just forged like the rest of it?" (Adoptee, NSW)
A concerning number of participants disclosed abuse they had suffered by their adoptive parents, and felt it was important that the message be communicated more broadly that not all adoptees went to good homes. Their responses demonstrate the variety of ways in which they are still dealing with the lifelong effects of these abuses. Carrying the physical and psychological scars and their need for medical and psychological support has come at great cost, financially and emotionally.
For some, it is a question now of how those responsible for their placements could have let this happen to them. Many adoptees in this position who participated in the study would like to know who was in fact responsible, and are asking for those involved to be held accountable.
Adoptive parents
The effects of past adoptions on the adoptive parents who participated in the study were varied. For many, they focused more on the effects on their children, particularly in their child's search for medical information of their birth families.
Adoptive parents did mention the lack of support that existed at the time of adoption. For many, they hadn't been provided with the information to adequately equip or prepare them for some of the issues they might face. There was limited discussion among participants regarding how the effects of infertility had affected them both physically and emotionally; they had had little or no support through this experience at the time.
Some respondents were concerned that there was too much negative publicity about adoption that was detrimental to their mental health and the mental health of their sons/daughters and grandchildren. Addressing this imbalance was a need identified by some of the adoptive parents.
The efforts that their sons/daughters have made to search for and make contact with birth families has raised a number of complex issues. Some adoptive parents were encouraging and supportive of their son or daughter's search for their family of origin; however, others felt threatened or hurt when the adopted person decided to search. A portion of the comments from the survey reflect an underlying suggestion of an "us or them" mentality - and this is supported by what was found from the surveyed adoptees and mothers.
A small number of study participants spoke about the distress they had felt when their adopted child had died and they did not have any information about the birth mother in order to contact her to inform her of her child's death. This was an issue that they would like to see resolved in current adoption policy.
The main areas of current support needs identified by adoptive parents were:
- access to medical information for their son or daughter;
- support for them and their son or daughter during the search and contact process, and beyond; and
- assisting with emotional responses from adoptive parents, children and other family members to publicity around past adoption issues that has the capacity to hurt or sensitise them, when they felt they were doing the best thing.
Other family members
The importance of hearing from other family members in this study is significant, as it provides us with a broader understanding of the complexities associated with the varying effects of past adoptions in Australia. We had a wide representation of relatives within this group of participants, including spouses, siblings, children and grandparents of those within the core respondent groups.
Interestingly, of the other family members who participated in this study, the majority had engaged in some form of support or accessed services to help them with issues associated with the adoption experience of their relative. Around one-quarter had utilised professional counsellors such as a psychologist, psychiatrist or social worker.
As with the core groups in the study, other family members who are directly affected by adoption (e.g., those who find that their mother had lost a child to adoption and now wish to search for their lost sibling) commented on the effects of not knowing the truth, and having access to the details surrounding the adoption was of significance. Secrecy and lies have a lasting impact, and were the most serious issue, according to many of the family members who participated in our study. For others (such as spouses) providing support to their relative who has been directly affected by adoption, the most significant issue was not knowing how best to support their loved one and that this has affected the quality of their relationships.
Other family members in this study said that support for their loved one, assistance in the search/contact process and having access to information about their relative were all areas in which they thought further support was required.
11.3 Service use
Use of services varied between respondent groups, as did their levels of satisfaction. Search and contact services (both government and non-government), post-adoption services and individual professionals such as psychologists, psychiatrists and counsellors were all examples of where study participants had engaged in some level of support.
Adopted individuals have commonly utilised search and contact services, as well as sought further support from peer groups or one-to-one psychological intervention, to assist in dealing with the broader effects of their adoption (such as identity and attachment, their own parenting, and capacity to engage in trusting and fulfilling relationships).
Mothers had also utilised search and contact services, as well as peer support groups and individual counselling with professionals for assistance with trauma-related issues, grief and loss support.
Although adoptive parents were most likely to have received support from an informal source such as their spouses, friends and church community, a number identified that they would like to have more effective mechanisms for their child(ren) to access information about themselves, particularly medical/genetic information.
Fathers had typically utilised a limited amount of support in the form of formal services. Some had relied on support groups (although very small numbers said they had done this), and others were more likely to have simply used formal search and contact services.
Other family members had a relatively high rate of service utilisation, most commonly in the form of formalised counselling or accessing search and contact services. However, most had relied on the support of family and friends in helping them deal with any issues relating to their adoption experience.
Although most who had utilised more formalised supports found them to be helpful generally, there were some significant limitations identified with regard to the level of knowledge and understanding of adoption-specific issues by those service professionals. The focus group discussions in particular revealed a sense of frustration toward the continued need to "educate the educated", and this was often viewed as a significant barrier to accessing support/ information/referral that appropriately matched the specific needs of this group. This frustration is often compounded for adopted individuals, who have the added complexity of not having knowledge of their family's medical/genetic histories. A simple visit to the GP, which many people take for granted, was described by many study participants as something to be dreaded. For them, there is a never-ending need to inform medical professionals when asked about family medical histories that they don't know because they are adopted.
Information, search and contact services
Over half of the adopted individuals and almost 70% of the mothers had used search/contact services. The most common type of service utilised was a government department (including the Registrar of Births, Deaths and Marriages and the Electoral Commission), followed by non-government organisations (such as Jigsaw, in most instances) or the institution through which the adoption had been organised. Peer support groups and post-adoption resource centres were also used.
Mothers who had negative experiences with search and contact services were largely feeling the frustration of not being entitled to information about their son/daughter due to privacy restrictions such as contact and information vetos. Use of these services largely focused on accessing records from the time of the pregnancy and birth.
For adopted individuals, the search process was mostly undertaken through state government departments responsible for adoptions, who can assist with the provision of original birth certificates and other information (both identifying and non-identifying) when they turn 18, or when a member of their birth family wanted to make contact.
Adopted individuals mostly reported their experience of information and search services as being helpful in some way, even if it was just the provision of information that enabled them to conduct a search or find information themselves. However, there were numerous accounts of the lack of professionalism displayed by some staff with whom they had contact in the information/search process.
Barriers to service utilisation
There were numerous factors identified across respondent groups relating to their experiences of services that were seen as impeding their progress in either the search and contact process, or managing the effects of their adoption experience.
- Cost was a significant concern for many. The ongoing requirement to pay for information (such as from the Registrar of Births, Deaths and Marriages, where you pay for every 10 years of search information) and copies of original documentation was viewed as an unnecessary, and indeed, unfair burden for those affected by past adoption practices:
It should be free. We pay money in our taxes. Why should we continue to pay for something that is ours? (Adoptee, NSW)
They all want to charge me a fortune to go back and see if they can find [the birth certificate]. I'm just not going to pay it. I'm sick of paying. (Adoptee, NSW)
In addition, many participants concluded that the costs of psychological interventions were an impediment to their ongoing capacity to engage with this much-needed form of support. Some spoke of having made significant sacrifices in many areas of their lives (such as permanent housing) in order to fund their ongoing treatment with mental and other health professionals.
This is a significant finding in light of the results of the health and wellbeing measures used in this study. As we have learned, adoption-related issues are often lifelong, and for many, there will be a long-term need for support. The service providers who participated in the study supported this. It is also a key consideration in the development of appropriate service and support models.
- Navigation of the search and contact "system" was an area consistently identified by study participants as impeding their ongoing capacity (and often their willingness) to find information about either themselves (such as medical and adoption records) or their family member. Inconsistencies in processes across states and territories was frequently raised in focus group discussions for both adopted individuals and mothers as an issue that placed significant stress and pressure on themselves and other family members, both emotionally and financially:
Government post-adoption services can be frustrating at times, as they have to carefully administer policies for a wide range of stakeholders. (57, 2012)
I do have negative attitudes towards the Registry of Births, Deaths and Marriages, whilst concomitantly recognising that they are bound by laws etc. in place at the time. I think [state's] registry laws are designed to be as difficult and insensitive as possible - a classic bureaucratic system. (206, 2012)
Participants across all respondent groups were largely in support of developing a nationally centralised database as one way of addressing this issue, and believed that this is a priority area that could readily address the needs of many affected by past adoptions.
- Staff attitudes, experience and professionalism were recognised as being of significance in study participants' reflections on the quality of service provision and subsequent effects on their willingness and confidence to engage further in such services. These more negative experiences were not limited to search and contact services, but more particularly to those in the position of information provision, such as the Registrars of Births, Deaths and Marriages. Respondents provided a number of examples of their experiences of search and contact services that raised some concerning issues relating to the basic handling of cases. Similarly, they talked about a number of examples of departmental services that reflected insensitivity, or other poor practices (see section 7.10).
These accounts demonstrate the potentially devastating effects of poorly devised, implemented and regulated processes within agencies/departments responsible for the provision of information, search and contact services. Training of such professionals was consistently identified as being imperative in order to ensure the wellbeing and protection of individuals seeking information and support.
- Lack of support/guidance throughout the search and contact process and after was a key issue identified as being a major barrier to either the success of making contact and/or the ongoing wellbeing of those involved, including the wider circle of family members. Adoptees wanted information about the likelihood of reunions succeeding. They wanted support in the follow-up period - both in terms of how to maximise the likelihood of the reunion being positive, and how to negotiate the new relationship - as well as how to manage the pain of rejection if it did not go well.
Professional support
Many participants in this study expressed frustration with their experience of GPs, counsellors and other professionals who were either not aware of or dismissed the effect that separation through adoption had had on their lives. Survey data show that those who had accessed formal forms of support from professionals found them to be largely ineffective.
For many in this study, they spoke of frustrations associated with the ongoing financial cost of trying to get support that meets their needs adequately.
Also, the experiences of those accessing professional supports have been varied in terms of quality, which was generally not consistent or reliable. However, those who had good support found it life-saving. Those professionals understood adoption-specific issues and the trauma lens through which a lot of their issues need to be viewed.
The inadequacy of the Medicare mental health scheme for accessing quality psychological services was raised. The limited number of sessions was seen as problematic, particularly for those with serious mental health issues, such as personality disorders.
Peer groups
Peer support groups have been used effectively in the mental health and alcohol and other drug sectors for a long time. However, there are pros and cons with this using method of "intervention" with people who have been affected by adoption.
Many respondents from across the different participant groups saw the value of peer support. It can be a safe space where there are others with shared experiences. However, some of the issues people have had were if there were competing interests or needs within the group (particularly if both birth parents and adoptees were in the same group),31 the lack of regulation, quality of facilitation, and the distance of the venues.
However, even though one adoptee found that "the dysfunction was being repeated in the group" and found the group experience overwhelming, they still acknowledged that some people found the group very valuable, and thought it was an important option to retain in a service delivery model.
11.4 Current service and support needs
Drawing together the depth of experience across respondent groups, we are now able to summarise the key consistent viewpoints of study participants as to what they view as being of most benefit to them in helping them deal with their past adoption experiences now and into the future.
If we examine the effects of past adoptions on participants in this study through the lens of a public health perspective, then the social and economic costs and consequences of preventable health issues are borne not only by individuals, but also by the entire community. Studies have consistently shown that population-level prevention and early intervention is cost-effective and can positively alter risk and protective factors that affect individuals. For the purposes of this discussion, this will be the lens through which the approaches that were identified by study participants will be viewed. (For more information about a public health approach to child welfare issues, see Hunter, 2011.)
We will firstly examine the key actions identified by study participants that would be of most benefit to them now, in their own words, and then move to a broader discussion based on the analysis of study data and draw conclusions for service and support interventions accordingly.
Acknowledgement and recognition of past practices
Knowing where their thinking came from does not condone their treatment of us. (Mother, NSW).
Although not directly a "service or support need", one of the most important things that participants said would be of benefit to them now and into the future was acknowledgement of the common adoption practices of the past and the subsequent effects that have been experienced by those who participated in this study. This includes acknowledgment and recognition that what happened happened, and that the information that has been gathered in relation to the effects of past practices acts as a point of reference to ensure that mistakes are not repeated.
For some participants, the recognition that one of the consequences of the closed adoption system that had operated in Australia, was the denial of the right for all those most closely affected to grieve - the mothers and fathers who were not allowed to grieve the loss of their child; adopted individuals not allowed to grieve the loss of identity and the separation from their birth family; and the adoptive parents not allowed to grieve their infertility.
Adopted individuals were very strong in their focus on the need for public acknowledgement - both for themselves and the mothers:
Acknowledgement of the wrongs done to the victims of the adoption boom era. Acknowledgement of adult adoptees' right to feel anger for what was done to them in the name of bad public policy. (Adoptee, 704, 2012)
I think the most important thing is that there is acknowledgement of the societal pressure placed on single mothers in the 1970s to give up their children. I am quite accepting of my role of an adopted child, but know that my natural mother is scarred by the decisions that she made and it had significant impact later on her life choices. (Adoptee, 676, 2012)
One adoptee spoke about the effect that learning about the Senate Inquiry had on her, and how being exposed to this information instigated a shift in her understanding of the circumstances of so many mothers.
I think that the Inquiry is essential. I had no idea that this could have happened to me and my (birth) mother. All my life I have thought that she hasn't wanted to make contact with me, and now I find out that she may have been told I was dead? I feel sick about the way she may have been treated. It's appalling that thousands of Australians are in this position and the government needs to reveal the truth. Being adopted never goes away you know. (Adoptee, 441, 2012)
The role of apologies: By whom and for what purpose?
Although this study found some divergent views from participants on the merits of apologies relating to past adoption practices, and many saw a national apology from the government as being of more significance to mothers than adopted individuals in this study, there was generally overall support for this happening.
It is important to note that the question of whether an apology is needed was not asked specifically in the survey; rather, many participants spontaneously identified it as the most important thing that could happen now to help them deal with their experience of adoption. It was then an avenue for discussion in the focus groups when some participants raised it, or drew comparisons between themselves and the Stolen Generations and Forgotten Australians.
In terms of addressing current needs, the themes that emerged from this study suggest that apologies can play a role by:
- starting a conversation and ending the silence;
- allowing affected persons to have a voice they have not felt they have been able to have previously;
- broadening the general population's understanding and awareness of the potential issues people with an adoption story may have; and
- improving the quality of service provision available to appropriately address adoption-related issues within the broader health and welfare sectors.
Even if individuals did not feel they personally needed, or would benefit from an apology, some still argued that it would bring about a public awareness to the issues. Some study participants spoke about their need for institutions (such as hospitals and maternity homes) to make full disclosure of the common practices to which mothers were subjected:
I would like to see honest and full disclosure of practices in hospitals and maternity homes. In particular, the withholding of information and provision of false information and the forced management of residents' financial benefits … disclosure of all illegal practices by organisations and individuals, and an acknowledgement that closed adoption was a practice of social engineering, and not carried out in the interests of either the mother or children who were separated. (Mother, 146, 2012)
The Senate Inquiry's (2012) final report spoke about an apology to mothers, fathers, adopted individuals and other family members; however, many participants from all respondent groups articulated that an apology is only appropriate if all those within the adoption circle are addressed:
- mothers and fathers - for their rights and entitlements being withheld and for the violations of care they experienced:
An acknowledgement by the perpetrators of the illegality and the personal wrong done to myself and other individuals due to the practice of taking babies from young unmarried and unsupported mothers who wanted their baby, in order to give them to other women keen to adopt a child, along with an apology at the very least. If there had not been a "market" for these babies, then the horror might not have been so forced on young and vulnerable women who had not done any wrong other than offend some social values of the time. (381, 2012)
To say sorry to the generations of women who felt they had no power over what happened to either their bodies or their future. (Adoptee, 621 2012)
- adopted individuals - for the lack of duty of care by governments, agencies, or others in authority to ensure that their best interests were central to the decisions related to their eventual adoption; that their rights to information regarding their identities have been withheld; and that the effects of closed adoption practices and policies have in many cases perpetuated a culture of secrecy and shame:
Recognition of the injustices suffered by myself and my three adoptive siblings, including one who suicided, which should include exposure of the system which allowed it to happen. (265, 2012)
I want the government to apologise - I want my adoptive mother to know I was taken by force, not given over legally. (Adoptee, Qld)
Truth, recognition and apology from our government. Adoptees that were given to families and subsequently abused are seeking better services for pain, suffering, grief and trauma. We are seeking an apology not only for being taken from our mothers and family, but for the lack of screening of potential adoptive parents that should have protected us from perceived harm. (50, 2012)
- adoptive parents - that they were not always advised of the rights of the mothers and fathers and that they were not given the appropriate support to grieve their infertility.
Opposition to apologies
Those who were opposed to or had some reservations about an apology had a number of different viewpoints. These participants tended to focus on other actions that they saw as being more important:
It's just a word. Unless they actually have an action behind the word, then it's not going to mean anything. (Adoptee, NSW)
In some ways I think it would be good, you know, to kind of have some recognition. But I don't want everything to be hung on that. (Adoptee, Victoria)
I don't think I need an apology or anything, but for me it's a personal thing. I don't think that would assist me. I feel personally that it would take away from what I have done for myself. (Adoptee, Qld)
The apology might make some people feel better, but others … Just make sure it doesn't happen again. (NSW adoptee)
For apologies to be meaningful, the Senate Inquiry (2012) identified a number of guidelines that should be followed. Their guidelines are consistent with the key messages emerging from the current study.
Financial compensation
For adopted individuals, the right to financial compensation was mainly raised by those who suffered abuse at the hands of their adoptive families; in addition, there were small numbers of participants who wanted to be compensated for their loss of inheritance rights (from both birth family and adoptive family), as well as medical costs for issues relating to the trauma they have suffered.
Mothers who identified financial compensation as something they were seeking were generally identifying it as recognition of the trauma/abuses that were suffered in some of the hospitals and maternity homes, and compensation for the physical and psychological impacts that have been lifelong and debilitating, and the costs of medical and psychological services that have been incurred.
The broader view held by respondents, however, was that, rather than compensation, access to support services such as professional counselling, funding for ongoing psychological care and access to information should be freely available or heavily subsidised for all those affected. A suggestion was also made about the possibility of having travel allowances to enable contact between themselves and their loved ones. Another innovative suggestion for a service provision model to address past adoption effects was to offer free private medical cover for life for all those with a substantial complaint. As one respondent pithily put it:
I don't give a shit about money and compensation; I just want to be heard. I want some changes so you feel like you've been heard - someone acknowledging the fact that what was done was wrong. They can make it up to us by giving us the services and information we need. They're simple things - it's not like we're asking for a lot. (Adoptee, NSW)
Education and awareness
Education of the wider community about the effects of past adoption practices was seen by many study participants as being integral to their own capacity to begin the journey of healing. While fostering community education and awareness is not explicitly part of what would normally be considered a "service delivery model", for participants this was a strong theme for them in what would help them. Some of the key messages that participants wanted communicated included:
- adoption changes lives forever and that it's not about being grateful or lucky;
- there are untold stories of grief and loss in the adoption community (across all members, including adoptive parents);
- it wasn't a case of mothers not wanting their babies and being happy to give them up ("I was not a 'bad girl' and that giving up my son was not my 'choice'.");
- it hurts people to deny the effects of adoption;
- the issues are difficult and complex for all parties; and
- the effects of past adoption policies in Australia are widespread, with wide-ranging repercussions.
Increased public awareness was viewed by many participants as being a way of enabling the issues associated with adoption to be heard and discussed more openly, which would then allow affected individuals to feel what they feel without guilt, shame or stigma. These types of sentiments were shared across respondent groups. Broader education and awareness would remove some of the stigma attached to adoption and provide a balanced viewpoint of adoption experiences.
As was seen in respondents' articulation of their reasons for participating in the study, for many - across the different respondent groups - it was about feeling relief that they were not alone, especially for those who had never sought support, and it was about providing information to other parties in the adoption circle so that others can be made aware of experiences from different perspectives.
The sharing of personal stories in the public arena was viewed by many as being a powerful tool for validating people's adoption experiences: it allows people to see, beyond the stigma attached to adoption, how it actually affects people. An education and awareness campaign can therefore play a strong role in opening up the conversation within the community that adoption needs to be destigmatised and not considered a taboo subject. An aware community was seen by many of those affected as being integral to feeling they can come forward and receive better, informed services and practices by service providers.
One of the positive expectations that respondents had of public awareness campaigns - in addition to educating the professional and broader community - was also to "normalise" the experiences for people affected:
I think it would be useful for people to normalise it a bit more. It is quite enlightening when you do read about other people's experiences and you go, ah, I'm not the only one that has felt that or experienced that. I think that's what's missing - that commonality and common experiences - and for people to realise it is quite normal to be paranoid about being rejected in interpersonal relationships, or not being able to relate to your children as well as you would like to. Those sorts of things are quite common. We all think that we are the ones that are broken. (Adoptee, Tasmania)
There is a lot of stuff out there now about how families are made up of endless, different combinations - same-sex couples, step-families - adoption fits very neatly into that because people affected by adoption are just another type of family. So bring it into the normal range and just make it as another one of those mini combinations that families are. Take the stigma out of it, take the secrecy out of it, take the blame and shame. (Adoptee, Qld)
Workforce training and development
Adoption is obviously a smaller proportion of the population, but it is still something that professionals should have some recognition of and know what some of the potential issues are. (Adoptee, Tasmania)
Before we look in more detail at the types of support services that participants have identified as being most needed, the issue of workforce capacity, and the development that is required to deliver such services appropriately and adequately, requires further reflection.
Participants provided their accounts of both positive and negative experiences of services, government departments, other organisations and individual professionals in their adoption stories. One of the most pertinent issues raised was the risk of re-traumatising individuals who are presenting for support, given some participants' experience of professionals as being dismissive, misinformed, or completely inadequate. As one mother articulated:
The understanding and empathy of the wider community … would especially include those working in the psychological professions, who too often see adoption as just a tick-a-box and so do not recognise the possible long-term impact of separation loss for both mother and child. (71, 2012)
GPs can play an integral part in an individual's search for appropriate supports and interventions, usually by way of referral. Their role is vital, as they often act as "gatekeepers" to information and sources of support. Some participants spoke about the importance of GPs having a thorough understanding of adoption-related issues, as there is the potential for misdiagnosis of mental health issues in particular, given the similar symptomology of conditions such as borderline personality disorder and the commonly seen attachment and identity issues for adopted individuals.
Given the accounts of the broad effects of adoption on physical, emotional and psychological wellbeing, it makes sense to target for workforce training and development those working in the fields that those affected would be utilising to help deal with such issues (such as GPs, psychologists, psychiatrists, mental health workers, alcohol and other drug clinicians, etc.):
Just one question saying, "Have you or anyone in your family been affected by adoption?" That's really all you need to know in the initial assessment where you can explore further down the track. (Adoptee, Tasmania)
It is important that the experience of asking for information be normalised; for example, by incorporating it into standardised screening and assessment tools, or by simply starting the conversation, by asking a question such as, "Do you have an adoption experience?" And if there is an affirmative answer, to follow up with, "Do you believe that your adoption experience in any way relates to your presentation at this service today?"
