Multi-type maltreatment and polyvictimisation
A comparison of two research frameworks
You are in an archived section of the AIFS website
Child maltreatment and child protection have commanded much public attention in recent years. From persistent media scrutiny of child protection systems to public outrage such as that in 2008 surrounding the photographs of artist Bill Henson,1 the protection of Australia's children is a topic that ignites popular interest like few others. It is easy to forget, then, that academic interest in child abuse and neglect2 only gathered momentum relatively recently, catalysed by Kempe and colleagues' seminal 1962 article on "battered child syndrome" in the Journal of the American Medical Association (described in Feerick & Snow, 2006; James, 2000). Although concern about child maltreatment dates back centuries, it is only in the last few decades that it has been widely acknowledged, systematically studied and recognised as a public policy issue (Feerick & Snow, 2006; Miller-Perrin & Perrin, 2007).
One of the defining features of the first few decades of child maltreatment research was a focus on individual forms of abuse and neglect, and the attempt to identify risk factors and outcomes specific to these forms (Anderson, 2010; Higgins, 2004a). In the 1960s and 1970s, much child maltreatment research focused on physical abuse and, to a lesser extent, neglect (Herrenkohl & Herrenkohl, 2009; James, 2000). The 1980s saw the focus of attention move to child sexual abuse and paedophilia (James, 2000), which grew out of a strong emphasis of second-wave feminism on rape and sexual assault. In the 1990s, more attention was directed towards understanding the nature, prevalence and consequences of psychological (or emotional) maltreatment (Higgins, 2004a), and many began to consider the witnessing of family violence as an independent subtype of abuse (James, 1994; Miller-Perrin & Perrin, 2007). Although understanding of the different forms of abuse increased markedly in this period, attempts to identify risk factors and outcomes specific to individual forms of maltreatment were largely unsuccessful (Higgins, 2004a, 2004b).
While it is useful to distinguish between the different subtypes of child maltreatment in order to understand them more thoroughly, it can also create the misleading impression that there are always strong lines of demarcation between the different childhood adversities, or that they usually occur in isolation (Miller-Perrin & Perrin, 2007; Price-Robertson, 2012). There is a growing body of evidence, however, to suggest that experiences of abuse or neglect seldom occur in isolation; the majority of individuals with a history of maltreatment report exposure to two or more subtypes (Arata, Langhinrichsen-Rohling, Bowers, & O'Farrill-Swails, 2005; Higgins & McCabe, 2000a; Ney, Fung, & Wickett, 1994). Indeed, some individual acts of violence against children involve multiple forms of maltreatment. For example, an adult who sexually abuses a child may also hit them (physical abuse) and belittle them (emotional abuse). There is also evidence to suggest that broader experiences of victimisation tend to cumulate for certain individuals or in certain environments. For instance, children who have been maltreated in a family context may be more susceptible than others to peer violence or exposure to crime, while those who have been sexually abused may be more susceptible than others to re-victimisation (Finkelhor, Ormrod, & Turner, 2007a; Tseloni & Pease, 2003).
One of the most recent major shifts in the focus of child maltreatment research has been the recognition of the interrelatedness of childhood victimisation experiences (Anderson, 2010; Higgins, 2004a). Two main frameworks have been developed to better understand and measure this interrelatedness: multi-type maltreatment, which provides a theoretical framework for the inclusion of five forms of maltreatment in a single measure (i.e., sexual abuse, physical abuse, psychological maltreatment, neglect, and witnessing family violence); and polyvictimisation, which focuses not only on different forms of maltreatment, but also on broader experiences of victimisation, such as bullying and exposure to neighbourhood conflicts.
The purpose of this paper is to compare these two frameworks. This is important because although they share many features, they also differ in significant ways, and may have more or less utility in different research contexts. This paper first compares multi-type maltreatment and polyvictimisation conceptually, outlining the history of the development of the two frameworks, the measurement tools used to operationalise them, and a selection of illustrative findings from some pivotal studies in their respective histories. And second, this study compares these frameworks empirically, using data from the Australian Temperament Project (ATP) to explore the respective utility of the concepts in identifying the long-term psychosocial outcomes associated with childhood adversity.
