What is effective primary prevention in sexual assault?
Translating the evidence for action
You are in an archived section of the AIFS website
Overview
This Wrap provides an evidence-based summary of the key issues involved in program design in primary prevention initiatives. It is targeted at those working in the policy and program development areas of sexual assault prevention. Its purpose is to assist decision-making about what primary prevention is, and isn't, and what elements are required for primary prevention to be effective - drawing on information from sexual assault and other fields of primary prevention.
Key messages
-
Primary prevention has been identified as a priority in challenging sexual violence but there is a lack of understanding around what primary prevention is and is not.
-
Although increasing knowledge or awareness of sexual assault may be a feature of primary prevention, it is not a sufficient outcome. Primary prevention must also change behaviours.
-
This paper aims to clarify what primary prevention is, based on a multi-level, ecological conceptualisation of the causes of violence.
-
Although the evidence base lacks many examples of successful primary prevention programs for the sexual assault sector, some work has been done on identifying the elements required for effective primary prevention.
These include: comprehensiveness, community engagement, theory-driven programming, contextualised programming, and evaluation.
Introduction
Primary prevention strategies are implemented before the problem ever occurs … [These] strategies aim to lessen the likelihood of boys and men using violence or girls and women suffering violence in the first place … They are successful when the first instance of sexual violence is prevented. (White Ribbon Foundation, n.d., p.1)
Since 2000, sexual assault and other forms of gender-based violence have been increasingly framed within public policy as a significant public health issue. Major reports have demonstrated the prevalence of sexual violence globally (World Health Organization [WHO], 2002), and the health costs and financial costs of intimate partner violence to the Australian community (Access Economics, 2004; VicHealth, 2004).
In the latter part of the decade, primary prevention has been elevated to a key priority in policy and program design across local, state and territory, and Commonwealth initiatives. This is due to a feminist-informed evidence base - some 30 years in the making - which challenged historical attitudes around sexual violence and concepts of gender, combined with the added insights and tools of a public health approach.
There is broad agreement across disciplines and sectors that the most effective form of prevention is to stop sexual assault from occurring in the first place; and that this means targeting the underlying conditions in relationships, communities, and society that make sexual assault possible.
Challenges emerge however, in translating this consolidated evidence-base into particular operational and institutional contexts. As much as there is shared agreement that primary prevention is the priority (compared for instance to rape avoidance education or using the criminal law as a general deterrent to perpetrators), there is less clarity about what primary prevention programs do, and do not, involve and about how effectiveness or success is to be measured.
The purpose of this Wrap is to summarise the current evidence that underpins primary prevention and that should inform resourcing and decision-making in program design and evaluation. Specifically, it considers:
- primary prevention - what it is and what it isn't;
- key principles of primary prevention programming; and
- characteristics of effective primary prevention programs.
What is “primary prevention”?
Primary prevention in a health context is about changing behaviour to prevent an undesirable social consequence. It may be targeted at a large or specific population. Primary prevention has become the central priority of policy development, implementation and funding - in Australia and internationally - with a large increase in the number of studies, reports, policy frameworks, funding rounds, tenders, and programs for "primary prevention". This represents a real shift in how sexual assault prevention - generally - has been conceived and there is significant activity occurring in the primary prevention space, particularly in prevention education programs.
At the same time, this "explosion" has meant a bewildering array of concepts, terminology, practice standards, and methods for many service providers, educators, policy advisors and funding bodies. The breadth of the current literature has, at times, meant a lack of clarity about what constitutes primary prevention (compared to community education, for example), or what the minimum conditions for effective primary prevention programs are. This paper aims to assist with identifying the characteristics that are present in the design and implementation of effective primary prevention programs.
Primary prevention is often targeted for delivery in an education-based format. Increasing knowledge of a particular issue and changing attitudes with education is a relatively inexpensive method of delivering primary prevention strategies. However, this is only one aspect of prevention and only one way of carrying out primary prevention.1 The key concepts of prevention can be transposed to other settings and other types of programs. What is apparent, however, from the primary prevention literature, is that interventions need shaping and customising depending on their local contextual conditions (Schensul, 2009). The following section is a brief outline of the key concepts of prevention for public health promotion. These basic concepts can be used for the development of primary prevention in a wide range of settings.
