Children's exposure to parental and familial adversities
You are in an archived section of the AIFS website
May 2010
Download Family Matters article
Abstract
Clinical, community and retrospective studies are consistent in reporting the detrimental consequences of childhood adversity, including parental or family difficulties. The full extent of childhood adversity is difficult to estimate, however, due to a dearth of relevant information in general population surveys. This study estimated Australian children’s exposure to a range of parental and familial adversities using data from a national household survey. Parents’ responses from the Household, Income, and Labour Dynamics in Australia (HILDA) survey were used to estimate the number and proportion of families and children who were exposed to thirteen adversities. It was found that a substantial proportion of Australian children experience these adversities. For example, parents in 22.4% and 28.8% of families reported financial hardships and long-term health conditions respectively. Further, approximately one-fifth of children were exposed to three or more of the stressors we considered, indicating the tendency for adversities to co-occur. This study endorses the usefulness of household surveys to explore this issue, while highlighting the need for more comprehensive data collection at the population level. Such information can be used to better identify families in the general community who are at risk of poor social and health outcomes, including those who may not readily take up existing services.
The experience of trauma, loss and bereavement during childhood have both immediate and long-term consequences for health and general wellbeing. Children who have experienced the death of a parent or witnessed violent and/or traumatic events report more psychological symptoms than those who have not (Cerel, Fristad, Verducci, Weller, & Weller, 2006; Freeman, Mokros, & Poznanski, 1993). Children's exposure to violence has also been associated with lower IQ scores and poorer reading ability (Delaney-Black et al., 2002). Further, retrospective reports of physical and sexual abuse and maltreatment during childhood have consistently been linked to an increased likelihood of depression (Chapman et al., 2004; Diaz, Simantov, & Rickert, 2002; Molnar, Buka, & Kessler, 2001), suicidality (Mullen, Martin, Anderson, Romans, & Herbison, 1996), low self-esteem (Diaz et al., 2002; Mullen et al., 1996) and alcohol and drug use during adolescence and adulthood (Diaz et al., 2002; Molnar et al., 2001).
Risks to children's wellbeing are not, however, limited to "extreme traumatic stressors" (American Psychiatric Association, 2000) involving physical or sexual harm. Adverse life events or stressors that occur to a child's parent or within their familial context have also been connected to health, behavioural and social difficulties during childhood, and poorer outcomes later in life. For example, higher rates of depression (Kessler, Davis, & Kendler, 1997; Pirkola et al., 2005), substance use (Lieb, Isensee, Hofler, Pfister, & Wittchen, 2002) and lower educational attainment (Ensminger, Hanson, Riley, & Juon, 2003) have been found among adults who grew up with parents who experienced mental health problems. Children of divorced or separated parents also appear more likely to demonstrate poor health and risk behaviours during their adolescent and adult years (Rodgers, 1996; Sawyer et al., 2001). Moreover, cumulative and/or concurrent exposure to a number of these adversities (i.e., "multiple adversities") has been linked to exponentially poorer outcomes for children compared to their exposure to single adversities (Chapman et al., 2004; Felitti et al., 1998; Jaffee, Caspi, Moffitt, Polo-Tomas, & Taylor, 2007; Turner & Lloyd, 1995; Zubrick et al., 2005).
Described as "proximal stressors" (Zubrick, Silburn, Burton, & Blair, 2000), parental or familial adversities are thought to have these potential effects on children because the distress they cause parents may lead to them having difficulties engaging or spending time with their children (Menaghan, Kowaleski Jones, & Mott, 1997), or because these adversities represent or inhibit access to resources that are protective to children's wellbeing (Bradley & Corwyn, 2002; Brooks-Gunn & Duncan, 1997). This latter point also offers an explanation for the common co-occurrence of many of these adversities (e.g., parental unemployment may result in financial hardship), and the links between these adversities, children's mental health and families' experience of broader social exclusion (Hayes, Gray, & Edwards, 2008; Saunders, Naidoo, & Griffiths, 2007). "Social exclusion" refers to the lack or denial of a person's, family's or community's access to resources and services, including their inability to participate in "economic, social, cultural or political arenas" (Levitas et al., 2007, p. 25). For example, parental ill health may be a barrier to social and workforce participation and, consequently, financial resources. As discussed above, each of these adversities or stressors can affect children's mental health and wellbeing; however, their co-occurrence exemplifies and/or may lead to a more entrenched position of disadvantage that can be described as social exclusion. Due to the multiple and interdependent adversities experienced by these families, this position itself may affect children's mental health and inhibit their capacity to otherwise cope with single or fewer stressors.
The development and provision of services to address and prevent poor outcomes during childhood and subsequent adulthood first requires estimates for the extent of childhood adversities at the general population level, followed by the identification of individuals and groups who are most likely to experience these adversities (Allen Consulting Group, 2008; Department of the Prime Minister and Cabinet, Social Inclusion Unit, 2009; Dwyer, Nicholson, & Battistutta, 2003; Hayes et al., 2008). This information has been lacking in the Australian context due to a scarcity in nationwide surveys of children. A recent exception is Growing Up in Australia: The Longitudinal Study of Australian Children (LSAC), which collects information about a range of child outcomes using two cohorts of children who began the survey at ages < 12 months and 4-5 years (Gray & Smart, 2008; Sanson et al., 2002). The health, psychological distress, life stressors and financial wellbeing of children's primary parent and a second parent are also surveyed. Data from LSAC are currently available for children up to 7 years, with more to follow. To date, national estimates of the range of childhood adversities have been collated across several data sources that include information about one or some childhood adversities (Allen Consulting Group, 2008; Australian Institute of Health and Welfare [AIHW], 2005). This is problematic because sources typically refer to divergent samples and methods of data collection that prevent comparisons about the relative prevalence of different adversities or the experience of concurrent adversities. Further, data are often restricted to clinical settings that provide an underestimation of the true extent of adversity in the population by including only families who have sought or been referred to service providers.
An alternative method for estimating children's exposure to familial adversity in the absence of a dedicated, nationwide survey of Australian children across all ages is the use of data from population surveys of adults. Several population surveys of Australian adults have sought information about stressors, including ill health and negative life events such as relationship separation. When combined with additional data about respondents' parental status, the number of (respondents') children who are exposed to these stressors may be calculated. This method is not without limitations, however, because the majority of adult surveys have not been designed with this purpose in mind. A common sampling strategy, for example, involves the random selection of households or dwellings within geographic areas, followed by the random selection of one adult per household (Australian Bureau of Statistics [ABS], 1999, 2006). This means that only children of this adult can be considered, at the potential exclusion of other children in their household who do not have a biological relationship with the respondent. Moreover, this method negates the consequences of children's exposure to adversities experienced by other adults or parent figures in their household who are not surveyed. Estimates derived from these surveys may consequently underestimate the true number of children exposed to parental and familial adversities.