11.5 The service system
Information
For many adopted individuals in this study, access to personal information that the broader community takes for granted, such as birth certificates, was viewed as being an important issue. Yet according to our respondents, access to this information and documentation was often frustratingly difficult and expensive. They didn't want to have to beg for what they feel is rightfully theirs. Not being provided with information about their background has had a direct effect on adopted individuals' sense of identity and place within society:
The law says, because I am adopted by her, I am not her daughter, but the birth certificate says that I am. So who am I? (Adoptee, WA)
Similarly, for the mothers who were subjected to the forced adoption of their son/daughter, the desire for obtaining their records, from the time of their pregnancies through to when their child was placed with their adoptive families, appears to be integral to their ongoing healing and recovery from their experiences.
Access to the medical histories of the adopted individuals' birth family was one of the most frequently stated issues by study participants (including from the perspective of adoptive parents), who felt that such access should be available regardless of contact status. For those who have attempted to find information about the medical histories of their family of origin and either been unable to connect or had obstructions to finding such information (such as contact/information vetos or non-disclosure of identifying information about fathers), this may literally be a case of life or death. We heard from adoptees and their other family members about cases where potentially life-threatening illnesses were unable to be appropriately detected or diagnosed because in some cases they weren't aware at the time that they were adopted, or more commonly, because they lacked personal and/or family information. The effects of not having this information are widespread, both for their own health issues and the capacity for accurate screening and diagnosis, and for subsequent generations' health issues.
A centralised information system or register is highly desired by those affected. The barriers presented when attempting to navigate an often complex and bureaucratic system across states and territories appears to have ramifications for individuals' ongoing efforts to piece together their identity personal histories.
Governments and non-government agencies responsible for the holding and distribution of adoption information require specialised training in how to sensitively and effectively manage the sharing of this information.
The abolition of processing fees for adopted individuals and mothers wishing to access their own records, particularly original birth certificates, was strongly advocated by study participants, particularly adopted individuals:
Why should we have to pay for something that everybody else can readily achieve or obtain? (Adoptee, Qld)
Some participants spoke about contact registers in that they would like to see that they are regularly updated, giving people the opportunity to revisit their decisions to be or not be contacted. This was seen as being of particular importance for those whose parents/children have contact vetos in place. Adopted individuals in particular voiced their frustration with how this affects their right to medical/genetic information. For many, it is simply about having the information available to them, and the need for actual contact as being something they can accept not having:
It's not about meeting her as such, it's about having the lineage. (Adoptee, SA).
Search and contact
Management of information searches
Study participants made it clear that the process of search, contact and navigating new relationships needs to be managed from the very first stage when information is being sought. Suggestions included having a referral to a support agency prior to and upon receipt of information from any government department or other agency that is holding records. Others suggested that information packages could be made available that contain information such as what to expect when searching; how this may affect self and other family/loved ones; and how to manage expectations around search outcomes.
Another option was the allocation of a case manager to all those engaging in the process of search and contact, who can assist in the often complex navigation of varied systems and who can act as a single point of contact for both the person searching and the external parties providing information. This role could also extend to the coordination of support to other family members - such as spouses, children and parents (including adoptive parents) - in order to remove/displace some of the pressures on the person at the centre of the search who may be going through an emotional and trying time. Given the discussions from all respondent groups regarding the effects of divided loyalties, having access to a person in such a role who can act as a mediator, would perhaps address many of these issues. As one participant said, there are psychological benefits to "outsourcing the search and thus removing myself from discovering possible rejection of my enquiry" (Adoptee, 189, 2012).
Characteristics of search and contact services that reflect best practice
Participants stated that one of the most helpful aspects of search and contact services was the attitude of service staff - their capacity to be understanding, sensitive, respectful, professional and knowledgeable on the issues. The broader view of study participants was that professionals do not necessarily have to have a personal adoption experience, but they do need to have training and be adequately equipped with the necessary specialised knowledge. Having said this, study participants were generally also in favour of all those providing such services being required to undergo some level of training to ensure an appropriate standard of practice. This was viewed as being one measure of accountability for those who do have a personal adoption experience who are in a position of providing support, so that their own issues are not transferred to those seeking assistance and that appropriate boundaries are established.
A number of key elements of good practice emerged from the data we collected in the current study. These elements of good practice include:
- requests for information from departmental/organisational staff are responded to in a timely way;
- information is delivered in a sensitive and respectful manner;
- advice and information is given about what to expect throughout the entire journey, not just about how to search;
- formalised complaints processes are made known and readily available to service users as a means of accountability to address some of the concerns raised by participants regarding poor levels of professionalism;
- staff are available - being a point of contact when/if needed and that there are flexible hours of operation to accommodate the varying needs of service users, including meeting the needs of those living in more remote locations, where access to a physical site may be impossible;
- service providers are well-informed and understand the issues associated with adoption for all members of the adoption circle;
- ongoing support and follow-up from the agency involved is provided in acknowledgement that for those affected, it's not just about getting the information and then being left to deal with the outcomes of contact; and
- support, education and information for the other family members is readily available.
Ongoing support options
It's always been for me, desperately trying to find someone you can talk to who has some kind of knowledge or experience or understanding. (Mother, Qld)
As articulated by many in this study, and supported by the findings of the Senate Inquiry (2012), apologies are of little value if they are not followed by actions. The view of study participants is that both government and institutions involved in past practices have an obligation to provide funding for the development of appropriate support systems and to enhance the capacity of existing services.
Key support options that were identified in this study include:
- adoption-specific support services (post-adoption support) offering a "one-stop shop" for accessing information, search, contact and ongoing support/referral to appropriate professionals, including support for the wider circle of family members and mediation services for new family relationships, as well as managing existing relationships;
- availability of professional one-to-one support/counselling/therapeutic interventions, delivered by psychiatrists, psychologists and other professionals who have had specialised training or experience in adoption-related issues such as trauma, relational interactions, attachment, abandonment;
- peer support groups that offer a variety of options, are monitored for quality and accountability, and can accommodate the diverse needs of those affected by past adoptions, such as "mixed" groups; "silo" groups; and those targeted at people at different "stages" of their adoption journey (e.g., contact versus no contact etc.); and
- primary and allied health services professionals having training and access to information regarding adoption-related issues.
Specialist counselling
At present, we rely upon service providers who have little or no knowledge of this country's appalling history of adoption and the way in which we were treated. We are unable to find or afford skilled, therapeutic therapists that have extensive knowledge and comprehension of adoption and abuse that causes deep psychological scarring and manifests into complex mental health disorders that are often left untreated or misdiagnosed … because it is believed that we all went to good homes. (Adoptee, Qld)
Specialised counselling was seen as being integral to meeting the current needs of those affected; that is, counselling by professionals who have specialised knowledge of the issues associated with adoption (including trauma and relational and attachment-focused therapy). Specialised counselling needs to remain available to those affected throughout the life span - adoption-related issues can be triggered at any time, and often the individual is left in a very vulnerable state when events trigger an emotional response:
I think that ongoing support through not just the immediate adoption and reunification, but the ongoing - as in the next generation parenting, inter-personal relations, educational outcomes - all those sorts of things. Employment, substance abuse, all those things that apparently we are over-represented for. Those supports need to be there and those professionals need to know, potentially what issues come out of adoption. (Adoptee, Tasmania)
I have four children and there are various ages and stages when I have struggled a bit with parenting, in terms of showing affection and that sort of thing. And I found a Facebook adoption support group and I talked to other adoptees at my work and found that's quite a common experience to have difficulty relating to your children. So I think parenting in general and interpersonal relationships are an issue for a lot of adoptees and that's where the support is also needed. Not just the immediate adoption experience, but also the ramifications of that long-term, and how that affects the next generation. (Tasmania)
Participants expressed frustration with not knowing where they can get advice, support, information or referral at the time they need it. The need for timely contact with someone in a supporting role is a significant issue. Many participants suggested a 24-hour telephone line staffed by trained professionals as one way to address the issues of immediacy and accessibility. However, the ability to physically go to a place where they could see a counsellor that they know is knowledgeable about adoption issues was also seen as important.
Specialist services would need to offer a range of support options, such as information and referral to more in-depth counselling by trained staff. Another option in this vein would be online counselling options, such as those that are currently used in the mental health and alcohol and other drugs sectors.
Peer support
I think a diversity of support groups: one about the search, one about the track-down issues and navigating two families. And the tricky birth mother relationships. Dealing with emotions, dealing with society's responses of what you are going through. (Adoptee, Victoria)
The findings of the study suggest that there is a role for peer support models, with a diversity of options within this type of support seen as necessary. Peer support is a viable option for people living in all locations, and can provide the opportunity to meet other individuals who have shared experiences, which acts to normalise their own experience. Peer support can also support those who are at different stages of their adoption journey, and can be a useful source of information and advice from those who are further along the continuum. Peer support also seems to work well as an avenue of support that is available when required (i.e., it is easy to engage and disengage as necessary). The Senate Inquiry (2012) also acknowledged the valuable role that peer support models can play for those affected by forced adoptions.
Some participants were also aware of the different benefits that can be obtained from peer versus professional support:
Both [peer and professional support] can benefit an enormous amount. It is beneficial to share experiences in a supportive way and it is really validating to know that someone else has gone through that as well. But certainly you need that sort of professional person there, and ideally professionals that are working on adoption stuff and they know all those issues. (Adoptee, Queensland)
Our experience of conducting the focus groups, in terms of how easy it was to coordinate, how much participants valued it, and how the vast majority were in favour of such avenues for peer discussion being available in their local area, provides a strong indication that such groups could be readily established and supported (see Box 11.3 on page 217). There are and have been a number of groups established in metropolitan areas; however, data from our study suggest a high level of need for such groups in regional and rural areas. One possibility of how this could be achieved is through the introduction of a "travelling road show", whereby the establishment of a support group is facilitated in rural and regional communities and sufficient guidance provided to let the community lead the way from there. Local community houses could be appropriate venues. It only takes someone to get it started, and with the appropriate level of connection to more formalised support services staffed by trained professionals, this could well be a viable option for providing a solution to an identified support need within this cohort.
Another option that was suggested is to incorporate adoption-related support into existing services, such as family support services, parenting services, or existing phone line services. This was seen as being a particularly useful option for adopted individuals in relation to strategies to deal with issues in their own parenting that are associated with their adoption experience:
Rather than a standalone agency, I think you could incorporate that into the support that is already there for families. So incorporating that into family support resources that are already up and running, and educating those professionals would probably be the most sensible approach. (Adoptee, Tasmania)
Information and support resources
There were many creative ideas that participants suggested as to how better information and support resources could be provided. Some examples included:
- publications that explain the history of adoption, the common reasons for adoption and the common emotional outcomes:
- a series of short easy-to-read well-presented fact sheets on key aspects (such as the mothers' experiences, the adopted persons' experiences, the adoptive parents' experiences, other family members' experiences, how to find information about your birth family, and so on);
- for the wider circle of family members, information resources with advice on how to best support their loved one who is affected by adoption;
- a booklet that contains stories of people affected by past adoptions, in their own words, that gives insight into a variety of experiences, and which could be distributed widely for doctors' waiting rooms and the like; and
- a comprehensive website with all the issues relating to adopted people through the different life stages (such as giving birth) linked up to the most up-to-date research, fact sheets, help sheets, information resource sheets, appropriate contact details (for seeking help, such as counselling), and links to government and non-government agencies where people can find assistance with making contact with birth parents.
Current adoption environment and donor conception
Although not included within the scope of this study, current adoption policies and donor conception in Australia were raised on a very frequent basis, both within the survey open-response items and the focus group discussions. As these are areas that study participants identified as being issues of concern, we will therefore present some of the more pertinent points within this discussion. As we highlighted earlier in this chapter, one mother's viewpoint, which we will use again now, encapsulates the broader sentiments of study participants who spoke of these issues.
Without understanding the past, how can we hope to appropriately inform the right actions going forward? (Mother, WA)
Both adoptees and mothers in particular raised their concerns regarding broader community attitudes to current overseas adoptions in Australia; in particular, that the needs of the child aren't necessarily at the centre of people's motivations to adopt. The issues of identity, attachment and "knowing where you come from" were all highlighted as being potential effects on children adopted from overseas if there is a failure to properly inform the child of their heritage and integrate that knowledge and culture into their everyday life. The view of the child as a commodity; something that is "acquired", ran parallel to the stories of many of the adoptees who participated in this study's own adoption experience. The attempt to assimilate the child into Australian culture without recognition of their family and country of birth is a major concern for many who are concerned that history will indeed repeat itself.
While not raised by all adoptees, a fairly common theme was the parallels between their past experiences with adoption, and current issues with intercountry adoption, donor conception and surrogacy. Their concerns are that children are being put in similar situations where they will never know who both their parents are, and where the focus is on the needs of the parents, not the child. Adoptees often talked about how adoption should be the last resort and only for children who don't have anyone who is fit to raise them:
It is still something that people believe is the right thing to do. Intercountry adoption is seen as quite acceptable; to go to another country and bring that child over - pay someone $5,000 to take the child. It's huge, and I think we need to - for those people [intercountry adoptees] to have a voice and say, this is what it did to us. (Adoptee, SA)
Why aren't we supporting them to keep their own children instead of changing somebody's name, changing their cultural heritage, changing everything, creating a false identity, putting them in a family that's nothing like them. I don't think adoption makes sense unless it's really severe circumstances, or they are actually completely orphans. (Adoptee, Qld)
The education of potential adoptive parents was seen as being imperative for many study participants - in terms of what has transpired for those who have been affected by past adoption experiences - so that they can be better informed about the potential issues.
Some participants commented that the "solution" to infertility has shifted from adopting Australian babies of unmarried mothers, to adopting those living in communities where the economic disadvantage is so devastating that those families find it difficult to afford to keep their children in their care. It is not about their families "not wanting" them:
Now we have overseas adoption and I think the problem has just been transferred to other societies. There will be the same problems, but they will be harder to solve. (Adoptee, 407, 2012)
The Senate Inquiry (2012) also highlighted the complexities of the current adoption climate in Australia and determined that the findings of their report be considered in any discussions about local adoptions (section 13.16), and the information provided to the Committee is consistent with the contributions made by participants in this study.
11.6 Summary of implications for best practice models
If a government can't support these sorts of initiatives, then they shouldn't be supporting the practices. (Mother, WA)
The following summarises the information arising from the study that can be used in the development of best practice models or practice guidelines for the delivery of supports and services for individuals affected by past practices.
The feedback from the service providers corroborated what mothers and adoptees told us about their experiences of accessing services. The predominant issue was that there were not enough services, and when they were available, the professionals were often not knowledgeable on adoption-specific issues. Furthermore, many clients were not aware of the services available and those who were aware often found that the cost of the services made long-term involvement prohibitive.
The service providers involved in the survey had very similar perceptions of the service system, its strengths and its weaknesses, with the strongest message from them being the need for support for counselling. Financial support to assist people affected by past adoption experiences to afford counselling, as well as training support to assist in the development and cost of training counsellors in adoption-specific issues. One respondent suggested implementing a model similar to Find and Connect, which is a service developed to address the needs of people who have been in out-of-home care as children, whether as Forgotten Australians or former child migrants.
Service professionals also held similar views in relation to there being a need for more awareness around the issues stemming from past adoption experiences and promotion of the services available. Respondents advocated for public awareness campaigns involving the media, government agencies and other organisations. As with the mothers, service providers believed that validating the experiences of those affected by past experiences of adoption was fundamental and a first step to addressing the stigma associated with adoption.
Many respondents were mindful that the inadequate availability of information on adoption-related issues also needs to be tackled. This included the availability of information on best practice models for organisations as well as information about birth families for clients themselves. They advocated for the facilitation of access to information, and wanted increased funding for search, contact and reunion services; funding; training; and inter-agency cooperation.
Respondents supported the development of a system-wide network that can connect clients with services, and support services with other related services. Furthermore, search and reunion organisations advocated for a better relationship with government agencies to assist in the sharing of information.
Funding is a key issue that overlaps many of the previous discussion points. Primarily, funding for counselling was strongly advocated.
There were divergent views about the capacity of existing systems to effectively meet the needs of people affected by past adoptions. Some common strategies that were identified within both the core group as well as service provider components of the study around how the needs of those affected by past adoption experiences could be addressed include:
- Improving education and training of professionals who work with people affected by past adoption practices, such as counsellors, social workers, mental health professionals. Respondents believed that better professional development and training in adoption-related issues would assist in meeting the needs of those affected and that this could be addressed through improving education and training. Respondents frequently suggested one way this could be achieved is to include education about adoption in tertiary education for a range of welfare professionals so they are capable of helping clients deal with issues such as grief and loss, identity, shame, trauma, excess feelings of guilt, rejection, emotions of anger/hurt, difficulty maintaining friendships or close relationships with family (attachment issues), anxiety, and self-confidence problems.
Other suggestions of how this could be achieved were by:
- publishing good practice guidelines;
- funding conferences for national post-adoption workers;
- dissemination of information and research; and
- conducting research into topics of adoption (especially longitudinal studies).
- Enriched awareness and information in both the professional community and in the general public would be beneficial in addressing the needs of clients. A "concerted effort" is needed so that the "lifelong impacts of adoption" can be addressed. Respondents proposed increasing promotional material, with information about adoption issues and relevant services being made available to people affected by past adoption experiences.
Broader "advertising" of the past practices of adoption as well as the availability of services for those in need could improve the general public's understanding of issues resulting from past adoption experience and strip the shame and stigma associated with it. Suggestions of how to achieve this included:
- educating teachers, hospital staff, allied health practitioners, mental health workers, counsellors, social workers, ministers of religion etc.;
- government awareness campaigns; and
- interviews/discussions in the media.
The media was seen as playing a role in this broader awareness raising. Many respondents asserted that television programs such as Find my Family encourage an inaccurate perception of adoption issues.
- Improved funding for specialised adoption services, as well as funding to assist people on a fixed or low income who struggle to afford the costs of adoption-related services. A large proportion of service providers who participated in the study believed that their clients are in need of counselling and support services; however, the current availability of such services was considered to be inadequate and too costly.
Study participants were for the most part supportive of the provision of funding to make counselling more affordable for those affected. Improved funding encompasses all aspects of investment: funding to support ongoing or intermittent counselling as well as for training more counsellors and publicising the availability of these services. Access to counselling services for all people affected by past adoption practices could be delivered in a format similar to that offered to the Forgotten Australians and former child migrants.
- Better networking would improve the liaison between organisations, agencies and state/territories around best practice issues. This could be achieved through an improved interagency network that facilitated this communication. Suggestions on how to achieve this included:
- developing a practitioner network similar to the Mental Health Practitioner Network; and
- standardising legislation across jurisdictions.
- Support with search, contact, and mediation, which was identified as an issue across all respondent groups as well as service providers. This included assistance with the contact phase and with mediating between families, and informing families of their adoption experience (mothers) or their intent to find their birth families (adoptees). Intermediary and mediation services are needed for clients who require assistance during the reunion process in managing the contact with the birth family.
- Facilitating access to information - Suggestions on how to achieve this included:
- ensuring consistent access policies from Births, Deaths and Marriages departments across all states;
- digitising records and housing a searchable database in each state;
- simplifying the process of accessing information;
- waiving fees for accessing records;
- reviewing privacy laws in the context of adoption;
- employing more caseworkers, researchers administration support and staff;
- providing materials to share with clients on adoption-related issues, including simple fact sheets with information about which agencies offer which services in each state, through to material describing the effects of adoption and sharing stories about reunion, and healing journeys;
Other suggestions for improving the services provided included:
- offering online and telephone support services to provide access to clients in rural and remote areas;
- encouraging face-to-face interactions with clients when providing adoption information, allowing counsellors who have established a relationship with client to pass on sensitive information;
- providing external clinical supervision and support;
- promoting awareness about past adoption practices from government/community; and
- enhancing cooperation between various agencies providing support for people affected by past adoption experiences.
11.7 Conclusion
Across the various respondent groups, despite the range of views and issues raised, there are some important areas where the majority of participants aligned in relation to the needs and priority actions for responding to the ways closed adoption has affected their lives. These include:
- acknowledgement and recognition of past practices (including the role of apologies and financial resources to address current service and support needs);
- raising community education and awareness of past practices and subsequent impacts;
- providing specialised workforce training and development for primary health carers, mental and broader health and welfare professionals to appropriately respond to the needs of those affected;
- reviewing the current search and contact service systems, with commitment for improved service models;
- improving access to information through the joining of state and territory contact databases, governed by a single statutory body;
- improving access and assistance with costs for mental, behavioural and physical health services; and
- ensuring that lessons from past practices are learned, and translated where appropriate into current child welfare policies, and that adoption-specific services are created or enhanced to respond to the implications of past practices.
11.8 Strengths and limitations of the current study
There are some serious limitations to the study that should be noted.
Most importantly, data were collected from a self-selected sample as there is no identified database or other sampling frame from which to randomly invite people to participate. Therefore, we cannot say with confidence that our findings are representative of all people who have experienced closed adoption in Australia.
Also, the data were collected "within the shadow" of the Australian Government's Senate Community Affairs References Committee's inquiry into former forced adoption policies and practices, which ran from November 2010 to February 2012 (data collection for our study ran from August 2011 to May 2012). The publicity surrounding the inquiry may have influenced people's decision to participate, as well as the issues that were "front-of-mind" for them in responding to our survey or discussing issues with fellow participants in the focus groups. For example, we found that some topics - such as the role of a national apology - were raised spontaneously, which may have been influenced by the public discourse and interest group activism around the Senate Inquiry.
Finally, the purpose of our study was not to discern the "truth" of any one respondent's historic circumstances. It was a psychologically focused study - looking at people's reports of their experiences, but most particularly, on the ways in which they see their adoption experience as having affected them and with which issues they need services and supports. Therefore, the study identifies the strength and variety of views that participants had about past events and their impact on them now, and what they want to assist them in leading stronger, happier lives.
Nevertheless, there are numerous strengths to this study that mean the data will be a reliable source of information on the experiences and current needs of Australians affected by past adoption practices. These strengths include:
- the large number of respondents in the study (n = 1,528), which represents a small but significant proportion of people currently alive who are likely to have been affected by closed adoption from the mid- to late 20th century in Australia;
- the use of online surveys to facilitate ease of participation, supported by hard-copy surveys (as requested) and/or phone interviews, and supplemented by a very large in-depth follow-up series of focus groups and interviews with participants (n > 300);
- the wide-ranging approach to recruitment of participants, supported by a comprehensive communications strategy designed to raise awareness among all Australians of the existence of the study, and the opportunity for people with a closed adoption experience to participate and tell their story;
- our national perspective, with participants coming from all states and territories;
- the integration of quantitative and qualitative data to give quantifiable statistics, as well as rich accounts of people's lived experiences of closed adoption;
- the use of standardised measures of wellbeing, which allows comparison with other nationally representative data;
- the integration of different perspectives from the "adoption triangle" (as it is often called, or as we suggest here, the "adoption circle"): including mothers, fathers, adoptees, adoptive parents, and other family members;
- supplementing information on the current service needs of respondents with data from service providers and agencies responsible for specific adoption-related services (such as the Find and Connect service);
- reflecting the views of a wide variety of respondents, including those who are part of a support or advocacy group and others who are not affiliated in any way, and those who saw their experiences of adoption as being positive, neutral, or negative; and
- the use of neutral questions, and adopting an open and questioning approach to the topics (e.g., rather than assuming people's adoption experiences had been singularly negative or positive, we asked people to describe or rate it for themselves, so that we did not bias their response one way or another).