Key concepts in prevention planning
It is now common for those working in sexual assault prevention (and violence prevention more broadly) to distinguish between programs or interventions as primary, secondary or tertiary prevention activities. These distinctions are often used as shorthand for three inter-related dimensions:
- when interventions occur (the time dimension);
- who they are targeted at (the population dimension); and
- their location within the social-ecological model (discussed further below) of influences and risk factors for violence (the ecological dimension) (Centers for Disease Control and Prevention, 2004; Sethid, Marais, Seedat, & Butchart, 2004)
Time: when to intervene?
In reference to time, interventions are classified according to when they occur in the chain of circumstances leading up to or following an incident of sexual assault. The US Centers for Disease Control (2004) and VicHealth (2007) delineate the time dimension as such:
- An intervention that occurs before violence occurs with the aim of preventing such violence from ever occurring is classified as primary prevention.
- Secondary prevention or early intervention is aimed at specific individuals or groups who show evidence of becoming perpetrators or victims of sexual violence. The aim is to target certain behaviours before they become established.
- Tertiary prevention describes responses that occur after sexual assault that deal with the immediate and the long-term impacts of sexual assault for victims. It aims to prevent or minimise the impacts from violence and to prevent sex offenders from re-offending.
Who to target
The population dimension refers to who the intervention is targeted at: everyone (universal), those at heightened risk of perpetrating or experiencing sexual assault (selected); or those who have already engaged in sexual assault or have been sexually assaulted (indicated).
The social-ecological model
Current approaches to sexual assault and gender-based violence prevention acknowledge that:
There is no single factor to explain why one person and not another behaves in a violent manner, nor why one community will be torn apart by violence while a neighbouring community lives in peace. Violence is an extremely complex phenomenon that has its roots in the interaction of many factors - biological, social, cultural, economic and political. (WHO, 2002, p. 9)
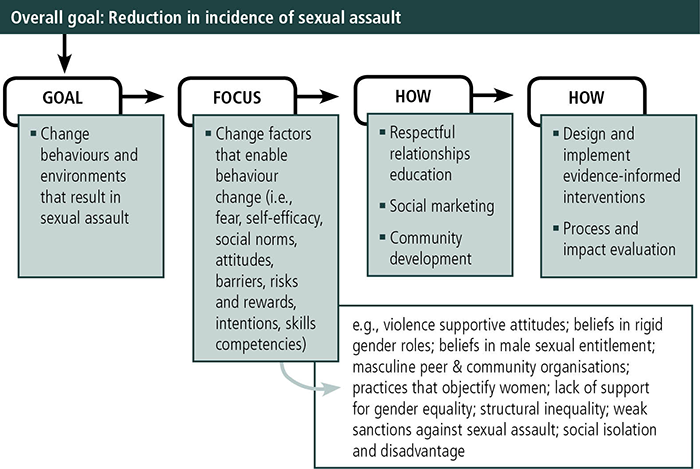
This understanding of gender-based violence as having multiple causal factors is best conceptualised in the social-ecological model that demonstrates the interactive nature of factors that cause violence. Developed initially by Bronfenbrenner (1977), the social-ecological model describes the interrelatedness of different spheres of social life and the interactions between individuals and their environments (see Figure 1 below). The ecological dimension refers to these spheres in the following way (Adapted from Centers for Disease Control and Prevention, 2004, pp. 4-5)
Figure 1: Ecological model of the factors influencing sexual violence perpetration
Footnote
1 Prevention education in schools has been especially targeted in violence prevention sectors because the evidence base demonstrates that working with young people in particular can be a very effective way of shifting the individual and relationship determinants that lead to sexual assault.
Multiple casualty - acknowledging complexity in sexual assault prevention
The ecological framework has been the focus of much of the sexual violence prevention literature, particularly with strategies targeting the community/organisational level. The concept of the "community" or "organisational" level in this discussion refers to the mesosystem in the ecological setting rather than any particular construct of the word community. A community in the context of primary prevention may be any setting selected for a particular intervention, either a geographic location or a particular organisation in which the intervention will be implemented. It is a nebulous concept that can be shaped by the process of developing the intervention. But a community will generally have particular features or characteristics that identify it as such and may be more than a geographical aspect, for example a shared history and social organisation (Schensul, 2009).