The use of "relationship grids" in household surveys overcomes the above limitation by collecting demographic information about all child and adult members of a surveyed household and the nature of the relationship between each member (Brandon, 2004). This method enables all children to be linked to all responding adults in their household whose actions and/or experiences may affect that child, including non-biological parents, grandparents, and older siblings in a parenting role. The ability to consider children living with non-biological parent figures is a significant strength because it is likely to be children's cohabitation with adults, rather than their biological relationship, that leaves them susceptible to the secondary consequences of parental adversities. Further, children living with non-biological parent figures - for example, in step- or blended families - may be more likely to experience adversity and poor outcomes than others (Amato & Keith, 1991). Australia's most recent longitudinal population survey, the Household, Income, and Labour Dynamics in Australia (HILDA) survey, has included a relationship grid for each surveyed household. In addition, the HILDA survey, seeks detailed personal data about workforce participation, health and various aspects of wellbeing from all consenting household members aged 15 and older. This distinguishes HILDA from other surveys that include relationship grids, such as the Australian Bureau of Statistics' Census, that do not collect information about a range of potential adversities.
A small number of authors have previously utilised the household structure of the HILDA survey to examine characteristics of Australian children, using data provided by responding adults and/or parents. Headey and Verick (2006) estimated the number of Australian children who live in households where no working-age adult is employed (jobless households). Brandon (2004) also identified the number of Australian children who lived with an unemployed adult, and explored this and other socio-economic outcomes according to the family structure of the household. De Vaus and Gray (2003, 2004) used detailed information about births to, and the relationship history of, mothers in the HILDA survey to estimate the proportion of children who had experienced parental separation at different stages of their childhood. The objective of the present study was to use the household structure of the HILDA survey to provide population-based estimates of the rate and number of Australian families with children, and individual children, who are currently exposed to a range of parental and familial adversities.
Methods
Sample
Data were from Wave 5 of the HILDA survey, which was conducted in 2005. This was the most recent available wave of data when this study began. The HILDA survey is a national household panel survey that is funded by the Australian Department of Families, Housing, Community Services and Indigenous Affairs (FaHCSIA), and has been conducted annually since 2001 by the Melbourne Institute of Applied Economic and Social Research (MIAESR). The original HILDA sample was derived using a multi-stage procedure that produced a representative sample of private Australian households and individuals (Watson & Wooden, 2002). Members of participating households have been traced at each subsequent wave of data collection (Goode & Watson, 2007).
The HILDA survey contains four questionnaires: a) the Household Form (HF), which records basic information about the composition of the household; b) the Household Questionnaire (HQ), which gathers demographic information about all household members and the relationships between them; c) the Person Questionnaire (PQ), which is conducted with all consenting household members aged 15 and older; and d) the Self-Completion Questionnaire (SCQ), which is sought from all respondents of the PQ. Data collected from the HF and HQ are used to create household-level datasets; data from the PQ and SCQ form person-level datasets. With the exception of the SCQ, all questionnaires are administered by trained interviewers. The dataset used for the present study combined data from Wave 5 household- and person-level datasets.
We used a sub-sample from Wave 5 of the HILDA survey that included households consisting of parent figures and children under 15 years old. This sub-sample was derived by: a) selecting adults (respondents aged 18 years and older) from the person-level dataset who lived in households with child(ren) less than 15 years old; and b) further excluding adults from this sample who were not parent figures to these children. This resulted in the exclusion of a small number of households (n = 19) in which only non-parent adults completed the PQ. The resulting sample included 3,630 parent figures, from 2,081 households. Responses to adversity-related items from parent figures within the same household were combined to form a household-level dataset. This dataset was used to identify the proportion of households in which one or more parent figures experienced each adversity. To estimate the rate of individual children who experienced parental and familial adversities, this household-level dataset was transposed so that the experiences of parent figures were mapped to each child in their household, that is, children became the unit of analyses. This child-level dataset included 3,862 children.
A slightly reduced sample was used to estimate adversities that were represented by items in the SCQ (see Table 1) because only 3,330 parents (of 3,506 children in 1,888 households) completed this additional survey component. This reduction is consistent with the response rate for the SCQ in the total HILDA sample (Goode & Watson, 2007). However, in addition to the aforementioned small number of households with non-responding parents, this meant that the presented estimates may slightly underestimate the prevalence of adversities. Finally, there was a very small amount of missing data for each of these adversities due to non-response by parents in up to 8 of the 1,888 households. Consequently, the denominator used to estimate the rate of each adversity in the SCQ varied slightly, and this is noted in the presentation of our results.
| Household adversity | Questionnaire | Period of time referenced |
|---|---|---|
| Environmental stressors | ||
| Parent(s) currently unemployed | PQ | Current |
| Parent(s) fired or redundant (job loss) | SCQ | Last 12 months |
| Household income < 50% of median (poverty) | HQ | Last financial year |
| 2+ financial hardships | SCQ | Since beginning of calendar year |
| Loss or separation | ||
| Parent(s) jailed in last 12 months | SCQ | Last 12 months |
| Parent(s) separated or divorced | PQ | Current |
| Parent(s) changed residences | SCQ | Last 12 months |
| Bereavement | ||
| Parent(s) spouse or child has died | SCQ | Last 12 months |
| Death of parent(s), close relative/family member | SCQ | Last 12 months |
| Poor health | ||
| Parent(s) currently has long-term health condition | PQ | Current |
| Parent(s) currently has MHI-5 score <= 50 | SCQ | Past 4 weeks |
| Parent(s) had serious injury/illness | SCQ | Last 12 months |
| Serious injury/illness in parent's family | SCQ | Last 12 months |
Notes: HQ = Household Questionnaire ; PQ = Person Questionnaire; SCQ = Self-Completion Questionnaire.
Measures
Defining parent figures
Intra-household relationships were captured in the HILDA survey using a relationship grid, which provides detailed information about the relationships between all household members. Our definition of "parent" included all adults who were the biological, step- and/or foster parents to children < 15 years in their household (n = 3,543). A small number of grandparents (n = 78) were also included, as were adult siblings of children who were not themselves a child or grandchild of another household member (i.e., other parent figures were not present; n = 9). This definition of "parent" encapsulates the varied composition of modern families and acknowledges that children's cohabitation with adults, rather than their biological relationship, leaves them susceptible to the secondary consequences of parental stressors.