Our hope is that the rich detail provided of individuals' journeys through the period of closed adoption in Australia, through to the issues they now face, and to whom services and supports could be better targeted is reflective of the variety of perspectives that were shared with us. We also hope that the trust that more than 1,500 Australians placed in us to hear their journey and convey their messages is well placed, and that this report honours the pain, courage, joy, anger, energy and commitment that was so evident in the people who contributed.
Box 11.1: Key service system implications
Mothers
- Mental health professionals - including psychologists, psychiatrists and psychotherapists - will require specialised education and training to respond effectively to the needs of those affected by past adoptions. The two key issues mothers talked about that related to professional education were: (a) knowledge about the events that surrounded closed adoption and the range of experiences that those affected may have encountered; and (b) training in specialist therapeutic skills to address the ongoing effects of trauma, identity issues, negative self-concept, and relationship issues that relate specifically to the adoption experience. This suggests that development of appropriate training modules that are readily accessible to those working in such professions is needed.
- Many current service provision agencies and professions (e.g., church-based agencies, social workers) are strongly associated in the minds of many mothers with their experiences of trauma. Any expansion or creation of new services should be undertaken with sensitivity to this.
- As well as developing a specialist workforce, health and welfare professionals in the broader services would benefit from education about the effects of past adoptions on mothers (including potential physical, social and psychological effects), and training in how to provide appropriate assessment, diagnosis and referral to specialists.
- Post-adoption support services would be obvious places that could act as central points for the provision of information and referral to the broader health and welfare sectors.
- With appropriate resourcing, existing post-adoption services could provide ongoing engagement with those who are at all stages of their adoption journeys. Continuity of care (i.e., not having to repeat one's "story" or build rapport with a new service provider) will play a significant part in the likelihood of those affected feeling adequately supported.
- Addressing current physical and mental health problems that mothers attribute to their past adoption experiences is closely linked to recognising their need for acknowledgement, restitution and positive self-identity.
Fathers
Fathers' accounts suggest areas of improved service provision relate to:
- inclusion of their names on birth certificates;
- access to "search and contact" services;
- advice and assistance with managing ongoing contact with son/daughter, including assistance with helping sons/daughters understand why they were adopted, and that it wasn't necessarily the fathers' choice;
- funded, professional counselling by qualified counsellors who have an understanding of adoption issues and its effects (including post-traumatic stress);
- coordination of peer supports for fathers who have been damaged by their experience of adoption; and
- increased societal awareness and understanding of what happened and why, and acknowledgement of the injustice of past practices.
Persons who were adopted
- Addressing the variability between state and territory-based systems and laws regarding adoptees' access to information would be of significant benefit. The difficulties in navigating often complex systems, along with the associated costs, has been identified as a barrier to the formation of sense of self and identity, as well obtaining potentially life-saving information regarding medical histories. The centralisation of all state and territory databases would be the most efficient way of addressing this issue.
- Reviewing and potentially harmonising state and territory laws relating to contact and information vetos was seen as a high priority. Currently, vetos are seen by many adoptees to deny them access to medical/genetic information that they regard as their right, and differences in state/territory laws also create difficulties for situations where the two parties live in two different jurisdictions, or a different jurisdiction from where the adoption occurred. Harmonisation would still need to take into account the needs of those adoptees and birth family member(s) who do not wish to be personally identified in the information provided.
- Mental health professionals, including psychologists, psychiatrists and psychotherapists, will require specialised education and training to respond effectively to the needs of those affected by past adoptions. Key issues adoptees talked about that related to professional education were: (a) knowledge about the range of experiences that those affected may have encountered, including abuse and neglect and late discovery of adoption; and (b) training in specialist therapeutic skills to address the ongoing effects of identity issues and negative self-concept, and relationships that relate specifically to the adoption experience. This suggests that development of appropriate training modules that are readily accessible to those working in such professions is needed.
- As well as developing a specialist workforce, health and welfare professionals in the broader system would benefit from education about the effects of past adoptions on adoptees, and the potential physical, social and psychological effects. They would also benefit from training in how to provide appropriate assessment, diagnosis and referral to specialists.
- With appropriate resourcing, existing post-adoption services could provide ongoing engagement throughout the adoption journey. Continuity of care (i.e., not having to repeat one's "story", and build rapport with a new service provider) will play a significant part in the likelihood of those affected feeling adequately supported.
Adoptive parents
Adoptive parents talked about the need for ongoing support at the time of the adoption, so were less focused on current service needs. Their accounts suggest areas of improvement to current service provision relate to:
- managing contact with birth parents;
- managing their own emotions when children decide to seek information or make contact with birth parents;
- assistance with medical information/family history for their son/daughter;
- public awareness of adoption issues to be balanced with positive stories, and reflecting the motivations of adoptive parents (e.g., many assumed they were doing a service by keeping a baby out of institutional care); and
- some (limited) need for peer support or professional counselling services for themselves, but more so for their sons/daughters (especially during the search/contact process).
Other family members
Other family members who completed surveys or participated in focus groups talked about the need for ongoing support for themselves, as well as their family members. Their accounts suggest areas of improvement to current service provision relate to:
- support to help them deal with traumatised family members;
- wanting help and direct support for their family member affected by adoption; and
- public acknowledgement of (including an apology for) past experiences and its effects to create awareness and greater openness.
Service providers
The most common suggestions by respondents for enhancing the services provided by the support system were:
- improving access to information and awareness on:
- services operating and a referral list of trained colleagues;
- available training;
- developments within the adoption community; and
- best practice and procedure;
- increasing funding for:
- employing more caseworkers, researchers administration support and staff;
- subsidising counselling and other relevant services for people affected by adoption;
- allowing professionals more time to work with clients;
- promoting the services offered by agencies;
- arranging training, seminars and workshops; and
- research into issues relating to adoption and the various healing modalities that can be employed to assist the professionals providing support;
- providing materials to share with clients on adoption-related issues:
Materials and resources to share with people affected by adoption, from simple fact sheets with information about which agencies offer which services in each state, to material describing the impact of adoption and sharing stories about reunion, healing journeys.
Other suggestions for improving the services provided included:
- offering online support services to provide access to clients in rural and remote areas;
- encouraging face-to-face interactions with clients when providing adoption information, allowing counsellors who have established a relationship with their client to pass on sensitive information;
- providing external clinical supervision and support;
- promoting awareness by government and other relevant agencies about past adoption practices; and
- enhanced cooperation between various agencies to provide support for people affected by past adoption experiences.
Box 11.2: Key features of good practice
The implications from our study for "good practice" when implementing improvements to service provision are summarised in terms of information delivery; search and contact services, and other professional and informal counselling and supports.
1. Good information services (including identifying information and access to personal records) are:
- delivered by trained staff;
- responsive to requests in a timely way;
- accessible through moderated websites, and/or 24-hour phone lines;
- provided with sensitivity to the needs of those seeking it (confidentiality, discretion, language used, etc.);
- relevant to the "stage of the journey" of individuals; and
- provided with a range of support levels (e.g., access to support person - onsite and follow-up).
2. Good search and contact services:
- enable access to counselling and ongoing support during the search and contact journey;
- provide advice and information about what to expect throughout the entire journey, not just about how to search;
- use an independent mediator to facilitate searching for information and exchanging information; and
- address expectations before contact is made and provide ongoing support afterwards.
3. Quality professional and informal supports:
- incorporate adoption-related supports into existing services (such as Family Support Program funded services, or Medicare-funded psychological services);
- provide options for both professional and peer supports; and
- address trauma, loss, grief and identity issues.
Across all three types of services, the following elements of good practice also apply:
- Formalised complaints processes are made known and readily available to service users to ensure service accountability.
- Staff are available to be a point of contact when/if needed and there are flexible hours of operation to accommodate the varying needs of service users. This also includes meeting the needs of those living in more remote locations, where access to a physical site may be impossible.
- Service providers are well-informed and understand the issues associated with adoption for all members of the adoption circle.
- Ongoing support and follow-up from the agency involved is provided, in acknowledgement that for those affected, it's not just about getting the information and then being left to deal with the outcomes of contact.
- Support, education and information for the other family members is readily available.
29 These data are taken from Wave 8 of the HILDA survey. The survey uses an 11-point scale (0 to 10) for its life satisfaction scale. To make this more comparable with our 10-point measure, we rescaled the HILDA scores by a factor of 10/11.
30 Our methodology does not allow us to conclude whether all mothers have this same risk profile, or whether there were fewer mothers with positive mental health who chose to participate in the current study.
31 The potential for - and the reality of - these conflicts was similarly noted in the Senate Inquiry report (2012).
References
- Australian Bureau of Statistics. (1988). Year book Australia (Cat. No. 1301.0). Canberra: ABS.
- Australian Institute of Health and Welfare. (2009). Adoptions Australia 2007-08 (Child Welfare Series No. 46; Cat. No. CWS 34). Canberra: AIHW. Retrieved from <www.aihw.gov.au/publications/>.
- Australian Institute of Health and Welfare. (2012). Adoptions Australia 2010-11 (Child Welfare Series No. 52). Canberra: AIHW. Retrieved from <www.aihw.gov.au/publication-detail/?id=10737420776>.
- Bowlby, J. (1969). Attachment: Vol. 1. Attachment and loss. London: Hogarth.
- Clapton, G. (2007). The experiences and needs of birth fathers in adoption: What we know now and some practice implications. Practice: A Journal of the British Association of Social Workers, 19(1), 61-71.
- Cole, C. A. (Ed.). (2008). Releasing the past: Mothers' stories of their stolen babies. Sydney: Sasko Veljanov.
- Cole, C. A. (2009). The thin end of the wedge: Are past draconian adoptive practices re-emerging in the 21st century? Public submission to the National Human Rights Consultation. Canberra: National Human Rights Consultation.
- Coles, G. (2009). Why birth fathers matter. (PDF 32 KB) Australian Journal of Adoption, 1(2). Retrieved from <www.nla.gov.au/openpublish/index.php/aja/article/view/1542/1847>.
- Connor, P. K., & Higgins, D. J. (2008). The "HEALTH" Model: Part 1. Treatment program guidelines for complex PTSD. Sexual and Relationship Therapy, 23(4), 293-303.
- Farrar, P. D. (1998). "What we did to those poor girls!" The hospital culture that promoted adoption. In Separation, reunion, reconciliation: Proceedings of the Sixth Australian Conference on Adoption, Brisbane, June 1997 (pp. 116-127). Stones Corner, Qld: J. Benson for Committee of the Conference.
- Goodwach, R. (2001). Does reunion cure adoption? Australian and New Zealand Journal of Family Therapy, 22(2), 73-79.
- Grafen, M., & Lawson, M. (1996). Relinquishing and non-relinquishing mothers: Emotionality, personality, and experience. Interlogue, 7(1), 50-64.
- Higgins, D. J. (2012). Past and present Adoptions in Australia: Facts sheet. Melbourne: Australian Institute of Family Studies. Retrieved from <www.aifs.gov.au/institute/pubs/factssheets/2012/fs201202/fs201202.html>.
- Higgins, D. J. (2011a). Current trauma: The impact of adoption practices up to the early 1970s. Family Relationships Quarterly, 19, 6-9. Retrieved from <www.aifs.gov.au/afrc/pubs/newsletter/frq019/frq019-2.html>.
- Higgins, D. J. (2011b). Unfit mothers … unjust practices? Key issues from Australian research on the impact of past adoption practices. Family Matters 87, 56-67. Retrieved from <www.aifs.gov.au/institute/pubs/fm2011/fm87/fm87g.html>.
- Higgins, D. J. (2010). Impact of past adoption practices: Summary of key issues from Australian research(Final Report). Canberra: Department of Families, Housing, Community Services and Indigenous Affairs. Retreived from <fahcsia.gov.au/our-responsibilities/families-and-children/publications-articles/impact-of-past-adoption-practices-summary-of-key-issues-from-australian-research>.
- Hunter, C. (2011). Defining the public health model for the child welfare services context (NCPC Resource Sheet). Melbourne: Australian Institute of Family Studies. Retrieved from <www.aifs.gov.au/nch/pubs/sheets/rs11/index.html>.
- Inglis, K. (1984). Living mistakes: Mothers who consented to adoption. North Sydney, NSW: Allen and Unwin.
- Iwanek, M. (1997). Healing history: The story of adoption in New Zealand. Social Work Now, 8, 13-17.
- Lindsay, V. (1998). Adoption trauma syndrome: Honouring the survivors. In Separation, reunion, reconciliation: Proceedings of the Sixth Australian Conference on Adoption, Brisbane, June 1997 (pp. 239-254). Stones Corner, Qld: J. Benson for Committee of the Conference.
- McGuire, G. (1998). You only have one mother. Springwood, NSW: Conference Publications.
- National Transport Commission. (2006). National Standard for Health Assessment of Rail Safety Workers: The Kessler Psychological Distress Scale (K10)(PDF 177 KB) (Fact Sheet for Authorised Health Professionals). Melbourne: National Transport Commission. Retrieved from <www.ntc.gov.au/filemedia/bulletins/RAILKesslerFactSheetAug2006.pdf>.
- New South Wales Law Reform Commission. (1993). Review of the Adoption of Children Act 1965 (Issues Paper No. 9). Sydney: NSWLRC.
- New South Wales Legislative Council Standing Committee on Social Issues. (2000). Releasing the past: Adoption practices 1950-1998. Final report (Report 22; Parliamentary Paper No. 600). Sydney: NSW Legislative Council.
- Marshall, A., & McDonald, M. (2001). The many-sided triangle: Adoption in Australia. Carlton, Vic.: Melbourne University Press.
- Murphy, K., Quartly, M., & Cuthbert, D. (2009). "In the best interests of the child": Mapping the (re) emergence of pro-adoption politics in contemporary Australia. Australian Journal of Politics & History, 55, 201-218.
- Passmore, N. L., & Coles, G. (2008, 2-5 September). The impact of relinquishment on birth fathers. Paper presented at the 9th Australian Adoption Conference, Sydney.
- Passmore, N. L., & Coles, G. (2012). Birth fathers' perspectives on reunions with their relinquished children. Manuscript submitted.
- Rickarby, G. (1998). Adoption grief: Irresolvable aspects. In Separation, reunion, reconciliation: Proceedings of the Sixth Australian Conference on Adoption, Brisbane, June 1997 (pp. 54-58). Stones Corner, Qld: J. Benson for Committee of the Conference.
- Senate Community Affairs References Committee (2012). Commonwealth contribution to former forced adoption policies and practices. Canberra: Senate Community Affairs References Committee.
- Swain, P., & Swain, S. (Eds.) (1992). The search of self: The experience of access to adoption information. Sydney: Federation Press.
- Swain, S., & Howe, R. (1995). Single mothers and their children: Disposal, punishment and survival in Australia. Oakleigh, Vic.: Cambridge University Press.
- van der Kolk, B. A., & McFarlane, A. C. (1996). The black hole of trauma. In B. A. van der Kolk, A. C. McFarlane, & L. Weisaeth (Eds.), Traumatic stress: The effects of overwhelming experience on mind, body, & society (pp. 3-23). New York: Guildford.
- Verrier, N. (1998). Adoption: The need for a new paradigm. In Separation, reunion, reconciliation: Proceedings of the Sixth Australian Conference on Adoption, Brisbane, June 1997 (pp. 9-17). Stones Corner, Qld: J. Benson for Committee of the Conference.
- Verrier, N. (n. d.). Adoption: The primal wound. Effects of separation from the birth mother on adopted children. Retrieved from <www.freewebs.com/ksattach/Adoption%20The%20Primal%20Wound.doc>.
- Winkler, R., Brown, D. W., van Keppel, M., & Blanchard, A. (1988). Clinical practice in adoption (Psychology Practitioner Guideline Books). Oxford: Pergamon.
- World Health Organization. (1997). WHOQOL: Measuring quality of life. (PDF 69 KB) Geneva: WHO. Retrieved from <www.who.int/mental_health/media/68.pdf>.
Attachment A - Technical Advisory Group
A1 Technical Advisory Group (TAG) Membership
Membership of the Technical Advisory Group comprised representatives from among research academics, and from service agencies and government organisations:
- Mr Brian Babington, Families Australia
- Ms Kathleen Clark, The Benevolent Society
- Dr Susan Gair, James Cook University
- Dr Daryl Higgins, Australian Institute of Family Studies
- Associate Professor Renate Howe, Deakin University
- Associate Professor Nola Passmore, University of Southern Queensland
- Ms Kathie Scott, Queensland Department of Communities, representing CDSMAC
- Professor Shurlee Swain, Australian Catholic University
- Ms Tricia Murray, Wanslea Family Service Inc., representing the Child and Family Welfare Association of Australia
- Ms Karen Wilson, Department of Families, Housing, Community Services and Indigenous Affairs
A2 Terms of reference for TAG
The terms of reference for the Technical Advisory Group were to:
- advise on the project scope and methodology;
- assist with the communication strategy and recruitment of respondents;
- contribute to the survey instrument development; and
- provide other advice and feedback to the study as requested.
Attachment B - Mothers separated from child by adoption: Quantitative tables
B1 Characteristics of child and mother when child born
| Child's characteristics | Number | Per cent |
|---|---|---|
| Sex of child | ||
| Male | 272 | 54.0 |
| Female | 230 | 45.5 |
| Twins: | 3 | 0.6 |
| Both twins male | 2 | 0.4 |
| Both twins female | 1 | 0.2 |
| No. of observations | 505 | 100.0 |
| Year of child's birth | ||
| Prior to 1960 | 21 | 4.2 |
| 1960-64 | 82 | 16.2 |
| 1965-69 | 171 | 33.8 |
| 1970-74 | 149 | 29.4 |
| 1975-79 | 52 | 10.3 |
| 1980 and later | 30 | 5.9 |
| No. of observations | 505 | 100.0 |
| Where child was born | ||
| New South Wales | 169 | 33.4 |
| Victoria | 119 | 23.5 |
| Queensland | 61 | 12.1 |
| South Australia | 51 | 10.1 |
| Western Australia | 41 | 8.1 |
| Tasmania | 12 | 2.4 |
| Northern Territory | 3 | 0.6 |
| Australian Capital Territory | 6 | 1.2 |
| Overseas | 35 | 6.9 |
| Missing data | 8 | 0.4 |
| No. of observations | 505 | 100.0 |
| Region where born | ||
| Capital city | 406 | 80.4 |
| Regional centre | 69 | 13.7 |
| Rural area | 19 | 3.8 |
| Missing data | 11 | 1.8 |
| No. of observations | 505 | 100.0 |
| Place of birth | ||
| Hospital | 451 | 89.3 |
| Maternity home | 42 | 8.3 |
| Children's home | 3 | 0.6 |
| Private home | 2 | 0.4 |
| Church home | 1 | 0.2 |
| Other | 6 | 1.2 |
| No. of observations | 505 | 100.0 |
| Age of child when separated from mother | ||
| Separation immediately or soon after birth | 355 | 70.3 |
| Within a week | 100 | 19.8 |
| Within a month | 30 | 5.9 |
| Over a month | 20 | 4.0 |
| No. of observations | 505 | 100.0 |
Note: Percentages may not total exactly 100.0% due to rounding.
Source: Mothers separated from child by adoption
| Mother's characteristics | Number | Per cent |
|---|---|---|
| Age at time of birth a | ||
| 15 years and under | 26 | 5.1 |
| 16 years | 63 | 12.5 |
| 17 years | 71 | 14.1 |
| 18 years | 81 | 16.0 |
| 19 years | 104 | 20.6 |
| 20 years | 58 | 11.5 |
| 21 years | 38 | 7.5 |
| 22 years | 14 | 2.8 |
| 23 years | 19 | 3.8 |
| 24 years | 13 | 2.6 |
| 25 years and over | 18 | 3.6 |
| No. of observations | 505 | 100.0 |
| Year of mother's birth a | ||
| Prior to 1940 | 19 | 3.8 |
| 1941-45 | 70 | 13.9 |
| 1945-49 | 142 | 28.1 |
| 1950-54 | 156 | 30.9 |
| 1955-59 | 71 | 14.1 |
| 1960-64 | 30 | 5.9 |
| 1965 and later | 17 | 3.4 |
| No. of observations | 505 | 100.0 |
| Marital status | ||
| Never married | 459 | 90.9 |
| De facto/same-sex partnership | 13 | 2.6 |
| Separated/divorced | 10 | 2.0 |
| Missing | 23 | 4.6 |
| No. of observations | 505 | 100.0 |
| Relationship to father of child | ||
| Husband | 2 | 0.4 |
| Fiancé | 20 | 4.0 |
| De facto | 10 | 2.0 |
| Boyfriend/steady date | 338 | 66.9 |
| Acquaintance | 93 | 18.4 |
| Relative | 3 | 0.6 |
| Stranger | 20 | 4.0 |
| Refused to answer | 19 | 3.8 |
| No. of observations | 505 | 100.0 |
| Whether pregnancy the result of consensual sex | ||
| Yes | 412 | 81.6 |
| No | 54 | 10.7 |
| Refused to answer | 36 | 7.1 |
| Missing data | 3 | 0.6 |
| No. of observations | 505 | 100.0 |
| Where lived during pregnancy | ||
| Maternity home (church/charity-run) | 175 | 34.7 |
| With parent(s) | 117 | 23.2 |
| Boarding (worked as a domestic in return) | 53 | 10.5 |
| With relatives | 45 | 8.9 |
| By self | 29 | 5.7 |
| With friends | 18 | 3.6 |
| With the father of son/daughter | 16 | 3.2 |
| Hostels associated with the hospital | 11 | 2.2 |
| Other institution (including academic and vocational accommodation) | 13 | 2.6 |
| Group house (shared rental accommodation) | 8 | 1.6 |
| Family friends | 5 | 1.0 |
| Other | 6 | 1.2 |
| Missing data | 9 | 1.8 |
| No. of observations | 505 | 100.0 |
| Whether mother's parents knew of pregnancy | ||
| Both knew | 367 | 72.7 |
| Only mother knew | 37 | 7.3 |
| Only father knew | 1 | 0.2 |
| Only mother knew (father deceased) | 26 | 5.1 |
| Only father knew (mother deceased) | 12 | 2.4 |
| Parent(s) did not know | 55 | 10.9 |
| Parent(s) deceased | 7 | 1.4 |
| No. of observations | 505 | 100.0 |
Notes: a Age of mother at time of child's birth estimated from age of mother at time of interview and year child was born. Percentages may not total exactly 100.0% due to rounding.
Source: Mothers separated from child by adoption
B2 Details about birth of child
| Number | Per cent | |
|---|---|---|
| Aware of drugs given before, during or after birth | ||
| No | 179 | 36.8 |
| Yes | 308 | 63.2 |
| Drugs affected ability to make decision about child | ||
| Yes | 152 | 49.4 |
| No | 139 | 45.1 |
| Missing data | 17 | 5.5 |
| Experienced ongoing health effects from drugs | ||
| Yes | 89 | 28.9 |
| No | 196 | 63.6 |
| Missing data | 23 | 7.5 |
| No. of observations a | 487 | 100.0 |
| Whether treated with same level of care as other mothers | ||
| Yes | 121 | 24.8 |
| No | 366 | 75.2 |
| No. of observations a | 487 | 100.0 |
Note: a Respondents were given the option of not answering the questions about the birth of their child, as this could be distressing for them. Eighteen women chose not to answers these questions, so n = 487.