According to the ecological model, the community setting is where the formal and informal social structures that influence an individual can best impact on the risk of violence against women. A strategy at this level aims to modify the characteristics of the particular settings selected (such as schools, workplaces or neighbourhoods) in order to decrease the risks of victimisation and perpetration (DeGue et al., 2012).
Strategies that target the community level are a logical delivery point in primary prevention, in the sense that if only individual level behaviours are targeted, small and unsustainable effects are the most likely result (DeGue et al., 2012). In addition, interventions that are based in a community context have the advantage of involving local knowledge, culture and resources in the process of development and implementation which, in turn, is also likely to enhance acceptance and support of the intervention activities (Trickett, 2002). Community strategies, by their nature, must go beyond enacting individual behaviour change. They must alter the environment or context that continues to tolerate or facilitate the unacceptable behaviour (DeGue et al., 2012).
One aspect of this is the culture of the community that is targeted by an intervention. By understanding the local popular culture, and the role it plays in shaping the behaviour of individuals and groups, primary prevention interventions that will impact on behavioural change can be attached to relevant cultural forces and designed to be comprehensible and acceptable to the target community (Trickett, 2002). Examples of primary prevention interventions that target cultural change are bystander interventions that attempt to enable community members to recognise and intervene in situations where particular language or behaviours perpetuate the conditions that enable sexual assault to occur (Casey & Lindhorst, 2009).
Community-level strategies include those that aim to change the norms of that particular community, including risk factors and policies within those communities (DeGue et al., 2012). For example, to implement a strategy for promotion of equal and respectful relationships between men and women there will be a need to address cultural forces that support sexism and discrimination against women (Schwartz & Lindley, 2009).
This approach is sometimes referred to as a community "social norms" approach that aims to change not just individual attitudes, but also the wider community perceptions that violent behaviour is acceptable or "normal". It is, in effect, aimed at changing popular culture to reflect values that don't support sexual assault, which will in turn impact on behaviour.
Identifying community settings
As noted by DeGue et al. (2012), there is a lack of guidance in the sexual violence literature around identification of promising programs and strategies that are effective in behaviour change. It could be argued that primary prevention strategies aimed at the community level are still in a development phase and there is still much learning to be undertaken in expanding the evidence base (Trickett, 2009). Trickett pointed out that this provides opportunity for collaborations between agencies to develop links, or to streamline overlapping programs in order to effect change more broadly. In other words, sexual assault primary prevention is still in a phase that warrants creative thinking and collaboration in order to develop promising programs, potentially drawing on the experiences of primary prevention in other sectors.
Educational settings have been identified as an important focus for violence prevention by fostering appropriate attitudes and relationship skills in young people who are at a pivotal age of influence (Carmody, 2009; Flood, Fergus, & Heenan, 2009). However, this is only one setting in which community level strategies can be applied.
Identification of appropriate settings can evolve from consideration of the environments where change is required. For example, VicHealth (2012) recently assisted five very different community level projects that operated in different settings aimed at attitude and behaviour change. These included:
- a corporate workplace - where the intervention included a whole-of-organisation program to promote gender equity and change organisational culture;
- a community health centre - where a program targeted couples transitioning to parenthood and aimed at changing attitudes and behaviours around gendered parenting roles;
- a faith organisation - where the intervention sought to increase the skills of faith leaders to carry out primary prevention work within their local communities; and
- a local government - which sought to drive cultural shift across all of its functions, to ensure gender equity and non-violent norms became standard social norms.
The variety of settings and diversity of programs indicates that community-level primary prevention offers rich opportunities for creative programing and policy development. Effective evaluation of these interventions will add further knowledge to the sexual violence prevention aetiology and develop understandings around what works in primary prevention.
