Elder abuse
Key issues and emerging evidence
June 2019
Adam Dean
Download Policy and practice paper
Summary
Elder abuse is a multifaceted and often hidden form of abuse. There is currently no national data on the prevalence of elder abuse in Australia. Based on international studies, it is estimated that between 2% and 14% of older people in high- or middle-income countries experience elder abuse every year. The term 'elder abuse' covers a range of harmful behaviours, including physical, emotional, sexual and financial abuse and neglect.
This paper provides an overview of elder abuse in Australia. It discusses key issues involved in how elder abuse is defined and examines its prevalence, impact and associated risk factors, with a focus on implications of recent research for policy and practice.
Key messages
-
Elder abuse is a complex phenomenon that takes many forms, including physical, psychological, sexual and financial abuse and neglect.
-
An estimated 2-14% of older people in high- or middle-income countries are victims of abuse or neglect every year. Prevalence rates are likely to be much higher in institutional care settings than in community settings.
-
A range of factors associated with older people, perpetrators, relationships and broader contextual factors contribute to older people's risk of abuse and neglect. Emerging evidence suggests that social isolation and poor quality relationships are among the main risk factors associated with elder abuse in community settings.
-
Social support and healthy relationships with family members are key protective factors for older people at risk of abuse or neglect.
-
Research and evaluation on specific prevention and intervention strategies are needed to give a clearer understanding of what works to protect and promote the dignity of older Australians.
Introduction
Elder abuse1 is a multifaceted and often hidden form of abuse. Based on international prevalence data, between 2-14% of older people in high- or middle-income countries are likely to be victims of abuse or neglect every year (Kaspiew, Carson, & Rhoades, 2016). This rate is likely to be higher for older people with disability and those living in institutional care settings (Yon, Ramiro-Gonzalez, Mikton, Huber, & Sethi, 2018). The term 'elder abuse' covers a range of harmful behaviours, including physical, emotional, sexual and financial abuse and neglect.
While not a new phenomenon, the abuse of older adults has gained increasing recognition in Australia in recent years. Several recent public inquiries2 - including the inquiry into Protecting the Rights of Older Australians from Abuse conducted by the Australian Law Reform Commission (ALRC; 2017) - have helped raise awareness of elder abuse in the community and highlighted the need to develop comprehensive and coordinated approaches to address it.
This paper provides an overview of elder abuse in Australia with a focus on the implications of recent research for policy and practice. It reviews recent theoretical literature to explore what it is and how it is defined, and draws on recent empirical research to examine its prevalence in community and institutional care settings, its impact and associated risk factors. The paper also summarises current initiatives and policy frameworks that aim to prevent and address elder abuse, and explores the emerging evidence for effective or promising practices that respond to the needs of older adults at risk of abuse. The paper concludes with future directions for research, policy and practice.
1 The term elder abuse is used throughout the paper to refer to the abuse or neglect of older people. However, it should be noted that in some Aboriginal and Torres Strait Islander communities the term 'elder' is a title reserved for community leaders (Office of the Public Advocate, 2005). The 'abuse or neglect of older people' is a preferred term when used in reference to older Aboriginal and/or Torres Strait Islander peoples.
2 Recent public inquiries that have focused, or have included a focus, on elder abuse have been conducted in New South Wales (Inquiry into Elder Abuse NSW), South Australia (Joint Committee on Matters Relating to Elder Abuse), Victoria (Royal Commission into Family Violence) and Western Australia (Inquiry into Elder Abuse). At the time of writing, a Royal Commission into Aged Care Quality and Safety has been established with a final report due by 30 April 2020.
Older people in Australia
In Australia, older people are generally defined as aged 65 years or older (Australian Bureau of Statistics [ABS], 2016b), though some definitions of elder abuse define older people as aged 60 years and older (Kaspiew et al., 2016).3 For Aboriginal and Torres Strait Islander peoples, who have a lower life expectancy than non-Indigenous Australians, older people are typically defined as 45-50 years and older (Kaspiew et al., 2016).
In 2017, an estimated 3.8 million people were aged 65 years or older in Australia. In 2016, an estimated 124,000 Indigenous Australians were aged 50 and over (Australian Institute of Health and Welfare [AIHW], 2019).
Life expectancy and an ageing population
The proportion of people aged 65 and over has grown steadily over the last century from 5% in 1926 to 15% in 2016, and is projected to rise to 22% by 2056 (Figure 1; AIHW, 2017b). Following this trend, people aged 85 years and older represented 2% of the population in 2017 and are predicted to increase to 4.4% in 2057 (AIHW, 2017a).
Life expectancies for people born in Australia during 2014-16 were 80.4 years for males and 84.6 years for females. In the same period, people aged 65 years could expect to live longer than the average life expectancy; males had an expected age at death of 84.6 years and females had an expected age at death of 87.3 years. For Aboriginal and Torres Strait Islander peoples born between 2015-17, life expectancies were approximately eight or nine years lower than non-Indigenous Australians: 71.6 years for Indigenous males and 75.6 years for Indigenous females (Department of the Prime Minister and Cabinet, 2019).
Figure 1: Australia's ageing population: Proportion of Australian population aged 65 years and older (%)
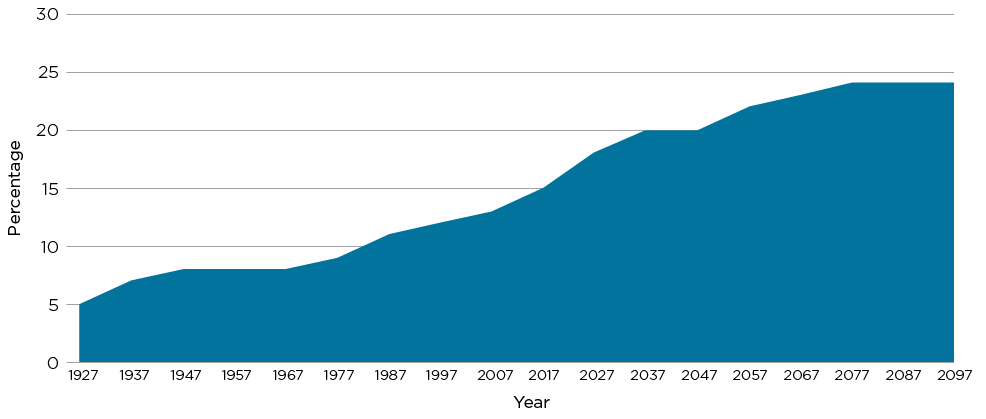
Source: AIHW (2017b)
Box 1: Australia's ageing population and elder abuse
It is hard to talk about elder abuse in Australia in its broader context without reference to Australia's ageing population. As the proportion of people aged 65 years and over increases over time, the overall population of older people vulnerable to abuse is expected to increase with it.
This observation can be double-edged. On the one hand, an ageing population raises important issues relating to workforce participation, its impact on economic outcomes and the provision of social support and other services that respond to the diverse needs of older Australians, including the costs associated with their care and protection (Productivity Commission, 2013). On the other hand, this focus can exacerbate existing intergenerational conflicts and further contribute to ageist attitudes that view older people as a burden to society (Dow & Joosten, 2012; Harbison et al., 2012). As discussed in this paper, emerging evidence suggests that attitudes that devalue the role and status of older people can negatively impact their health and wellbeing and may contribute to their risk of abuse by others (ALRC, 2017; Hirst et al., 2016). It is important, therefore, to balance these considerations; to take seriously the social and economic challenges of an ageing population while avoiding disempowering older people through negative stereotypes and social exclusion.
Diverse backgrounds
Older people in Australia are a diverse population, representing different cultural backgrounds, lifestyles and abilities. In 2016, more than a third (37%) of older people were born overseas, mainly from European (67% of those born overseas) and Asian backgrounds (16%) (ABS, 2016a). Aboriginal and Torres Strait Islander peoples had a younger age profile than non-Indigenous people with 4.8% of the Aboriginal and Torres Strait Islander population aged 65 and older compared to 16% for the non-Indigenous population (ABS, 2016a).
Employment
An increasing proportion of older Australians are in paid employment. In early 2018, 13% of Australians aged 65 years and older participated in the workforce compared to 8% of older Australians in 2006 (AIHW, 2018). A large proportion of older Australians receive a government-funded age pension, with 66% of all people aged 65 and older receiving at least a partial age pension in 2017 (AIHW, 2018).
Disability
Older people are much more likely to have a disability or a severe or profound core activity limitation than younger people. In 2015, an estimated 18% of Australia's total population had a disability and 5.8% had a severe or profound core activity limitation (AIHW, 2017a). In comparison, around half (50.7%) of all older people had a disability during the same year and 36.4% of those adults had a severe or profound activity limitation (ABS, 2016b).
Dementia
Like disability, the risk of dementia increases with age. While there is no nationally consistent data on the diagnosis of dementia, it is estimated that about 365,000 people in Australia were living with dementia in 2017, with the vast majority (99%) of those aged 60 years or older (AIHW, 2017a). Based on AIHW (2017a) analysis, almost all people with dementia have a disability and increasingly need assistance from others as dementia progresses. In 2015, around half (51%) of people with dementia lived in households, while just under half (49%) lived in care accommodation (AIHW, 2017a).
Living arrangements
In 2015, most older people (94.8%) lived in private households with only a small proportion (5.2%) living in care accommodation, such as residential aged care (ABS, 2016b). For people living in households, about a quarter (27%) lived alone - with women (35%) more likely than men (18%) to live alone (AIHW, 2017a).
Many older people need assistance with a range of daily activities, such as reading and writing, communication, mobility, transport and self-care (AIHW, 2017a). Older people's need for assistance also increases with age, with around 22% of people aged 65-69 years and 89% of those aged 90 years and older needing assistance with activities (AIHW, 2017a). In 2015, most assistance was provided by informal carers (73%), followed by formal carers (60%) (AIHW, 2017a).
While disability, dementia and the need for assistance all increase with age, these factors are not intrinsic to ageing itself. As discussed in this paper, it is important to recognise that while disability, dependence on others and dementia can represent vulnerability for older people, it is the combination of other factors, such as poor quality relationships or low social support, that can exacerbate the risk of abuse for older people.
3 In this paper, 'older people' refers to people aged 65 years and over, unless otherwise stated.
What is elder abuse?
In Australia, elder abuse is typically defined as involving a form of mistreatment of an older person that occurs within a relationship where there is an expectation of trust (ALRC, 2017; Kaspiew et al., 2016). It can be in a range of forms, including physical, psychological, sexual, financial or social abuse and neglect. Perpetrators of elder abuse may include, but are not limited to, family members, friends, health and social welfare professionals, and formal and informal carers. Elder abuse can occur in a range of settings, including community-based and institutional care settings. However, despite some widely recognised definitions of elder abuse, there is no universal consensus on its definition (Kaspiew et al., 2016).
This section begins with a brief history of the concept in research and practice, before outlining some of the main issues involved in defining elder abuse, its prevalence in community and institutional care settings, its impact on victims and associated risk factors.
A brief history
The definition of elder abuse has been approached in various ways since the 1970s and has developed alongside changing social and historical contexts (Jackson, 2016b; Mysyuk, Westendorp, & Lindenberg, 2013). Beginning in the 1970s, early definitions of elder abuse focused on the physical abuse of female victims, known variously as 'granny battering', 'granny bashing' and 'granny battering syndrome' (Mysyuk et al., 2013). Early definitions narrowly conceived elder abuse as the physical abuse of older women. They carried with them assumptions of older women as vulnerable, burdensome and dependent on caregivers, with the abuse usually the result of caregiver stress (Jackson, 2016b).