Source: Mothers separated from child by adoption
| Not at all | A little | Moderately | Mostly | Completely | Missing data | No. of observations a | |
|---|---|---|---|---|---|---|---|
| Age | 41 | 28 | 37 | 61 | 140 | 59 | 366 |
| Social and economic status | 74 | 29 | 25 | 45 | 107 | 86 | 366 |
| Race/ethnicity | 208 | 4 | 6 | 4 | 12 | 132 | 366 |
| Marital status | 2 | 4 | 19 | 47 | 278 | 16 | 366 |
| Religion | 179 | 19 | 12 | 10 | 21 | 125 | 366 |
| Other | 77 | 3 | 8 | 8 | 45 | 225 | 366 |
Note: a Only includes mothers who thought they had been treated with less care than other mothers (see Table B3; n = 366).
Source: Mothers separated from child by adoption
| Number a, b | Per cent ( n = 487) | Later found untrue | Missing data | ||
|---|---|---|---|---|---|
| Yes | No | ||||
| Baby had died c | 7 | 1.4 | 4 | 0 | 3 |
| Baby was "gone" | 60 | 12.3 | 47 | 12 | 1 |
| Mother was medically or emotionally unfit to make decisions | 118 | 24.2 | 82 | 21 | 15 |
| Baby had already been placed with a new family | 126 | 25.9 | 89 | 25 | 12 |
| Something else that led mother to believe she could not decide child's future | 233 | 47.8 | 188 | 32 | 13 |
| None of the above | 129 | 26.5 | |||
Notes: a Respondents were given the option of not answering the questions about the birth of their child, as this could be distressing for them. Eighteen women chose not to answers these questions, so n = 487. b Respondents could choose more than one option. c None of the mothers who were told that their baby had died received a death certificate. Percentages may not total exactly 100.0% due to rounding.
Source: Mothers separated from child by adoption
| Had contact with child | Applied for information about child | Someone else told me | Other | No. of observations a | |
|---|---|---|---|---|---|
| Baby had died b | 1 | 1 | 2 | 0 | 4 |
| Baby was "gone" | 7 | 19 | 8 | 13 | 47 |
| Mother was medically or emotionally unfit to make decisions | 3 | 21 | 19 | 31 | 74 |
| Baby had already been placed with a new family | 23 | 30 | 16 | 16 | 85 |
| Something else that led mother to believe she could not decide child's future | 22 | 34 | 62 | 58 | 176 |
Notes: a Only includes mothers who later found that what they were told at the time of birth was untrue (see Table B5). There is small amount of missing data for some of the categories which accounts for the discrepancies between this table and Table B5. b None of the mothers who were told that their baby had died received a death certificate.
Source: Mothers separated from child by adoption
B3 Contact with child at time of birth
| Number | Per cent ( n = 487) | |
|---|---|---|
| Advice about contact a | ||
| Advised against having contact | 167 | 34.3 |
| Prevented from having contact | 299 | 61.4 |
| No choice but to have contact | 19 | 3.9 |
| Completely my decision whether to have contact | 51 | 10.5 |
| Encouraged to have contact | 19 | 3.9 |
| None of the above | 23 | 4.7 |
| Given opportunity to see child after birth | ||
| No | 278 | 57.1 |
| Yes: | 209 | 42.9 |
| Once | 109 | 52.2 |
| A few times | 69 | 33.0 |
| Often | 23 | 11.0 |
| No. of observations | 487 | 100.0 |
| Encouraged to name child | ||
| Yes | 107 | 22.0 |
| No | 96 | 19.7 |
| Missing data | 284 | 58.3 |
| No. of observations | 487 | 100.0 |
Note: a Respondents could choose more than one option.
Source: Mothers separated from child by adoption
| Able to: | Yes | No | Sometimes | Missing data | No. of observations |
|---|---|---|---|---|---|
| Hold child | 109 | 86 | 9 | 5 | 209 |
| Nurse child | 29 | 140 | 5 | 35 | 209 |
| Bathe child | 19 | 148 | 0 | 42 | 209 |
| Feed child | 43 | 128 | 6 | 32 | 209 |
Note: Only includes mothers who were given the opportunity to see the child after birth (see Table B7; n = 209).
Source: Mothers separated from child by adoption
B4 Details about adoption
| Number | Per cent ( n = 505) | |
|---|---|---|
| Advice given about adoption a | ||
| I was told about financial support that was available to me if I kept my son/daughter/child | 9 | 1.8 |
| I was told about the possible long-term effects of my son/daughter/child being adopted | 8 | 1.6 |
| I was asked if anyone was pressuring me into placing my son/daughter/child for adoption | 11 | 2.2 |
| I was asked if I needed more time to think things through | 12 | 2.4 |
| I was told my consent must be given freely and voluntarily | 68 | 13.5 |
| The legal effect of consenting to adopt was explained to me | 105 | 20.8 |
| I was told I could revoke (take back) my consent in a given timeframe and given information about how to do this | 107 | 21.2 |
| None of these | 282 | 55.8 |
| Other | 0 | 0.0 |
| Consent process a | ||
| I believe I was affected by drugs administered to me during labour at the time the process of consent was undertaken | 90 | 17.8 |
| I recall I did not sign any documents consenting to my son/daughter/child's adoption | 17 | 3.4 |
| I do not recall whether I signed any documents consenting to my son/daughter/child's adoption | 46 | 9.1 |
| I recall I signed a form but I did not fully understand it (e.g., I thought it was just a temporary thing) | 89 | 17.6 |
| I believe someone else signed something on my behalf | 22 | 4.4 |
| I recall I freely and voluntarily consented to my son/daughter/child being adopted and signed the documents that were given to me | 113 | 22.4 |
| I signed something but I felt that I didn't have any other choice | 345 | 68.3 |
| None of these | 13 | 2.6 |
| Attempt to revoke consent | ||
| Yes: | 108 | 21.4 |
| My child was returned to me | 5 | 4.6 |
| I was told it was too late - child already adopted | 100 | 92.6 |
| Other/missing | 3 | 2.8 |
| No | 190 | 37.6 |
| Not aware that could revoke consent | 207 | 41.0 |
| No. of observations | 505 | 100.0 |
Notes: a Respondents could choose more than one option.
Source: Mothers separated from child by adoption
| Number | Per cent ( n = 505) | |
|---|---|---|
| Adoption organised through: a | ||
| Institution: | ||
| Hospital | 155 | 30.7 |
| Church | 129 | 25.5 |
| Government adoption agency | 143 | 28.3 |
| Maternity home | 98 | 19.4 |
| Home for children/ward of the state | 19 | 3.8 |
| Private: | ||
| Parents | 37 | 7.3 |
| Family GP | 18 | 3.6 |
| Family lawyer | 3 | 0.6 |
| Private adoption agency | 13 | 2.6 |
| Other | 25 | 5.0 |
| Individual: | ||
| Social worker | 98 | 19.4 |
| GP | 17 | 3.4 |
| Priest | 6 | 1.2 |
| Family friend | 1 | 0.2 |
| Other | 100 | 19.8 |
| Don't know | 69 | 13.7 |
| Whether opinion of father taken into account | ||
| Yes | 73 | 14.5 |
| No | 294 | 58.2 |
| Father did not know of pregnancy | 69 | 13.7 |
| Missing data | 69 | 13.7 |
| No. of observations | 505 | 100.0 |
| Whether copy of birth certificate received when child was born | ||
| No | 472 | 93.5 |
| Yes: | 33 | 6.5 |
| Father named on birth certificate | 6 | 18.2 |
| Father named on birth registration form, not certificate | 4 | 12.1 |
| Father not named on either registration form or certificate | 16 | 48.5 |
| Don't know/don't remember if father named/no longer have it | 3 | 9.1 |
| Other/missing data | 4 | 12.1 |
| No. of observations | 505 | 100.0 |
| How satisfied interests were looked after in adoption process | ||
| Completely satisfied | 9 | 1.8 |
| Mostly satisfied | 28 | 5.5 |
| Neither satisfied nor dissatisfied | 63 | 12.5 |
| Mostly dissatisfied | 63 | 12.5 |
| Completely dissatisfied | 339 | 67.1 |
| Missing data | 3 | 0.6 |
| No. of observations | 505 | 100.0 |
| Whether wanted to keep baby | ||
| Yes | 338 | 66.9 |
| No | 34 | 6.7 |
| Uncertain | 125 | 24.8 |
| Missing data | 8 | 1.6 |
| No. of observations | 505 | 100.0 |
| Whether believe could have kept child with sufficient financial and other support | ||
| Yes | 369 | 73.1 |
| No | 40 | 7.9 |
| Maybe | 86 | 17.0 |
| Missing data | 10 | 2.0 |
| No. of observations | 505 | 100.0 |
| Which of the following best describes adoption experience | ||
| I placed my child for adoption | 20 | 4.0 |
| I lost my child to adoption | 106 | 21.0 |
| I gave up my child for adoption | 105 | 20.8 |
| I surrendered my child for adoption | 58 | 11.5 |
| My child was taken from me | 78 | 15.4 |
| My child was stolen from me | 125 | 24.8 |
| Other | 11 | 2.2 |
| Missing data | 2 | 0.4 |
| No. of observations | 505 | 100.0 |
Notes: a Respondents could choose more than one option. Percentages may not total exactly 100.0% due to rounding.
Source: Mothers separated from child by adoption
B5 Support around time of pregnancy and birth
| Sources of support a | Number | Per cent ( n = 505) |
|---|---|---|
| Parents | 135 | 26.7 |
| Other family members b | 91 | 18.0 |
| Father of child | 51 | 10.1 |
| Friends | 72 | 14.3 |
| Social worker or counsellor | 38 | 7.5 |
| Registered psychologist or psychiatrist | 6 | 1.2 |
| GP | 21 | 4.2 |
| Church group | 15 | 3.0 |
| Support group | 4 | 0.8 |
| Did not have any supports | 215 | 42.6 |
| Did not want/need any supports | 6 | 1.2 |
| Other b | 82 | 16.2 |
Note: a Respondents could choose more than one source or support. b "Spouse" was not provided as an option for this question, so spouses may have been included in the categories of "Other" or "Other family members". Sometimes respondents specified "husband" in the "Other" category.
Source: Mothers separated from child by adoption
| Received support | Very helpful | Somewhat helpful | Not helpful | Unhelpful | Very unhelpful | Missing data | |
|---|---|---|---|---|---|---|---|
| Parents | |||||||
| Emotional support | 80 | 26 | 39 | 8 | 2 | 5 | |
| Family planning advice | 5 | 1 | 4 | ||||
| Financial | 69 | 35 | 25 | 3 | 3 | 3 | |
| Legal | 5 | 1 | 1 | 1 | 2 | ||
| Psychotherapy or counselling | 5 | 1 | 1 | 1 | 2 | ||
| Other | 25 | 3 | 13 | 5 | 1 | 2 | 1 |
| Other family members a | |||||||
| Emotional support | 72 | 33 | 30 | 5 | 1 | 3 | |
| Family planning advice | 4 | 2 | 1 | 1 | |||
| Financial | 17 | 9 | 5 | 2 | 1 | ||
| Legal | 5 | 1 | 3 | 1 | |||
| Psychotherapy or counselling | 5 | 3 | 2 | ||||
| Other | 23 | 8 | 8 | 2 | 1 | 1 | 3 |
| Father of child | |||||||
| Emotional support | 44 | 19 | 17 | 4 | 2 | 2 | |
| Family planning advice | 5 | 2 | 1 | 2 | |||
| Financial | 21 | 10 | 9 | 1 | 1 | ||
| Legal | 5 | 3 | 2 | ||||
| Psychotherapy or counselling | 6 | 1 | 1 | 2 | 0 | 2 | |
| Other | 2 | 2 | |||||
| Friends | |||||||
| Emotional support | 65 | 29 | 30 | 4 | 1 | 1 | |
| Family planning advice | 2 | 1 | 1 | ||||
| Financial | 3 | 1 | 1 | 1 | |||
| Legal | 3 | 1 | 1 | 1 | |||
| Psychotherapy or counselling | 3 | 1 | 1 | 1 | |||
| Other | 10 | 6 | 2 | 1 | 1 | ||
| Social worker/counsellor | |||||||
| Emotional support | 19 | 3 | 9 | 2 | 5 | ||
| Family planning advice | 6 | 1 | 1 | 1 | 3 | ||
| Financial | 4 | 1 | 1 | 2 | |||
| Legal | 8 | 1 | 5 | 2 | |||
| Psychotherapy or counselling | 14 | 1 | 3 | 2 | 1 | 7 | |
| Other | 7 | 1 | 2 | 3 | 1 | ||
| Registered psychologist or psychiatrist | |||||||
| Emotional support | 1 | 1 | |||||
| Family planning advice | 2 | 1 | 1 | ||||
| Psychotherapy or counselling | 4 | 1 | 3 | ||||
| Other | 1 | 1 | |||||
| GP | |||||||
| Emotional support | 7 | 3 | 3 | 1 | |||
| Family planning advice | 6 | 2 | 2 | 1 | 1 | ||
| Financial | 1 | 1 | |||||
| Legal | 1 | 1 | |||||
| Psychotherapy or counselling | 2 | 2 | |||||
| Other | 7 | 1 | 2 | 2 | 1 | 1 | |
| Church group | |||||||
| Emotional support | 6 | 1 | 1 | 1 | 3 | ||
| Family planning advice | 3 | 2 | 1 | ||||
| Financial | 3 | 1 | 1 | 1 | |||
| Legal | 2 | 2 | |||||
| Psychotherapy or counselling | 3 | 1 | 2 | ||||
| Other | 7 | 5 | 1 | 1 | |||
| Support group | |||||||
| Emotional support | 1 | 1 | |||||
| Family planning advice | 1 | 1 | |||||
| Psychotherapy or counselling | 1 | 1 | |||||
| Other | 1 | 1 | |||||
Note: a "Spouse" was not provided as an option for this question, so spouses may have been included in the categories of "Other" or "Other family members". Sometimes respondents specified "husband" in the "Other" category.
Source: Mothers separated from child by adoption
B6 Making contact with child
| Number | Per cent | |
|---|---|---|
| Ever tried to find information about child | ||
| No | 73 | 14.5 |
| Yes: | 432 | 85.5 |
| Did not try to search for child | 51 | 11.8 |
| Tried to search for child: | 381 | 88.2 |
| Used contact/reunion services | 292 | 76.6 |
| Did not use contact/reunion services | 134 | 35.2 |
| No. of observations | 505 | 100.0 |
| Had contact | ||
| Yes | 431 | 85.3 |
| No, because: | 69 | 13.7 |
| Have not wanted to establish contact | 2 | 2.9 |
| Believe it is child's choice to have contact and waiting for contact | 14 | 20.3 |
| Not been able to find any information about child | 8 | 11.6 |
| Have some information about child but have never met nor had communication | 14 | 20.3 |
| Child rejected the possibility of contact/relationship | 16 | 23.2 |
| There is a veto on contact with child | 11 | 15.9 |
| Child has passed away | 3 | 4.3 |
| Fear, guilt and emotional vulnerability | 10 | 14.5 |
| Other | 6 | 8.7 |
| Missing data | 5 | 1.0 |
| No. of observations | 505 | 100.0 |
Source: Mothers separated from child by adoption
| Number | Per cent | |
|---|---|---|
| Year first had contact | ||
| Prior to 1980 | 5 | 1.2 |
| 1980-84 | 11 | 2.6 |
| 1985-89 | 64 | 15.0 |
| 1990-94 | 142 | 33.3 |
| 1995-99 | 91 | 21.3 |
| 2000-04 | 47 | 11.0 |
| 2005-09 | 34 | 8.0 |
| 2010-11 | 33 | 7.7 |
| No. of observations | 427 | 100.0 |
| Age of mother at first contact | ||
| Under 30 years | 4 | 0.9 |
| 30-34 years | 22 | 5.2 |
| 35-39 years | 85 | 19.9 |
| 40-44 years | 119 | 27.9 |
| 45-49 years | 74 | 17.3 |
| 50-54 years | 56 | 13.1 |
| 55-59 years | 37 | 8.7 |
| 60-64 years | 19 | 4.4 |
| 65 years and over | 11 | 2.6 |
| No. of observations | 427 | 100.0 |
| Age of child at first contact | ||
| Under 10 years | 4 | 0.9 |
| 11-17 years | 18 | 4.2 |
| 18-19 years | 52 | 12.2 |
| 20-24 years | 135 | 31.6 |
| 25-29 years | 84 | 19.7 |
| 30-39 years | 57 | 13.3 |
| 40-49 years | 46 | 10.8 |
| 50-59 years | 22 | 5.2 |
| 60 years and over | 9 | 2.1 |
| No. of observations | 427 | 100.0 |
| Best way to describe contact with child | ||
| Ongoing relationship | 274 | 64.2 |
| Have met but no ongoing relationship | 108 | 25.3 |
| Have had contact but never met | 25 | 5.9 |
| Other | 7 | 1.6 |
| Missing data | 13 | 3.0 |
| No. of observations | 427 | 100.0 |
Notes: Only includes mothers who have had contact with their child (n = 427). Percentages may not total exactly 100.0% due to rounding.
Source: Mothers separated from child by adoption
| Very positive | Positive | No impact | Negative | Very negative | Totals | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | N | % | |
| Spouse | 79 | 24.9 | 99 | 31.2 | 68 | 21.5 | 39 | 12.3 | 32 | 10.1 | 317 | 100.0 |
| Other children | 81 | 23.1 | 137 | 39.0 | 52 | 14.8 | 52 | 14.8 | 29 | 8.3 | 351 | 100.0 |
| Parents | 21 | 8.1 | 70 | 27.0 | 59 | 22.8 | 61 | 23.6 | 48 | 18.5 | 259 | 100.0 |
| Other family | 56 | 16.6 | 123 | 36.4 | 82 | 24.3 | 47 | 13.9 | 30 | 8.9 | 338 | 100.0 |
Note: Totals include only those who responded to each option and for whom the particular family group was applicable.
Source: Mothers separated from child by adoption
B7 Support for mother since separation from child
| Sources of support a | Number | Per cent ( n = 505) |
|---|---|---|
| Parents | 44 | 8.7 |
| Other family members b | 94 | 18.6 |
| Father of child | 33 | 6.5 |
| Friends | 158 | 31.3 |
| Social worker or counsellor | 112 | 22.2 |
| Registered psychologist or psychiatrist | 147 | 29.1 |
| GP | 75 | 14.9 |
| Church group | 15 | 3.0 |
| Support group | 130 | 25.7 |
| Registered search/support organisation | 94 | 18.6 |
| Did not have any supports | 120 | 23.8 |
| Did not want/need any supports | 26 | 5.1 |
| Other b | 55 | 10.9 |
Notes: a Respondents could choose more than one source of support. b "Spouse" was not provided as an option for this question, so spouses may have been included in the categories of "Other" or "Other family members". Sometimes respondents specified "husband" in the "Other" category.
Source: Mothers separated from child by adoption
| Received support | Very helpful | Somewhat helpful | Not helpful | Unhelpful | Very unhelpful | Missing data | |
|---|---|---|---|---|---|---|---|
| Parents | |||||||
| Emotional support | 38 | 11 | 16 | 4 | 2 | 3 | 2 |
| Family planning advice | 3 | 1 | 1 | 1 | |||
| Financial | 16 | 9 | 4 | 2 | 1 | ||
| Legal | 2 | 1 | 1 | ||||
| Psychotherapy or counselling | 5 | 1 | 1 | 1 | 2 | ||
| Other | 3 | 2 | 1 | ||||
| Other family members | |||||||
| Emotional support | 91 | 33 | 43 | 9 | 1 | 2 | 3 |
| Family planning advice | 1 | 1 | |||||
| Financial | 3 | 2 | 1 | ||||
| Legal | 2 | 2 | |||||
| Psychotherapy or counselling | 7 | 1 | 4 | 1 | 1 | ||
| Other | 6 | 3 | 2 | 1 | |||
| Father of child | |||||||
| Emotional support | 27 | 9 | 10 | 1 | 2 | 1 | 4 |
| Financial | 3 | 2 | 1 | ||||
| Other | 6 | 2 | 1 | 1 | 2 | ||
| Friends | |||||||
| Emotional support | 148 | 66 | 69 | 5 | 1 | 2 | 5 |
| Family planning advice | 2 | 2 | |||||
| Financial | 3 | 2 | 1 | ||||
| Legal | 3 | 2 | 1 | ||||
| Psychotherapy or counselling | 12 | 4 | 6 | 2 | |||
| Other | 7 | 1 | 4 | 1 | 1 | ||
| Social worker/counsellor | |||||||
| Emotional support | 64 | 28 | 23 | 5 | 1 | 5 | 2 |
| Financial | 2 | 1 | 1 | ||||
| Legal | 2 | 1 | 1 | ||||
| Psychotherapy or counselling | 79 | 31 | 32 | 7 | 1 | 8 | |
| Other | 5 | 4 | 1 | ||||
| Registered psychologist or psychiatrist | |||||||
| Emotional support | 72 | 37 | 24 | 6 | 1 | 3 | 1 |
| Family planning advice | 1 | 1 | |||||
| Financial | 1 | 1 | |||||
| Legal | 2 | 2 | |||||
| Psychotherapy or counselling | 117 | 50 | 43 | 10 | 3 | 9 | 2 |
| Other | 4 | 3 | 1 | ||||
| GP | |||||||
| Emotional support | 47 | 15 | 23 | 4 | 2 | 2 | 1 |
| Family planning advice | 6 | 4 | 2 | ||||
| Financial | 0 | ||||||
| Psychotherapy or counselling | 19 | 8 | 10 | 1 | |||
| Other | 18 | 2 | 12 | 1 | 1 | 2 | |
| Church group | |||||||
| Emotional support | 13 | 5 | 3 | 3 | 1 | 1 | |
| Family planning advice | 1 | 1 | |||||
| Financial | 2 | 1 | 1 | ||||
| Legal | 1 | 1 | |||||
| Psychotherapy or counselling | 2 | 2 | |||||
| Other | 4 | 1 | 2 | 1 | |||
| Support group | |||||||
| Emotional support | 117 | 85 | 23 | 2 | 1 | 1 | 5 |
| Family planning advice | 0 | ||||||
| Financial | 1 | 1 | |||||
| Legal | 10 | 8 | 2 | ||||
| Psychotherapy or counselling | 16 | 10 | 5 | 1 | |||
| Other | 19 | 12 | 5 | 1 | 1 | ||
| Registered support organisation | |||||||
| Emotional support | 63 | 46 | 15 | 2 | |||
| Financial | 1 | 1 | |||||
| Legal | 10 | 7 | 1 | 1 | 1 | ||
| Psychotherapy or counselling | 29 | 18 | 8 | 1 | 2 | ||
| Other | 27 | 18 | 8 | 1 | |||
Source: Mothers separated from child by adoption
B8 Effects of separation
| Always | Often | Sometimes | Rarely/never | Totals | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | |
| At time of separation | 387 | 78.7 | 85 | 17.3 | 15 | 3.0 | 5 | 1.0 | 492 | 100.0 |
| Now | 241 | 49.8 | 214 | 44.2 | 28 | 5.8 | 1 | 0.2 | 484 | 100.0 |
Note: Totals include only those who responded to each option. Percentages may not total exactly 100.0% due to rounding.