Societal-level influences and prevention
As noted, much of the current literature focuses on interventions at community levels. There remains a knowledge gap around risk factors and effective interventions at a societal level (DeGue et al., 2012). In conceptualising the ecological interactions, it is logical to expect that change at multiple individual and community levels could also impact the social level, by facilitating a change in social norms (Nastasi & Hitchcock, 2009). Likewise, a policy or regulatory intervention at the interpersonal or societal level can influence and enhance interventions at the community level (Schensul, 2009). Community-level interventions enable contextual program design with local input that enhances relevance and acceptance, while societal-level change requires a broader perspective (Trickett, 2002). They can be designed to support each other towards a common goal. Social media campaigns can be a part of an intervention to target social norms. In addition to raising awareness or knowledge about a topic such as sexual assault, they use a marketing paradigm to influence behaviour in order to effect change (Quadara, 2010). Social media campaigns can also be used as at the community level of the ecological model to influence change at a greater pace (Schensul, 2009).
An example of a social norm that may be targeted at the societal level is gender inequality, which is known to be an underlying determinant in perpetuating violence against women (VicHealth, 2007). To exemplify the magnitude of change required and the entrenched nature of gender inequality, consider that in Australia, women working full-time today still earn 17.4% less than men (Personal Safety Survey Australia 2012, cited in Equal Opportunity for Women in the Workplace Agency, 2012). This income disparity and opportunity for earning prevails over the lifetime of women, including where women take work breaks for caring responsibilities that remain overwhelmingly a female task. Accordingly, women face significant economic disadvantages in accumulating wealth compared to men (Australian Human Rights Commission, 2009). This lack of economic equality is a significant disadvantage (VicHealth, 2007) in a society where wealth enables independence, advantage and privilege. Financial security can increase choices, including choices about remaining in abusive relationships (though this is only one factor and women may stay in these relationships for a variety of reasons). These factors trickle down to community and individual levels to impact on attitudes and the choices that perpetrators and the victims of sexual assault may make, such as behaviours and help-seeking. At a societal level, changes by governments to regulatory instruments or policy can influence the need for communities or organisations to make progress on reducing gender inequity by requiring certain changes.
So what should effective primary prevention programs look like?
The complex and multi-level nature of primary prevention means that there are obvious challenges for evaluating the success (or otherwise) of a particular intervention and therefore determining what is effective. There is a dearth of comprehensive evaluations of multi-level sexual assault programs to consider; establishing the effectiveness of particular features of primary prevention is still a relatively new science. Although this provides an opportunity for creative program design, a framework - or at least an understanding of what features make primary prevention effective - is still required. Much of the current literature draws on other areas of primary prevention in health to consider the features of successful programs that are likely to apply in sexual assault prevention.
The lack of a detailed evaluation base potentially makes the planning and design of primary prevention interventions less certain in terms of success and knowledge of "what works", but by identifying the elements that are needed to make primary prevention effective more generally, decisions around designing and implementing interventions can be clearer.
Comparable fields of prevention work, such as large public health programs, have formed an important source of intervention information that can assist with informing sexual assault primary prevention.
Two key pieces of work considered in this paper have examined the issue of primary prevention in sexual violence and gendered violence prevention. Both have identified factors that need to be present for effective primary prevention.
In the US, Casey and Lindhorst (2009) conducted a wide-ranging review of successful, multi-level primary prevention approaches in other fields (e.g., HIV transmission) that could also be applied to sexual assault prevention. Their study summarised the common factors identified as key requirements for ensuring the efficacy of interventions. The Australian work considered here focused on school-based educative prevention programs (Carmody et al., 2009; Flood et al., 2009), which is an efficient and effective primary prevention program delivery (but is by no means the only setting).
Casey and Lindhorst's (2009) study, which scoped other fields of health prevention, looked at a variety of settings. They identified six key elements for effective primary prevention:
- comprehensiveness;
- community engagement;
- contextualised programming;
- a focus on structural contributors to the problem;
- sound theoretical rationales or frameworks; and
- an emphasis on positive development.
In The National Association Sexual Assault Prevention Education Project, Carmody et al. (2009) identified six standards that should form best practice in primary prevention education delivery. These formed the basis of the Flood et al. (2009) evaluation of a sexual assault primary prevention education program. Flood et al. found that the following five key elements should be present for effective primary prevention in education settings:
- comprehensiveness;
- a program logic;
- effective delivery;
- relevant and socially inclusive practice; and
- evaluation strategies.
The factors identified by these two studies are virtually identical, although are expressed in slightly different terms. These elements are discussed in detail below.