Adversities
Adult respondents were asked about their experience of a range of personal and household adversities. Adversities considered in this study included four environmental stressors, three events of loss or separation, two experiences of bereavement, and four indicators of poor health. These adversities were selected on the basis of previous research on the sources of trauma and distress among children. Several of these adversities also correspond to local (Allen Consulting Group, 2008) and international (UNICEF, 2007) indicators of child health and wellbeing. Table 1 lists these thirteen adversities and indicates their source within the HILDA survey and the time period referenced by each item. We considered adversities at the household level to represent familial adversities because the vast majority (98%) of households with children in the present sample included only one family.
Household income was determined from items in the HQ and used to derive a measure of poverty - the first of two indicators of material adversity considered in this study. A measure of adjusted or "equivalised" household income was first created by dividing the household income by the number of adults and children in that household; a value of 1 was given for the first adult, 0.7 for additional adults and 0.5 for all children below the age of 15 years (Scutella & Smyth, 2005). A dichotomous variable was then created that identified households whose equalized income was less than 50% of the national median. This poverty threshold has previously been used both nationally (Allen Consulting Group, 2008; Scutella & Smyth, 2005) and internationally (Förster & D'Ercole, 2005).
Current unemployment, marital status and long-term health condition were determined from parents' responses to items in the PQ. All respondents in the current sample completed these items. Current unemployment status was derived from items on workforce participation, and defined as not working for pay but engaged in job searching. Respondents were asked to indicate their current martial status from a list of six options: married, separated (but not divorced), divorced, widowed, never married but living with someone in a relationship, and never married and not living with someone in a relationship. A dichotomous variable was created to represent people who were currently divorced or separated relative to all other options. Current long-term health condition was identified for parents who completed an item that listed 17 physical, neurological and emotional conditions. This item asked respondents if they "have any long-term health condition, impairment or disability (such as these) that restricts you in your everyday activities, and has lasted or is likely to last for 6 months or more".
The SCQ included a list of 21 stressful parental life events from which the presence of seven adversities was derived. These were: being fired or made redundant, changing residences, experiencing the death of a spouse or child, experiencing the death of a close relative/family member, having a serious injury/illness, and having a serious injury/illness in the family. These events were drawn from a scale developed by Holmes and Rahe (1967). Respondents were simply asked to indicate whether they had experienced each of these events in the past 12 months. The SCQ also included items for seven signs of financial hardship (e.g., going without meals, being unable to pay services bills) - our second indicator of material adversity. Responses to these items were summed to form a scale of hardship (Butterworth & Crosier, 2005). Reporting two or more of these events was considered indicative of significant financial hardship (Butterworth & Rodgers, 2006; Gill et al., 2006).
Respondents' mental health was measured in the SCQ using the Mental Health Index (MHI-5), which forms the mental health scale of the 36-item Short Form Health Questionnaire (SF-36; Ware & Sherbourne, 1992). The MHI-5 is a general measure of mental health, and includes two items for positive affect, and one each for depression, emotional control and anxiety. The depression and anxiety items have been shown to be strong predictors of diagnosable depression and anxiety disorders in the general Australian population (Gill, Butterworth, Rodgers, & Mackinnon, 2007). Respondents are asked to indicate the frequency of these psychological symptoms and feelings over the past four weeks on a 6-point Likert scale. Responses are then summed and transformed to a normalised scale of 0 to 100, where higher scores indicate the presence of positive emotional states. The MHI-5 has demonstrated satisfactory internal consistency and criterion validity in the HILDA survey (Butterworth & Crosier, 2004), and has proven an effective screening tool for mood disorders or severe depressive symptomatology in the general population of Germany and Japan (Rumpf, Meyer, Hapke, & John, 2001; Yamazaki, Fukuhara, & Green, 2005). In this study, parents were considered to be experiencing moderate to severe psychological distress if they reported a score of <= 50 on this scale (Butterworth & Rodgers, 2006; Gill et al., 2006).
A measure of multiple adversity was calculated to represent the total number of the 10 adversities experienced within each household and by each child. Three of the 13 adversities considered in this study, "parent fired in last 12 months", "parent has serious illness/injury in last 12 months" and household poverty, were not included in this sum, to avoid redundancy with "current unemployment", "parent has a long-term health condition" and financial hardship. Household poverty was used in place of financial hardship in our measure of multiple adversity because these two factors measure similar stressors, but the former is likely to be a more conservative indicator of material adversity. The estimates derived from this alternative measure were not notably different from those reported.
Approach to analyses
Estimates were sought for the proportion of Australian households with children < 15 years where one or more parent figures reported each adversity, and the proportion and number of Australian children exposed to these adversities (who live in these households). This was achieved using the household-level and child-level datasets described above, respectively. We used Complex Samples procedures in SPSS Version 15.0 to account for the HILDA sampling design when calculating these estimates, which were also weighted to reflect the Australian population of households or children. These weights are provided in the HILDA datasets and account for household and person (within-household) non-response (Goode & Watson, 2007).
Results
Sample characteristics
Table 2 displays the proportions of household/family types in our sample, and shows that the majority of children in this sample lived in households with an adult couple. A smaller proportion lived with a lone parent, and very few lived in households that included additional adults or multiple families. Most households included one or two children (83.4%) and two parent figures according to our criteria (69.0%). Only 2.0% of these households included more than two parent figures. These estimates of family structure are consistent with reports using other nationally representative samples of Australians (Trewin, 2003, 2004).
| Weighted proportion (%) | |
|---|---|
| Couple family with children < 15 years, without others | 74.2 |
| Couple family with children < 15 years, with other related | 1.7 |
| Couple family with children < 15 years, with other not related | 0.3 |
| Lone parent with children < 15 years, without others | 18.8 |
| Lone parent with children < 15 years, with other related | 1.8 |
| Lone parent with children < 15 years, with other not related | 0.5 |
| Multiple family household | 2.5 |
| Total number of observations | 2,108 |
Children exposed to parental and familial adversities
Table 3 displays estimates for the proportion of Australian households (with children) and number of children with one or more parent figure(s) who reported each of 13 adversities. Financial hardships in the household was the most common social/environmental stressor experienced by children (22.4% of households, or 23.6% of children), followed by another indicator of material wellbeing, household poverty (15.8% of households, or 17.2% of children). Consistent with national labour force estimates at the time of this HILDA survey (ABS, 2005), the rate of unemployment and recent job loss among parent figures was low. Very few Australian children lived with parents who had been recently jailed. Living with a parent figure who was separated from their partner or divorced was, however, relatively common (15.3% of children). In most cases, this partner is likely to be a parent of the child(ren) in this household and thus this figure provides an estimation of the number of children who have experienced separation from a parent and the secondary consequences of this separation for the parent with whom they currently live.