Source: Mothers separated from child by adoption
| Event a | Number | Per cent ( n = 505) |
|---|---|---|
| Child's birthday | 342 | 67.7 |
| Mother's Day | 301 | 59.6 |
| Christmas | 230 | 45.5 |
| Mother's birthday | 114 | 22.6 |
| Father's Day | 87 | 17.2 |
| Other: | ||
| Every day | 22 | 4.4 |
| Family gatherings | 30 | 5.9 |
| Events were difficult until I met my child | 18 | 3.6 |
| Other | 42 | 8.3 |
| No especially hard times or events | 93 | 18.4 |
Note: a Respondents could choose more than one option.
Source: Mothers separated from child by adoption
| Not at all | A little bit | Moderately | Quite a lot | Extremely | Totals | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | N | % | |
| Any reminder brought back feelings about it | 44 | 9.0 | 70 | 14.3 | 66 | 13.5 | 151 | 30.9 | 157 | 32.2 | 488 | 100.0 |
| I had trouble staying asleep | 163 | 34.2 | 65 | 13.7 | 74 | 15.5 | 102 | 21.4 | 72 | 15.1 | 476 | 100.0 |
| Other things kept making me think about it | 99 | 21.0 | 89 | 18.9 | 79 | 16.7 | 124 | 26.3 | 81 | 17.2 | 472 | 100.0 |
| I felt irritable and angry | 147 | 31.1 | 83 | 17.5 | 74 | 15.6 | 91 | 19.2 | 78 | 16.5 | 473 | 100.0 |
| I avoided letting myself get upset when I thought about it or was reminded of it | 104 | 22.5 | 100 | 21.6 | 117 | 25.3 | 97 | 21.0 | 44 | 9.5 | 462 | 100.0 |
| I thought about it when I didn't mean to | 107 | 23.1 | 87 | 18.8 | 60 | 12.9 | 143 | 30.8 | 67 | 14.4 | 464 | 100.0 |
| I felt as if it hadn't happened or wasn't real | 247 | 54.2 | 49 | 10.7 | 43 | 9.4 | 65 | 14.3 | 52 | 11.4 | 456 | 100.0 |
| I stayed away from reminders about it | 181 | 39.8 | 76 | 16.7 | 80 | 17.6 | 74 | 16.3 | 44 | 9.7 | 455 | 100.0 |
| Pictures about it popped into my mind | 103 | 22.1 | 88 | 18.9 | 73 | 15.7 | 112 | 24.0 | 90 | 19.3 | 466 | 100.0 |
| I was jumpy and easily startled | 208 | 44.8 | 76 | 16.4 | 61 | 13.1 | 63 | 13.6 | 56 | 12.1 | 464 | 100.0 |
| I tried not to think about it | 147 | 32.1 | 92 | 20.1 | 78 | 17.0 | 90 | 19.7 | 51 | 11.1 | 458 | 100.0 |
| I was aware that I still had a lot of feelings about it, but I didn't want to deal with them | 122 | 26.1 | 78 | 16.7 | 80 | 17.1 | 87 | 18.6 | 100 | 21.4 | 467 | 100.0 |
| My feelings about it were kind of numb | 158 | 34.4 | 79 | 17.2 | 73 | 15.9 | 80 | 17.4 | 69 | 15.0 | 459 | 100.0 |
| I found myself acting or feeling as though I was back at that time | 167 | 35.9 | 86 | 18.5 | 51 | 11.0 | 77 | 16.6 | 84 | 18.1 | 465 | 100.0 |
| I had trouble falling asleep | 167 | 36.0 | 79 | 17.0 | 62 | 13.4 | 73 | 15.7 | 83 | 17.9 | 464 | 100.0 |
| I have waves of strong feelings about it | 77 | 18.4 | 59 | 14.1 | 10 | 2.4 | 103 | 24.6 | 170 | 40.6 | 419 | 100.0 |
| I tried to remove it from my memory | 228 | 49.6 | 59 | 12.8 | 52 | 11.3 | 64 | 13.9 | 57 | 12.4 | 460 | 100.0 |
| I had trouble concentrating | 158 | 34.4 | 80 | 17.4 | 92 | 20.0 | 77 | 16.8 | 52 | 11.3 | 459 | 100.0 |
| I tried to remove it from my memory | 228 | 49.6 | 59 | 12.8 | 52 | 11.3 | 64 | 13.9 | 57 | 12.4 | 460 | 100.0 |
| Reminders of it caused me to have physical reactions such as sweating, trouble breathing, nausea, or a pounding heart | 195 | 42.3 | 70 | 15.2 | 51 | 11.1 | 64 | 13.9 | 81 | 17.6 | 461 | 100.0 |
| I had dreams about it | 199 | 43.0 | 66 | 14.3 | 46 | 9.9 | 83 | 17.9 | 69 | 14.9 | 463 | 100.0 |
| I felt watchful or on guard | 216 | 47.1 | 55 | 12.0 | 42 | 9.2 | 72 | 15.7 | 74 | 16.1 | 459 | 100.0 |
| I tried not to talk about it | 160 | 34.5 | 67 | 14.4 | 63 | 13.6 | 69 | 14.9 | 105 | 22.6 | 464 | 100.0 |
Note: Totals include only those who responded to each option. Percentages may not total exactly 100.0% due to rounding.
Source: Mothers separated from child by adoption
| Number | Per cent | |
|---|---|---|
| Number of children had in total | ||
| One | 68 | 13.5 |
| Two | 57 | 11.4 |
| Three | 183 | 36.5 |
| Four or more | 194 | 38.6 |
| No. of observations | 502 | 100.0 |
| Number of children separated from by adoption | ||
| One | 475 | 94.1 |
| Two | 25 | 5.0 |
| Three or more | 5 | 1.0 |
| No. of observations | 505 | 100.0 |
| Number of children prior to first adoption | ||
| None | 487 | 96.8 |
| One or more | 16 | 3.2 |
| No. of observations | 503 | 100.0 |
| Number of children not adopted | ||
| None | 74 | 14.7 |
| One | 60 | 12.0 |
| Two | 196 | 39.0 |
| Three or more | 172 | 34.3 |
| No. of observations | 502 | 100.0 |
| To what extent did the adoption experience influence decision/ability to have further children? | ||
| Not at all | 95 | 19.0 |
| A little | 56 | 11.2 |
| Moderately | 71 | 14.2 |
| Mostly | 104 | 20.8 |
| Entirely | 174 | 34.8 |
| No. of observations | 500 | 100.0 |
Note: Table includes only those who responded to each question. Percentages may not total exactly 100.0% due to rounding.
Source: Mothers separated from child by adoption
| Experience of adoption had an effect on: a | Number | Per cent ( n = 505) |
|---|---|---|
| Marriage | 330 | 65.3 |
| Disruption in employment (dismissed, resigned, began in new job, apprenticeship etc.) | 180 | 35.6 |
| Marital separation or divorce | 178 | 35.2 |
| Death of a close family member or friend | 137 | 27.1 |
| Change in residence | 124 | 24.6 |
| Major personal injury or illness | 123 | 24.4 |
| Disruption in schooling (changed schools, ceased formal schooling) | 92 | 18.2 |
| Major financial problems | 89 | 17.6 |
| Outstanding personal achievement | 83 | 16.4 |
| Significant ill health of a family member | 66 | 13.1 |
| Marital reconciliation | 24 | 4.8 |
| Broke the law by committing a major offence and/or spent time in an institution or jail | 10 | 2.0 |
| None of the above | 54 | 10.7 |
Note: a Respondents could choose more than one option.
Source: Mothers separated from child by adoption
B9 Wellbeing
| Physical | Psychological | Social relationships | Environment | Overall rating | Overall health | No. of observations a | |
|---|---|---|---|---|---|---|---|
| Mean scores | |||||||
| All mothers | 52 | 50 | 53 | 67 | 3.6 | 3.1 | 487 |
| Age at time of survey completion | |||||||
| Under 50 years | 52 | 48 | 52 | 61 | 3.6 | 3.2 | 32 |
| 50-54 years | 48 | 45 | 43 | 61 | 3.5 | 2.8 | 49 |
| 55-59 years | 51 | 50 | 52 | 65 | 3.5 | 2.9 | 111 |
| 60-64 years | 53 | 51 | 54 | 71 | 3.7 | 3.3 | 162 |
| 65-69 years | 54 | 51 | 53 | 67 | 3.5 | 3.0 | 103 |
| 70 years and over | 56 | 55 | 66 | 74 | 3.8 | 3.5 | 34 |
| Current marital status | |||||||
| Never married | 45 | 48 | 40 | 58 | 3.2 | 2.7 | 29 |
| De facto/same-sex partner | 55 | 50 | 63 | 72 | 3.7 | 3.2 | 26 |
| Married | 54 | 50 | 59 | 72 | 3.9 | 3.2 | 250 |
| Separated/divorced | 51 | 51 | 46 | 61 | 3.3 | 3.0 | 147 |
| Widowed | 49 | 49 | 48 | 63 | 3.3 | 3.0 | 34 |
| Current employment status | |||||||
| Working full-time | 55 | 49 | 52 | 69 | 3.8 | 3.3 | 100 |
| Working part-time | 55 | 51 | 57 | 73 | 3.9 | 3.3 | 108 |
| Not working | 51 | 50 | 52 | 65 | 3.4 | 2.9 | 274 |
| Highest level of education | |||||||
| Not completed secondary/high school | 51 | 50 | 50 | 64 | 3.3 | 3.0 | 81 |
| Secondary/high school | 51 | 51 | 56 | 68 | 3.7 | 3.2 | 118 |
| Diploma/certificate/trade qualification | 52 | 49 | 52 | 64 | 3.5 | 3.0 | 126 |
| Undergraduate degree | 53 | 50 | 54 | 69 | 3.7 | 3.1 | 43 |
| Graduate qualification | 54 | 52 | 55 | 73 | 3.9 | 3.2 | 55 |
| Postgraduate degree | 55 | 49 | 51 | 71 | 3.8 | 3.2 | 59 |
| Age at time of birth | |||||||
| 15 years and under | 46 | 43 | 45 | 56 | 3.3 | 2.7 | 25 |
| 16-17 years | 51 | 49 | 49 | 62 | 3.3 | 2.8 | 131 |
| 18-19 years | 52 | 50 | 53 | 70 | 3.7 | 3.2 | 176 |
| 20-21 years | 55 | 52 | 59 | 70 | 3.8 | 3.3 | 93 |
| 22 years and over | 54 | 52 | 56 | 71 | 3.7 | 3.2 | 62 |
| Whether given opportunity to see child after birth | |||||||
| Yes | 53 | 50 | 57 | 69 | 3.7 | 3.2 | 201 |
| No | 52 | 51 | 50 | 66 | 3.5 | 3.0 | 269 |
| How satisfied interests looked after in adoption process | |||||||
| Completely/mostly satisfied | 60 | 55 | 69 | 83 | 4.4 | 3.7 | 35 |
| Neither satisfied nor dissatisfied | 59 | 53 | 68 | 79 | 4.2 | 3.8 | 60 |
| Mostly dissatisfied | 54 | 51 | 61 | 74 | 3.9 | 3.2 | 61 |
| Completely dissatisfied | 50 | 49 | 47 | 62 | 3.4 | 2.9 | 329 |
| Whether wanted to keep baby | |||||||
| Yes | 50 | 49 | 48 | 63 | 3.4 | 2.9 | 322 |
| No | 59 | 54 | 70 | 82 | 4.4 | 3.8 | 33 |
| Uncertain | 57 | 51 | 62 | 75 | 4.0 | 3.5 | 124 |
| Whether believe could have kept child with sufficient financial and other support | |||||||
| Yes | 51 | 50 | 51 | 65 | 3.5 | 3.0 | 358 |
| No | 54 | 52 | 61 | 69 | 4.0 | 3.4 | 38 |
| Maybe | 57 | 50 | 59 | 74 | 3.8 | 3.3 | 82 |
| Which of the following best describes adoption experience | |||||||
| I placed my child for adoption | 59 | 53 | 68 | 76 | 4.4 | 3.7 | 19 |
| I lost my child to adoption | 52 | 49 | 52 | 67 | 3.7 | 3.1 | 103 |
| I gave up my child for adoption | 59 | 52 | 65 | 78 | 4.2 | 3.6 | 101 |
| I surrendered my child for adoption | 54 | 53 | 54 | 73 | 3.8 | 3.3 | 57 |
| My child was taken from me | 50 | 47 | 47 | 63 | 3.4 | 2.8 | 74 |
| My child was stolen from me | 47 | 49 | 44 | 57 | 3.0 | 2.6 | 120 |
| Support received at time of birth | |||||||
| Some support | 53 | 50 | 56 | 69 | 3.8 | 3.2 | 273 |
| No support | 52 | 50 | 49 | 65 | 3.4 | 3.0 | 214 |
| Support received since adoption | |||||||
| Some support | 52 | 50 | 54 | 67 | 3.6 | 3.1 | 347 |
| No support | 52 | 51 | 50 | 68 | 3.6 | 3.1 | 144 |
| Best way to describe contact with child | |||||||
| Had contact: | 53 | 50 | 53 | 67 | 3.6 | 3.1 | 414 |
| Have had contact but never met | 56 | 48 | 44 | 68 | 3.7 | 2.9 | 19 |
| Have met but no ongoing relationship | 50 | 51 | 49 | 63 | 3.5 | 3.0 | 87 |
| Ongoing relationship | 54 | 50 | 59 | 71 | 3.8 | 3.3 | 236 |
| No contact | 51 | 49 | 51 | 66 | 3.5 | 3.0 | 69 |
| How often think about child | |||||||
| Always | 50 | 49 | 51 | 63 | 3.4 | 2.9 | 235 |
| Often | 54 | 51 | 56 | 71 | 3.8 | 3.2 | 207 |
| Sometimes | 56 | 53 | 54 | 75 | 3.9 | 3.5 | 28 |
Note: a The number of observations varies across the subscales. The value given is the smallest value it takes.
Source: Mothers separated from child by adoption
| Likely to be well (%) | Likely to have a mild disorder (%) | Likely to have a moderate mental disorder (%) | Likely to have a severe mental disorder (%) | Mean scores | No. of observations a | |
|---|---|---|---|---|---|---|
| All mothers | 38.5 | 15.5 | 15.3 | 30.7 | 24 | 496 |
| Age at time of survey completion | ||||||
| Under 50 years | 27.3 | 15.2 | 18.2 | 39.4 | 27 | 33 |
| 50-54 years | 30.0 | 8.0 | 12.0 | 50.0 | 28 | 50 |
| 55-59 years | 32.7 | 18.5 | 13.9 | 34.5 | 26 | 115 |
| 60-64 years | 43.8 | 15.4 | 17.3 | 23.5 | 23 | 163 |
| 65-69 years | 37.1 | 17.1 | 15.2 | 20.5 | 27 | 109 |
| 70 years and over | 60.6 | 12.1 | 12.1 | 15.2 | 24 | 35 |
| Current marital status | ||||||
| Never married | 25.8 | 19.4 | 22.6 | 32.3 | 26 | 31 |
| De facto/same-sex partner | 36.0 | 24.0 | 8.0 | 32.0 | 26 | 26 |
| Married | 40.9 | 19.1 | 12.8 | 27.2 | 24 | 261 |
| Separated/divorced | 36.1 | 9.5 | 19.7 | 34.7 | 26 | 149 |
| Widowed | 46.9 | 6.3 | 12.5 | 34.4 | 28 | 34 |
| Current employment status | ||||||
| Working full-time | 41.0 | 16.2 | 19.1 | 23.8 | 23 | 105 |
| Working part-time | 46.4 | 16.4 | 14.6 | 22.7 | 22 | 110 |
| Not working | 34.6 | 14.6 | 14.2 | 36.7 | 28 | 284 |
| Highest level of education | ||||||
| Not completed secondary/high school | 31.7 | 15.2 | 13.9 | 39.2 | 30 | 84 |
| Secondary/high school | 40.5 | 17.4 | 15.7 | 26.5 | 24 | 122 |
| Diploma/certificate/trade qualification | 31.8 | 15.1 | 15.9 | 37.3 | 27 | 128 |
| Undergraduate degree | 40.0 | 11.1 | 15.6 | 33.3 | 26 | 46 |
| Graduate qualification | 48.3 | 22.4 | 10.3 | 19.0 | 21 | 58 |
| Postgraduate degree | 45.9 | 11.5 | 19.7 | 23.0 | 23 | 61 |
| Age at time of birth | ||||||
| 15 years and under | 26.9 | 11.5 | 11.5 | 50.0 | 28 | 26 |
| 16-17 years | 32.3 | 12.8 | 12.0 | 42.9 | 27 | 135 |
| 18-19 years | 36.1 | 17.9 | 18.9 | 27.2 | 25 | 184 |
| 20-21 years | 47.4 | 16.8 | 15.8 | 20.0 | 23 | 96 |
| 22 years and over | 50.0 | 14.5 | 12.9 | 22.6 | 24 | 64 |
| Whether given opportunity to see child after birth | ||||||
| Yes | 43.4 | 14.3 | 15.8 | 26.6 | 25 | 209 |
| No | 35.1 | 15.9 | 15.6 | 33.3 | 25 | 276 |
| How satisfied interests looked after in adoption process | ||||||
| Completely/mostly satisfied | 72.2 | 11.1 | 11.1 | 5.6 | 19 | 31 |
| Neither satisfied nor dissatisfied | 76.2 | 9.5 | 4.8 | 9.5 | 17 | 63 |
| Mostly dissatisfied | 42.9 | 27.0 | 14.3 | 15.9 | 21 | 63 |
| Completely dissatisfied | 26.9 | 15.1 | 18.1 | 39.9 | 28 | 339 |
| Whether wanted to keep baby | ||||||
| Yes | 29.9 | 14.8 | 17.5 | 37.8 | 28 | 338 |
| No | 79.4 | 11.8 | 2.9 | 5.9 | 16 | 34 |
| Uncertain | 50.4 | 18.7 | 13.8 | 17.1 | 22 | 125 |
| Whether believe could have kept child with sufficient financial and other support | ||||||
| Yes | 34.2 | 15.7 | 16.5 | 33.6 | 26 | 369 |
| No | 62.5 | 2.5 | 5.0 | 30.0 | 22 | 40 |
| Maybe | 47.6 | 21.4 | 16.7 | 14.3 | 23 | 86 |
| Which of the following best describes adoption experience | ||||||
| I placed my child for adoption | 65.0 | 5.0 | 15.0 | 15.0 | 18 | 20 |
| I lost my child to adoption | 37.5 | 12.5 | 20.2 | 29.8 | 26 | 106 |
| I gave up my child for adoption | 66.7 | 16.2 | 10.5 | 6.7 | 18 | 105 |
| I surrendered my child for adoption | 37.9 | 24.1 | 12.1 | 25.9 | 23 | 58 |
| My child was taken from me | 20.3 | 20.3 | 17.6 | 41.9 | 31 | 78 |
| My child was stolen from me | 18.9 | 13.1 | 15.6 | 52.5 | 31 | 125 |
| Support received at time of birth | ||||||
| Some support | 43.2 | 15.7 | 13.6 | 27.5 | 24 | 284 |
| No support | 32.4 | 15.3 | 17.6 | 34.7 | 27 | 221 |
| Support received since adoption | ||||||
| Some support | 38.4 | 15.5 | 16.1 | 29.9 | 25 | 359 |
| No support | 38.7 | 15.5 | 13.4 | 32.4 | 26 | 146 |
| Best way to describe contact with child | ||||||
| Had contact: | 38.6 | 16.6 | 16.1 | 28.7 | 25 | 431 |
| Have had contact but never met | 26.3 | 10.5 | 15.8 | 47.4 | 27 | 19 |
| Have met but no ongoing relationship | 32.6 | 20.2 | 16.9 | 30.3 | 28 | 93 |
| Ongoing relationship | 45.6 | 15.1 | 18.0 | 21.3 | 24 | 244 |
| No contact | 37.7 | 10.1 | 11.6 | 40.6 | 26 | 69 |
| How often think about child | ||||||
| Always | 31.1 | 15.3 | 13.2 | 40.4 | 28 | 241 |
| Often | 45.8 | 15.1 | 18.9 | 20.3 | 23 | 214 |
| Sometimes | 53.6 | 17.9 | 3.6 | 25.0 | 21 | 28 |
Note: a The number of observations varies across the subscales. The value given is the smallest value it takes.