Multi-type maltreatment
In order to convey the interconnectedness of childhood maltreatment experiences, Australian researchers introduced the term "multi-type maltreatment" (Higgins & McCabe, 1998). Initially, these researchers investigated multiple forms of abuse and neglect as a way of accounting for the effects of sexual abuse; by the mid-1990s, the hope of identifying symptoms specific to sexual abuse were not being realised,3 so attention shifted to the ways in which other forms of maltreatment may either mediate or contribute to the negative outcomes associated with sexual abuse. However, the case for adopting a framework that encompassed multiple forms of maltreatment became so compelling that Higgins and McCabe began to focus on the co-occurrence of maltreatment subtypes as an independent topic, rather than simply an adjunct to sexual abuse research. They reasoned that measuring multi-type maltreatment could help researchers account for variability in the short- and long-term psychological adjustment of children and adults who had experienced various forms of child abuse and neglect.
In 2001, Higgins and McCabe conducted a systematic review of studies that had measured more than one type of child abuse or neglect (Higgins & McCabe, 2001b). They identified only 29 such studies, the majority of which measured two or three types of maltreatment. Indeed, at that time, Higgins and McCabe's (2000b) and McGee, Wolfe and Wilson's (1997) studies were the only ones to have measured all five forms of maltreatment. Although the studies included in the 2001 systematic review varied considerably in their aims and methodologies, they tended to share two key findings. First, a large proportion of adults who experienced maltreatment in childhood were subjected to more than one type. In other words, maltreatment subtypes tended to be correlated. Second, those adults who reported experiencing more than one form of maltreatment demonstrated significantly poorer wellbeing than adults reporting a single form of abuse, or those reporting none.
These two key findings were confirmed when Higgins and McCabe (1998, 2001a) developed and used the Comprehensive Child Maltreatment Scale (CCMS), a research tool designed to measure multi-type maltreatment. The CCMS measured five forms of child maltreatment using continuous scales, and comprised separate versions for adults (i.e., CCMS-A: retrospective reports of their own childhood experiences) and parents (i.e., CCMS-P: reports on the experiences of their children aged 5-12). Studies using the CCMS demonstrated significant overlap in the occurrence of all types of child abuse and neglect, ranging from r = .24 (for sexual abuse and witnessing family violence) to r = .74 (for physical abuse and psychological maltreatment) (Higgins & McCabe, 1998). They also found that those with high scores on scales for two maltreatment types had poorer outcomes (e.g., internalising and externalising behaviours) than those with only a single type, and those with high scores on three or more abuse types had poorer outcomes still (Higgins & McCabe, 2000a). Indeed, Higgins (2004a) noted that:
Results from an analysis of parent-report and adult self-report data suggest that the degree (frequency and severity) to which young people experience a range of abusive/neglectful behaviours is more important than the particular sub-type of maltreatment in explaining subsequent psychological problems. (p. 50)
Subsequent multi-type maltreatment research has built upon these initial findings. Table A1 (in the appendix) outlines a selection of the main studies that have used multi-type maltreatment as a conceptual framework. As can be seen in this table, the majority of studies that have investigated correlations between multi-type maltreatment and psychosocial outcomes have focused on internalising problems (e.g., depression, anxiety) and externalising problems (e.g., antisocial behaviour, aggression). A small number of studies have explored the predictors of multi-type maltreatment, indicating that the quality of family relationships (e.g., low family cohesion, low family adaptability) and parental attitudes (e.g., traditional parental family values, parental sexual punitiveness) tend to influence the likelihood of the occurrence of multi-type maltreatment. The lifetime prevalence rates of multi-type maltreatment range from 8% (Price-Robertson, Smart, & Bromfield, 2010) to over 57% (Sesar, Zivcic-Becirevic, & Sesar, 2008).4
Polyvictimisation
David Finkelhor was among the first to advocate for an approach to child maltreatment research that considered multiple forms of victimisation together. In 1983, he said:
It may be important, both for the benefit of research and theory, and also to counteract some of the divisive tendencies, for researchers on the disparate forms of domestic violence to see what they can find in the way of commonalities. (p. 17)
However, it was not until more than 20 years later - in 2005 - that Finkelhor and colleagues at the University of New Hampshire introduced the concept of polyvictimisation (Finkelhor, Ormrod, Turner, & Hamby, 2005). Polyvictimisation has been defined as "having experienced multiple victimizations of different kinds, such as sexual abuse, physical abuse, bullying, and exposure to family violence" (Finkelhor, Turner, Hamby, & Ormond, 2011, p. 4). As this definition suggests, polyvictimisation includes not simply child maltreatment (e.g., sexual and physical abuse), but also a broad array of other adversities, including peer bullying, witnessing community violence and property crime.