| Parental/familial adversity | % households (SE) | % children (SE) | No. of children (95% CI) |
|---|---|---|---|
| Environmental stressors | |||
| 1. Parent(s) currently unemployed | 4.9% (0.5%)1 | 4.8% (0.6%)3 | 189,568 (141,377-237,758) |
| 2. Parent(s) fired or redundant (job loss) | 3.3% (0.4%)2 | 3.4% (0.4%)4 | 119,269 (87,909-150,628) |
| 3. Household income < 50% of median (poverty) | 18.2% (1.1%)1 | 20.8% (1.4%)3 | 821,293 (694,101-948,485) |
| 4. 2+ financial hardships | 22.4% (1.2%)2 | 23.6% (1.3%)4 | 832,439 (721,465-943,413) |
| Loss or separation | |||
| 5. Parent(s) jailed | 0.3% (0.1%)2 | 0.3% (0.1%)4 | 10,966 (789-21,144) |
| 6. Parent(s) separated/divorced | 16.0% (0.9%)1 | 15.3% (1.0%)3 | 604,258 (518,601-689,915) |
| 7. Parent(s) changed residences | 17.4% (0.9%)2 | 17.7% (0.9%)4 | 623,125 (545,576-700,674) |
| Bereavement | |||
| 8. Parent(s) spouse or child has died | 0.7% (0.3%)2 | 0.9% (0.5%)4 | 30,500 (-1,441-62,441) |
| 9. Death of parent(s) close relative/family member | 15.5% (1.0%)2 | 16.5% (1.1%)4 | 580,482 (492,277-668,686) |
| Poor health | |||
| 10. Parent(s) has long-term health condition | 28.8% (1.2%)1 | 28.1% (1.3%)3 | 1,107,658 (983,725-1,231,592) |
| 11. Parent(s) has MHI-5 score <= 50 | 16.2% (1.0%)2 | 16.6% (1.0%)4 | 586,904 (502,176-671,632) |
| 12. Parent(s) had serious injury/illness | 10.8% (0.8%)2 | 10.6% (0.9%)4 | 373,673 (310,701-436,645) |
| 13. Serious injury/illness in parent's family | 24.2% (1.1%)2 | 24.5% (1.1%)4 | 860,804 (761,857-959,750) |
Notes: SE = standard error; CI = confidence interval. 1 Based on a sample of 2,081 households. 2 Based on a sample of 1,880 to 1,883 households. 3 Based on a sample of 3,862 children (weighted frequency = 3,947,112). 4 Based on a sample of 3,484 to 3,497 children (weighted frequency = 3,514,343 to 3,532,352). The total number of children estimated in the Australian population at the time of Wave 5 of the HILDA Survey was 4,003,975. Parent data was available for an estimated 3,947,112 of these, or up to 3,526,402 on SCQ items. The estimated numbers of children living with these adversities are a proportion of these sub-samples of children with available data and therefore likely underestimate the total number of children living with these adversities.
While a very small proportion of children (0.9%) were living with a parent who had experienced the death of a spouse (likely to be the child's parent) or other child (likely to be the child's sibling) in the last 12 months, exposure to parental bereavement due to the death of a close relative or friend was much more common (16.5% of children). Exposure to parental ill health was the most widespread of all considered adversities. Of households with children, 28.8% included a parent(s) with a long-term health condition (affecting 28.1% of children) and 16.2% of households included a parent(s) with moderate to severe levels of psychological distress (16.6% of children). There is likely to be some overlap between this figure for parents' long-term health conditions and the 10.8% of households with parent figures who reported serious injury or illness in the last 12 months. Table 3 also displays the estimated number of Australian children aged 14 years and younger who, in 2005, were living in households where one or more parent figures reported these adversities. For example, an estimated 189,568 children were living in a household with at least one unemployed parent figure.
Multiple adversities
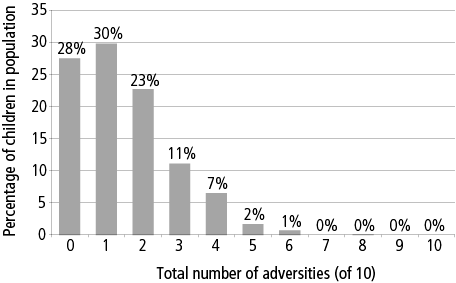
Figure 1 displays the total number of 10 adversities experienced by Australian children. This total excludes three potentially redundant adversities so as not to overestimate the prevalence of multiple adversities. More children had been exposed to (at least) one parental or household adversity (29.8% of children) than none (27.5% of children), and a substantial proportion (22.7%) of children experienced two of these adversities. Exposure to three or more adversities was less common, although, in total, these children comprised 20.0% of the population.
Figure 1: Number of adversities experienced by Australian children, of 10 non-redundant adversities
Discussion
Principle findings
A substantial proportion of Australian children are exposed to proximal stressors via the experiences of their parents. It is estimated that, in 2005, 16.6% of children in the population lived in households with parent figures who experienced psychological distress. Parents' mental health problems are believed to have potentially detrimental effects on children if the parents' symptoms prevent children's access to services and social networks (Department of Human Services, 2007) and/or affect parent-child relationships that are important for the child's development (Lancaster, 1999). These children are also more likely to experience depression and substance abuse as adults (Kessler et al., 1997; Lieb et al., 2002; Pirkola et al., 2005). We also found that 23.6% of Australian children lived in households that had recently experienced financial hardship and 17.2% lived in households whose income is considered below the poverty line. Material disadvantage has also been linked to children's physical and mental health as well as their academic success (Bradley & Corwyn, 2002; Brooks-Gunn & Duncan, 1997; Costello, Farmer, Angold, Burns, & Erkanli, 1997; Duncan, Yeung, Brooks-Gunn, & Smith, 1998; McLeod & Shanahan, 1996). Associations between other childhood stressors considered in this study - including parental separation (Rodgers, 1996) and unemployment (Christoffersen, 1994) - and poor outcomes such as depression, low self-esteem and substance use have also been demonstrated. Material disadvantage has also been linked to children's physical and mental health as well as their academic success (Bradley & Corwyn, 2002; Brooks-Gunn & Duncan, 1997; Costello, Farmer, Angold, Burns, & Erkanli, 1997; Duncan, Yeung, Brooks-Gunn, & Smith, 1998; McLeod & Shanahan, 1996). Associations between other childhood stressors considered in this study - including parental separation (Rodgers, 1996) and unemployment (Christoffersen, 1994) - and poor outcomes such as depression, low self-esteem and substance use have also been demonstrated.