Source: Mothers separated from child by adoption
| Score of 1-4 a (%) | Score of 5-7 a (%) | Score of 8-10 a (%) | Mean score | No. of observations b | |
|---|---|---|---|---|---|
| All mothers | 24.8 | 41.3 | 33.9 | 6.4 | 496 |
| Age at time of survey completion | |||||
| Under 50 years | 30.3 | 42.4 | 27.3 | 5.6 | 33 |
| 50-54 years | 36.0 | 44.0 | 20.0 | 5.6 | 50 |
| 55-59 years | 27.4 | 41.6 | 31.0 | 5.9 | 113 |
| 60-64 years | 21.5 | 42.3 | 36.2 | 6.3 | 163 |
| 65-69 years | 24.8 | 41.0 | 34.3 | 6.1 | 105 |
| 70 years and over | 9.4 | 31.3 | 59.4 | 7.4 | 32 |
| Current marital status | |||||
| Never married | 38.7 | 45.2 | 16.1 | 4.9 | 31 |
| De facto/same-sex partner | 20.0 | 40.0 | 40.0 | 6.3 | 25 |
| Married | 19.1 | 38.7 | 42.2 | 6.6 | 256 |
| Separated/divorced | 30.9 | 44.3 | 24.8 | 5.6 | 149 |
| Widowed | 32.3 | 41.9 | 25.8 | 5.8 | 31 |
| Current employment status | |||||
| Working full-time | 22.9 | 41.9 | 35.2 | 6.3 | 105 |
| Working part-time | 17.4 | 46.8 | 35.8 | 6.5 | 109 |
| Not working | 29.0 | 38.0 | 33.0 | 5.9 | 276 |
| Highest level of education | |||||
| Not completed secondary/high school | 28.8 | 40.0 | 31.3 | 5.8 | 80 |
| Secondary/high school | 20.2 | 42.0 | 37.8 | 6.3 | 119 |
| Diploma/certificate/ trade qualification | 32.5 | 38.1 | 29.4 | 5.7 | 126 |
| Undergraduate degree | 23.9 | 45.7 | 30.4 | 6.2 | 46 |
| Graduate qualification | 17.2 | 39.7 | 43.1 | 6.6 | 58 |
| Postgraduate degree | 21.3 | 44.3 | 34.4 | 6.3 | 61 |
| Age at time of birth | |||||
| 15 years and under | 30.8 | 46.2 | 23.1 | 5.3 | 26 |
| 16-17 years | 37.6 | 34.6 | 27.8 | 5.5 | 133 |
| 18-19 years | 22.8 | 45 | 32.2 | 6.2 | 180 |
| 20-21 years | 16.0 | 43.6 | 40.4 | 6.6 | 94 |
| 22 years and over | 14.3 | 39.7 | 46.0 | 6.7 | 63 |
| Whether given opportunity to see child after birth | |||||
| Yes | 22.1 | 38.2 | 39.7 | 6.4 | 204 |
| No | 26.6 | 44.0 | 29.5 | 5.9 | 275 |
| How satisfied interests looked after in adoption process | |||||
| Completely/mostly satisfied | 8.1 | 27.0 | 64.9 | 7.8 | 37 |
| Neither satisfied nor dissatisfied | 6.4 | 28.6 | 65.1 | 7.6 | 63 |
| Mostly dissatisfied | 15.9 | 41.3 | 42.9 | 6.7 | 63 |
| Completely dissatisfied | 31.8 | 45.5 | 22.7 | 5.5 | 330 |
| Whether wanted to keep baby | |||||
| Yes | 31.8 | 42.1 | 26.1 | 5.7 | 330 |
| No | 2.9 | 32.4 | 64.7 | 7.6 | 34 |
| Uncertain | 12.1 | 41.1 | 46.8 | 6.8 | 124 |
| Whether believe could have kept child with sufficient financial and other support | |||||
| Yes | 27.9 | 41.7 | 30.4 | 5.9 | 362 |
| No | 22.5 | 25.0 | 52.5 | 6.6 | 40 |
| Maybe | 10.7 | 47.6 | 41.7 | 6.7 | 84 |
| Which of the following best describes adoption experience | |||||
| I placed my child for adoption | 0.0 | 40.0 | 60.0 | 7.7 | 20 |
| I lost my child to adoption | 25.7 | 47.6 | 26.7 | 6.0 | 105 |
| I gave up my child for adoption | 7.6 | 33.3 | 59.1 | 7.4 | 105 |
| I surrendered my child for adoption | 22.4 | 46.6 | 31.0 | 6.2 | 58 |
| My child was taken from me | 22.4 | 51.3 | 26.3 | 5.9 | 76 |
| My child was stolen from me | 47.9 | 34.5 | 17.7 | 4.8 | 119 |
| Support received at time of birth | |||||
| Some support | 21.4 | 40.0 | 38.6 | 6.4 | 280 |
| No support | 29.2 | 43.1 | 27.8 | 5.7 | 216 |
| Support received since adoption | |||||
| Some support | 23.1 | 44.2 | 32.8 | 6.1 | 351 |
| No support | 29.0 | 34.5 | 36.6 | 6.1 | 145 |
| Best way to describe contact with child | |||||
| Had contact: | 24.4 | 41.6 | 34.0 | 6.1 | 423 |
| Have had contact but never met | 21.1 | 68.4 | 10.5 | 5.5 | 19 |
| Have met but no ongoing relationship | 30.8 | 36.3 | 33.0 | 5.7 | 91 |
| Ongoing relationship | 17.6 | 41.0 | 41.4 | 6.6 | 239 |
| No contact | 26.5 | 41.2 | 32.4 | 6.0 | 68 |
| How often think about child | |||||
| Always | 32.1 | 40.6 | 27.4 | 5.7 | 234 |
| Often | 17.3 | 43.5 | 39.3 | 6.5 | 214 |
| Sometimes | 17.9 | 28.6 | 53.6 | 7.0 | 28 |
Note: a Respondents were asked to indicate how satisfied they were with various aspects of their lives and with their life in general, using a rating scale ranging from 1 ("completely dissatisfied") to 10 ("completely satisfied"). This was based on the measurement used in the Household, Income and Labour Dynamics in Australia (HILDA) survey. b The number of observations varies across the subscales. The value given is the smallest value it takes.
Source: Mothers separated from child by adoption
| Few symptoms (%) | Several symptoms (%) | Many symptoms (%) | Mean score | No. of observations a | |
|---|---|---|---|---|---|
| All mothers | 18.8 | 24.7 | 56.5 | 36 | 437 |
| Age at time of survey completion | |||||
| Under 50 years | 18.8 | 18.8 | 62.5 | 41 | 32 |
| 50-54 years | 8.2 | 24.5 | 67.4 | 44 | 49 |
| 55-59 years | 16.0 | 24.5 | 59.4 | 38 | 106 |
| 60-64 years | 22.6 | 26.0 | 51.4 | 33 | 146 |
| 65-69 years | 15.1 | 26.7 | 58.1 | 37 | 86 |
| 70 years and over | 50.0 | 16.7 | 33.3 | 23 | 18 |
| Current marital status | |||||
| Never married | 6.9 | 31.0 | 62.1 | 39 | 29 |
| De facto/same-sex partner | 22.7 | 22.7 | 54.6 | 34 | 22 |
| Married | 18.9 | 26.4 | 54.6 | 35 | 227 |
| Separated/divorced | 20.2 | 19.4 | 60.5 | 39 | 129 |
| Widowed | 22.2 | 29.6 | 48.2 | 34 | 27 |
| Current employment status | |||||
| Working full-time | 22.1 | 21.1 | 56.8 | 34 | 95 |
| Working part-time | 19.1 | 28.6 | 52.4 | 34 | 105 |
| Not working | 17.2 | 24.6 | 58.2 | 38 | 232 |
| Highest level of education | |||||
| Not completed secondary/high school | 10.6 | 30.3 | 59.1 | 39 | 66 |
| Secondary/ high school | 21.0 | 23.0 | 56.0 | 37 | 100 |
| Diploma/certificate/trade qualification | 15.9 | 22.1 | 62.0 | 39 | 113 |
| Undergraduate degree | 26.8 | 29.3 | 43.9 | 30 | 41 |
| Graduate qualification | 27.3 | 30.9 | 41.8 | 28 | 55 |
| Postgraduate degree | 14.0 | 17.5 | 68.4 | 40 | 57 |
| Age at time of birth | |||||
| 15 years and under | 12.5 | 29.2 | 58.3 | 39 | 24 |
| 16-17 years | 9.9 | 26.5 | 63.6 | 42 | 121 |
| 18-19 years | 24.4 | 20.1 | 58.5 | 36 | 159 |
| 20-21 years | 27.5 | 26.3 | 46.3 | 30 | 80 |
| 22 years and over | 20.8 | 30.2 | 49.1 | 33 | 53 |
| Whether given opportunity to see child after birth | |||||
| Yes | 24.9 | 24.9 | 50.3 | 33 | 181 |
| No | 14.9 | 24.1 | 61.0 | 39 | 241 |
| How satisfied interests looked after in adoption process | |||||
| Completely/mostly satisfied | 63.3 | 20.0 | 16.7 | 15 | 30 |
| Neither satisfied nor dissatisfied | 36.8 | 40.4 | 22.8 | 19 | 57 |
| Mostly dissatisfied | 16.1 | 41.1 | 42.9 | 31 | 56 |
| Completely dissatisfied | 11.3 | 19.1 | 69.6 | 43 | 293 |
| Whether wanted to keep baby | |||||
| Yes | 12.5 | 22.8 | 64.7 | 41 | 289 |
| No | 55.2 | 27.6 | 17.2 | 14 | 29 |
| Uncertain | 24.8 | 29.2 | 46.0 | 30 | 113 |
| Whether believe could have kept child with sufficient financial and other support | |||||
| Yes | 13.1 | 25.0 | 61.9 | 40 | 320 |
| No | 50.0 | 20.6 | 29.4 | 23 | 34 |
| Maybe | 29.9 | 27.3 | 42.9 | 27 | 77 |
| Which of the following best describes adoption experience | |||||
| I placed my child for adoption | 66.7 | 11.1 | 22.2 | 13 | 18 |
| I lost my child to adoption | 12.0 | 27.2 | 60.9 | 39 | 92 |
| I gave up my child for adoption | 38.0 | 28.3 | 33.7 | 22 | 92 |
| I surrendered my child for adoption | 20.8 | 41.5 | 37.7 | 29 | 53 |
| My child was taken from me | 7.8 | 21.9 | 70.3 | 43 | 64 |
| My child was stolen from me | 3.8 | 12.3 | 84.0 | 52 | 106 |
| Support received at time of birth | |||||
| Some support | 20.0 | 27.6 | 52.4 | 35 | 250 |
| No support | 17.1 | 20.9 | 62.0 | 39 | 187 |
| Support received since adoption | |||||
| Some support | 18.5 | 22.8 | 58.6 | 37 | 324 |
| No support | 19.5 | 30.1 | 50.4 | 34 | 113 |
| Best way to describe contact with child | |||||
| Had contact: | 20.5 | 24.3 | 55.1 | 36 | 370 |
| Have had contact but never met | 11.8 | 11.8 | 76.5 | 40 | 17 |
| Have met but no ongoing relationship | 9.5 | 33.8 | 56.8 | 40 | 74 |
| Ongoing relationship | 28.9 | 23.2 | 47.9 | 32 | 211 |
| No contact | 7.9 | 27.0 | 65.1 | 41 | 63 |
| How often think about child | |||||
| Always | 11.6 | 22.7 | 65.7 | 43 | 198 |
| Often | 24.0 | 25.0 | 51.0 | 32 | 196 |
| Sometimes | 37.0 | 29.6 | 33.3 | 24 | 27 |
Note: a The number of observations varies across the subscales. The value given is the smallest value it takes.
Source: Mothers separated from child by adoption
Attachment C - Persons who were adopted: Quantitative tables
C1 Details of birth
| Child characteristics | Number | Per cent |
|---|---|---|
| Year of birth | ||
| Prior to 1940 | 23 | 2.8 |
| 1940-49 | 96 | 11.7 |
| 1950-59 | 181 | 22.0 |
| 1960-64 | 117 | 14.2 |
| 1965-69 | 182 | 22.1 |
| 1970-74 | 150 | 18.2 |
| 1975-79 | 42 | 5.1 |
| 1980 onward | 32 | 3.9 |
| No. of observations | 823 | 100.0 |
| Where born | ||
| New South Wales | 243 | 29.6 |
| Victoria | 247 | 30.1 |
| Queensland | 103 | 12.6 |
| South Australia | 107 | 13.0 |
| Western Australia | 47 | 5.7 |
| Tasmania | 22 | 2.7 |
| Northern Territory | 1 | 0.1 |
| Australian Capital Territory | 6 | 0.7 |
| Overseas | 44 | 5.4 |
| No. of observations | 820 | 100.0 |
| Region | ||
| Capital city | 679 | 83.1 |
| Regional centre | 110 | 13.5 |
| Rural area | 28 | 3.4 |
| No. of observations | 817 | 100.0 |
| Place of birth | ||
| Hospital | 662 | 80.4 |
| Maternity home | 77 | 9.4 |
| Children's home | 7 | 0.9 |
| Private home | 7 | 0.9 |
| Church home | 55 | 6.7 |
| Other | 13 | 1.6 |
| Missing data | 2 | 0.2 |
| No. of observations | 823 | 100.0 |
| Whether lived with birth mother or another family member before adopted | ||
| Yes | 84 | 10.7 |
| No | 639 | 81.3 |
| Unknown | 63 | 8.0 |
| No. of observations | 786 | 100.0 |
Note: Totals include only those who responded to each question. Percentages may not total exactly 100.0% due to rounding.
Source: Persons who were adopted
C2 Adoption characteristics
| Adoption characteristics | Number | Per cent |
|---|---|---|
| Age when found out adopted | ||
| Under 1 year | 40 | 4.9 |
| 1-2 years | 100 | 12.2 |
| 3 years | 103 | 12.5 |
| 4 years | 96 | 11.7 |
| 5 years | 118 | 14.3 |
| 6-10 years | 195 | 23.7 |
| 11-20 years | 77 | 9.4 |
| 21-30 years | 31 | 3.8 |
| 31-40 years | 23 | 2.8 |
| 41-50 years | 26 | 3.2 |
| Over 50 years | 12 | 1.5 |
| Missing data | 2 | 0.2 |
| No. of observations | 823 | 100.0 |
| How found out adopted | ||
| My adopted parents told me | 517 | 68.2 |
| Another family member told me | 38 | 5.0 |
| I found out by accident | 62 | 8.2 |
| When my birth family contacted me | 9 | 1.2 |
| I do not recall - told at a young age | 132 | 17.4 |
| No. of observations | 758 | 100.0 |
| Whether aware of reasons placed for adoption | ||
| Yes | 639 | 78.6 |
| No | 174 | 21.4 |
| No. of observations | 813 | 100.0 |
| Whether believe being adopted had effect on health, behaviours or wellbeing while growing up | ||
| Yes | 565 | 68.7 |
| No | 211 | 25.6 |
| Did not know until adult | 47 | 5.7 |
| No. of observations | 823 | 100.0 |
| Number of adoptive siblings in adoptive family | ||
| None | 353 | 43.2 |
| One | 371 | 45.4 |
| Two | 69 | 8.4 |
| Three or more | 25 | 3.1 |
| No. of observations | 818 | 100.0 |
| Whether being an adopted person had effect on decision to have children | ||
| Not at all | 396 | 49.3 |
| A little | 119 | 14.8 |
| Moderately | 80 | 10.0 |
| Mostly | 57 | 7.1 |
| Completely | 151 | 18.8 |
| No. of observations | 803 | 100.0 |
Note: Totals include only those who responded to each question. Percentages may not total exactly 100.0% due to rounding.
Source: Persons who were adopted
C3 Sources of support when growing up
| Sources of support a | Number | Per cent ( n = 823) |
|---|---|---|
| Parents | 274 | 33.3 |
| Other family members | 91 | 11.1 |
| Friends | 100 | 12.2 |
| Social worker or counsellor | 36 | 4.4 |
| Registered psychologist or psychiatrist | 24 | 2.9 |
| GP | 10 | 1.2 |
| Church group | 13 | 1.6 |
| Support group | 10 | 1.2 |
| Adoption service | 29 | 3.5 |
| Did not have any supports | 320 | 38.9 |
| Did not want/need any supports | 114 | 13.9 |
| Other | 71 | 8.6 |
Note: a Respondents could choose more than one option.
Source: Persons who were adopted
| Received support | Very helpful | Somewhat helpful | Not helpful | Unhelpful | Very unhelpful | Missing data | |
|---|---|---|---|---|---|---|---|
| Parents | |||||||
| Emotional support | 207 | 129 | 64 | 9 | 5 | ||
| Medical | 67 | 56 | 5 | 3 | 1 | 2 | |
| Legal | 26 | 19 | 3 | 2 | 2 | ||
| General support and information | 209 | 106 | 84 | 12 | 2 | 4 | 1 |
| Other | 11 | 6 | 2 | 2 | 1 | ||
| Other family members | |||||||
| Emotional support | 82 | 47 | 23 | 4 | 4 | 4 | |
| Medical | 2 | 2 | |||||
| General support and information | 39 | 23 | 14 | 2 | |||
| Other | 3 | 2 | 1 | ||||
| Friends | |||||||
| Emotional support | 91 | 38 | 45 | 4 | 1 | 2 | 1 |
| General support and information | 32 | 16 | 14 | 1 | 1 | ||
| Other | 2 | 1 | 1 | ||||
| Social worker/counsellor | |||||||
| Emotional support | 18 | 9 | 7 | 2 | |||
| Medical | 1 | 1 | |||||
| Financial | 3 | 2 | 1 | ||||
| General support and information | 27 | 6 | 11 | 5 | 2 | 3 | |
| Legal | 2 | 1 | 1 | ||||
| Other | 1 | 1 | |||||
| Registered psychologist or psychiatrist | |||||||
| Emotional support | 17 | 7 | 10 | ||||
| Medical | 11 | 4 | 5 | 1 | 1 | ||
| General support and information | 8 | 2 | 5 | 1 | |||
| Other | 4 | 1 | 1 | 2 | |||
| GP | |||||||
| Emotional support | 5 | 3 | 2 | ||||
| Medical | 7 | 1 | 3 | 1 | 1 | 1 | |
| General support and information | 3 | 2 | 1 | ||||
| Church group | |||||||
| Emotional support | 11 | 5 | 5 | 1 | |||
| General support and information | 6 | 2 | 1 | 1 | 2 | ||
| Other | 1 | 1 | |||||
| Support group | |||||||
| Emotional support | 9 | 4 | 3 | 2 | |||
| General support and information | 4 | 3 | 1 | ||||
| Other | 2 | 1 | 1 | ||||
| An adoption service | |||||||
| Emotional support | 7 | 5 | 1 | 1 | |||
| Legal | 5 | 3 | 2 | ||||
| General support and information | 28 | 14 | 11 | 1 | 2 | ||
| Other | 2 | 1 | 1 | ||||
Source: Persons who were adopted
C4 Seeking information and making contact
| Contact characteristics | Number | Per cent |
|---|---|---|
| Ever tried to find information about birth family | ||
| Yes | 725 | 88.1 |
| No | 98 | 11.9 |
| No. of observations | 823 | 100.0 |
| How adoptive parents reacted when told going to try to find out information a | ||
| They were supportive | 238 | 34.8 |
| They were anxious | 163 | 23.8 |
| They encouraged me | 96 | 14.0 |
| They tried to discourage me | 49 | 7.2 |
| I didn't tell them | 138 | 20.2 |
| Not applicable - my parents had passed away | 93 | 13.6 |
| Other | 146 | 21.3 |
| No. of observations | 684 | 100.0 |
| Whether worried that adoptive parents would think being disloyal | ||
| Yes | 370 | 52.1 |
| No | 253 | 35.6 |
| Not applicable - my parents had passed away | 87 | 12.3 |
| No. of observations | 710 | 100.0 |
| Whether experienced sense of divided loyalty | ||
| Yes | 236 | 37.7 |
| No | 390 | 62.3 |
| No. of observations | 626 | 100.0 |
| Whether ever received identifying information about birth family | ||
| Yes | 659 | 91.3 |
| No | 63 | 8.7 |
| No. of observations | 722 | 100.0 |
| Ever used contact/reunion services | ||
| Yes | 385 | 53.3 |
| No | 285 | 39.5 |
| I would have if had known they exist | 52 | 7.2 |
| No. of observations | 722 | 100.0 |
Note: Totals include only those who responded to each question. a Respondents could choose more than one option. Percentages may not total exactly 100.0% due to rounding.
Source: Persons who were adopted
| Contact characteristics | Number | Per cent |
|---|---|---|
| Whether had contact with birth mother | ||
| Yes | 518 | 62.9 |
| No | 305 | 37.1 |
| No. of observations | 823 | 100.0 |
| Reason for not having contact ( N = 305) | ||
| Mother has died | 85 | 27.9 |
| Have not wanted to establish contact | 49 | 16.1 |
| Have some information about mother but have never met nor had communication | 41 | 13.4 |
| Not been able to find any information about mother | 38 | 12.5 |
| Mother rejected the possibility of contact/relationship | 38 | 12.5 |
| I am not ready to have contact at this time | 23 | 7.5 |
| Believe it is mother's choice to have contact and waiting for contact | 19 | 6.2 |
| There is a veto on contact with mother | 17 | 5.6 |
| Other | 54 | 17.7 |
| Whether want contact in future | ||
| Yes | 22 | 28.6 |
| No | 15 | 19.5 |
| Uncertain | 20 | 26.0 |
| Not applicable | 20 | 26.0 |
| No. of observations | 77 | 100.0 |
| Year when first had contact | ||
| Prior to 1980 | 19 | 3.7 |
| 1980-84 | 29 | 5.7 |
| 1985-89 | 75 | 14.7 |
| 1990-94 | 148 | 29.0 |
| 1995-99 | 76 | 14.9 |
| 2000-04 | 64 | 12.5 |
| 2005-09 | 70 | 13.7 |
| 2010 onwards | 30 | 5.9 |
| No. of observations | 511 | 100.0 |
| Age when first had contact | ||
| Under 18 years | 21 | 4.1 |
| 18-19 years | 45 | 8.8 |
| 20-24 years | 86 | 16.8 |
| 25-29 years | 77 | 15.1 |
| 30-34 years | 78 | 15.3 |
| 35-39 years | 83 | 16.2 |
| 40-44 years | 49 | 9.6 |
| 44-49 years | 30 | 5.9 |
| 50-54 years | 23 | 4.5 |
| 55 years and over | 19 | 3.7 |
| No. of observations | 511 | 100.0 |
| How best to describe contact with birth mother ( N = 439) | ||
| Had contact but never met | 58 | 13.2 |
| Have met, but no ongoing relationship | 146 | 33.3 |
| Have met, have ongoing relationship | 235 | 53.5 |
Note: Totals include only those who responded to each question. Percentages may not total exactly 100.0% due to rounding.
Source: Persons who were adopted
| Contact characteristics | Number | Per cent |
|---|---|---|
| Whether had contact with birth father | ||
| Yes | 210 | 25.5 |
| No | 613 | 74.5 |
| No. of observations | 823 | 100.0 |
| Reason for not having contact | ||
| Not been able to find any information about father | 258 | 42.1 |
| Father has died | 95 | 15.5 |
| Have not wanted to establish contact | 79 | 12.9 |
| Have some information about father but have never met nor had communication | 62 | 10.1 |
| I am not ready to have contact at this time | 27 | 4.4 |
| Father rejected the possibility of contact/relationship | 24 | 3.9 |
| Believe it is father's choice to have contact and waiting for contact | 19 | 3.1 |
| There is a veto on contact with father | 5 | 0.8 |
| Other | 44 | 7.2 |
| No. of observations | 613 | 100.0 |
| Whether want contact in future | ||
| Yes | 23 | 28.0 |
| No | 23 | 28.0 |
| Uncertain | 24 | 29.3 |
| Not applicable | 12 | 14.6 |
| No. of observations | 82 | 100.0 |
| Year when first had contact | ||
| Prior to 1980 | 5 | 2.4 |
| 1980-84 | 13 | 6.3 |
| 1985-89 | 19 | 9.2 |
| 1990-94 | 45 | 21.7 |
| 1995-99 | 37 | 17.9 |
| 2000-04 | 30 | 14.5 |
| 2005-09 | 34 | 16.4 |
| 2010 onwards | 24 | 11.6 |
| No. of observations | 207 | 100.0 |
| Age when first had contact | ||
| Under 18 years | 9 | 4.3 |
| 18-19 years | 19 | 9.2 |
| 20-24 years | 31 | 15.0 |
| 25-29 years | 33 | 15.9 |
| 30-34 years | 33 | 15.9 |
| 35-39 years | 34 | 16.4 |
| 40-44 years | 24 | 11.6 |
| 45-49 years | 12 | 5.8 |
| 50 years and over | 12 | 5.8 |
| No. of observations | 207 | 100.0 |
| How best to describe contact with birth father ( N = 182) | ||
| Had contact but never met | 17 | 9.3 |
| Have met, but no ongoing relationship | 60 | 33.0 |
| Have met, have ongoing relationship | 105 | 57.7 |
Note: Totals include only those who responded to each question. Percentages may not total exactly 100.0% due to rounding.