In the 1980s, definitions of elder abuse were expanded to include a wider range of abusive behaviours (e.g. psychological and financial abuse) and potential victims, including older men (Mysyuk et al., 2013). The view that elder abuse was solely the result of caregiver stress was also challenged. Alternative theories, borrowing from developments in the field of family violence, focused on the perpetrators of abuse, rather than the victims' vulnerabilities or self-neglect (Jackson, 2016b). In the 1990s, broader definitions were proposed to include a wider range of potential perpetrators - not just caregivers - as well as recognising the wide range of contexts in which abuse may occur (Mysyuk et al., 2013).
Over recent decades, understandings of elder abuse have continued to develop to recognise that it is not a single phenomenon but a complex and diverse set of abusive behaviours. This is, in part, a recognition that there are many disciplinary perspectives that can be applied to its definition. As Jackson (2016b) argues, elder abuse is 'sometimes a crime, sometimes a medical issue, sometimes a social services issue, and sometimes a combination of these and more' (p. 5).
Rights-based perspectives have challenged traditional views that have assumed older people are primarily in need of protection and have instead promoted the need to recognise and respect the dignity and autonomy of older adults (Clare, Clare, Blunde, & Clare, 2014; Dow & Joosten, 2012; Harbison et al., 2012). At the same time, public health approaches have been applied to broaden prevention and response strategies in recognition of the various societal and community level factors that may be associated with the incidence of elder abuse (Kaspiew et al., 2016).
How is elder abuse currently defined?
One of the most widely accepted definitions of elder abuse, which is adopted by the World Health Organization (WHO),4 defines elder abuse as:
a single or repeated act, or lack of appropriate action, occurring within any relationship where there is an expectation of trust which causes harm or distress to an older person. (WHO, 2008, p. 1)
This is a broad definition that covers a wide range of abuse types that many recognise as necessary for an adequate definition of elder abuse (ALRC, 2017; Qu et al., 2017). An important characteristic of this definition is its focus on the relationship between abuser and older person - a relationship defined by trust. In this sense, elder abuse defined this way can be characterised as a 'betrayal of trust' (Mysyuk et al., 2013, p. 55). While defined in this way, it remains an area of debate about what kinds of relationships include an expectation of trust (Qu et al., 2017). In its final report for the inquiry into Protecting the Rights of Older Australians from Abuse, the ALRC defines these relationships as those that:
include an expectation of trust as a result of an 'affective relationship', such as family members, friends, and informal carers, and those in a 'functional position of trust', such as paid carers and some professionals. (ALRC, 2017, p. 37)
In addition to this clarification, it is also important to highlight that this definition is not limited to the abuse of older people by younger people but also includes the abuse of older people by older people, such as spouses/partners. While not captured in this definition, some studies include the abuse of older people by their peers (e.g. older residents in institutional care settings).
In Australia, there is no nationally consistent definition of elder abuse (see Box 2). Definitions of elder abuse face a range of conceptual difficulties that arise in relation to the diversity of behaviours and experiences encompassed by the term 'elder abuse', debate about who should be considered as potential victims and perpetrators, and the kinds of policy and practice responses needed to address it. The main issues involved in defining elder abuse (ALRC, 2017; Harbison et al., 2012; Jackson, 2016b; Jackson & Hafemeister, 2016; Joosten, Vrantsidis, & Dow, 2017; Lacey, Middleton, Bryant, & Garnham, 2017; Mysyuk et al., 2013; Roberto, 2016) include:
- Who should be included as potential victims (e.g. all adults over a certain age or particular 'at-risk' adults)?
- What types of abuse should be recognised as elder abuse?
- How does elder abuse relate to other forms of abuse (e.g. family violence)?
- How do older people view elder abuse (e.g. older people's views may differ from the views of researchers, policy makers and practitioners)?
It is necessary to clarify these issues to understand what elder abuse is, the contexts in which it occurs and how it should be addressed in policy and practice. These issues are discussed below.
Box 2: Developing a definition of elder abuse for future research
As part of the Elder Abuse National Research project commissioned by the Australian Government, Attorney-General's Department, consultations about what constitutes elder abuse have been undertaken with a range of stakeholders. This project and earlier research (Qu et al., 2017) suggest there is broad consensus for a definition that is inclusive of a wide range of abuse types and potential perpetrators.
Older people or 'at-risk' adults?
There is some debate about whether potential victims of elder abuse should be defined by a particular age threshold or by a particular kind of vulnerability to abuse (i.e. 'at-risk' adults). Notably, the WHO definition of elder abuse does not define who counts as an older person. While WHO (2018) more generally defines an older person as someone aged 60 years or older, this age threshold may vary depending on the life expectancy and cultural understandings of particular populations. In Australia, where there is, approximately, a 10-year difference in life expectancies between Indigenous and non-Indigenous populations (AIHW, 2018), an older person is usually defined as someone aged 65 years or older (ABS, 2016b) for non-Indigenous people, and 45-50 years and older for Aboriginal and Torres Strait Islander peoples (Kaspiew et al., 2016).
There are other considerations relating to age as a defining feature of elder abuse. Some researchers and advocates have argued that, while particular risks for abuse increase as people get older (e.g. disability, cognitive impairment, frailty, limited mobility, etc.), these should not be seen as inherent to ageing itself (ALRC, 2017; Joosten et al., 2017; Moir, Blundell, Clare, & Clare, 2017). Rather, it is argued, elder abuse would be better conceptualised as relating to adults who are 'at-risk' of mistreatment, such as adults with cognitive impairment or who are socially isolated, which may make some people more vulnerable to abuse than others (ALRC, 2017). Such approaches to defining elder abuse seek, in part, to avoid characterising all older people above a certain age as vulnerable to abuse and neglect in the same ways. On the other hand, others have argued that defining elder abuse in reference to an age threshold is a valid approach because it captures a diverse set of capacities, vulnerabilities and experiences closely associated with ageing, even if these are not intrinsic to ageing itself (ALRC, 2017; Hamby, Smith, Mitchell, & Turner, 2016).
The tension between defining potential victims of elder abuse as 'older people' or 'at-risk adults' remains unresolved in research and policy literature. In Australia, there is an increasing recognition of the diversity of older populations in terms of older people's capacities, vulnerabilities and experiences (ALRC, 2017; Joosten et al., 2017). This has led to an emphasis on particular 'at-risk' adults in policies and practices that respond to elder abuse in its specific forms (ALRC, 2017), while definitions of elder abuse in research and theoretical literature have tended to retain their reference to age as a defining feature. Different terminology, therefore, may be needed for different purposes (e.g. referring to particular 'at-risk' adults when responding to particular forms of elder abuse; or referring to older people when discussing overall prevalence rates of elder abuse).
What types of abuse are considered elder abuse?
In policy and practice, elder abuse is generally recognised as one or more of the following five main types of abuse (ALRC, 2017; Kaspiew et al., 2016; Pillemer, Burnes, Riffin, & Lachs, 2016):
- physical abuse
- psychological or emotional abuse
- sexual abuse
- financial abuse
- neglect.
Table 1 provides an example of how the main types of elder abuse can be defined, as provided in the National Plan to Respond to the Abuse of Older Australians (Elder Abuse) 2019-2023 published by the Attorney-General's Department. Definitions of elder abuse types may vary between jurisdictions. Readers are encouraged to refer to how elder abuse is defined within their state or territory and as it applies to their practice.
| Abuse type | Definition |
|---|---|
| Physical abuse | An act that causes physical pain or injury to an older person. It can include, but is not limited to, actions such as hitting, pushing or kicking. Inappropriate use of drugs or physical restraints is also an example of physical abuse. |
| Psychological or emotional abuse | An act that causes emotional pain or injury to an older person. It can include insulting or threatening a person, acts of humiliation or disrespect, and controlling behaviours including confining or isolating a person. |
| Sexual abuse | Any sexual behaviour without a person's consent. It includes sexual interactions and non-contact acts of a sexual nature. |
| Financial abuse | The misuse or theft of an older person's money or assets. It can include but is not limited to, behaviours such as using finances without permission, using a legal document such as an enduring power of attorney for purposes outside what it was originally signed for, withholding care for financial gain, or selling or transferring property against a person's wishes. |
| Neglect | The failure to meet a person's basic needs such as food, housing and essential medical care. |
Source: Council of Attorneys-General (2019)
There is debate about whether there are additional categories of abuse and neglect distinct from the five main types outlined. Though less widely recognised as distinct categories, other forms of abuse may include social abuse, chemical/medical abuse, self-neglect and abandonment (Clare et al., 2014; Department of Health and Human Services, 2009; Jackson, 2016a; Rzeszut, 2017; SA Health, 2014). However, it may be considered that these types of abuse are already incorporated in the five main types defined above or, alternatively, are not within scope. For example, chemical/medical abuse is sometimes identified as a distinct form of abuse but may also be incorporated in to definitions of physical abuse or neglect (Hall, Karch, & Crosby, 2016). Abandonment may be identified as a distinct form of abuse or be incorporated in to definitions of neglect (Department of Health and Human Services, 2009). Social abuse that involves controlling and restricting an older person's movements and access to family and friends can also be considered a form of psychological/emotional abuse (ALRC, 2017).
In some policy frameworks, definitions of elder abuse explicitly exclude mistreatment that occurs within residential aged-care settings.5 However, most theoretical definitions do not exclude institutional care settings from among their potential contexts. In such institutional care settings, some types of elder abuse can manifest in pronounced ways. For example, restrictive practices that are sometimes used in residential care facilities - for example, seclusion, physical restraint or sedatives - may amount to the physical or psychological abuse of older people if used improperly or disproportionate to need (Office of the Public Advocate (Qld), 2017).
Adding to the complexity of conceptualising elder abuse as distinct types of abuse is the recognition that different forms of abuse can co-occur as a form of poly-victimisation (Heisler, 2017; Ramsey-Klawsnik & Heisler, 2014). Recent focus on poly-victimisation has highlighted the intersection of multiple forms of abuse as a pattern of victimisation, as well as the cumulative effects over the life course that can lead to abuse in older age (Hamby et al., 2016).
Poly-victimisation also highlights the potential severity of abuse experienced by older people (Burnes, Pillemer, & Lachs, 2017). Recent research has suggested that a substantial proportion of all elder abuse incidents are not single events but rather part of a series of abuse (Burnes et al., 2017). For example, in their analysis of elder abuse in the state of New York, USA, Burnes and colleagues (2017) found that most cases of emotional abuse and neglect occurred at least 2-10 times over a 12-month period, with around a quarter of all emotional abuse and neglect experienced 10 or more times.
How is elder abuse different to family violence?
Another consideration relating to the definition of elder abuse is its relationship to family violence and whether or not it should be seen as a distinct phenomenon. While elder abuse often occurs within a family context, it is generally recognised as a broader phenomenon than family violence (ALRC, 2017; Harbison et al., 2012; State of Victoria, 2016). Elder abuse may, however, be a form of family violence, insofar as it may occur within families and may share similar sets of risk factors (e.g. history of family violence, child abuse, substance abuse). In Australia, the Family Law Act 1975 (Cth) defines family violence as:
violent, threatening or other behaviour by a person that coerces or controls a member of the person's family (the family member), or causes the family member to be fearful. (s. 4AB(1))
This definition of family violence holds much in common with WHO's definition of elder abuse, discussed above, which defines abuse as a form of harm or distress caused to an older person. However, unlike family violence, elder abuse can occur outside family contexts and can be perpetrated by a wider range of potential abusers (Harbison et al., 2012; State of Victoria, 2016). In addition, the victims of elder abuse are typically identified as people aged 60 years and older or 65 years and older, whereas victims of family violence may be any age. Family violence, therefore, can sometimes be a form of elder abuse, and vice versa, but is not synonymous with it.