Looking at the essential elements for effective primary prevention programs
1. Comprehensiveness: Embedding the program within the community setting
This element may also be described as a whole-of-community approach. It understands that for the program to achieve its objectives - particularly in the longer term (i.e., program impact and program sustainability) - it needs to be embedded within the larger context of the community. Comprehensiveness therefore relates to the inclusion of multiple strategies that target the same outcome and that are implemented at two or more levels at the same time (Casey & Lindhorst, 2009).
In the Flood et al. (2009) example of prevention education programs, a whole school approach ensured that respectful relationships programs were not isolated, vulnerable interventions within the school environment; that they could feasibly be sustained in the longer term by the school community; and that students participating in the programs were supported throughout the school to practice the skills and behaviours the programs aimed to effect.
2. Program logic: Connecting theory and action
Any sound multi-layered intervention will have a theoretically and empirically informed framework of what the problem is (what needs to be changed) and how it can be changed. Program logic refers to the rationale linking these steps.
Understanding the problem - Conceptual theory and addressing structural factors
The first part of the program logic element ties in with Casey and Lindhorst's (2009) finding that addressing structural factors is an important aspect of a successful program. In relation to sexual assault, a theoretical framework is particularly relevant. Gender-based violence requires consideration of a feminist-informed ecological model because sexual assault is recognised as having a base in social structures that perpetuate gender role models and gender inequity.
Socio-cultural feminist approaches are central to a robust conceptual understanding of the problem of sexual assault, since "feminist research … provides the most comprehensive and credible account of the causes and consequences of relationship and family violence" (Flood et al., 2009, p. 34). The current evidence about sexual assault is clear that:
- sexual assault is part of the spectrum of behaviours that constitute violence against women;
- perpetrators are typically male and located within survivors' familial, social, collegial, or romantic networks;
- sexual assault is located at the intersection of gender, power and inequality;
- attitudes, beliefs and social norms about sexuality and gender can facilitate and condone sexual assault; and
- all levels of the social order - including social and structural levels - have a role in sexual assault prevention (Centers for Disease Control and Prevention, 2004; VicHealth, 2007; World Health Organisation, 2002)
These findings mean that effective primary prevention needs to address the fundamental links between gendered power relations, inequality, and forms of violence against women. Efforts in prevention need to challenge culturally structured beliefs and norms about heterosexuality, seduction, masculinity and femininity, which are expressed at all levels of the socio-ecological model. As such, successful programs need to:
- move beyond rape-avoidance training for women;
- move beyond addressing individual beliefs and perceptions about gender;
- avoid focusing on risk factors, such as alcohol consumption and drug taking, in isolation from notions of masculinity, femininity, and peer relationships; and
- reflect the overlap and interconnection between sexual assault and domestic/family violence.
Change theory - How will the program achieve its goals?
The second aspect of a program being based on theoretical logic, as both the Flood et al. (2009) study and the Casey and Lindhorst (2009) study identified, is the need for prevention work to be premised on clearly theorised rationales for the particular prevention activities, not just on what seems logical or what has always been done. Overall, the purpose of a primary prevention intervention is to reduce the incidence of sexual violence in a community by changing people's behaviours. How will a particular intervention do this? It appears that few programs identify their theory of change (i.e., how will these activities lead to the desired changes?): "many simply assume that their efforts to provide information or improve attitudes will lessen young people's involvement in violence perpetration or victimisation (Flood et al., 2009, p. 35). What is required is an explicit theory of change that links prevention activities to theory about the causes of the problems and the theory of behavioural or community change (Casey & Lindhorst, 2009).
See Box 1 for examples of widely recognised theoretical models of how successful change happens.
Box 1: Examples of successful change theories
Prochaska and DiClemente's Change Theory: conceptualises behaviour change as a staged process. It is visualised as a cyclical process with individuals going through various stages in their change journey: pre-contemplation; contemplation; preparation for action; and action and maintenance (Prochaska, Wright, & Velicer, 2008).
Social Cognitive Theory: describes the relationship between an individual's beliefs and their behaviour in that people select, react to, and learn from experiences and can - through a process of self-monitoring, self-guidance and corrective self-reactions - implement change (Webb, Sniehotta, & Michie, 2010).