A small number of studies have previously considered the prevalence of similar childhood adversities in the Australian population. These studies have typically focused on a single stressor rather than a range of childhood adversities, and used methods that did not account for children's exposure to non-biological parent figures. However, we compared the results of these studies to the present estimates as a means of assessing the validity of our findings. The present study found that 15.3% of Australian children lived with at least one parent who was separated or divorced in 2005. This figure is likely to be a slight underestimation of all children who have experienced parental separation because it is based on current living arrangements only, and thus excludes children whose parents have remarried. This in mind, our estimate is largely consistent with previous studies of parental separation. Slee (1993) estimated that 13.4-14.7% of school children aged 5-13 years had experienced parental separation in 1993 and, more recently, DeVaus and Gray (2003) estimated that 24% of Australian children aged 12 years in 2001 will have spent time living without a biological parent.
Using information from the National Survey of Mental Health and Wellbeing and the Family Characteristics Survey, Maybery, Reupert, Patrick, Goodyear, and Crase (2005) estimated that 21.7-23.5% of Australian children live with a parent who has a mental illness. This is similar to retrospective estimates by Rosenman and Rodgers (2004), who found that 17.8% and 23.8% of adults in a large general community sample reported that their father and mother, respectively, suffered "nervous or emotional trouble or depression" during their childhood. The present estimate that 16.6% of children in the HILDA survey were living with one or more parents with psychological distress is slightly below these previous figures. This is not unexpected given the use of divergent indicators of mental health and the shorter reference period used here. The MHI-5 refers to individuals' symptoms and feelings in the past 4 weeks, whereas Maybery et al.'s and Rosenman and Rodgers' estimates were derived from 12-month prevalence rates of mental illness and total childhood respectively.
Scutella and Smyth (2005) used data from earlier waves of the HILDA survey to estimate that 16.7%, 15.8% and 14.5% of all Australian children aged 0-17 years lived in households with incomes below the poverty line in 2001, 2002 and 2003 respectively. Förster and d'Ercole (2005) reported that 11.6% of Australian children in the same age range lived in households that experienced poverty in 1999, a rate that was higher than 10 other OECD countries. Estimates derived from the ABS 2002-03 Survey of Income and Housing indicated that 21.9% of children below the age of 15 years lived in households whose income was in the lowest quintile at that time (i.e., in the lowest 20% of distribution of Australian household incomes; AIHW, 2005). The criterion for poverty used in this AIHW report (less than 50% of the median household income) was the same as that used for the present study. Unlike the present study, however, Scutella and Smyth's (2005) and Förster and d'Ercole's (2005) estimates included children up to the age of 17 years and those in households without responding parents. Methods used to equalise household incomes also differed across the cited studies above. These discrepancies may account for the somewhat higher poverty rate estimated from the present study and ABS data.
One-fifth of Australian children in our HILDA sample had been exposed to three or more of ten parental and familial adversities we investigated. This is a conservative estimate given that a small proportion of surveyed parents did not respond to the adversity items and because we took care to exclude potentially redundant adversities. Multiple adversities were examined in this study because the likelihood of poor outcomes for children who experience multiple and/or concurrent stressors is known to be greater than those who experience single adverse events (Anda et al., 2006; Briere, Kaltman, & Green, 2008; Cerel et al., 2006; Chapman et al., 2004; Costello, Erkanli, Fairbank, & Angold, 2002; Felitti et al., 1998; Kessler et al., 1997; Rutter, 1993; Tiet et al., 1998; Zubrick et al., 2005). It is difficult, however, to compare this estimate to other studies that have considered the prevalence of multiple adversities because each of them have tested a different range of adversities. Slee (1993), for example, found that 25.1% of urban Australian primary school children had experienced three or more of eight "serious" events, including parental separation and death. Kessler et al. (1997) found that 35.0% of British adults in a general population sample retrospectively reported three or more of 25 childhood adversities, ranging from parental separation to sexual abuse. The prevalence of multiple adversities will also vary substantially with characteristics of the sampled population. For example, 69.6% of primary carers of Aboriginal children in Western Australia reported experiencing three or more of 14 stressful life events, including financial hardship and the death of a family member (Zubrick et al., 2005). Comparative estimates for other adversities that were considered in this study were either not available or not informative due to even wider discrepancies in the methods used to measure these adversities.
Strengths and weaknesses of the study
Weaknesses of this study relate to methodological limitations that arise because the HILDA survey was not specifically designed to measure childhood adversity. The first is that several adversities examined here refer to different time frames. For example, parental unemployment refers to employment status at the time of interview, whereas parental illness/injury included any instance in the 12 months prior to the survey. Had all adversities been estimated in the latter method, we would expect higher rates of parental unemployment, psychological distress and financial hardship than those presented. These differences do not invalidate estimates; rather, some caution must be taken when describing the relative prevalence of adversities and multiple adversities. Secondly, we were unable to estimate the prevalence of several important proximal stressors on children, such as exposure to family violence or conflict, as well as direct instances of trauma, including child abuse and neglect, because this information was not collected in the HILDA survey.
These shortcomings in mind, this study has nonetheless highlighted the capacity of existing data sources on adults and families to provide valuable information about children's exposure to adversity in the absence of child-focused surveys on this topic. It is also the first study to provide national estimates of this range of childhood adversities using a single sample. A further strength of these estimates is that they are based on an inclusive definition of "parent figure" that is not limited to a biological or nuclear concept of family. This definition recognises that children's cohabitation with parent figures - rather than their biological relationship - leaves them susceptible to the secondary consequences of parental and familial adversities. Estimates restricted to biological relationships are likely to underestimate the true extent of childhood adversity and be unrepresentative of many Australian households that include step- and blended families.