How do older people view elder abuse?
A final consideration relating to the definition of elder abuse concerns the views of older people. It is important to consider older people's views to ensure that research, policy and practice responses are not dominated by particular professional perspectives but are inclusive of older people's own experiences and understandings of elder abuse (Anand, Begley, O'Brien, Taylor, & Killick, 2013; Killick, Taylor, Begley, Carter Anand, & O'Brien, 2015; National Ageing Research Institute & La Trobe University, 2013).
Based on the relatively few studies conducted, older people have tended to view elder abuse in broader terms that are not limited to interpersonal acts of abuse or neglect. In a systematic review, Killick and colleagues (2015) found that older people conceptualise elder abuse both in terms of interpersonal mistreatment and as relating to broader social attitudes and expectations. At this level, elder abuse has been described in terms of intergenerational disrespect, loss of agency, limitation of social roles, social exclusion, age discrimination and systemic abuse (e.g. availability of appropriate public services) (Anand et al., 2013; Killick et al., 2015). The available evidence suggests that, for some older people, elder abuse is viewed as both a form of ageism that devalues their status and role in society and as an act of interpersonal abuse and neglect (Anand et al., 2013; Dow & Joosten, 2012; Harbison et al., 2012; Killick et al., 2015; Taylor, Killick, O'Brien, Begley, & Carter-Anand, 2014).
4 The definition of elder abuse used by the World Health Organization was originally developed in 1995 by the non-government organisation Action on Elder Abuse, based in the UK. See the Action on Elder Abuse website for more information: www.elderabuse.org.uk/Pages/Category/what-is-it
5 For example, Preventing and Responding to Abuse of Older People (Elder Abuse): NSW Interagency Policy; see www.facs.nsw.gov.au/download?file=591024
Prevalence of elder abuse
Little is known about the national prevalence of elder abuse in Australia. While several prevalence studies have been conducted in other countries, a prevalence study is yet to be conducted in Australia. The available evidence is limited and does not provide a clear understanding of the prevalence of elder abuse in Australia. However, data collected through advocacy organisations, related population studies (e.g. ABS Personal Safety Survey), criminal justice agencies and other administration data provide some insight into its incidence and dynamics (Kaspiew et al., 2016).
Evidence relating to the prevalence of elder abuse is further limited by a lack of studies in institutional care settings and the likely under-representation of adults with disability or cognitive impairment in population studies more generally (Chesterman & Bedson, 2017; Pillemer et al., 2016; Yon et al., 2018).
International findings
Community settings
Internationally, a recent meta-analysis of elder abuse prevalence studies estimated that 15.7% of older adults (60 years and older) in community settings had experienced some form of abuse in the past 12 months (Yon, Mikton, Gassoumis, & Wilber, 2017). This estimated figure represents the combination of one or more subtypes of abuse experienced by older people. Prevalence rates for particular subtypes of abuse were lower and ranged between 0.9% and 11.6% depending on type:
- sexual abuse (0.9%)
- physical abuse (2.6%)
- neglect (4.2%)
- financial abuse (6.8%)
- psychological abuse (11.6%).
The study found that the prevalence of elder abuse varied by region of the world, with high-income countries reporting lower prevalence than low-income countries. Overall, it revealed very little difference between males and females in combined prevalence rates, though it did support other findings that show older women are more likely to be victims of intimate partner violence than older men.
These estimates are, however, limited by some significant methodological issues. This includes variations in how elder abuse is defined and measured across studies and the under-representation of people with disability or cognitive impairment (e.g. dementia) in the studies. The prevalence of elder abuse for older adults with disability and cognitive impairment is likely to be comparatively higher than for the general population (Yon et al., 2018).
Institutional care settings
There is very limited data to accurately estimate the prevalence of elder abuse in institutional care settings (Castle, Ferguson-Rome, & Teresi, 2015; Yon et al., 2018). Based on the few rigorous studies conducted, Yon and colleagues (2018) estimate that elder abuse is likely to be more prevalent in institutional care settings than in community-based settings. Table 2 presents summary results of a systematic review of prevalence studies of elder abuse in institutional care settings from various countries around the world (none of which were conducted in Australia).
| Elder abuse types | Prevalence of elder abuse reported by older adults (%) | Prevalence of elder abuse reported by staff (%) |
|---|---|---|
| Psychological | 33.4 | 32.5 |
| Physical | 14.1a | 9.3 |
| Sexual | 1.9 | 0.7 |
| Neglect | 11.6 | 12.0 |
| Financial | 13.8 | N/A |
| Overall | N/A | 64.2 |
Notes: aAdjusted for publication bias.
Source: Yon et al. (2018)
Due the small number of studies available, differences in definitions used and the range of different contexts in which they were conducted, these results should be read with caution. Even so, the results show a general consistency in prevalence rates for each abuse type reported by older adults and staff. Psychological abuse is the most prevalent form of abuse reported by both older people and staff, estimated to affect between 32.5% and 33.4% of all older people in institutional care settings.
Australian findings
With no national prevalence data of elder abuse available in Australia, researchers have looked to international studies to provide an insight in to how prevalent it might be in Australia. As Kaspiew and colleagues observe (2016, p. 26), 'if international indications provide any guidance, it is likely that between 2% and 14% of older Australians experience elder abuse in any given year' (see also Lacey et al., 2017). While this estimate provides an indication of its potential prevalence in Australia, it should be treated with some caution because it may not reflect the Australian experience.
Incidence of elder abuse in Australia
While there is no prevalence data available in Australia, there is some data relating to the incidence and dynamics of elder abuse in Australia. Based on analysis of the ABS 2012 Personal Safety Survey (PSS), it was found that older women aged 55 years and older were less likely to experience cohabiting partner violence - physical assault, physical threat, sexual assault or sexual threat - compared to a younger cohort (aged 25-34 years) in the past 12 months; 0.4% of all older women aged 55 years and older compared to 3% of women aged 25-34 years (Kaspiew et al., 2016). Based on the Australian Longitudinal Study of Women's Health, around 8% of older women reported some form of abuse when surveyed in 2008 (aged 82-87 years) and 2011 (aged 85-90 years), with slightly lower rates of abuse reported at a younger age (70-81 years). The study also revealed that 20% of women aged 70-75 years and 85-90 years experienced neglect (Kaspiew et al., 2016).
A more recent analysis of ABS datasets examined the incidence of abuse of people aged 55 years and older (Hill & Katz, 2019). It found that, in 2016, 1.7% of older people aged 55 years and older experienced physical violence (either physical assault or threat) in the past 12 months, with slightly more older men experiencing physical violence than older women. Although not directly comparable due to the use of a different dataset and definition of physical abuse, this analysis found higher rates of physical abuse among older Aboriginal and Torres Strait Islander people aged 45 years and over in 2014/15, with 16.4% reporting an experience of physical abuse (including threats of violence) in the past 12 months. According to PSS data collected during 2005, 2012 and 2016, between 0.1% and 0.4% of women aged 55 years and older reported experiencing sexual violence in the past 12 months (limited sample sizes and low prevalence rates prevented analysis of sexual violence for older men). Analysis of PSS data also revealed that older women experienced higher rates of emotional abuse by a partner in the last 12 months than older men: 2.5-3.2% of women aged 55 years and older compared to 1.0-2.6% of men the same age (Hill & Katz, 2019).
Data collected by state- and territory-based advocacy organisations reveal further details about the proportion of abuse types and victim/perpetrator characteristics reported to helplines. That is, it provides some insights about the characteristics of elder abuse incidents reported to advocacy organisations but not about their prevalence at a population level. In its 2015/16 national elder abuse report, Advocare Incorporated (2016) compiled administration data collected by 12 advocacy organisations around Australia. Of the 2,717 advocacy cases and 12,993 information calls received during 2015/16, financial abuse (38%) and psychological abuse (36%) were the most frequently reported, followed by neglect (14%), physical abuse (9%), social abuse (6%) and sexual abuse (0.3%). Sons or daughters (including stepsons and daughters) were the most frequently reported perpetrators (60%), other perpetrators included friends and neighbours, parents, spouses, siblings, grandchildren, and nieces and nephews.
Similar findings are reported by other state-based advocacy organisations, such as Seniors Rights Victoria (SVR), Aged Rights Advocacy Service (ARAS) in South Australia, the Elder Abuse Prevention Unit (EAPU) in Queensland and the NSW Elder Abuse Helpline and Resource Unit of New South Wales. Helpline data collected by these agencies reveal consistent patterns of financial and psychological abuse as the most frequently reported types of abuse. Older women are the most frequently reported victims of abuse overall, and sons and daughters were the most frequently reported perpetrators (Joosten, Dow, & Blakey, 2015; Lacey et al., 2017; NSW Elder Abuse Helpline and Resource Unit, 2015; Spike, 2015).
Impacts of elder abuse
The abuse of older people negatively impacts the victims in a range of ways. In a general sense, elder abuse has the common effect of reducing an older person's quality of life (Jackson & Hafemeister, 2016). The main effects of elder abuse can include (Acierno, Hernandez-Tejada, Anetzberger, Loew, & Muzzy, 2017; ALRC, 2017; Dong, Chen, Chang, & Simon, 2013; Jackson & Hafemeister, 2016):
- psychological distress and emotional difficulties (e.g. depression, fear, chronic stress)
- disruptions in social and family relationships
- compromised health
- physical injury and hospitalisation
- premature mortality
- restrictions on, or elimination of, autonomy
- changes in living arrangement
- loss of assets and finances.
As in other areas of elder abuse research, there is relatively little evidence about the various effects of elder abuse; not only on victims but also on family members (Hamby et al., 2016). The impact of abuse, like the abuse itself, can often go undetected and is difficult to quantify (Roberto, 2016). In one of the few studies that have investigated the long-term impacts of elder abuse, Acierno and colleagues (2017) found that victims of elder abuse experienced higher rates of depression, post-traumatic stress disorder, anxiety and poor health compared to non-victims, with these effects enduring over long periods of time (see also Roberto, 2016).
In response to the relative lack of evidence on the impacts of elder abuse, Hamby and colleagues (2016) have argued that future research should incorporate a wider view of potential impacts of elder abuse that includes subjective, financial, family and spiritual wellbeing.
Risk factors for elder abuse
This section draws on research literature - predominantly international population studies but also Australian studies where available - to outline emerging evidence on the various risk factors associated with elder abuse, with a focus on risk factors for victims and perpetrators, as well as relationship and contextual factors (see also the Appendix for a summary of risk factors associated with particular abuse types). While outlined in this way, these risk factors should not be seen in isolation. Rather, as research evidence suggests, the risk for elder abuse often involves a combination of factors associated with victims, perpetrators and contexts (Johannesen & LoGiudice, 2013). As Day, Boni, Evert, and Knight (2017) summarise:
Elder abuse is best conceptualised as resulting from a complex interaction between the victim and perpetrator, which is influenced by specific individual characteristics, the quality of the relationship, and the influence of the wider social and cultural environment. (p. 1532)
Box 3 outlines the main theoretical frameworks used to explain the complex interactions between various types of risk factors that contribute to elder abuse.
Box 3: Theoretical frameworks for understanding elder abuse
Theoretical frameworks help clarify the nature and dynamics of elder abuse (Harbison et al., 2012; Jackson & Hafemeister, 2016). In particular, they help make sense of the range of potential risk factors that may be involved in elder abuse, how they might interact, and the kinds of prevention and intervention strategies needed to respond.