Theory of Reasoned Action and Planned Behaviour: proposes that behavioural intentions are a function of attitudes and perceived approval of important others. This means that changes in behaviour follow from changes in the beliefs that influence behaviour (Webb et al., 2010).
3. Effective delivery
The effective delivery of primary prevention programs is an important consideration in program design. Casey and Lindhorst (2009) identified contextualised programming, addressing structural factors (as discussed above), and health and strengths promotion as key elements in effective interventions. Contextualised programming identifies and responds to localised attitudes and perspectives and work within those perceptions to ensure relevance and acceptance to participants and other stakeholders. For example, attitudes about sex, gender, and intimate partnerships may vary in different cultural communities; therefore, sexual violence prevention needs to be aware of the differences and operate with these views in mind.
In Flood et al.'s (2009) discussion of effective program delivery in an educational setting, the factors identified correlated with the health and strengths promotion identified by Casey and Lindhorst (2009). That is, positive shifts in attitudes and behaviours are more sustainable in environments that feature positive role modelling, social support, and pro-social activities. One example that Casey and Lindhorst used was that of bystander interventions which are seen as a capacity building approach because they work to empower bystanders to achieve skills to intervene and challenge incidents of violence or attitudes that reflect gender discrimination. This type of approach is building positive skills in supportive environments with a focus on pro-social activity such as enhancing positive relationships between men and women. Flood et al. (2009) similarly identified part of effective delivery as including capacity building, engagement, and focus on the environment and changing social norms as aspects of effective delivery.
4. Relevant and socially inclusive practice
Casey and Lindhorst (2009) found that effective multi-level prevention programs involve partnering with the community in identifying change strategies, thereby ensuring relevance in their application. Flood et. al., (2009) similarly identified relevant and socially inclusive practice as an important aspect of successful programs. Their work indicated that programs should be:
- relevant - that is, informed by knowledge of target groups or population and local contexts;
- inclusive and culturally sensitive; and
- involve consultation with representatives or leaders from the population groups participating in the program where appropriate.
Casey and Lindhorst (2009) discussed the need to ensure local experiences, beliefs, language, and social constraints are included to ensure that prevention language and programming can mirror these.
5. Impact evaluation: An issue for multi-level primary intervention
Casey and Lindhorst (2009) noted that "no rigorous evaluations of sexual violence-oriented social norms campaigns appear in the [US] literature" (p. 105) and that there is limited empirical evidence of the efficacy of social norms campaigns in relation to sexual violence. However, they also noted that there is a glaring need for evaluations of these types of primary prevention programs.
Flood et al. (2009) identified a comprehensive evaluation as an essential component of an effective primary prevention education-based program. They indicated that such an evaluation should: reflect program framework and logic; include evaluation of impact or outcomes; and include a process for dissemination of findings to add to the violence prevention knowledge base.
There will be challenges in evaluating mutli-level, cross-disciplinary strategies such as those required for sexual assault primary prevention. The need for a number of stakeholders - often with different perspectives, resources and agendas - to work together to agree on an evaluation design that is useful and acceptable to all will require substantial effort and negotiation.
In addition, the nature of sexual assault and entwined issues of ethics, privacy, under-reporting and trauma make some traditional evaluation methods inapplicable or at the very least, more difficult to utilise in application to sexual assault prevention programs.
Although beyond the scope of this paper, and worthy of attention as a separate issue, some of the challenges evaluators face include issues such defining indicators of success or effectiveness. For example, how could nebulous concepts such as "improved gender equity" or "improved relationships" be measured?
The current climate of stringent, quantifiable accountability seems to demand measurement in quantitative terms but the nature of conceptually difficult social change objectives such as "gender equity" may preclude the use of traditional quantitative measurement and create evaluation scenarios that require much more complexity and nuanced analysis than in other areas where success or failure can be more objectively measured.
As policy and funding bodies operate in ever-more fiscally restrained environments, what measures are appropriate to quantify accountability, for example, how long is long enough to measure change? What is reasonable to expect from a behaviour change program and what can be learnt from so-called "failure"?