Meaning of the study
With the prevention and early intervention of mental health problems high on the policy agenda (Council of Australian Governments, 2006; Department of Health and Aged Care, 2000a), risk factors for children's mental health and wellbeing must be targets for intervention (Department of Health and Aged Care, 2000a; Murray, 2005; Zubrick et al., 2000). Parental and familial stressors are consistently linked to poorer developmental, academic and health outcomes during childhood and later adulthood. This is particularly true for children who experience multiple adversities (e.g., Zubrick et al., 2005). Prevention and intervention begins with knowledge about the extent of these risk factors in the general community (Department of Health and Aged Care, 2000b; Dwyer et al., 2003; Murray, 2005) and thus the extent of need. Such estimates also provide a baseline for measuring change over time, including changes that are due to policies and interventions. The present study has shown that children's exposure to several parental and familial adversities is widespread. Not all of these children will demonstrate poorer outcomes than those who experience no adversity (Rutter, 2000, 2007). However, the prevalence of this exposure in the general community suggests the need for population-level approaches (Department of Health and Aged Care, 2000b; Raphael, 2000) and provides justification for the continuation of existing strategies, such as the development and dissemination of guidelines for service providers to children of parents with mental illness (Australian Infant Child Adolescent and Family Mental Health Association, 2001; see also Council of Australian Governments, 2006).
Closely linked to these policy priorities for mental health is Australia's goal to reduce the extent and causes of social exclusion among children and families (Department of the Prime Minister and Cabinet, Social Inclusion Unit, 2009; National Institute for Mental Health in England, 2006). Several of the adversities measured in this study (e.g., financial hardship and parental unemployment) are themselves indicators and/or contributors to social exclusion (Hayes et al., 2008; Saunders et al., 2007). Children and families who are most likely to experience social exclusion are those 20% who are exposed to multiple, co-occurring adversities. Multiple adversities are thought to be indicative of "deep" social exclusion, a circumstance that is considered to be entrenched and require multiple and collaborative solutions (Hayes et al., 2008). Not surprisingly, though most importantly, these children are also known to be at greater risk of poor mental health outcomes, relative to those who experience one or fewer stressors (Chapman et al., 2004; Felitti et al., 1998; Jaffee et al., 2007; Turner & Lloyd, 1995; Zubrick et al., 2005). Future research will extend the estimates presented in this study to identify the characteristics of families who are most at risk of multiple adversities and their consequences. This will provide valuable information for the targeting of policies that are currently being developed to prevent mental health problems and address social exclusion (Department of the Prime Minister and Cabinet, Social Inclusion Unit, 2009).
Summary and future directions
Future research will aim to identify the characteristics of those families who are most at risk of adversity; that is, those who are more likely to experience specific and multiple adversities. This information will facilitate more targeted intervention and research efforts in the policy priority areas of mental health and social inclusion. While the HILDA survey has enabled us to provide estimates for the prevalence of a range of parental and familial stressors, information about other adversities - childhood trauma, abuse and neglect - and children's associated outcomes was not available in this survey. Moreover, the absence of information about children's health and wellbeing prevented this study from demonstrating the associations between these outcomes and familial adversity. This again highlights the need for further population-based assessments of childhood adversity alongside children's mental health (Allen Consulting Group, 2008; Trewin, 2006), and the importance of current data collection efforts such as the Longitudinal Study of Australian Children (Gray & Smart, 2008; Sanson et al., 2002) and the Longitudinal Study of Indigenous Children (FaHCSIA, 2009). The sensitivities and complexities involved in measuring children's experiences using traditional child- and parent-based surveys, and the demonstrated efficacy of using family-based samples for this purpose in the present study, indicates that such estimates may be achievable via the inclusion of relevant items in existing family-level surveys.
References
- Allen Consulting Group. (2008). The ARACY Report Card on the wellbeing of young Australians: Technical report. Canberra: ARACY.
- Amato, P. R., & Keith, B. (1991). Parental divorce and the well-being of children: A meta-analysis. Psychological Bulletin, 110(1), 26-46.
- American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders: DSM-IV-TR (4th, text revision ed., pp. 463). Washington, DC: APA.
- Anda, R. F., Felitti, V. J., Bremner, J. D., Walker, J. D., Whitfield, C., Perry, B. D., et al. (2006). The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience, 256(3), 174-186.
- Australian Bureau of Statistics. (1999). National Survey of Mental Health and Wellbeing of Adults: Users' guide (Cat. No. 4327.0). Canberra: ABS.
- Australian Bureau of Statistics. (2005). Labour force, Australia, Feb 2005 (Cat. No. 6202.0). Canberra: ABS.
- Australian Bureau of Statistics. (2006). General Social Survey: User guide (Cat. No. 4159.0.55.002). Canberra: ABS.
- Australian Infant Child Adolescent and Family Mental Health Association. (2001). Children of Parents Affected by a Mental Illness Scoping Project. Canberra: Mental Health and Special Programs Branch, Department of Health and Aged Care.
- Australian Institute of Health and Welfare. (2005). A picture of Australia's children (AIHW Cat. No. PHE 58). Canberra: AIHW.
- Bradley, R. H., & Corwyn, R. F. (2002). Socioeconomic status and child development. Annual Review of Psychology, 53, 371-399.
- Brandon, P. D. (2004). Identifying the diversity in Australian children's living arrangements. Journal of Sociology, 40(2), 179-192.
- Briere, J., Kaltman, S., & Green, B. L. (2008). Accumulated childhood trauma and symptom complexity. Journal of Traumatic Stress, 21(2), 223-226.
- Brooks-Gunn, J., & Duncan, G. J. (1997). The effects of poverty on children. The Future of Children, 7(2), 55-71.
- Butterworth, P., & Crosier, T. (2004). The validity of the SF-36 in an Australian national household survey: Demonstrating the applicability of the Household Income and Labour Dynamics in Australia (HILDA) survey to examination of health inequalities. BMC Public Health, 4(44), 1-11.
- Butterworth, P., & Crosier, T. (2005). Deriving a measure of financial hardship from the HILDA survey. Australian Social Policy, 2005, 1-12.
- Butterworth, P., & Rodgers, B. (2006). Concordance in the mental health of spouses: Analysis of a large national household panel survey. Psychological Medicine, 36(5), 685-697.
- Cerel, J., Fristad, M. A., Verducci, J., Weller, R. A., & Weller, E. B. (2006). Childhood bereavement: Psychopathology in the 2 years postparental death. Journal of the American Academy of Child and Adolescent Psychiatry, 45(6), 681-690.
- Chapman, D. P., Whitfield, C. L., Felitti, V. J., Dube, S. R., Edwards, V. J., & Anda, R. F. (2004). Adverse childhood experiences and the risk of depressive disorders in adulthood. Journal of Affective Disorders, 82(2), 217-225.