Three of the main theoretical frameworks for understanding elder abuse are:
- ecological framework
- life-course perspective
- human rights-based framework.
These frameworks are often used in conjunction with each other (Castle et al., 2015; Jackson, 2016b; McDonald & Thomas, 2013; Norris, Fancey, Power, & Ross, 2013). Other theoretical perspectives, such as carer stress theory, have been offered as explanations for particular forms of abuse but have tended to be too limited in their focus to accommodate the complexities of elder abuse (McDonald & Thomas, 2013; Norris et al., 2013). These theoretical perspectives and others are often combined in complementary ways to provide a more holistic view of the complex dynamics of elder abuse (Jackson, 2016b).
Ecological framework
An ecological framework focuses on the range of environmental contexts that influence the risk or occurrence of elder abuse (Schiamberg & Gans, 1999; von Heydrich, Schiamberg, & Chee, 2012). It comprises four inter-related environmental layers:
- an older person's immediate social environment (e.g. family)
- an older person's family relationships and other social support networks
- an older person's external social environments
- broader cultural values, norms and practices within society.
This framework provides an understanding of how various risk and protective factors operating at each level interact with each other. A bi-focal perspective is often applied to this framework to focus on the relationship between perpetrators and victims, rather than only focusing on the victims of elder abuse (von Heydrich et al., 2012). Figure 2 presents a simplified model of this bi-focal ecological framework.
Figure 2: Bi-focal ecological model of elder abuse
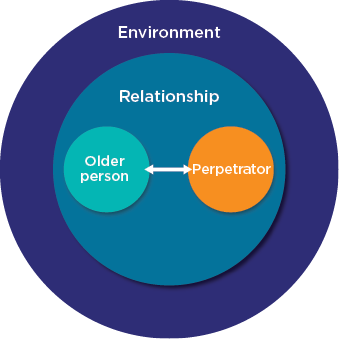
Source: Diagram adapted from Johannesen and LoGiudice (2013)
Life-course perspective
A life-course perspective focuses on the intergenerational aspects of elder abuse, particularly how the history of family relationships and transitions to different life stages influence the risk of elder abuse (McDonald & Thomas, 2013; Schiamberg & Gans, 1999). This perspective provides an understanding of how early life events (e.g. child abuse, family violence or family conflict) can affect an older person's risk of abuse, including the quality of carer-care recipient relationships.
Human rights-based framework
A human rights perspective offers a normative framework to consider how broader social, cultural and legal factors can either inhibit or enable the enjoyment of an older person's right to dignity, autonomy and self-determination (ALRC, 2017; Biggs & Haapala, 2013; Dow & Joosten, 2012; Lacey, 2014). In this perspective, elder abuse is viewed as an issue of dignity and justice for older people that has broader social and systemic causes, such as age discrimination and loss of agency (Anand et al., 2013; Biggs & Haapala, 2013; Lacey, 2014; State of Victoria, 2016).
Risk factors for victims
There are multiple factors relating to an older person that can contribute to their risk of abuse. Cognitive impairment, functional or care dependency, psychological difficulties, lower income or poverty, problem behaviours, poor physical health and social isolation are some of the main factors associated with victims of elder abuse that have emerged from international prevalence studies (Dong, 2015; Dow & Joosten, 2012; Jackson & Hafemeister, 2016; Johannesen & LoGiudice, 2013; Kaspiew et al., 2016; Pillemer et al., 2016; von Heydrich et al., 2012). Other factors identified in prevalence studies include frailty, alcohol use, trauma or history of abuse, ethnicity (i.e. minority groups), relationship status, incontinence and personality traits (Burnes et al., 2015; Johannesen & LoGiudice, 2013; Ostaszkiewicz, 2017; Pillemer et al., 2016).
Box 4: A note about risk factors
Risk factors is a widely used term that refers to an association between a particular factor (e.g. social isolation) and an outcome (e.g. abuse). Risk factors do not usually demonstrate a causal relationship between things. For example, if cognitive impairment is a risk factor for elder abuse, it does not mean that cognitive impairment causes elder abuse.
In addition, risk factors identified in research are usually in relation to a particular study population (e.g. people aged 65 years and over living in Chicago, USA, in 2006) and, as such, do not necessarily translate to other populations or contexts. The reliability of particular risk factors between contexts generally depends on the strength of the association found and its consistency across different studies.
Cognitive impairment and disability
Cognitive impairment - including dementia - has consistently emerged as a strong risk factor for elder abuse across a range of empirical studies (Bagshaw, Wendt, Zannettino, & Adams, 2013; Dong, 2015; Fang & Yan, 2018; Johannesen & LoGiudice, 2013; Kaspiew et al., 2016). Deterioration in cognitive functioning, such as memory loss or confusion, limits an older person's ability to carry out routine tasks and self-care (Fang & Yan, 2018). As such, older adults with cognitive impairment are likely to require assistance with daily living from a caregiver, with more severe forms of impairment needing more intensive support. A heavy care burden may lead to caregiver stress and burnout that can exacerbate the risk of abuse of care recipients (Fang & Yan, 2018; Johannesen & LoGiudice, 2013). In addition, behavioural problems associated with dementia can cause conflict between the caregiver and the older adult, which may also lead to abuse (Fang & Yan, 2018).
Similar to the care or assistance needs relating to cognitive impairment, functional or care dependency is also associated with elder abuse (Dong, 2015; Johannesen & LoGiudice, 2013). This may be a result of physical function impairment (e.g. physical disability and frailty) that, as described above, limits self-care and creates situations of dependency, which can increase the risk of abuse.
Poor mental health
Where present, the poor mental health of older adults, such as depression and psychological distress, is a significant risk factor associated with abuse (Dong, 2015; Dong et al., 2013; Jackson & Hafemeister, 2016; McDonald & Thomas, 2013; Pillemer et al., 2016). Like other risk factors identified, poor mental health may co-occur with other factors that exacerbate the risk of abuse of older adults. Poor mental health may be associated with dementia or other forms of cognitive impairment, for example, and thus also be associated with care dependency (Fang & Yan, 2018). It may be both a result of past abuse and a risk for future abuse (Acierno et al., 2017; McDonald & Thomas, 2013).
Social isolation
Social isolation is another factor associated with the abuse of older people identified across a range of population and smaller scale studies (Acierno et al., 2017; Johannesen & LoGiudice, 2013; Kaspiew et al., 2016; von Heydrich et al., 2012). Researchers have suggested that social isolation creates a condition of vulnerability for older people due to limited access to social support, increased demands on caregivers, and less opportunities for abuse to be detected and reported by others (Kaspiew et al., 2016; von Heydrich et al., 2012). In a US population study, Acierno and colleagues (2017) found that low levels of social support were strongly associated with the mistreatment of older people in a US-based population study (see also Acierno et al., 2010). Conversely, a high level of social support was found to both reduce the negative impacts of elder abuse and be a protective factor against future abuse (Acierno et al., 2017).
History of abuse, family violence or conflict
A history of abuse, family violence and family conflict has been found to be a risk factor associated with some types of elder abuse, particularly physical abuse and neglect (Jackson & Hafemeister, 2016; Johannesen & LoGiudice, 2013; Kaspiew et al., 2016; McDonald & Thomas, 2013). This may be part of a continuation of abuse and conflict within family and intimate partner relationships that occurs over the life course (Kaspiew et al., 2016). McDonald and Thomas (2013), for example, found evidence that abuse experienced in childhood can increase the likelihood of experiencing abuse in later life. Similarly, Jackson and Hafemeister (2016) suggest that cases of neglect may be a consequence of poor child-parent relationships that have developed from insecure attachment in early childhood. In such cases, an adult child, who has a poor relationship with their parent and has reluctantly taken on a caregiving role, may lack the motivation and requisite skills to provide appropriate care for their older parent, which may lead to neglect.
Other factors
Ethnic backgrounds (i.e. minority populations), low income, poverty and poor physical health are some of the other more frequently identified risk factors associated with victims of elder abuse to have emerged from population studies (Johannesen & LoGiudice, 2013; Pillemer et al., 2016). While some population studies have revealed broader demographic characteristics, such as ethnicity and poverty as risk factors for elder abuse, relatively little research has explored what causes or dynamics might be involved (Jervis et al., 2016). Jervis and colleagues (2016), for example, note that race/ethnicity is often associated with low income and poverty, and so caution against cultural explanations for increased risk of elder abuse among some ethnic minority populations. Where race/ethnicity has been found to be a risk factor even after controlling for other variables, Jervis and colleagues (2016) suggest further research is needed to determine the range of contributing factors, such as discrimination, that may be involved.
Risk factors for perpetrators
Less is known about risk factors associated with perpetrators of elder abuse than for victims (Pillemer et al., 2016). Based on available evidence, several factors have been identified that may contribute to the risk of individuals perpetrating elder abuse. Caregiver burden or stress, dependency on older person, sense of entitlement, drug and alcohol abuse, history of family violence or conflict, mental health difficulties (including psychiatric illness and psychological problems) are some of the main factors that may be associated with elder abuse (Jackson, 2016a; Jackson & Hafemeister, 2016; Johannesen & LoGiudice, 2013; McDonald & Thomas, 2013; Pillemer et al., 2016). The risk factors discussed below focus on attributes of the perpetrator but not on the type of relationship itself (e.g. spousal, parent-child, carer-care recipient relationships).
Caregiver stress
Caregiver stress has featured strongly in early theories about the causes of elder abuse (Jackson, 2016a). This has been supported to some extent in subsequent studies that have found caregiver stress to be a risk for elder abuse, particularly when providing care to older people with dementia or disability (Johannesen & LoGiudice, 2013). However, like other risk factors, this is likely to be the result of a combination of factors - specifically those associated with caregiver skills and capacity and an older person's aggressive behaviours that strain relationships between caregivers and older adults (Labrum, 2017; von Heydrich et al., 2012). In other words, the quality of relationships and other supports may moderate the negative effects of caregiver stress.
Financial or emotional dependency on older adult
Dependency on older people is a risk factor for elder abuse. Perpetrators of abuse are more likely to depend on an older person in various ways - emotionally, financially, housing - than non-perpetrators of abuse (Joosten et al., 2017; Pillemer et al., 2016). In some cases, such relationships of dependency have been described as 'parasitic', where an adult child with associated risks lives in a dependent relationship with their older parent (Jackson & Hafemeister, 2016). In these situations, an older person's risk of abuse may increase substantially. This can be exacerbated further in relationships of interdependency, where an older adult feels responsible for protecting an abusive adult child and may be less inclined to report incidents of abuse (Jackson & Hafemeister, 2016).
Poor mental health
Various studies have found poor mental health, including psychiatric disorders, to be a significant risk factor among perpetrators of abuse (Jackson & Hafemeister, 2016; Labrum, 2017; Pillemer et al., 2016). Poor mental health is more likely to co-occur with behavioural problems, substance abuse, dependency on older adults and relationship conflict that exacerbate the risk for elder abuse.
Alcohol and other drugs
Alcohol and substance misuse are risk factors for perpetrators of elder abuse (Jackson, 2016a; Johannesen & LoGiudice, 2013; Pillemer et al., 2016). Similar to the associations between perpetrators and poor mental health and dependency on older adults, it may be a combination of factors - as opposed to substance misuse alone - that can increase this risk (Jackson & Hafemeister, 2016). There is some evidence to suggest substance abuse is more closely associated with physical and emotional abuse than other forms of elder abuse (Moore & Browne, 2017).