Source: Persons who were adopted
| Contact characteristics | Number | Per cent |
|---|---|---|
| Whether had contact with other members of birth family | ||
| Yes | 532 | 64.6 |
| No | 291 | 35.4 |
| No. of observations | 823 | 100.0 |
| Reason for not having contact ( N = 291) | ||
| Not been able to find any information about other members of birth family | 81 | 27.8 |
| Have not wanted to establish contact | 61 | 21.0 |
| Have some information about other members of birth family but have never met nor had communication | 26 | 8.9 |
| Believe it is other members of birth family's choice to have contact and waiting for contact | 18 | 6.2 |
| I am not ready to have contact at this time | 17 | 5.8 |
| Other members of birth family rejected the possibility of contact/relationship | 16 | 5.5 |
| There is a veto on contact with other members of birth family | 8 | 2.7 |
| Other members of birth family has died | 1 | 0.3 |
| Other | 50 | 17.2 |
| Whether want contact in future | ||
| Yes | 21 | 26.3 |
| No | 19 | 23.8 |
| Uncertain | 25 | 31.3 |
| Not applicable | 15 | 18.8 |
| No. of observations | 80 | 100.0 |
| Year when first had contact | ||
| Prior to 1980 | 16 | 3.1 |
| 1980-84 | 18 | 3.5 |
| 1985-89 | 65 | 12.6 |
| 1990-94 | 125 | 24.2 |
| 1995-99 | 80 | 15.5 |
| 2000-04 | 70 | 13.5 |
| 2005-09 | 95 | 18.4 |
| 2010 onwards | 48 | 9.3 |
| No. of observations | 517 | 100.0 |
| Age when first had contact | ||
| Under 18 years | 22 | 4.3 |
| 18-19 years | 28 | 5.4 |
| 20-24 years | 59 | 11.4 |
| 25-29 years | 63 | 12.2 |
| 30-34 years | 73 | 14.1 |
| 35-39 years | 96 | 18.6 |
| 40-44 years | 57 | 11.0 |
| 44-49 years | 45 | 8.7 |
| 50-54 years | 30 | 5.8 |
| 55-59 years | 19 | 3.7 |
| 60 years and over | 25 | 4.8 |
| No. of observations | 517 | 100.0 |
| How best to describe contact with other members of birth family | ||
| Had contact but never met | 37 | 7.7 |
| Have met, but no ongoing relationship | 142 | 29.5 |
| Have met, have ongoing relationship | 302 | 62.8 |
| No. of observations | 481 | 100.0 |
Note: Totals include only those who responded to each question. Percentages may not total exactly 100.0% due to rounding.
Source: Persons who were adopted
| Very positive | Positive | No impact | Negative | Very negative | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | N | % | |
| Spouse | 86 | 18.1 | 126 | 26.5 | 188 | 39.6 | 46 | 9.7 | 29 | 6.1 | 475 | 100.0 |
| Own children | 94 | 20.6 | 158 | 34.6 | 155 | 33.9 | 40 | 8.8 | 10 | 2.2 | 457 | 100.0 |
| Adoptive parents | 27 | 6.1 | 93 | 20.9 | 183 | 41.1 | 85 | 19.1 | 57 | 12.8 | 445 | 100.0 |
| Other family | 34 | 6.6 | 116 | 22.6 | 270 | 52.5 | 65 | 12.6 | 29 | 5.6 | 514 | 100.0 |
Note: Table includes only those who responded to the question and for whom the particular family group was applicable. Percentages may not total exactly 100.0% due to rounding.
Source: Persons who were adopted
| Sibling 1 | Sibling 2 | Sibling 3 | Sibling 4 | |
|---|---|---|---|---|
| Much better than my experience | 39 | 8 | 1 | 0 |
| Somewhat better than my experience | 30 | 4 | 3 | 1 |
| About the same as my experience | 33 | 8 | 3 | 2 |
| A bit worse than my experience | 27 | 3 | 1 | 1 |
| Much worse than my experience | 57 | 9 | 4 | 3 |
| Not applicable | 55 | 30 | 16 | 11 |
| Not had contact | 214 | 37 | 10 | 6 |
Source: Persons who were adopted
C5 Quality of relationships and sources of support for adoption
| Very poor | Poor | Neither poor nor good | Good | Very good | NA - parent has died | Totals | |
|---|---|---|---|---|---|---|---|
| Parents - Number | |||||||
| When growing up | 18 | 25 | 21 | 40 | 36 | Not asked | 140 |
| Now | 23 | 15 | 42 | 29 | 31 | Not asked | 140 |
| Parents - Per cent | |||||||
| When growing up | 12.9 | 17.9 | 15.0 | 28.6 | 25.7 | - | 100.0 |
| Now | 16.4 | 10.7 | 30.0 | 20.7 | 22.1 | - | 100.0 |
| Mother - Number | |||||||
| When growing up | 79 | 95 | 103 | 150 | 238 | 18 | 683 |
| Now | 59 | 25 | 56 | 90 | 163 | 290 | 683 |
| Mother - Per cent | |||||||
| When growing up | 11.6 | 13.9 | 15.1 | 22.0 | 34.8 | 2.6 | 100.0 |
| Now (exc. NA) | 15.0 | 6.4 | 14.2 | 22.9 | 41.5 | - | 100.0 |
| Father - Number | |||||||
| When growing up | 53 | 66 | 90 | 176 | 271 | 26 | 682 |
| Now | 49 | 17 | 45 | 83 | 121 | 367 | 682 |
| Father - Per cent | |||||||
| When growing up | 7.8 | 9.7 | 13.2 | 25.8 | 39.7 | 3.8 | 100.0 |
| Now (exc. NA) | 15.6 | 5.4 | 14.3 | 26.3 | 38.4 | - | 100.0 |
Notes: a The first version of this question asked respondents about both parents in the one question; after the instrument was revised, each parent was asked about separately. Percentages may not total exactly 100.0% due to rounding.
Source: Persons who were adopted
| Sources of support a | Number | Per cent ( n = 823) |
|---|---|---|
| Adoptive parents | 160 | 19.4 |
| Birth parents | 111 | 13.5 |
| Other family members | 171 | 20.8 |
| Friends | 266 | 32.3 |
| Social worker or counsellor | 176 | 21.4 |
| Registered psychologist or psychiatrist | 209 | 25.4 |
| Adoption support service | 195 | 23.7 |
| GP | 71 | 8.6 |
| Support group | 106 | 12.9 |
| Church group b | 11 | 1.3 |
| Did not have any supports | 29 | 3.5 |
| Did not want/need any supports | 90 | 10.9 |
| Other | 63 | 7.7 |
Notes: a Respondents could choose more than one source of support. b This was only asked of respondents after the questionnaire was changed.
Source: Persons who were adopted
| Received support | Very helpful | Somewhat helpful | Not helpful | Unhelpful | Very unhelpful | Missing data | |
|---|---|---|---|---|---|---|---|
| Adoptive parents | |||||||
| Emotional support | 132 | 73 | 46 | 5 | 2 | 6 | |
| Family planning advice | 12 | 7 | 4 | 1 | |||
| Financial | 45 | 33 | 9 | 1 | 2 | ||
| Legal | 9 | 5 | 3 | 1 | |||
| Psychotherapy or counselling | 12 | 8 | 2 | 2 | |||
| Other | 19 | 5 | 3 | 2 | 2 | 6 | 1 |
| Birth parents | |||||||
| Emotional support | 84 | 46 | 28 | 3 | 4 | 3 | |
| Family planning advice | 4 | 4 | |||||
| Financial | 6 | 3 | 3 | ||||
| Legal | 2 | 2 | |||||
| Psychotherapy or counselling | 3 | 3 | |||||
| Other | 17 | 5 | 7 | 5 | |||
| Other family members | |||||||
| Emotional support | 143 | 81 | 56 | 3 | 1 | 2 | |
| Family planning advice | 3 | 2 | 1 | ||||
| Financial | 1 | 1 | |||||
| Legal | 1 | 1 | |||||
| Psychotherapy or counselling | 4 | 2 | 2 | ||||
| Other | 18 | 8 | 6 | 2 | 2 | ||
| Friends | |||||||
| Emotional support | 227 | 107 | 112 | 7 | 1 | ||
| Family planning advice | 4 | 2 | 2 | ||||
| Financial | 2 | 1 | 1 | ||||
| Legal | 2 | 1 | 1 | ||||
| Psychotherapy or counselling | 7 | 3 | 3 | 1 | |||
| Other | 12 | 7 | 4 | 1 | |||
| Social worker/counsellor | |||||||
| Emotional support | 106 | 49 | 45 | 8 | 2 | 2 | |
| Family planning advice | 5 | 3 | 1 | 1 | |||
| Financial | 2 | 2 | |||||
| Legal | 6 | 1 | 4 | 1 | |||
| Psychotherapy or counselling | 132 | 48 | 65 | 11 | 4 | 3 | 1 |
| Other | 10 | 5 | 3 | 1 | 1 | ||
| Registered psychologist or psychiatrist | |||||||
| Emotional support | 90 | 46 | 35 | 7 | 1 | 1 | |
| Family planning advice | 3 | 2 | 1 | ||||
| Financial | 2 | 1 | 1 | ||||
| Legal | 2 | 1 | 1 | ||||
| Psychotherapy or counselling | 180 | 73 | 84 | 8 | 8 | 4 | 3 |
| Other | 11 | 3 | 4 | 1 | 2 | 1 | |
| An adoption support service | |||||||
| Emotional support | 133 | 77 | 43 | 5 | 4 | 4 | |
| Legal | 19 | 10 | 6 | 1 | 1 | 1 | |
| Psychotherapy or counselling | 47 | 27 | 18 | 1 | 1 | ||
| Other | 58 | 31 | 16 | 6 | 3 | 2 | |
| GP | |||||||
| Emotional support | 37 | 14 | 16 | 3 | 2 | 2 | |
| Family planning advice | 4 | 3 | 1 | ||||
| Financial | 1 | 1 | |||||
| Legal | 2 | 1 | 1 | ||||
| Psychotherapy or counselling | 27 | 10 | 13 | 1 | 2 | 1 | |
| Other | 19 | 4 | 7 | 2 | 5 | 1 | |
| Support group | |||||||
| Emotional support | 91 | 31 | 19 | 1 | 1 | 3 | 36 |
| Family planning advice | 1 | 1 | |||||
| Legal | 5 | 2 | 3 | ||||
| Psychotherapy or counselling | 10 | 5 | 4 | 1 | |||
| Other | 19 | 11 | 1 | 1 | 6 | ||
| Church group a | |||||||
| Emotional support | 8 | 3 | 5 | ||||
| Psychotherapy or counselling | 2 | 1 | 1 | ||||
| Other | 3 | 2 | 1 | ||||
Note: a This was only asked of respondents after the questionnaire was changed.
Source: Persons who were adopted
| Life events a | Number | Per cent ( n = 823) |
|---|---|---|
| Marriage | 311 | 37.8 |
| Death of a close family member or friend | 199 | 24.2 |
| Marital separation or divorce | 183 | 22.2 |
| Disruption in employment (dismissed, resigned, began in new job, apprenticeship etc.) | 182 | 22.1 |
| Disruption in schooling (changed schools, ceased formal schooling) | 166 | 20.2 |
| Outstanding personal achievement | 155 | 18.8 |
| Major personal injury or illness | 133 | 16.2 |
| Change in residence | 130 | 15.8 |
| Major financial problems | 97 | 11.8 |
| Significant ill health of a family member | 85 | 10.3 |
| Broke the law by committing a major offence and/or spent time in an institution or jail | 22 | 2.7 |
| Marital reconciliation | 18 | 2.2 |
| Other | 137 | 16.6 |
| None of the above | 240 | 29.2 |
Notes: a Respondents could choose more than one life event.
Source: Persons who were adopted
C6 Wellbeing
| Physical | Psychological | Social relationships | Environment | Overall rating | Overall health | No. of observationsa | |
|---|---|---|---|---|---|---|---|
| Mean scores | |||||||
| Australian norms | 80 | 73 | 72 | 75 | 4.3 | 3.6 | 396 |
| SD | 17 | 14 | 19 | 14 | 0.8 | 0.9 | |
| All respondents | 56 | 51 | 59 | 72 | 4.1 | 3.5 | 794 |
| SD | 13 | 9 | 24 | 19 | 1.0 | 1.2 | |
| Age at time of survey completion | |||||||
| Under 35 years | 55 | 49 | 65 | 71 | 4.3 | 3.6 | 51 |
| 35-39 years | 59 | 52 | 64 | 75 | 4.4 | 3.8 | 91 |
| 40-44 years | 54 | 49 | 59 | 71 | 4.1 | 3.4 | 200 |
| 45-49 years | 57 | 51 | 62 | 73 | 4.1 | 3.5 | 133 |
| 50-54 years | 55 | 49 | 52 | 70 | 3.9 | 3.2 | 89 |
| 55-59 years | 55 | 53 | 56 | 72 | 4.0 | 3.4 | 90 |
| 60-64 years | 56 | 53 | 57 | 71 | 3.9 | 3.2 | 63 |
| 75 years and over | 57 | 54 | 64 | 74 | 4.1 | 3.5 | 81 |
| Current marital status | |||||||
| Never married | 53 | 50 | 49 | 67 | 3.7 | 3.1 | 122 |
| De facto/same-sex partner | 57 | 51 | 64 | 74 | 4.3 | 3.7 | 127 |
| Married | 57 | 51 | 64 | 75 | 4.3 | 3.6 | 416 |
| Separated/divorced | 54 | 52 | 49 | 65 | 3.6 | 3.2 | 120 |
| Widowed | 54 | 51 | 65 | 74 | 4.1 | 3.2 | 19 |
| Current employment status | |||||||
| Working full-time | 60 | 52 | 62 | 77 | 4.3 | 3.7 | 324 |
| Working part-time | 57 | 51 | 61 | 73 | 4.2 | 3.6 | 218 |
| Not working | 50 | 50 | 55 | 65 | 3.7 | 3.0 | 252 |
| Highest level of education | |||||||
| Not completed secondary/high school | 46 | 46 | 49 | 58 | 3.6 | 2.9 | 75 |
| Secondary/high school | 56 | 50 | 63 | 72 | 4.2 | 3.5 | 138 |
| Diploma/certificate/trade qualification | 55 | 50 | 58 | 70 | 4.0 | 3.4 | 242 |
| Undergraduate degree | 57 | 51 | 60 | 74 | 4.1 | 3.4 | 95 |
| Graduate qualification | 58 | 52 | 62 | 76 | 4.2 | 3.6 | 88 |
| Postgraduate degree | 59 | 54 | 63 | 78 | 4.3 | 3.7 | 156 |
| Age found out adopted | |||||||
| Under 2 years | 59 | 50 | 64 | 77 | 4.4 | 3.8 | 138 |
| 3-5 years | 56 | 51 | 60 | 73 | 4.1 | 3.5 | 307 |
| 6-10 years | 55 | 50 | 60 | 71 | 4.0 | 3.4 | 188 |
| 11-20 years | 53 | 51 | 56 | 64 | 3.6 | 3.0 | 75 |
| 21 years and over | 54 | 53 | 55 | 70 | 4.0 | 3.4 | 90 |
| Whether had contact with birth mother | |||||||
| No | 56 | 51 | 59 | 72 | 4.1 | 3.4 | 300 |
| Yes | 56 | 51 | 60 | 72 | 4.1 | 3.5 | 517 |
| Whether had contact with birth father | |||||||
| No | 56 | 51 | 61 | 73 | 4.1 | 3.5 | 609 |
| Yes | 54 | 51 | 57 | 70 | 4.0 | 3.5 | 208 |
| Whether had contact with other members of birth family | |||||||
| No | 56 | 50 | 61 | 73 | 4.1 | 3.5 | 289 |
| Yes | 56 | 51 | 59 | 72 | 4.1 | 3.4 | 528 |
| Whether believe being adopted had effect on health, behaviours or wellbeing while growing up | |||||||
| Yes | 53 | 50 | 55 | 69 | 3.9 | 3.3 | 550 |
| No | 62 | 53 | 72 | 81 | 4.6 | 4.0 | 201 |
| Did not know until adult | 56 | 53 | 61 | 73 | 4.1 | 3.4 | 47 |
| Support received when growing up | |||||||
| Some support | 57 | 51 | 64 | 74 | 4.3 | 3.6 | 378 |
| No support | 54 | 51 | 56 | 70 | 3.9 | 3.3 | 420 |
| Support received since adult | |||||||
| Some support | 55 | 50 | 59 | 71 | 4.0 | 3.4 | 571 |
| No support | 58 | 52 | 61 | 75 | 4.2 | 3.6 | 251 |
Note: a The number of observations varies across the subscales. The value given is the smallest value it takes.
Source: Persons who were adopted
| Likely to be well (%) | Likely to have a mild disorder (%) | Likely to have a moderate mental disorder (%) | Likely to have a severe mental disorder (%) | Mean scores | No. of observationsa | |
|---|---|---|---|---|---|---|
| 2001 National Health Survey (age standardised) | ||||||
| Males | 85.6 | 8.3 | 3.1 | 2.7 | - | - |
| Females | 79.6 | 10.6 | 5.5 | 4.4 | - | - |
| All respondents | 54.3 | 17.4 | 10.4 | 17.9 | 21 | 820 |
| Age at time of survey completion | ||||||
| Under 35 years | 53.9 | 13.5 | 11.5 | 21.2 | 21 | 52 |
| 35-39 years | 67.0 | 14.9 | 7.5 | 10.6 | 18 | 94 |
| 40-44 years | 50.8 | 15.9 | 10.0 | 23.4 | 22 | 202 |
| 45-49 years | 56.6 | 18.4 | 8.8 | 16.2 | 21 | 137 |
| 50-54 years | 40.4 | 22.3 | 18.1 | 19.2 | 23 | 92 |
| 55-59 years | 52.1 | 15.6 | 10.4 | 21.9 | 21 | 96 |
| 60-64 years | 50.0 | 25.0 | 11.8 | 13.2 | 20 | 68 |
| 75 years and over | 67.1 | 15.2 | 6.3 | 11.4 | 21 | 82 |
| Current marital status | ||||||
| Never married | 44.4 | 15.7 | 13.0 | 27.0 | 24 | 116 |
| De facto/same-sex partner | 57.4 | 19.4 | 7.0 | 16.3 | 19 | 127 |
| Married | 59.5 | 16.7 | 8.7 | 15.1 | 20 | 427 |
| Separated/divorced | 42.1 | 20.6 | 15.1 | 22.2 | 24 | 128 |
| Widowed | 57.1 | 14.3 | 19.1 | 9.5 | 20 | 21 |
| Current employment status | ||||||
| Working full-time | 60.7 | 15.7 | 11.5 | 12.1 | 19 | 332 |
| Working part-time | 59.0 | 18.1 | 7.9 | 15.0 | 20 | 227 |
| Not working | 42.3 | 18.6 | 10.9 | 28.3 | 24 | 260 |
| Highest level of education | ||||||
| Not completed secondary/high school | 36.0 | 14.7 | 14.7 | 34.7 | 27 | 77 |
| Secondary/high school | 58.0 | 16.8 | 7.7 | 17.5 | 21 | 146 |
| Diploma/certificate/trade qualification | 48.0 | 22.2 | 10.5 | 19.4 | 21 | 248 |
| Undergraduate degree | 51.0 | 22.5 | 9.2 | 17.4 | 20 | 96 |
| Graduate qualification | 61.5 | 13.2 | 13.2 | 12.1 | 19 | 91 |
| Postgraduate degree | 67.1 | 11.2 | 9.9 | 11.8 | 18 | 161 |
| Age found out adopted | ||||||
| Under 2 years | 65.7 | 10.0 | 11.4 | 12.9 | 19 | 140 |
| 3-5 years | 54.4 | 19.6 | 8.5 | 17.4 | 20 | 317 |
| 6-10 years | 50.0 | 19.6 | 10.3 | 20.1 | 22 | 195 |
| 11-20 years | 42.3 | 20.5 | 12.8 | 24.4 | 26 | 79 |
| 21 years and over | 55.4 | 14.1 | 13.0 | 17.4 | 21 | 92 |
| Whether had contact with birth mother | ||||||
| No | 55.3 | 16.6 | 10.9 | 17.2 | 21 | 305 |
| Yes | 53.7 | 18.0 | 10.0 | 18.3 | 21 | 518 |
| Whether had contact with birth father | ||||||
| No | 54.7 | 18.3 | 10.6 | 16.4 | 21 | 613 |
| Yes | 53.1 | 14.8 | 9.6 | 22.5 | 22 | 210 |
| Whether had contact with other members of birth family | ||||||
| No | 56.3 | 14.6 | 12.2 | 17.0 | 21 | 291 |
| Yes | 53.2 | 19.0 | 9.4 | 18.4 | 21 | 532 |
| Whether believe being adopted had effect on health, behaviours or wellbeing while growing up | ||||||
| Yes | 44.8 | 19.2 | 12.8 | 23.3 | 23 | 565 |
| No | 79.1 | 11.9 | 4.8 | 4.3 | 16 | 211 |
| Did not know until adult | 57.5 | 21.3 | 6.4 | 14.9 | 20 | 47 |
| Support received when growing up | ||||||
| Some support | 60.3 | 15.9 | 8.5 | 15.4 | 19 | 389 |
| No support | 48.8 | 18.8 | 12.1 | 20.2 | 23 | 434 |
| Support received since adult | ||||||
| Some support | 50.3 | 18.7 | 10.7 | 20.3 | 22 | 571 |
| No support | 63.5 | 14.5 | 9.6 | 12.5 | 20 | 252 |
Source: Persons who were adopted
| Score of 1-4a (%) | Score of 5-7a (%) | Score of 8-10a (%) | Mean score | No. of observationsb | |
|---|---|---|---|---|---|
| All persons | 16.0 | 34.4 | 49.6 | 6.9 | |
| Age at time of survey completion | |||||
| Under 35 years | 11.5 | 38.5 | 50 | 7.2 | 52 |
| 35-39 years | 7.5 | 35.1 | 57.45 | 7.3 | 92 |
| 40-44 years | 14.4 | 40.1 | 45.54 | 6.8 | 202 |
| 45-49 years | 18.3 | 30.7 | 51.09 | 6.8 | 137 |
| 50-54 years | 23.4 | 31.9 | 44.68 | 6.4 | 92 |
| 55-59 years | 24.0 | 32.3 | 43.75 | 6.5 | 96 |
| 60-64 years | 14.7 | 32.4 | 52.94 | 7.0 | 68 |
| 65 years and over | 12.2 | 30.5 | 57.32 | 7.3 | 82 |
| Current marital status | |||||
| Never married | 30.2 | 33.6 | 36.2 | 6.0 | 116 |
| De facto/same-sex partner | 9.5 | 33.1 | 57.5 | 7.3 | 127 |
| Married | 10.8 | 32.1 | 57.1 | 7.3 | 427 |
| Separated/divorced | 26.6 | 45.3 | 28.1 | 5.9 | 128 |
| Widowed | 9.5 | 38.1 | 52.4 | 7.2 | 21 |
| Current employment status | |||||
| Working full-time | 9.9 | 32.2 | 57.8 | 7.3 | 332 |
| Working part-time | 14.1 | 33.0 | 52.9 | 7.1 | 227 |
| Not working | 25.0 | 38.5 | 36.5 | 6.2 | 260 |
| Highest level of education | |||||
| Not completed secondary/high school | 29.9 | 40.3 | 29.9 | 5.8 | 77 |
| Secondary/high school | 15.8 | 30.1 | 54.1 | 7.1 | 146 |
| Diploma/certificate/trade qualification | 17.7 | 36.3 | 46.0 | 6.7 | 248 |
| Undergraduate degree | 14.6 | 34.4 | 51.0 | 6.9 | 96 |
| Graduate qualification | 7.7 | 40.7 | 51.7 | 7.3 | 91 |
| Postgraduate degree | 11.8 | 29.2 | 59.0 | 7.3 | 161 |
| Age found out adopted | |||||
| Under 2 years | 7.9 | 30.0 | 62.1 | 7.4 | 140 |
| 3-5 years | 17.4 | 29.7 | 53.0 | 7.0 | 317 |
| 6-10 years | 15.9 | 40.5 | 43.6 | 6.7 | 195 |
| 11-20 years | 22.3 | 43.0 | 36.7 | 6.3 | 79 |
| 21 years and over | 18.5 | 38.0 | 43.5 | 6.6 | 92 |
| Whether had contact with birth mother | |||||
| No | 16.4 | 34.1 | 49.5 | 6.8 | 305 |
| Yes | 15.8 | 34.7 | 36.7 | 6.3 | 518 |
| Whether had contact with birth father | |||||
| No | 15.0 | 33.9 | 51.1 | 6.9 | 613 |
| Yes | 18.1 | 36.2 | 45.7 | 6.7 | 210 |
| Whether had contact with other members of birth family | |||||
| No | 15.1 | 33.0 | 51.9 | 6.9 | 291 |
| Yes | 16.5 | 35.2 | 48.3 | 6.8 | 532 |
| Whether believe being adopted had effect on health, behaviours or wellbeing while growing up | |||||
| Yes | 20.4 | 40.0 | 39.7 | 6.4 | 565 |
| No | 4.3 | 20.38 | 75.36 | 8.0 | 211 |
| Did not know until adult | 12.8 | 31.91 | 55.32 | 7.1 | 47 |
| Support received when growing up | |||||
| Some support | 10.8 | 32.9 | 56.2 | 7.3 | 389 |
| No support | 20.5 | 35.9 | 43.7 | 6.5 | 435 |
| Support received since adult | |||||
| Some support | 17.0 | 37.1 | 45.9 | 6.8 | 571 |
| No support | 13.1 | 28.6 | 58.3 | 7.1 | 252 |
Note: a Respondents were asked to indicate how satisfied they were with various aspects of their lives and with their life in general, using a rating scale ranging from 0 ("completely dissatisfied") to 10 ("completely satisfied"). This was based on the measurement used in the Household, Income and Labour Dynamics in Australia (HILDA) survey. b The number of observations varies across the subscales. The value of N given is the smallest value it takes.