The efficacy of primary prevention and of accompanying evaluation will continue to develop as an issue while sexual violence aetiology continues to indicate the need for multi-level and structural interventions. ACSSA aims to consider the issues around complex, multi-level evaluation further in forthcoming publications.
Conclusion
While the evidence base favours primary prevention as the most efficient and effective strategy in the prevention of sexual assault, there is still little actual, evaluated program information on how to best undertake this. In addition, the proliferation of programs identifying as primary prevention can be misleading. How can policy-makers and funders be certain that the programs identified for funding actually do constitute primary prevention? A key feature is that primary prevention must move beyond only working to change attitudes or improve knowledge about sexual assault. It must target behaviour change that will result in lower levels of sexual violence. The multi-level nature of these type of interventions also go towards tackling the inherent complexity of social factors that combine to enable a negative social phenomena such as sexual violence. By clarifying and generating a better understanding of what exactly is and what isn't primary prevention, policy development sectors and program funders can be more certain that particular programs and interventions are correctly targeted.
Evidence from other fields of public health indicates that multi-level interventions that simultaneously facilitate shifts at a number of levels - including policy or regulatory levels, as well as among communities or peers and individuals - are the most effective (Casey & Lindhorst, 2009; Schensul, 2009). As such, prevention programing and policy should prioritise these interventions and acknowledge the features identified that create successful program design. Some examples of successful strategies that can be adapted across different settings include those aimed at social norms changes and bystander development approaches.
Although key strategies such as these may be transferable, what is clear from this discussion on effective design in primary prevention and from the literature is that specific interventions will need customising when transferring from one community to the next, or from one setting to another. The need for a contextual and community-informed approach is likely to mean that each intervention should be crafted with the characteristics of its setting and audience clearly at the forefront. The dynamic nature of communities and complex systems means that change occurs in different ways and at different speeds (Schensul, 2009). This has implications for policy and program delivery in that the unique nature of each setting and community audience being targeted must be acknowledged and involved. There cannot be a "one-size fits all" program, particularly when considering the multiple social causes of sexual and other forms of gendered violence.
Although evaluations of multi-level preventative interventions in sexual assault are limited, literature from other fields indicates that an approach that is contextualised and community-centred offers the most promising approaches. An intervention that does not capitalise on local knowledge may be considered irrelevant to those in the front-line of problem solving, such as teachers, service delivery workers or policy developers, because it doesn't incorporate this knowledge or perhaps addresses a problem they don't see as primarily important (Schensul, 2009). Frameworks that acknowledge that multi-level interventions are operating in dynamic environments will be the most useful. In order to evaluate the sustainability of behaviour change over time, consideration must be given to the changing and dynamic nature of these environments.
This Wrap has considered various elements that must be present in order for sexual assault prevention programs to be effective and provides quite specific guidance in identifying what constitutes primary prevention. Consideration of the primary prevention literature as it relates to sexual assault and prevention of violence against women also highlights the need for more evaluations of multi-level primary prevention programs to inform the evidence base and confirm the best approaches to tackling sexual violence prevention using primary prevention interventions. Currently there is a deficit of strong evaluation data to confirm the most effective programs and approaches to primary prevention of sexual violence at community levels.
References
- Access Economics. (2004). The cost of domestic violence to the Australian economy. Canberra: Office of the Status of Women.
- Australian Human Rights Commission. (2009). Accumulating poverty? Women's experiences of inequality over the lifecycle. Sydney: Australian Human Rights Commission.
- Bronfenbrenner, U. (1977). Toward an experimental ecology of human development. American Psychologist, 32(7), 513-531.
- Carmody, M. (2009). Conceptualising the prevention of sexual assault and the role of education (ACSSA Issues No. 10). Melbourne: Australian Institute of Family Studies Melbourne.
- Carmody, M., Evans, S., Krogh, C., Flood, M., Heenan, M., & Ovenden, G. (2009). Framing best practice: National standards for the primary prevention of sexual assault through education. Sydney: University of Western Sydney Australia.
- Casey, E., & Lindhorst, T. (2009). Toward a multi-level, ecological approach to the primary prevention of sexual assault: Prevention in peer and community contexts. Trauma, Violence and Abuse, 10(2), 91-114.