Attitudes of entitlement
There is some evidence to suggest that family members' attitudes of entitlement contribute to the risk of abuse, particularly financial abuse (Bagshaw et al., 2013; Miskovski, 2014). In a small Australian study focused on financial abuse, Bagshaw and colleagues (2013) found that service providers and older people both reported that family members' sense of entitlement to an older person's assets was one of the main causes underlying emotional and financial abuse (see also Miskovski, 2014). Attitudes of entitlement are closely related to issues concerning ageism, which are discussed in more detail below.
Relationship and contextual risk factors
In addition to the risks associated with victims and perpetrators of abuse, there are also relationship and contextual factors that can contribute to the risk of elder abuse. These factors operate at the level of relationships, community and society.
Relationship risk factors
A range of relationship factors are associated with elder abuse, including the type and quality of relationships. Importantly, risks associated with relationship types do not necessarily represent entirely new sets of factors from those described above but rather a combination of factors associated with victims and perpetrators (Jackson, 2016a).
Different relationship types are associated with different forms of abuse (von Heydrich et al., 2012). For instance, family has been found to be the most common relationship type involved in overall cases of elder abuse in some population studies (Jackson, 2016a). In some studies, adult children have been found to be more likely to neglect their older parents than other perpetrators, with paid carers and spouses slightly less likely to neglect an older person's care than adult children (Jackson, 2016a). On the other hand, available evidence suggests that intimate partners are more likely to be physically and psychologically abusive than other perpetrators (Jackson, 2016a; Pillemer et al., 2016; Wijeratne & Reutens, 2016).
More generally, family conflict and poor relationships are strongly associated with elder abuse (Johannesen & LoGiudice, 2013; von Heydrich et al., 2012). In other words, the quality of relationships between older adults and their adult children can influence the risk of abuse, with an older adult's perception of the quality of family life being a good indicator of increased risk (von Heydrich et al., 2012). Some research has suggested that relationship quality and social supports are the most consequential factors influencing the risk of elder abuse (Johannesen & LoGiudice, 2013). This risk can be exacerbated when an adult child with other associated risk factors (e.g. problem behaviours, substance abuse, financial dependence) lives with their older parent (Jackson & Hafemeister, 2016). In some cases, this can be exacerbated further within relationships of interdependency if the parent feels responsible for the adult child and is unable to leave the abusive relationship (Jackson & Hafemeister, 2016).
Community-level risk factors
Community-level factors may affect other individual and relationship factors that increase the risk of elder abuse. In a study examining the influence of community-level factors on elder abuse, von Heydrich and colleagues (2012) found that alienation from community increases the risk for abuse, but that its impact was moderated by the quality of relationship between caregivers and older adults. The loss of friends for older people is another factor operating at this level that may increase social isolation, which can, in turn, limit access to social support and affect caregiver/older adult relationships. Formal social supports or networks for older people have been suggested as a key protective factor for older adults at risk of social isolation (Johannesen & LoGiudice, 2013).
Institutional care contexts
There is a lack of rigorous research relating to elder abuse in institutional care settings (Yon et al., 2018). However, based on the available research conducted internationally, it is likely that older people living in care institutions are at greater risk of experiencing mistreatment and may face different risks than older people in community settings (Castle et al., 2015; Fang & Yan, 2018), though this may not reflect the Australian experience. Some research suggests that the greater risk of abuse in institutional care settings may be the result of the cohabitation of other residents with associated characteristics that increase the risk of abuse (e.g. dementia, disability, problem/aggressive behaviours), opportunities for resident-to-resident abuse, unregulated restrictive practices, inadequate institutional resources, and carer stress, emotional exhaustion and lack of appropriate caregiver skills (Castle et al., 2015; Day et al., 2017; Office of the Public Advocate (Qld), 2017; Yon et al., 2018).
There is also some evidence to suggest that resident-to-resident abuse is the most prevalent form of abuse in institutional care settings (Castle et al., 2015). Similar findings also suggest that caregiving staff are vulnerable to aggressive or violent behaviours from older people in institutional care settings, which further exacerbates the risk of elder abuse that may result from retaliatory responses by caregiving staff (Castle et al., 2015; McDonald et al., 2012; Yon et al., 2018).
Culturally and linguistically diverse communities
Available research suggests that older people from culturally and linguistically diverse (CALD) communities may face additional risks of abuse as a result of increased social isolation, language barriers and greater dependence on family members (Office of the Public Advocate, 2006). There may also be cultural variations in understanding elder abuse, including differences in expectations of caring roles within families or attitudes towards reporting abuse and seeking assistance (Jervis et al., 2016; Roberto, 2016).
Aboriginal and Torres Strait Islander communities
There is very little research available in relation to the abuse of older Aboriginal and/or Torres Strait Islander peoples. However, there are some recognised differences between Indigenous and non-Indigenous understandings and experiences of elder abuse (Office of the Public Advocate, 2005). As a consequence of lower life expectancies for Aboriginal and Torres Strait Islander peoples, older people are generally defined as those aged 45-50 years and older (Kaspiew et al., 2016). There are also differences in terminology relating to the term 'elder', which in some Aboriginal and Torres Strait Islander communities is a title reserved for community leaders (Office of the Public Advocate, 2005). Differences in cultural understandings of relationships of trust, obligations to family and community members, and family structures mean that risks associated with the abuse of older adults in some Aboriginal and Torres Strait Islander contexts may be different from non-Indigenous contexts.
Societal risk factors
Some researchers have suggested that broader societal factors may create conditions that exacerbate the risk of elder abuse. However, little empirical research has been conducted that demonstrate the particular dynamics that may exist between societal factors and interpersonal abuse and neglect (Hamby et al., 2016; Pillemer et al., 2016). Societal factors may include (Kaspiew et al., 2016; Miskovski, 2014; Pillemer et al., 2016; von Heydrich et al., 2012; Weston & Qu, 2016):
- ageism
- inadequate health and social services for older people
- economic pressures (e.g. affordable housing, intergenerational wealth disparities)
- intergenerational conflict.
In Australia, some have argued that overall wealth disparities between baby boomer and younger generations create conditions for intergenerational conflict, which can exacerbate risks of abuse - particularly forms of financial abuse (Kaspiew et al., 2016). In such cases, wealth disparities between generations may combine with ageist attitudes and lead to what Miskovski (2014) describes as 'inheritance impatience', whereby family members 'deliberately or recklessly prematurely acquire their ageing relatives' assets' (p. 18).
Prevention and intervention
This section outlines a public health model approach to the prevention and intervention of elder abuse in Australia. Specifically, it explores the various legislative, policy and practice frameworks that aim to address elder abuse and summarises the available evidence for particular interventions.
A public health model to the prevention of elder abuse operates at the levels of primary, secondary and tertiary interventions:
- Primary (or universal) interventions target whole communities or populations to prevent elder abuse.
- Secondary interventions target particular at-risk populations (i.e. at-risk adults and/or at-risk perpetrators).
- Tertiary interventions respond to victims and/or perpetrators of elder abuse.
Overall, elder abuse interventions face significant challenges with respect to the complex forms of abuse involved and the lack of a strong evidence base that would inform effective policies and practices (Baker, Francis, Hairi, Othman, & Choo, 2016; Day et al., 2017; Moore & Browne, 2017). In response to these challenges, some have identified the need for prevention and intervention studies to focus on particular sets of risks involving particular victim-perpetrator dyads and specific forms of abuse (Dong, 2015; Jackson & Hafemeister, 2016; Teresi et al., 2016) - for example, older adults with dementia at risk of financial abuse from caregiving relatives.
Primary interventions
Primary interventions that aim to prevent elder abuse can be implemented at various levels (e.g. national, state/territory, system, community, organisational, programmatic levels) and target particular populations (e.g. community members, older adults, caregivers, professionals) and sectors (e.g. health, aged care, social, legal or financial sectors) (Day et al., 2017; Joosten et al., 2017; Moore & Browne, 2017). Prevention strategies operating at broader national or state and territory levels may include:
- Commonwealth and state/territory-based legislation relevant to preventing or remediating forms of elder abuse
- Commonwealth and state/territory-based policy frameworks to guide policy and practice
- education and awareness strategies
- sector-wide workforce development and support for relevant professionals.
Funding for elder abuse prevention initiatives may also be considered part of an overall primary intervention strategy (Hirst et al., 2016).
Australian legislation
There is currently no over-arching legal framework that addresses elder abuse at a national level in Australia. Instead, a range of intersecting federal and state/territory-based laws cover many of its diverse aspects (Kaspiew et al., 2016). This includes a range of civil and criminal laws across Australian jurisdictions that are not usually specific to elder abuse or older people but may nonetheless apply to particular cases of elder abuse (e.g. physical assault, misuse of powers of attorney, etc.) (ALRC, 2017; Joosten et al., 2017).
Commonwealth
The most relevant legal mechanisms in relation to elder abuse at a Commonwealth level are the Aged Care Act 1997 (Cth) and the Age Discrimination Act 2004 (Cth) (Kaspiew et al., 2016; Lacey, 2014). The Aged Care Act primarily contains legal provisions focused on the regulation and monitoring of residential aged-care services, including service accreditation, service provider obligations and the mandatory reporting of physical or sexual assault within federally funded services (Kaspiew et al., 2016).
In its recent inquiry report, the ALRC has recommended the strengthening of the Aged Care Act to: better respond to what it refers to as 'serious incidents'; improve pre-employment screening; and improve regulation around the use of restrictive practices in aged care settings (ALRC, 2017). The Age Discrimination Act has broader legal provisions that, unlike the Aged Care Act, are not focused on any particular service sector. Rather, it is a general mechanism that enables investigations and conciliation in cases of age discrimination, though not elder abuse specifically (Kaspiew et al., 2016).
States and territories
Australian states and territories have a comparatively greater involvement across a wider range of legal provisions and policy frameworks relevant to elder abuse than the Commonwealth. Laws relating to the protection of adults are primarily state/territory based, though they do not necessarily cover all aspects of elder abuse (Lacey, 2014). This includes laws relating, but not limited, to (Joosten et al., 2017; Kaspiew et al., 2016):
- powers of attorney
- guardianship and administration
- criminal justice (e.g. theft, assault)
- wills
- estate planning
- property law.
The Australian Law Reform Commission has recommended the introduction of adult safeguarding laws in Australian states and territories that respond to a broader range of vulnerable adults than currently exist but has not recommended any additional criminal offences relating specifically to elder abuse (ALRC, 2017).
Australian policy frameworks
In March 2019, the Council of Attorneys-General released its National Plan to Respond to the Abuse of Older Australians (Elder Abuse) 2019-2023 (the National Plan). This national policy framework was developed in response to a key recommendation of the ALRC's report, Elder Abuse - A National Legal Response (ALRC, 2017). See Box 5 for more information about the principles guiding the ALRC's recommendations to address elder abuse in Australian policy and practice.
The National Plan outlines five priority areas of action:
- enhancing our understanding
- improving community awareness and access to information
- strengthening service responses
- planning for future decision making
- strengthening safeguards for vulnerable older adults.
These priority areas of action include a range of key initiatives for Australian governments to pursue in response to the abuse of older people. See the National Plan for more information.
Box 5: Australian Law Reform Commission: Balancing two principles
In 2017, the ALRC (2017) published its final report on the inquiry into Protecting the Rights of Older Australians from Abuse. The inquiry covered a range of legal and policy issues relating to elder abuse, including aged care, enduring appointments, family agreements, superannuation, wills, banking, guardianship and financial administration, disability, social security, criminal justice responses and safeguarding adults at risk.