- Christoffersen, M. N. (1994). A follow-up study of longterm effects of unemployment on children: Loss of self-esteem and self-destructive behavior among adolescents. Childhood, 2(4), 212-220.
- Costello, E. J., Erkanli, A., Fairbank, J. A., & Angold, A. (2002). The prevalence of potentially traumatic events in childhood and adolescence. Journal of Traumatic Stress, 15(2), 99-112.
- Costello, E. J., Farmer, E. M., Angold, A., Burns, B. J., & Erkanli, A. (1997). Psychiatric disorders among American Indian and white youth in Appalachia: The Great Smoky Mountains Study. American Journal of Public Health, 87(5), 827-832.
- Council of Australian Governments. (2006). National Action Plan on Mental Health 2006-2011. Canberra: COAG.
- De Vaus, D., & Gray, M. (2003). Family transitions among Australia's children. Family Matters, 61, 10-17.
- De Vaus, D., & Gray, M. (2004). The changing living arrangements of children, 1946-2001. Journal of Family Studies, 10(1), 9-19.
- Delaney-Black, V., Covington, C., Ondersma, S., Nordstrom-Klee, B., Templin, T., Ager, J., et al. (2002). Violence exposure, trauma, and IQ and/or reading deficits among urban children. Archives of Pediatrics & Adolescent Medicine, 156(3), 280-285.
- Department of Families, Housing, Community Services and Indigenous Affairs. (2009). Footprints in Time: The Longitudinal Study of Indigenous Children (LSIC). Canberra: FaHCSIA. Retrieved 15 November 2009, from <www.fahcsia.gov.au/sa/indigenous/progserv/families/lsic/Pages/default.aspx>.
- Department of Health and Aged Care. (2000a). National Action Plan for Promotion, Prevention and Early Intervention for Mental Health. Canberra: Mental Health and Special Programs Branch, Department of Health and Aged Care.
- Department of Health and Aged Care. (2000b). Promotion, prevention and early intervention for mental health: A monograph. Canberra: Mental Health and Special Programs Branch, Department of Health and Aged Care.
- Department of the Prime Minister and Cabinet, Social Inclusion Unit. (2009). The Australian Public Service policy design and delivery toolkit. Canberra: Commonwealth of Australia.
- Diaz, A., Simantov, E., & Rickert, V. I. (2002). Effect of abuse on health: Results of a national survey. Archives of Pediatrics & Adolescent Medicine, 156(8), 811-817.
- Duncan, G. J., Yeung, W. J., Brooks-Gunn, J., & Smith, J. R. (1998). How much does childhood poverty affect the life chances of children? American Sociological Review, 63(3), 406-423.
- Dwyer, S. B., Nicholson, J. M., & Battistutta, D. (2003). Population level assessment of the family risk factors related to the onset or persistence of children's mental health problems. Journal of Child Psychology and Psychiatry and Allied Disciplines, 44(5), 699-711.
- Ensminger, M. E., Hanson, S. G., Riley, A. W., & Juon, H. S. (2003). Maternal psychological distress: Adult sons' and daughters' mental health and educational attainment. Journal of the American Academy of Child and Adolescent Psychiatry, 42(9), 1108-1115.
- Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., et al. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245-258.
- Förster, M., & D'Ercole, M. (2005). Income distribution and poverty in OECD countries in the second half of the 1990s (OECD Social, Employment and Migration Working Papers). Paris: OECD.
- Freeman, L. N., Mokros, H., & Poznanski, E. O. (1993). Violent events reported by normal urban school-aged children: Characteristics and depression correlates. Journal of the American Academy of Child and Adolescent Psychiatry, 32(2), 419-423.
- Gill, S. C., Butterworth, P., Rodgers, B., Anstey, K. J., Villamil, E., & Melzer, D. (2006). Mental health and the timing of men's retirement. Social Psychiatry and Psychiatric Epidemiology, 41(7), 515-522.
- Gill, S. C., Butterworth, P., Rodgers, B., & Mackinnon, A. (2007). Validity of the Mental Health Component Scale of the 12-item Short-Form Health Survey (MCS-12) as measure of common mental disorders in the general population. Psychiatry Research, 152(1), 63-71.
- Goode, A., & Watson, N. (Eds.). (2007). HILDA user manual: Release 5.0. Melbourne: Melbourne Institute of Applied Economic and Social Research.
- Gray, M., & Smart, D. (2008). Growing Up in Australia: The Longitudinal Study of Australian Children is now walking and talking. Family Matters, 79, 5-13.
- Hayes, A., Gray, M., & Edwards, B. (2008). Social inclusion: Origins, concepts and key themes. Canberra: Australian Institute of Family Studies.
- Headey, B., & Verick, S. (2006). Jobless households: Longitudinal analysis of the persistence and determinants of joblessness using HILDA data for 2001-03 (Melbourne Institute Report No. 7). Melbourne: Melbourne Institute of Applied Economic and Social Research.
- Holmes, T. H., & Rahe, R. H. (1967). The Social Readjustment Rating Scale. Journal of Psychosomatic Research, 11(2), 213-218.
- Jaffee, S. R., Caspi, A., Moffitt, T. E., Polo-Tomas, M., & Taylor, A. (2007). Individual, family, and neighborhood factors distinguish resilient from non-resilient maltreated children: A cumulative stressors model. Child Abuse & Neglect, 31(3), 231-253.
- Kessler, R. C., Davis, C. G., & Kendler, K. S. (1997). Childhood adversity and adult psychiatric disorder in the US National Comorbidity Survey. Psychological Medicine, 27(5), 1101-1119.
- Lancaster, S. (1999). Being there: How parental mental illness can affect children. In V. Cowling (Ed.), Children of parents with mental illness (Vol. 1, pp. 14-34). Melbourne: Australian Council for Educational Research.
- Levitas, R., Pantazis, C., Fahmy, E., Gordon, D., Lloyd, E., & Patsios, D. (2007). The multi-dimensional analysis of social exclusion. London: Social Exclusion Task Force.
- Lieb, R., Isensee, B., Hofler, M., Pfister, H., & Wittchen, H. U. (2002). Parental major depression and the risk of depression and other mental disorders in offspring: A prospective-longitudinal community study. Archives of General Psychiatry, 59(4), 365-374.
- Maybery, D., Reupert, A., Patrick, K., Goodyear, M., & Crase, L. (2005). VicHealth research report on children at risk in families affected by parental mental illness. Melbourne: Victorian Health Promotion Foundation.