Source: Persons who were adopted
Attachment D - Adoptive parents: Quantitative tables
D1 Details of adoption
| Details of adoption | Number |
|---|---|
| Year of child's birth | |
| 1950-59 | 7 |
| 1960-64 | 12 |
| 1965-69 | 28 |
| 1970-74 | 29 |
| 1975-79 | 7 |
| 1980 and later | 11 |
| No. of observations | 94 |
| Year of child's adoption | |
| 1950-59 | 6 |
| 1960-64 | 11 |
| 1965-69 | 28 |
| 1970-74 | 27 |
| 1975-79 | 10 |
| 1980 and later | 12 |
| No. of observations | 94 |
| Age child when adopted | |
| 1-2 weeks | 19 |
| 3-5 weeks | 14 |
| 6 weeks | 19 |
| 7-9 weeks | 11 |
| 10-13 weeks | 10 |
| 4-6 months | 8 |
| 9-10 months | 6 |
| 4 years and over | 4 |
| Missing data | 3 |
| No. of observations | 94 |
| Where lived when child adopted | |
| New South Wales | 23 |
| Victoria | 34 |
| Queensland | 9 |
| South Australia | 9 |
| Western Australia | 7 |
| Tasmania | 1 |
| Northern Territory | 1 |
| Australian Capital Territory | 5 |
| Overseas | 5 |
| No. of observations | 94 |
| Whether child related to adoptive parents | |
| No | 92 |
| Yes | 1 |
| Missing data | 1 |
| No. of observations | 94 |
| Main reason for adoption | |
| Unable to conceive | 70 |
| An unmarried relative was pregnant and decided to adopt child | 1 |
| Suffered a miscarriage/stillbirth and hospital arranged for adoption while was a patient | 3 |
| Preference to adopt | 13 |
| Other | 7 |
| No. of observations | 94 |
| Number of children adopted | |
| One | 40 |
| Two | 44 |
| Three | 9 |
| Four | 1 |
| No. of observations | 94 |
Source: Adoptive parents
D2 Support at time of adoption
| Sources of support a | Number |
|---|---|
| Parents | 28 |
| Other family members | 16 |
| Spouse | 58 |
| Friends | 33 |
| Social worker or counsellor | 27 |
| Registered psychologist or psychiatrist | 1 |
| GP | 15 |
| Church group | 14 |
| Support group | 1 |
| Other | 7 |
| Did not have any supports | 9 |
| Did not want/need any supports | 13 |
Notes: a Respondents could choose more than one life event.
Source: Adoptive parents
| Received support | Very helpful | Somewhat helpful | Not helpful | Unhelpful | Very unhelpful | Missing | |
|---|---|---|---|---|---|---|---|
| Parents | |||||||
| Emotional support | 26 | 17 | 8 | 1 | |||
| Family planning advice | 1 | 1 | |||||
| Financial | 2 | 1 | 1 | ||||
| Legal | 1 | 1 | |||||
| Psychotherapy or counselling | 2 | 1 | 1 | ||||
| Other | 1 | 1 | |||||
| Other family members | |||||||
| Emotional support | 16 | 12 | 2 | 2 | |||
| Financial | 1 | 1 | |||||
| Psychotherapy or counselling | 1 | 1 | |||||
| Other | 1 | 1 | |||||
| Spouse | |||||||
| Emotional support | 55 | 46 | 5 | 1 | 3 | ||
| Family planning advice | 4 | 3 | 1 | ||||
| Financial | 20 | 14 | 3 | 1 | 2 | ||
| Legal | 7 | 5 | 1 | 1 | |||
| Psychotherapy or counselling | 3 | 1 | 1 | 1 | |||
| Other | 2 | 2 | |||||
| Friends | |||||||
| Emotional support | 32 | 21 | 9 | 2 | |||
| Financial | 1 | 1 | |||||
| Legal | 1 | 1 | |||||
| Psychotherapy or counselling | 1 | 1 | |||||
| Other | 1 | 1 | |||||
| Social worker/counsellor | |||||||
| Emotional support | 12 | 8 | 3 | 1 | |||
| Family planning advice | 5 | 2 | 1 | 2 | |||
| Financial | 2 | 2 | |||||
| Legal | 7 | 6 | 1 | ||||
| Psychotherapy or counselling | 8 | 2 | 5 | 1 | |||
| Other | 10 | 7 | 3 | ||||
| Registered psychologist or psychiatrist | |||||||
| Psychotherapy or counselling | 1 | 1 | |||||
| Other | 1 | 1 | |||||
| GP | |||||||
| Emotional support | 9 | 5 | 4 | ||||
| Family planning advice | 4 | 3 | 1 | ||||
| Financial | 1 | 1 | |||||
| Legal | 2 | 1 | 1 | ||||
| Other | 5 | 4 | 1 | ||||
| Church group | |||||||
| Emotional support | 11 | 7 | 3 | 1 | |||
| Family planning advice | 4 | 2 | 1 | 1 | |||
| Financial | 2 | 1 | 1 | ||||
| Legal | 3 | 2 | 1 | ||||
| Psychotherapy or counselling | 2 | 1 | 1 | ||||
| Other | 4 | 3 | 1 | ||||
| Support group | |||||||
| Emotional support | 1 | 1 | |||||
Source: Adoptive parents
D3 Adoption process
| Number | |
|---|---|
| Adoption organised through: a | |
| Institution: | |
| Hospital | 17 |
| Church | 22 |
| Government adoption agency | 49 |
| Maternity home | 5 |
| Home for children/ward of the state | 4 |
| Private: | |
| Family lawyer | 3 |
| Private adoption agency | 6 |
| Individual: | |
| Social worker | 10 |
| Priest | 1 |
| Family friend | 3 |
| Other | 11 |
| No. of observations | 131 |
| Overall satisfaction with adoption process | |
| Completely satisfied | 47 |
| Mostly satisfied | 31 |
| Neither satisfied nor dissatisfied | 10 |
| Mostly dissatisfied | 4 |
| Completely dissatisfied | 2 |
| No. of observations | 94 |
| Whether experienced any problems during adoption process | |
| Yes | 20 |
| No | 74 |
| No. of observations | 94 |
| Whether believe being adopted had effect on son/daughter's health, behaviours or wellbeing while growing up | |
| Yes | 44 |
| No | 50 |
| No. of observations | 94 |
Note: a Respondents could choose more than one option.
Source: Adoptive parents
D4 Seeking information and contact
| Number | |
|---|---|
| When told son/daughter they were adopted | |
| Before started school | 70 |
| When in primary school | 6 |
| When independent adult | 1 |
| Told by someone else | 1 |
| Other | 12 |
| No. of observations | 90 |
| Whether son/daughter tried to find information about family | |
| No | 29 |
| Yes: | 65 |
| Son/daughter used contact/reunion services | 36 |
| Son/daughter did not use contact/reunion services | 20 |
| Don't know | 9 |
| No. of observations | 94 |
| Whether adoptive parents had involvement with reunion services at this time | |
| No | 28 |
| Yes: | 6 |
| Reunion service provided support about how adoptive parents might feel about the contact: | 2 |
| The information/support was very helpful | 1 |
| The information/support was somewhat helpful | 1 |
| Reunion service did not provide support about how adoptive parents might feel about the contact | 4 |
| No. of observations | 34 |
| Has son/daughter had contact with members of birth family | |
| Don't know | 3 |
| Yes | 55 |
| No, because: | 34 |
| Son/daughter has not wanted contact | 19 |
| Son/daughter has not been able to find any information | 4 |
| Son/daughter has some information but has never met or communicated | 7 |
| Son/daughter has a veto on being contacted | 1 |
| Birth family has veto on being contacted | 2 |
| Son/daughter not ready to have contact | 3 |
| Son/daughter has passed away | 4 |
| No. of observations | 92 |
| Year when first had contact | |
| Prior to 1980 | 1 |
| 1980-84 | 7 |
| 1985-89 | 18 |
| 1990-94 | 10 |
| 1995-99 | 6 |
| 2000-04 | 4 |
| 2004 and later | 5 |
| No. of observations | 51 |
| Age when first had contact | |
| Under 18 years | 10 |
| 18-19 years | 5 |
| 20-24 years | 20 |
| 25-29 years | 5 |
| 30-34 years | 9 |
| 35-39 years | 2 |
| No. of observations | 51 |
| How best to describe contact with birth family | |
| Had contact but never met | 3 |
| Have met, but no ongoing relationship | 17 |
| Have met, have ongoing relationship | 26 |
| Other | 1 |
| Missing data | 8 |
| No. of observations | 55 |
Source: Adoptive parents
| Very positive | Positive | No impact | Negative | Very negative | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | N | % | |
| Adoptive parents | 18 | 36.0 | 7 | 14.0 | 16 | 32.0 | 7 | 14.0 | 2 | 4.0 | 50 | 100.0 |
| Their children | 6 | 20.0 | 12 | 40.0 | 9 | 30.0 | 3 | 10.0 | 0 | 0.0 | 30 | 100.0 |
| Their spouse | 10 | 37.0 | 4 | 14.8 | 10 | 37.0 | 1 | 3.7 | 2 | 7.4 | 27 | 100.0 |
| Adoptive family members | 7 | 17.1 | 9 | 22.0 | 20 | 48.8 | 4 | 9.8 | 1 | 2.4 | 41 | 100.0 |
Note: Table includes only those who responded to the question and for whom the particular family group was applicable.
Source: Adoptive parents
| Yes | No | Don't know | No. of observations | |
|---|---|---|---|---|
| Second child | 31 | 19 | 3 | 53 |
| Third child | 9 | 1 | 1 | 11 |
| Fourth child | 2 | 1 | 3 |
Source: Adoptive parents
D5 Support during years since adoption
| Source of support a | Number |
|---|---|
| Spouse | 27 |
| Friends | 24 |
| Parents | 12 |
| Other family members | 12 |
| Church group | 11 |
| Social worker or counsellor | 9 |
| Registered psychologist or psychiatrist | 7 |
| GP | 7 |
| Support group | 5 |
| Other | 7 |
| Did not have any supports | 17 |
| Did not want/need any supports | 30 |
Note: a Respondents could choose more than one option.
Source: Adoptive parents
| Received support | Very helpful | Somewhat helpful | Not helpful | Unhelpful | Very unhelpful | Missing data | |
|---|---|---|---|---|---|---|---|
| Parents | |||||||
| Emotional support | 12 | 8 | 4 | ||||
| Financial | 1 | 1 | |||||
| Other family members | |||||||
| Emotional support | 9 | 6 | 3 | ||||
| Other | 1 | 1 | |||||
| Spouse | |||||||
| Emotional support | 27 | 23 | 4 | ||||
| Financial | 7 | 6 | 1 | ||||
| Legal | 1 | 1 | |||||
| Psychotherapy or counselling | 1 | 1 | |||||
| Other | 3 | 3 | |||||
| Friends | |||||||
| Emotional support | 23 | 14 | 8 | 1 | |||
| Psychotherapy or counselling | 2 | 2 | |||||
| Other | 11 a | ||||||
| Social worker/counsellor | |||||||
| Emotional support | 6 | 2 | 2 | 1 | 1 | ||
| Financial | 1 | 1 | |||||
| Legal | 1 | 1 | |||||
| Psychotherapy or counselling | 2 | 1 | 1 | ||||
| Other | 1 | 1 | |||||
| Registered psychologist or psychiatrist | |||||||
| Emotional support | 1 | 1 | |||||
| Psychotherapy or counselling | 4 | 2 | 2 | ||||
| Other | 2 | 2 | |||||
| GP | |||||||
| Emotional support | 4 | 2 | 2 | ||||
| Psychotherapy or counselling | 1 | 1 | |||||
| Other | 3 | 2 | 1 | ||||
| Church group | |||||||
| Emotional support | 9 | 6 | 2 | 1 | |||
| Financial | 1 | 1 | |||||
| Legal | 1 | 1 | |||||
| Other | 4 | 1 | 2 | 1 | |||
| Support group | |||||||
| Emotional support | 3 | 2 | 1 | ||||
| Other | 2 | 2 | |||||
Note: a Information regarding levels of helpfulness were not provided in this response.
Source: Adoptive parents
Lists of tables and figures
List of tables
- Table 3.1 Quantitative survey response, by respondent and survey type
- Table 3.2 Hard-copy survey distribution and response, by respondent type and distributor
- Table 3.3 How survey respondents found out about the study, by information source and respondent type
- Table 3.4 Whether survey respondents were involved with adoption support organisation, by type of involvement and respondent type
- Table 3.5 Characteristics of mothers separated from child by adoption
- Table 3.6 Characteristics of persons who were adopted
- Table 3.7 Characteristics of adoptive parents
- Table 4.1 Focus group locations and numbers
- Table 5.1: Reasons mother thought they were treated less well than other mothers
- Table 5.2: Quality of life scores of survey respondents compared to Australian norms, by domain, WHOQOL-BREF
- Table 5.3: Mental health of respondents compared to female National Health Survey respondents, by likelihood of having a mental disorder, K10
- Table 6.1: Effects of contact with son/daughter on other relationships
- Table 7.1: Quality of life scores of study adoptees compared to Australian norms, by domain, WHOQOL-BREF
- Table 7.2: Mental health of study adoptees compared to National Health Survey respondents, by likelihood of having a mental disorder, K10
- Table 7.3: Life satisfaction scores of study adoptees compared with HILDA respondents
- Table 9.1: Relationship of family member to person affected by past adoption practices
- Table 9.2: Search and contact activities
- Table 9.3: Effect of contact with birth relative on other relationships
- Table 9.4: Type of support by how helpful it was for each source of support
- Table B1: Child's characteristics
- Table B2: Mother's characteristics at time of child's birth
- Table B3: Treatment of mother at birth of child
- Table B4: Reasons mothers thought they were treated with less care than other mothers
- Table B5: What mother was told at time of birth
- Table B6: How mother separated by adoption found information given at time of birth to be untrue
- Table B7: Contact between mother and child at time of child's birth
- Table B8: Type of contact between mother and child at time of child's birth
- Table B9: Advice given to mothers about adoption and the consent process
- Table B10: Adoption process for mothers separated from child by adoption
- Table B11: Sources of support for mother around time of pregnancy and birth
- Table B12: Types and helpfulness of support given to mother at time of birth
- Table B13: Mothers separated from child by adoption searching for and making contact with child
- Table B14: First and ongoing contact between child and mother separated by adoption
- Table B15: How contact between child and mother separated by adoption has affected relationships with other people
- Table B16: Sources of support for mother since separation from child
- Table B17: Types and helpfulness of support given to mother since separation from child
- Table B18: How often mother separated by adoption thinks/thought about child
- Table B19: Times or events that are especially hard for mother separated by adoption
- Table B20: Effects of times or events on mother
- Table B21: Other children had by mother
- Table B22: The effects of mother's adoption experiences on particular life events
- Table B23: Health and wellbeing of mothers separated from child by adoption, by mother characteristics and World Health Organization Quality of Life measures
- Table B24: Mental health of mothers separated from child by adoption, by mother characteristics and Kessler Psychological Distress Scale (K10) measures
- Table B25: Life satisfaction of mothers separated from child by adoption, by mother characteristics and HILDA life satisfaction scores
- Table B26: Effects of events on mothers separated from child by adoption, by mother characteristics and number of symptoms of PTSD
- Table C1: Child characteristics of persons who were adopted
- Table C2: Adoption characteristics of persons who were adopted
- Table C3: Sources of support when adopted person was growing up
- Table C4: Types and helpfulness of support given to adopted person when growing up
- Table C5: Effect on adoptive parents of adopted person making contact with birth family
- Table C6: Adopted person making contact with birth mother
- Table C7: Adopted person making contact with birth father
- Table C8: Adopted person making contact with other members of birth family
- Table C9: How contact between adopted person and birth family has affected relationship with other people
- Table C10: Adoptive person's experience of reunion compared with those of adoptive siblings
- Table C11: Quality of relationship between adopted person and their adoptive parents
- Table C12: Sources of support for adopted person's experience of adoption
- Table C13: Types and helpfulness of support given to adopted person for experience of adoption
- Table C14: Whether experiences of adoption had an effect on adopted person's experience of life events
- Table C15: Health and wellbeing of persons who were adopted, by characteristics and World Health Organization Quality of Life measures
- Table C16: Mental health of persons who were adopted, by characteristics and Kessler Psychological Distress Scale (K10) measures
- Table C17: Life satisfaction of persons who were adopted, by characteristics and HILDA life satisfaction scores
- Table D1: Details of adoption by adoptive parents
- Table D2: Sources of support for adoptive parents around time of adoption
- Table D3: Types and helpfulness of support given to adoptive parents at time of adoption
- Table D4: Adoption process for adoptive parents
- Table D5: Role of adoptive parents in adoptive son/daughter seeking information and contact
- Table D6: How contact with birth family has affected son/daughter's relationship with other people, adoptive parents reports
- Table D7: Whether other adopted children of adoptive parents have had contact with birth family
- Table D8: Sources of support for adoptive parents since adoption
- Table D9: Types and helpfulness of support given to adoptive parents at time of adoption
List of figures
- Figure 2.1: Number of adoptions in Australia from 1968-69 to 2010-11
- Figure 2.2: Number of adoptions in Australia from 1951-52 to 1984-85
- Figure 5.1: Number of adoptions in Australia and trends based on study respondents, 1950 to 1993
- Figure 5.2: Sources and levels of helpfulness of support given to mothers at time of birth
- Figure 5.3: Sources and levels of helpfulness of support given to mothers since separation from child
- Figure 7.1: Distribution of adopted respondents, by year of birth
- Figure 7.2: Age when adoptees found out they had been adopted
- Figure 7.3: Sources of support when adoptee was growing up
- Figure 7.4: Whether adoption experience affected adoptees' experience of life events
- Figure 7.5: Age of adopted person when first had contact with birth family, by mothers, fathers and other family members
- Figure 7.6: Effects of contact with birth family on other family members
- Figure 7.7: Sources of support received by adoptees as adults, by type of support
- Figure 8.1: Year of birth of adopted child, by gender
- Figure 8.2: Age of child when adopted
- Figure 8.3: Place of residents at time of adoption
- Figure 8.4: Sources of support given to adoptive parents at the time of adoption
- Figure 8.5: Emotional support provided to adoptive parents at time of adoption
- Figure 8.6: Age of son/daughter at first contact with family of origin
- Figure 8.7: Effect of contact with family of origin on son/daughters' relationships
- Figure 8.8: Sources and helpfulness of support given to adoptive parents at time of adoption
- Figure 10.1: Responses to service provider surveys, Phases 1 and 2
- Figure 10.2: Age distribution and gender of general service provider survey respondents
- Figure 10.3: Postgraduate qualifications of general service provider survey respondents
- Figure 10.4: Types of services provided and years of working experience of general service provider survey respondents
- Figure 10.5: Clients' level of awareness of services available
Pauline Kenny was a Research Fellow at the Australian Institute of Family Studies, Daryl Higgins was Deputy Director (Research) at the Australian Institute of Family Studies, Carol Soloff was a Senior Research Fellow at the Australian Institute of Family Studies, and Reem Sweid was a Research Officer at the Australian Institute of Family Studies at the time of writing.
The research team wish to acknowledge the following individuals and groups, without whom this study would not have been possible:
- Community and Disability Services Ministers' Conference (CDSMC) and the Department of Families, Housing Community Services and Indigenous Affairs (FaHCSIA) for commissioning the research;
- the technical and stakeholder advisory groups who continued to keep in touch with us over the course of the project to keep us up to speed on current issues/activities and who went above and beyond what is considered a reasonable level of contribution;
- the organisations that gave us the use of their facilities for free to conduct focus groups and interviews across the country;
- organisations who posted out survey forms for us; and
- colleagues from AIFS who assisted with communications for the study, particularly Margaret O'Shannessy, Alister Lamont, Lan Wang and Lauren Di Salvia.
But above all, our thanks and gratitude go to the participants of this study. The authors would like to acknowledge all the people who responded to the survey. We would particularly like to thank the large number of people who gave their time and energy to attend the focus group discussions around the country; for meeting with us in unconventional locations; for being open to sharing their stories with other participants and listening respectfully to perspectives that may not have been in line with their own; and, most especially, for opening their lives and hearts to us. We are more than understanding of the huge effect that even just participating has had on some people, and for this, we thank you. You have allowed us to come on a little bit of the journey with you, and this has been an absolute privilege. We hope we have been able to do your stories justice and that you will be satisfied that your participation has been worth it.
This work was commissioned and funded by the Australian Government Department of Families, Housing, Community Services and Indigenous Affairs. Views expressed in this publication are those of individual authors and may not reflect those of the Australian Government or the Australian Institute of Family Studies.
Kenny, P., Higgins, D., Soloff, C., & Sweid, R. (2012). Past adoption experiences: National Research Study on the Service Response to Past Adoption Practices (Research Report No. 21). Melbourne: Australian Institute of Family Studies.
978-1-922038-05-0