As part of its inquiry, the ALRC made a series of recommendations that aimed to balance two guiding principles:
- dignity and autonomy
- protection and safeguarding.
These principles recognise both the capabilities and agency of older people, while also recognising that various measures are needed to protect and safeguard some older people at increased risk of abuse. Policy and practice responses to elder abuse are, therefore, presented with challenges to balance these principles to both respect an older person's dignity and autonomy with regard to decision making and participation, while also implementing preventative measures that help protect and safeguard older people from potential abuse or neglect. See the ALRC report for more information.
State and territory policy frameworks
Most Australian states and territories have established policy frameworks for the prevention and intervention of elder abuse. These frameworks tend to sit within health or social services portfolios, though increasingly aim to sit across a range of relevant portfolios, such as the NSW Government interagency policy for preventing and responding to abuse of older people. Table 3 summarises the state and territory government policy frameworks in place at the time of writing.
| State/territory | Organisation/department | Policies and guidelines |
|---|---|---|
| Vic. | Department of Health and Human Services | Elder Abuse Prevention and Response Guidelines for Action 2012-14 (2012); and With Respect to Age Practice Guidelines (2009) |
| SA | SA Health | Strategy for the Safeguarding of Older South Australians Action Plan 2014-21 (2015) |
| NSW | NSW Government, Department of Family and Community Services | Preventing and Responding to Abuse of Older People (Elder Abuse) NSW Interagency Policy (June 2018); and NSW Ageing Strategy 2016-2020 (2016) |
| Tas. | Department of Health and Human Services | Protecting Older Tasmanians from Abuse: Elder Abuse Prevention Action Plan 2015-18 (2015); and Responding to Elder Abuse: Tasmanian Government Practice Guidelines for Government and Non-Government Employees (2012) |
| ACT | ACT Government | ACT Elder Abuse Prevention Program Policy (2012) |
| WA | Alliance for the Prevention of Elder Abuse | Elder Abuse Protocol: Guidelines for Action (2013) |
| Qld | Queensland Government | Positively Ageless: Queensland Seniors Strategy 2010-20 (2010) (contains some strategic elements relating to the prevention of elder abuse) |
| NT | - | - |
Source: Table adapted and updated from Kaspiew et al. (2016) and Joosten et al. (2017)
Education and awareness strategies
Education and awareness strategies aim to increase a target population's knowledge and understanding of elder abuse as an early intervention to prevent its occurrence. Education programs are usually targeted to specific populations, such as older adults, potential perpetrators and professionals (Moore & Browne, 2017). Moore and Browne (2017) reviewed a range of education programs that target older adults, professionals in community settings, residents and staff in institutional settings and perpetrators, noting that the evidence supporting these prevention strategies is mixed.
Some evidence-based practices have demonstrated that education programs have increased participants' knowledge and skills in ways that have improved responses to elder abuse, such as increased reporting of abuse by professionals or increased self-esteem and wellbeing reported by older adults (see also Baker et al., 2016). However, there is currently no evidence that demonstrates their effectiveness in preventing or reducing the occurrence of elder abuse (Baker et al., 2016).
Box 6: Barriers to reporting elder abuse
Older people and professionals can face a range of barriers to reporting elder abuse to the appropriate service providers or authorities, depending on the nature of the abuse. For older people, barriers can include (Jackson & Hafemeister, 2016; Norris et al., 2013):
- fear of reporting
- fear of retaliation
- embarrassment and shame
- concerns about consequences for abusive adult children if reported.
For both older adults and professionals, abuse (particularly financial abuse/exploitation) may go undetected (Bagshaw et al., 2013). For professionals, barriers to recognising and reporting abuse may include (Hirst et al., 2016):
- reluctance to acknowledge the abuse
- limited knowledge or lack of protocols to identify abuse
- fear of liability
- lack of appropriate support services that could respond if reported.
Hirst and colleagues (2016) summarise key elements of effective education programs in health care settings based on their review of the literature. In principle, effective education programs for health professionals should comprise the discussion of ethical issues and professional/legal responsibilities in responding to cases of suspected abuse, training strategies that increase knowledge about elder abuse and the ability to modify attitudes that condone abuse (Hirst et al., 2016).
Secondary intervention
Secondary interventions target particular at-risk populations to prevent or intervene early to reduce the incidence of elder abuse and its harmful impacts. The main kinds of secondary interventions for elder abuse (Day et al., 2017; Dong, 2015; Hirst et al., 2016; Moore & Browne, 2017) include:
- screening and risk assessment strategies
- social support and capacity building strategies.
Screening and risk assessment strategies
Screening and risk assessment strategies perform an important role in both the prevention and intervention of elder abuse, and are typically implemented in health care settings (Dong, 2015; Hirst et al., 2016). Risk assessment strategies aim to screen an older person for known risk factors, assess their risk of abuse and help determine what actions should be taken in response (Moore & Browne, 2017). Moore and Browne (2017) note that the majority of risk assessment tools for elder abuse lack a rigorous evidence base but many demonstrate the status of either emerging or best practice. Hirst and colleagues (2016) summarise key elements of effective screening and risk assessment strategies in health care settings, which they argue should include a multifaceted approach to assessment, be conducted routinely in health care settings, and employ the skills of a team of experts.
Social and other support strategies
Prevention strategies that provide social support are broader in scope than education programs or risk assessment strategies. Some of the more common social support strategies include caregiver/family support services, financial management programs, legal assistance and elder abuse helplines (ALRC, 2017; Pillemer et al., 2016). Caregiver support may be offered in the form of housekeeping, respite care or support groups that aim to reduce caregiver burden or stress in an effort to prevent elder abuse. Pillemer and colleagues (2016) suggest that there is some evidence for the effectiveness of caregiver support programs as a strategy to prevent elder abuse. Similarly, there is some evidence to suggest that financial management programs targeted to at-risk older adults may help prevent financial abuse (Pillemer et al., 2016). Elder abuse helplines that offer advice and referrals to older people and family members are similarly supported by limited, but positive, evidence that suggests that they may be effective in preventing abuse (Pillemer et al., 2016).
Box 7: Social support as a key protective factor
Social support has emerged as one of the strongest protective factors identified in elder abuse studies (Acierno et al., 2017; Hamby et al., 2016; Pillemer et al., 2016). Social support in response to social isolation and poor quality relationships has also been identified as a promising focus of intervention because, unlike some other risk factors (e.g. disability, cognitive impairment), there is greater potential to improve the negative effects of social isolation (Hamby et al., 2016).
Tertiary interventions
Tertiary interventions aim to address the incidence and impact of elder abuse after it has occurred and typically target either older adults who have been victims of abuse or the perpetrators of abuse.
Tertiary interventions responding to elder abuse face some serious challenges. The complexity of elder abuse in its multiple and diverse forms prevents a one-size fits all approach to intervention (Joosten et al., 2017). Consequently, many researchers have argued that interventions should address particular forms of elder abuse, rather than elder abuse as a general phenomenon (Dong et al., 2013; Hirst et al., 2016; Jackson & Hafemeister, 2016).
Interventions are further hampered by a general lack of evidence about what works to effectively address elder abuse and respond to the needs of its victims and/or perpetrators (Baker et al., 2016; Day et al., 2017; Dong et al., 2013; Hirst et al., 2016). Beyond these challenges and in recognition of the complex forms that elder abuse can take, others have suggested that interventions should incorporate an understanding of poly-victimisation that is client-focused (rather than incident-focused) and trauma-informed (Heisler, 2017).
Elder abuse intervention strategies typically focus on either older people, caregivers/perpetrators or family relationships (Joosten et al., 2017). An overview of the main kinds of interventions that target each of these population groups is provided below.
Interventions targeting older people
While the evidence is still emerging, some researchers have argued that multidisciplinary and coordinated intervention approaches are needed to respond to the complexities of elder abuse (Chesterman, 2016; Day et al., 2017; Hirst et al., 2016; Joosten et al., 2017). Multidisciplinary interventions bring together various combinations of social, legal, health and mental health professionals to provide holistic and tailored responses to particular forms of elder abuse. Multidisciplinary approaches to risk and needs assessment and referral operate in a similar way by drawing upon various expertise to ensure comprehensive identification of an older person's potential risks and needs (Joosten et al., 2017). Such approaches are designed to respond to the range of unique needs of older people who have been victims of one or more forms of abuse.
Case management and advocacy interventions may also involve multidisciplinary responses but, rather than being managed by a team, are facilitated by a case manager to assess an older person's needs and assist them to access other support services (Joosten et al., 2017). Motivational interviewing is a practice technique that aims to assist older people with decision making in relation to desired responses to cases of elder abuse, which may be effective in helping resolve an older person's feelings of ambivalence towards taking action (Joosten et al., 2017).
Other interventions for which the evidence is still emerging include elder abuse helplines and emergency shelters. Based on their review, Pillemer and colleagues (2016) found some evidence to support the use of elder abuse helplines that aim to help advocate for an older person by providing advice and assistance to refer to other support services. Emergency shelters that cater for the unique needs of older adults living in unsafe environments are another intervention for which the evidence is still emerging and will need further evaluation to demonstrate its efficacy (Pillemer et al., 2016).
Interventions targeting perpetrators
Interventions that focus on caregivers who have perpetrated abuse are less common than those focused on victims of abuse. Consistent with other prevention and intervention strategies, there is very limited evidence to support particular caregiver/perpetrator interventions, particularly with regard to reducing the occurrence of elder abuse and its related harms (Baker et al., 2016). However, there is some evidence to support some psychological approaches to caregivers/perpetrators (Joosten et al., 2017; Pillemer et al., 2016), including psycho-educative support groups for caregivers, anger management for caregivers and counselling for perpetrators. The positive results that some of these interventions show relate primarily to improved knowledge or reduced anxiety or depression for caregivers but do not relate to a reduction in incidents of elder abuse itself (Baker et al., 2016; Joosten et al., 2017).
Interventions targeting families
Interventions that focus on family relationships include family mediation, family care conferences and family-focused psychological or counselling approaches (Joosten et al., 2017). In Australia, these interventions mainly operate at a tertiary level, but it should be noted that they are sometimes implemented as secondary prevention measures.
These kinds of interventions are relatively new approaches to addressing elder abuse, with little research to demonstrate their effectiveness in reducing the incidence or impacts of elder abuse. However, given the importance of family relationships in moderating the risk of elder abuse, some have argued that family-focused approaches to elder abuse prevention and/or interventions should be explored further (Joosten et al., 2017).
Family mediation, facilitated by a trained professional, may be useful to help resolve family conflicts relating to care needs and financial matters (including inheritance disagreements), which may help reduce the risk of elder abuse. However, such approaches might not be appropriate in cases where elder abuse or family violence is being perpetrated. Family care conferences are run in similar ways to family mediation but focus on facilitating collaboration and communication between family members rather than aiming to resolve family conflict. Finally, psychological or counselling approaches that use family-based cognitive behavioural social work also show some promise in their ability to reduce the risk of perpetration among family caregivers, though more research is needed (Joosten et al., 2017).
Summary of prevention and intervention strategies
Policy and practice responses to elder abuse are still developing and are hampered by the lack of local evidence to inform and support particular strategies. However, there are promising policy initiatives currently underway, particularly the National Plan to Respond to the Abuse of Older Australians (Elder Abuse) 2019-2023, that aim to establish a more comprehensive and coordinated approach to responding to elder abuse in its complex forms. While the evidence to support prevention and intervention strategies is currently underdeveloped, available research on risk and protective factors for abuse provides a useful starting point for future developments in these areas. More research - including program evaluations - will be needed to establish an evidence base to inform future policy and practice development, particularly in relation to prevention and intervention strategies that target particular at-risk older adults at the community, organisational and programmatic levels.