- Centers for Disease Control and Prevention. (2004). Sexual violence prevention: Beginning the dialogue. Atlanta: Centers for Disease Control and Prevention.
- DeGroff, A., & Cargo, M. (2009). Policy implementation: Implications for evaluation. In J. Hawe (Ed.), Knowledge utilisation, diffusion, implementation, transfer and translation: Implications for evaluation (New Directions for Evaluation, No. 124).0 Hoboken, NJ: Jossey-Bass...
- DeGue, S., Holt, M., Massetti, G., Matjasko, J., Tharp, A., & Valle, L. (2012). Looking ahead toward community-level strategies to prevent sexual violence. Journal of Women's Health, 21(1), 1-3.
- Equal Opportunity for Women in the Workplace Agency. (2012). Gender pay gap: The facts. Retrieved from <www.eowa.gov.au/Pay_Equity/Pay_Equity_Information.asp>.
- Family Health International. (2002). Behavior change: A summary of four major theories (PDF 122 KB). Retrieved from <www.fhi.org/nr/rdonlyres/ei26vbslpsidmahhxc332vwo3g233xsqw22er3vofqvrfjvubwyzclvqjcbdgexyzl3msu4mn6xv5j/bccsummaryfourmajortheories.pdf>
- Flood, M., Fergus, L., & Heenan, M. (2009). Respectful relationships education: Violence prevention and respectful relationships in Victorian schools. Melbourne: Department of Education and Early Childhood Development.
- Nastasi, B. K., & Hitchcock, J. (2009). Challenges of evaluating multilevel interventions. American Journal of Community Psychology, 43, 360-376.
- Prochaska, J., Wright, J., & Velicer, W. (2008). Evaluating theories of health behaviour change: A hierarchy of criteria applied to the transtheoretical model. Journal of Applied Psychology: An International Review, 57(4), 561-588.
- Quadara, A. (2010). Public media campaigns in responding to and preventing sexual assault: A summary of the research. ACSSA Aware, 24, 19-24
- Schensul, J. (2009). Community, culture and sustainability in a multilevel dynamic systems intervention science. American Journal of Community Psychology, 43, 241-256.
- Schwartz, J., & Lindley, L. (2009). Impacting sexism through social justice prevention: Implications at the person and environment levels. Journal of Primary Prevention, 30, 27-41.
- Sethid. D., Marais, S., Seedat, M., & Butchart, A. (2004). Handbook for the documentation of interpersonal violence prevention programmes. Geneva: Department of Injuries and Violence Prevention, World Health Organization.
- Trickett., E. J. (2002). Context, culture and collaboration in AIDS intervention: Ecological ideas for enhancing community impact. The Journal of Primary Prevention, 23(2), 157-174.
- Trickett., E. J. (2009). Multilevel community-based culturally situated interventions and community impact: An ecological perspective. American Journal of Community Psychology, 43, 257-266.
- VicHealth. (2004). The health costs of violence. Measuring the burden of disease caused by intimate partner violence. Carlton: Victorian Health Promotion Foundation.
- VicHealth. (2007). Preventing violence before it occurs: A framework and background paper to guide the primary prevention of violence against women in Victoria. Melbourne: VicHealth.
- VicHealth. (2012). The respect responsibility and equality program: A summary report on five projects that build new knowledge to prevent violence against women. Melbourne: Victorian Health Promotion Foundation.
- Webb, T., Sniehotta, F., & Michie, S. (2010). Using theories of behaviour change to inform interventions for addictive behaviour. Addiction, (105), 1879-1892.
- White Ribbon Foundation. (no date). What is primary prevention? (Fact Sheet 12). Retrieved from <www.whiteribbon.org.au/resources/facts>.
- World Health Organization. (2002). World report on violence and health: Summary. Geneva: WHO.
Antonia Quadara was the Coordinator and Liz Wall was a Research Officer with the Australian Centre for the Study of Sexual Assault at the Australian Institute of Family Studies.
Quadara, A., & Wall, L. (2012). What is effective primary prevention in sexual assault? Translating the evidence for action (ACSSA Wrap No. 11). Melbourne: Australian Centre for the Study of Sexual Assault, Australian Institute of Family Studies.
978-1-922038-09-8
11 October 2012