- McLeod, J. D., & Shanahan, M. J. (1996). Trajectories of poverty and children's mental health. Journal of Health and Social Behavior, 37(3), 207-220.
- Menaghan, E. G., Kowaleski Jones, L., & Mott, F. L. (1997). The intergenerational costs of parental social stressors: Academic and social difficulties in early adolescence for children of young mothers. Journal of Health and Social Behavior, 38(1), 72-86.
- Molnar, B. E., Buka, S. L., & Kessler, R. C. (2001). Child sexual abuse and subsequent psychopathology: Results from the National Comorbidity Survey. American Journal of Public Health, 91(5), 753-760.
- Mullen, P. E., Martin, J. L., Anderson, J. C., Romans, S. E., & Herbison, G. P. (1996). The long-term impact of the physical, emotional, and sexual abuse of children: A community study. Child Abuse & Neglect, 20(1), 7-21.
- Murray, J. A. (2005). A psychology of loss: A potentially integrating psychology for the future study of adverse life events. In A. Columbus (Ed.), Advances in psychology research (Vol. 37, pp. 15-46). New York: Nova Science.
- National Institute for Mental Health in England. (2006). National Social Inclusion Programme: Second annual report. London: National Social Inclusion Programme.
- Pirkola, S., Isometsa, E., Aro, H., Kestila, L., Hamalainen, J., Veijola, J., et al. (2005). Childhood adversities as risk factors for adult mental disorders. Social Psychiatry and Psychiatric Epidemiology, 40(10), 769-777.
- Raphael, B. (2000). A population health model for the provision of mental health care. Canberra: Commonwealth of Australia.
- Rodgers, B. (1996). Social and psychological wellbeing of children from divorced families: Australian research findings. Australian Psychologist, 31(3), 174-182.
- Rosenman, S., & Rodgers, B. (2004). Childhood adversity in an Australian population. Social Psychiatry and Psychiatric Epidemiology, 39(9), 695-702.
- Rumpf, H.- J., Meyer, C., Hapke, U., & John, U. (2001). Screening for mental health: Validity of the MHI-5 using DSM-IV Axis I psychiatric disorders as gold standard. Psychiatry Research, 105(3), 243-253.
- Rutter, M. (1993). Cause and course of psychopathology: Some lessons from longitudinal data. Paediatric and Perinatal Epidemiology, 7, 105-120.
- Rutter, M. (2000). Resilience reconsidered: Conceptual considerations, empirical findings, and policy implications. New York: Cambridge University Press.
- Rutter, M. (2007). Commentary: Resilience, competence, and coping. Child Abuse & Neglect, 31(3), 205-209.
- Sanson, A., Nicholson, J., Ungerer, J., Zubrick, S. R., Wilson, K., Ainley, J., et al. (2002). Introducing the Longitudinal Study of Australian Children (LSAC Discussion Paper No. 1). Melbourne: Australian Institute of Family Studies.
- Saunders, P., Naidoo, Y., & Griffiths, M. (2007). Towards new indicators of disadvantage: Deprivation and social exclusion in Australia. Sydney: Social Policy Research Centre, University of New South Wales.
- Sawyer, M. G., Arney, F. M., Baghurst, P. A., Graetz, J. J. C. B. W., Kosky, R. J., Nurcombe, B., et al. (2001). The mental health of young people in Australia: Key findings from the child and adolescent component of the National Survey of Mental Health and Well-Being. Australian and New Zealand Journal of Psychiatry, 35(6), 806-814.
- Scutella, R., & Smyth, P. (2005). The Brotherhood's Social Barometer: Monitoring children's chances. Fitzroy, Vic.: Brotherhood of St Laurence.
- Slee, P. T. (1993). Children, stressful life events and school adjustment. Educational Psychology, 13(1), 3-10.
- Tiet, Q. Q., Bird, H. R., Davies, M., Hoven, C., Cohen, P., Jensen, P. S., et al. (1998). Adverse life events and resilience. Journal of the American Academy of Child and Adolescent Psychiatry, 37(11), 1191-1200.
- Trewin, D. (2003). Census of Population and Housing: Selected social and housing characteristics, Australia, 2001 (Cat. No. 2015.0). Canberra: ABS.
- Trewin, D. (2004). Family characteristics, Australia, 2003 (Cat. No. 4222.0). Canberra: Australian Bureau of Statistics.
- Trewin, D. (2006). Information paper: Improving statistics on children and youth. An information development plan (Cat. No. 4907.0). Canberra: Australian Bureau of Statistics.
- Turner, R. J., & Lloyd, D. A. (1995). Lifetime traumas and mental health: The significance of cumulative adversity. Journal of Health and Social Behavior, 36(4), 360-376.
- UNICEF. (2007). Child poverty in perspective: An overview of child well-being in rich countries (Innocenti Report Card No. 7). Florence: UNICEF Innocenti Research Centre.
- Department of Human Services. (2007). Families where a parent has a mental illness: A service development strategy. Melbourne: Department of Human Services.
- Ware, J. E., & Sherbourne, C. D. (1992). The MOS Short-Form Health Survey (SF-36): I. Conceptual framework and item selection. Medical Care, 30, 473-483.
- Watson, N., & Wooden, M. (2002). The Household, Income and Labour Dynamics in Australia (HILDA) survey: Wave 1 survey methodology (HILDA Project Technical Paper Series No. 1/02). Melbourne: Melbourne Institute of Applied Economic and Social Research.
- Yamazaki, S., Fukuhara, S., & Green, J. (2005). Usefulness of five-item and three-item mental health inventories to screen for depressive symptoms in the general population in Japan. Health and Quality of Life Outcomes, 3(1), 48-54.
- Zubrick, S. R., Silburn, S. R., Burton, P., & Blair, E. (2000). Mental health disorders in children and young people: Scope, cause and prevention. Australian and New Zealand Journal of Psychiatry, 34, 570-578.
- Zubrick, S. R., Silburn, S. R., Lawrence, D. M., Mitrou, F. G., Dalby, R. B., Blair, E. M., et al. (2005). The social and emotional wellbeing of Aboriginal children and young people (The Western Australian Aboriginal Child Health Survey, Vol. 2). Perth: Telethon Institute for Child Health Research and Curtin University of Technology.
Olesen, S. C., Macdonald, E., Raphael, B., & Butterworth, P. (2010). Children's exposure to parental and familial adversities. Family Matters, 84, 43-52.