Conclusion
Elder abuse is a complex phenomenon that involves a range of types of abuse perpetrated against older people. Currently, there are no data on the prevalence of elder abuse in Australia, with best estimates suggesting that between 2% and 14% of older Australians may experience some form of abuse every year. As the existing research literature makes clear, there is a wide range of factors relating to victims, perpetrators, relationships and contexts that may be associated with elder abuse. However, very little research is available to help inform practical responses to prevent or intervene to mitigate these risks and reduce the occurrence or recurrence of abuse.
Ageism and intergenerational conflict have emerged as major themes that some researchers have suggested may influence broader patterns of elder abuse in Australia. In response, many have suggested that greater efforts are needed to ensure that older people are valued and feel included in Australian society, communities and families. Social isolation and poor quality relationships - particularly between family members - have also emerged as factors that strongly influence the risk of abuse for older adults. Conversely, these issues are also promising sites for future prevention and intervention strategies that aim to mitigate these risks and prevent elder abuse from occurring.
Implications for policy and practice
Policy makers should consider the primary, secondary and tertiary interventions outlined in this paper and how they may be implemented at the various national, state/territory, system, community, organisational and programmatic levels. As national policy is strengthened through the implementation of the National Plan to address elder abuse, policy makers working at all levels should consider coordinated approaches to developing education and awareness strategies, supporting workforce development initiatives and building an evidence base to support evidence-informed practices.
Service providers and practitioners should also consider secondary and tertiary interventions outlined in this paper that target particular at-risk populations to prevent and respond to elder abuse. In recognition of the complex nature of elder abuse, service providers should consider working with others to develop multidisciplinary approaches that respond to the complex needs of at-risk older adults, perpetrators and family members.
This paper highlights a need for research on the prevalence of elder abuse in Australia, and its associated dynamics and risk factors, to inform policies and practices that aim to address elder abuse. It also highlights the need for research and evaluation on specific prevention and intervention strategies and programs to give a clearer understanding of what works to protect and promote the dignity of older Australians.
References
- Family Law Act 1975 (Cth)
- Acierno, R., Hernandez, M. A., Amstadter, A. B., Resnick, H. S., Steve, K., Muzzy, W., & Kilpatrick, D. G. (2010). Prevalence and correlates of emotional, physical, sexual and financial abuse and potential neglect in the United States: The National Elder Mistreatment Study. American Journal of Public Health, 100(2), 292-297.
- Acierno, R., Hernandez-Tejada, M. A., Anetzberger, G. J., Loew, D., & Muzzy, W. (2017). The National Elder Mistreatment Study: An 8-year longitudinal study of outcomes. Journal of Elder Abuse & Neglect, 29(4), 254-269. doi:10.1080/08946566.2017.1365031
- Advocare Incorporated. (2016). National elder abuse: Annual report 2015-2016. Perth: Advocare Incorporated. Retrieved from www.advocare.org.au/uploaded/files/client_added/NEA%20Annual%20Report%202015-2016(1).pdf
- Anand, J., Begley, E., O'Brien, M., Taylor, B., & Killick, C. (2013). Conceptualising elder abuse across local and global contexts: Implications for policy and professional practice on the island of Ireland. Journal of Adult Protection, 15(6), 280-289. doi:10.1108/JAP-03-2013-0011
- Australian Bureau of Statistics (ABS). (2016a). Ageing population, 2016. Canberra: ABS. Retrieved from www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/2071.0~2016~Main%20Features~Ageing%20Population~14
- ABS. (2016b). Disability, ageing and carers, Australia: Summary of findings, 2015. Canberra: ABS. Retrieved from www.abs.gov.au/ausstats/[email protected]/mf/4430.0
- Australian Institute of Health and Welfare (AIHW). (2017a). Australia's welfare 2017 (Cat. No. AUS 214). Canberra: AIHW. Retrieved from www.aihw.gov.au/reports/australias-welfare/australias-welfare-2017/contents/table-of-contents
- AIHW. (2017b). Older Australia at a glance (Cat. No. AGE 87). Canberra: AIHW. Retrieved from www.aihw.gov.au/reports/older-people/older-australia-at-a-glance/contents/summary
- AIHW. (2018). Closing the Gap targets: 2017 analysis of progress and key drivers of change (Cat. No. IHW 193). Canberra: AIHW. Retrieved from www.aihw.gov.au/reports/indigenous-australians/closing-the-gap-targets-2017-analysis-of-progress/contents/summary
- AIHW. (2019). Insights into vulnerabilities of Aboriginal and Torres Strait Islander people aged 50 and over: 2019 - In brief. (Cat. No. IHW 207). Canberra: AIHW. Retrieved from www.aihw.gov.au/reports/indigenous-australians/vulnerabilities-aboriginal-torres-strait-50-over/contents/table-of-contents
- Australian Law Reform Commission (ALRC). (2017). Elder abuse - a national legal response: Final report. Sydney: ALRC.
- Bagshaw, D., Wendt, S., Zannettino, L., & Adams, V. (2013). Financial abuse of older people by family members: Views and experiences of older Australians and their family members. Australian Social Work, 66(1), 86-103.
- Baker, P. R., Francis, D. P., Hairi, N. N., Othman, S., & Choo, W. Y. (2016). Interventions for preventing abuse in the elderly. Cochrane Database of Systematic Reviews, 8. doi:10.1002/14651858.CD010321.pub2
- Biggs, S., & Haapala, I. (2013). Elder mistreatment, ageism, and human rights. International Psychogeriatrics, 25(8), 1299-1306. doi:10.1017/S1041610212002372
- Burnes, D., Pillemer, K., Caccamise, P. L., Mason, A., Henderson, C. R., Jr., Berman, J. et al. (2015). Prevalence of and risk factors for elder abuse and neglect in the community: A population-based study. Journal of the American Geriatrics Society, 63(9), 1906-1912. doi:10.1111/jgs.13601
- Burnes, D., Pillemer, K., & Lachs, M. S. (2017). Elder abuse severity: A critical but understudied dimension of victimization for clinicians and researchers. Gerontologist, 57(4), 745-756. doi:10.1093/geront/gnv688
- Castle, N., Ferguson-Rome, J. C., & Teresi, J. A. (2015). Elder abuse in residential long-term care: An update to the 2003 national research council report. Journal of Applied Gerontology, 34(4), 407-443. doi:10.1177/0733464813492583
- Chesterman, J. (2016). Taking control: Putting older people at the centre of elder abuse response strategies. Australian Social Work, 69(1), 115-124.
- Chesterman, J., & Bedson, L. (2017). Are national elder abuse prevalence studies inclusive of the experiences of people with cognitive impairment? Findings and recommendations for future research. Melbourne: Office of the Public Advocate.
- Clare, M., Clare, B., Blunde, B. B., & Clare, J. (2014). Conceptualising elder abuse: Does this label fit? Communities, Children and Families Australia, 8(1), 37-48.
- Council of Attorneys-General. (2019). National Plan to Respond to the Abuse of Older Australians (Elder Abuse) 2019-2023. Canberra: Attorney-General's Department. Retrieved from www.ag.gov.au/elderabuse
- Day, A., Boni, N., Evert, H., & Knight, T. (2017). An assessment of interventions that target risk factors for elder abuse. Health & Social Care in the Community, 25(5), 1532-1541.
- Department of Health and Human Services. (2009). With respect to age - 2009. Melbourne: Department of Health and Human Services. Retrieved from www2.health.vic.gov.au/about/publications/policiesandguidelines/with-respect-to-age-2009
- Department of the Prime Minister and Cabinet. (2019). Closing the gap: Report 2019. Canberra: Department of the Prime Minister and Cabinet. Retrieved from ctgreport.pmc.gov.au
- Dong, X. (2015). Elder abuse: Systematic review and implications for practice. Journal of the American Geriatrics Society, 63(6), 1214-1238. doi:10.1111/jgs.13454
- Dong, X., Chen, R., Chang, E. S., & Simon, M. (2013). Elder abuse and psychological well-being: A systematic review and implications for research and policy. A mini review. Gerontology, 59(2), 132-142. doi:10.1159/000341652
- Dow, B., & Joosten, M. (2012). Understanding elder abuse: A social rights perspective. International Psychogeriatrics, 24(6), 853-855. doi:10.1017/S1041610211002584
- Fang, B., & Yan, E. (2018). Abuse of older persons with dementia: A review of the literature. Trauma, Violence & Abuse, 19(2), 127-147. doi:10.1177/1524838016650185
- Hall, J. E., Karch, D. L., & Crosby, A. E. (2016). Elder abuse surveillance: Uniform definitions and recommended core data elements for use in elder abuse surveillance, Version 1.0. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
- Hamby, S., Smith, A., Mitchell, K., & Turner, H. (2016). Poly-victimization and resilience portfolios: Trends in violence research that can enhance the understanding and prevention of elder abuse. Journal of Elder Abuse & Neglect, 28(4/5), 217-234.
- doi:10.1080/08946566.2016.1232182
- Harbison, J., Coughlan, S., Beaulieu, M., Karabanow, J., VanderPlaat, M., Wildeman, S., & Wexler, E. (2012). Understanding 'elder abuse and neglect': A critique of assumptions underpinning responses to the mistreatment and neglect of older people. Journal of Elder Abuse & Neglect, 24(2), 88-103. doi:10.1080/08946566.2011.644086
- Heisler, C. J. (2017). Moving forward: Recommendations for advancing late-life polyvictimization practice, policy, and research. Journal of Elder Abuse & Neglect, 29(5), 351-363. doi:10.1080/08946566.2017.1388013
- Hill, T., & Katz, I. (2019). Insights into abuse of older people: Analysis of Australian Bureau of Statistics datasets. (SPRC Report 3/19). Sydney: Social Policy Research Centre, UNSW Sydney. doi.org/10.26190/5c7494f7499b9
- Hirst, S. P., Penney, T., McNeill, S., Boscart, V. M., Podnieks, E., & Sinha, S. K. (2016). Best-practice guideline on the prevention of abuse and neglect of older adults. Canadian Journal on Aging, 35(2), 242-260. doi:10.1017/S0714980816000209
- Jackson, S. L. (2016a). All elder abuse perpetrators are not alike: The heterogeneity of elder abuse perpetrators and implications for intervention. International Journal of Offender Therapy and Comparative Criminology, 60(3), 265-285. doi:10.1177/0306624X14554063
- Jackson, S. L. (2016b). The shifting conceptualization of elder abuse in the United States: From social services, to criminal justice, and beyond. International Psychogeriatrics, 28(1), 1-8. doi:10.1017/S1041610215001271
- Jackson, S. L., & Hafemeister, T. L. (2016). Theory-based models enhancing the understanding of four types of elder maltreatment. International Review of Victimology, 22(3), 289-320. doi:10.1177/0269758016630887
- Jervis, L. L., Hamby, S., Beach, S. R., Williams, M. L., Maholmes, V., & Castille, D. M. (2016). Elder mistreatment in underserved populations: Opportunities and challenges to developing a contemporary program of research. Journal of Elder Abuse & Neglect, 28(4/5), 301-319. doi:10.1080/08946566.2016.1245644
- Johannesen, M., & LoGiudice, D. (2013). Elder abuse: A systematic review of risk factors in community-dwelling elders. Age and Ageing, 42(3), 292-298.
- Joosten, M., Dow, B., & Blakey, J. (2015). Profile of elder abuse in Victoria: Analysis of data about people seeking help from Seniors Rights Victoria. Summary report. Melbourne: Seniors Rights Victoria. Retrieved from seniorsrights.org.au/wp- content/uploads/2014/03/Summary-Report_Profile-of-Elder-Abuse-in-Victoria_Final.pdf
- Joosten, M., Vrantsidis, F., & Dow, B. (2017). Understanding elder abuse: A scoping study. Melbourne: Melbourne Social Equity Institute. Retrieved from socialequity.unimelb.edu.au/__data/assets/pdf_file/0012/2449659/Elder-Abuse-A-Scoping-Study-MSEI-and-NARI.pdf
- Kaspiew, R., Carson, R., & Rhoades, H. (2016). Elder abuse: Understanding issues, frameworks and responses. Melbourne: Australian Institute of Family Studies. Retrieved from aifs.gov.au/publications/elder-abuse
- Killick, C., Taylor, B. J., Begley, E., Carter Anand, J., & O'Brien, M. (2015). Older people's conceptualization of abuse: A systematic review. Journal of Elder Abuse & Neglect, 27(2), 100-120.
- Labrum, T. (2017). Factors related to abuse of older persons by relatives with psychiatric disorders. Archives of Gerontology and Geriatrics, 68, 126-134. doi:10.1016/j.archger.2016.09.007
- Lacey, W. (2014). Neglectful to the point of cruelty? Elder abuse and the rights of older persons in Australia. Sydney Law Review, 36(1), 131-161.
- Lacey, W., Middleton, H., Bryant, L., & Garnham, B. (2017). Prevalence of elder abuse in South Australia: Final report. Current data collection practices of key agencies. Adelaide: Analysis and Policy Observatory. Retrieved from apo.org.au/node/101301
- McDonald, L., Beaulieu, M., Harbison, J., Hirst, S., Lowenstein, A., Podnieks, E., & Wahl, J. (2012). Institutional abuse of older adults: What we know, what we need to know. Journal of Elder Abuse & Neglect, 24(2), 138-160. doi:10.1080/08946566.2011.646512
- McDonald, L., & Thomas, C. (2013). Elder abuse through a life course lens. International Psychogeriatrics, 25(8), 1235-1243. doi:10.1017/S104161021300015X
- Miskovski, K. (2014). Preventing financial abuse of people with dementia. North Ryde, NSW: Alzeimer's Australia NSW. Retrieved from www.dementia.org.au/sites/default/files/20140618-NSW-Pub-DiscussionPaperFinancialAbuse.pdf
- Moir, E., Blundell, B., Clare, J., & Clare, M. (2017). Best practices for estimating elder abuse prevalence in Australia: Moving towards the dynamic concept of 'adults at risk' and away from arbitrary age cut-offs. Current Issues in Criminal Justice, 29(2), 181-190.
- Moore, C., & Browne, C. (2017). Emerging innovations, best practices, and evidence-based practices in elder abuse and neglect: A review of recent developments in the field. Journal of Family Violence, 32(4), 383-397. doi:10.1007/s10896-016-9812-4
- Mysyuk, Y., Westendorp, R. G. J., & Lindenberg, J. (2013). Added value of elder abuse definitions: A review. Ageing Research Reviews, 12(1), 50-57.
- National Ageing Research Institute & La Trobe University. (2013). 'What older people want?': Outcomes from a consultation with older consumers about their priorities for research in ageing. Parkville: National Ageing Research Institute. Retrieved from www.nari.net.au/files/aaa_consultation_report_14_jan_2014.pdf
- Norris, D., Fancey, P., Power, E., & Ross, P. (2013). The critical-ecological framework: Advancing knowledge, practice, and policy on older adult abuse. Journal of Elder Abuse & Neglect, 25(1), 40-55. doi:10.1080/08946566.2012.712852
- NSW Elder Abuse Helpline and Resource Unit. (2015). Submission to the Parliamentary Inquiry into Elder Abuse in New South Wales (Submission No. 33). Sydney: Parliament of New South Wales. Retrieved from www.parliament.nsw.gov.au/committees/inquiries/Pages/inquiry-submission-details.aspx?pk=%2053721
- Office of the Public Advocate. (2005). Mistreatment of Older People in Aboriginal Communities Project: An investigation into elder abuse in Aboriginal communities. Perth: Office of the Public Advocate. Retrieved from www.publicadvocate.wa.gov.au/_files/Mistreatment_older_aboriginal.pdf
- Office of the Public Advocate. (2006). Care and respect: Project to research elder abuse in culturally and linguistically diverse communities. Perth: Office of the Public Advocate. Retrieved from www.publicadvocate.wa.gov.au/_files/Report_on_Elder_Abuse_in_CALD_communities.pdf
- Office of the Public Advocate (Qld). (2017). Legal frameworks for the use of restrictive practices in residential aged care: An Australian and international comparative analysis. Brisbane: Office of the Public Advocate.
- Ostaszkiewicz, J. (2017). A conceptual model of the risk of elder abuse posed by incontinence and care dependence. International Journal of Older People Nursing, 13(2). doi:10.1111/opn.12182
- Pillemer, K., Burnes, D., Riffin, C., & Lachs, M. S. (2016). Elder abuse: Global situation, risk factors, and prevention strategies. Gerontologist, 56, S194-S205. doi:10.1093/geront/gnw004
- Productivity Commission. (2013). An ageing Australia: Preparing for the future. Canberra: Productivity Commission. Retrieved from www.pc.gov.au/research/completed/ageing-australia/ageing-australia.pdf
- Qu, L., Carson, R., Kaspiew, R., Weston, R., Commerford, J., Dean, A. et al. (2017). Elder abuse prevalence scoping study: A report to the Australian Government Attorney-General's Department. Melbourne: Australian Institute of Family Studies.
- Ramsey-Klawsnik, H., & Heisler., C. (2014). Polyvictimization in later life. Victimization of the Elderly and Disabled, 17(1).
- Roberto, K. A. (2016). The complexities of elder abuse. American Psychologist, 71(4), 302-311. doi:10.1037/a0040259
- Rzeszut, S. M. (2017). The need for a stronger definition: Recognizing abandonment as a form of elder abuse across the United States. Family Court Review, 55(3), 444-457. doi:10.1111/fcre.12295
- SA Health. (2014). Strategy to Safeguard the Rights of Older South Australians 2014-2021. Adelaide: Government of South Australia. Retrieved from www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/about+us/publications+and+resources/plans/strategy+to+safeguard+the+rights+of+older+south+australians+2014-2021
- Schiamberg, L. B., & Gans, D. (1999). An ecological framework for contextual risk factors in elder abuse by adult children. Journal of Elder Abuse & Neglect, 11(1), 79-103.
- Spike, C. (2015). The EAPU helpline: Results of an investigation of five years of call data. Report for the International Association of Gerontology and Geriatrics Asia & Oceania Regional Congress 2015. Chermside Central, Qld: UnitingCare.
- State of Victoria. (2016). Royal Commission into Family Violence: Summary and recommendations. Melbourne: Royal Commission into Family Violence. Retrieved from www.rcfv.com.au/Report-Recommendations
- Taylor, B. J., Killick, C., O'Brien, M., Begley, E., & Carter-Anand, J. (2014). Older people's conceptualization of elder abuse and neglect. Journal of Elder Abuse & Neglect, 26(3), 223-243. doi:10.1080/08946566.2013.795881
- Teresi, J. A., Burnes, D., Skowron, E. A., Dutton, M. A., Mosqueda, L., Lachs, M. S., & Pillemer, K. (2016). State of the science on prevention of elder abuse and lessons learned from child abuse and domestic violence prevention: Toward a conceptual framework for research. Journal of Elder Abuse & Neglect, 28(4-5), 263-300. doi:10.1080/08946566.2016.1240053
- von Heydrich, L., Schiamberg, L. B., & Chee, G. (2012). Social-relational risk factors for predicting elder physical abuse: An ecological bi-focal perspective. International Journal of Aging & Human Development, 75(1), 71-94.
- Weston, R., & Qu, L. (2016). Attitudes towards intergenerational support. Melbourne: Australian Institute of Family Studies. Retrieved from aifs.gov.au/publications/attitudes-towards-intergenerational-support
- Wijeratne, C., & Reutens, S. (2016). When an elder is the abuser. Medical Journal of Australia, 2015(6), 246-247.e241.
- World Health Organization (WHO). (2008). A global response to elder abuse and neglect: Building primary health care capacity to deal with the problem worldwide. Geneva: WHO.
- WHO. (2018). Elder abuse. Geneva: WHO. Retrieved from www.who.int/news-room/fact-sheets/detail/elder-abuse
- Yon, Y., Mikton, C. R., Gassoumis, Z. D., & Wilber, K. H. (2017). Elder abuse prevalence in community settings: A systematic review and meta-analysis. Lancet Global Health, 5(2), e147-e156.
- Yon, Y., Ramiro-Gonzalez, M., Mikton, C. R., Huber, M., & Sethi, D. (2018). The prevalence of elder abuse in institutional settings: A systematic review and meta-analysis. European Journal of Public Health. doi:10.1093/eurpub/cky093
Appendix: Risk factors by abuse type
The table below summarises various risk factors associated with particular abuse types identified across a range of studies, but not necessarily all of them. It is important to highlight that the factors identified do not necessarily translate to all populations or contexts and are provided for summary purposes only. It should also be noted that it does not evaluate the strength of the evidence for each risk factor identified.
| Abuse type | Risk factors for older people | Risk factors for perpetrators | Relationship or contextual factors |
|---|---|---|---|
| Physical abuse | Age (<70 years) Gender (female) Low income Poor health Low social support Functional impairment/dependence Separated/divorced status Behavioural problems | Dependency on older adult History of family violence Employment status Poor mental health/psychological problems Social isolation Partner/spousal relationship Adult-child relationship | Caregiver/care recipient cohabitation Quality of relationships Lack of formal social supports |
| Psychological or emotional abuse | Lower age (<70 years) Previous trauma experience Low social support Functional impairment/dependence Separated/divorced status | History of family violence Poor mental health/psychological problems Social isolation Partner/spousal relationship Substance misuse | Lack of formal social supports |
| Sexual abuse | Previous trauma experience Gender (female) Low social support | History of family violence Poor mental health Social isolation Partner/spousal relationship Acquaintances | (Not available/reported) |
| Financial abuse | Cognitive impairment Functional impairment/dependence Poor health Ethnic minority status Previous trauma experience Fear of loss of dependence Lack of protective scepticism of others | History of family violence Family members Attitudes of entitlement Substance misuse | Intergenerational conflict |
| Neglect | Low income Low social support Need for assistance Ethnic minority status Poor health No use of social services Social isolation | Previous trauma/family violence experience Carer stress/burden Reluctance in caregiving role Resentment towards older person Lack of caregiving skills Adult children | Quality of relationships Family conflict |
Sources: Acierno et al. (2010); Bagshaw et al. (2013); Burnes et al. (2015); Fang and Yan (2018); Jackson (2016a); Jackson and Hafemeister (2016); Kaspiew et al. (2016); Miskovski (2014); Moore and Browne (2017); Pillemer et al. (2016); Schiamberg and Gans (1999)
Adam Dean is a Senior Research Officer with the Child Family Community Australia information exchange at the Australian Institute of Family Studies.
The author wishes to acknowledge and thank Rachel Carson, John Chesterman and Frances Byers for their review and expert feedback on this paper. The author also wishes to thank Karen Broadley, Joanne Commerford, Lixia Qu, Dinika Roopani and Amanda Coleiro for their feedback and advice during the process.
Featured image: © GettyImages/suzanamarinkovic