The reasons why Finkelhor and colleagues began investigating polyvictimisation were similar to those that saw Higgins and McCabe introduce multi-maltreatment almost a decade earlier: a number of independent lines of research pointed to the fact that children who experienced multiple forms of victimisation were at a particularly high risk of additional victimisation (whether of the same or different kind) and ongoing negative psychological effects (Finkelhor et al., 2011). Also, similarly to Higgins and McCabe, they hypothesised that measuring polyvictimisation would help account for large variations in the traumatic symptoms seen in children subjected to various forms of childhood adversity.
The main research tool used to measure polyvictimisation to date has been the Juvenile Victimization Questionnaire (JVQ) (Finkelhor et al., 2005). The JVQ measures 34 individual forms of victimisation,5 which can be grouped into five general categories: conventional crime (e.g., robbery), child maltreatment (including physical, emotional, and neglect), peer and sibling victimisation (e.g., bullying), sexual victimisation (including peer or adult perpetration), and witnessing and indirect victimisation (e.g., witnessing family violence, witnessing an assault with a weapon). As opposed to the CCMS, which was originally developed to measure either adults' retrospective experiences or parents' reports of their children, the JVQ was initially developed for self-reports of 10-17 year olds. However, more recent "caregiver" and "adult retrospective" versions, as well as abbreviated and reduced item versions, of the JVQ have been developed.6
Table A2 (in the appendix) outlines an illustrative selection of the key studies that have used polyvictimisation as a conceptual framework. Most of the studies with outcome measures focused on short-term trauma symptoms (i.e., anxiety, depressive symptoms, and anger/aggression). These studies tended to find that polyvictimisation was highly predictive of trauma symptoms, and when taken into account, greatly reduced or eliminated the association between individual victimisations (e.g., sexual abuse) and symptomatology. However, when assessing lifetime prevalence of victimisation, maltreatment experiences have been found to uniquely predict adult outcomes, even when controlling for polyvictimisation (Finkelhor, Ormrod, & Turner, 2009). (The implications of this finding are discussed in detail in the Implications for Research.)
Studies measuring predictors of polyvictimisation have generally focused on broader socio-demographic factors (e.g., socioeconomic status, place of residence), which have been found to significantly influence the likelihood that polyvictimisation will occur. Finally, the incidence and prevalence rates have varied considerably, depending on how polyvictimisation has been defined or the particular study sample used. However, in the largest representative studies, it was found that almost a quarter (22-23%) of all US children had been subjected to four or more different forms of victimisation in the past year.
Summary of the two research frameworks
The main similarities and differences between multi-type maltreatment and polyvictimisation are outlined in Table 1. The central feature of both research frameworks is their focus on multiple forms of victimisation; in this sense they are very similar. The central difference is one of scope: while multi-type maltreatment concentrates on experiences of child abuse and neglect, polyvictimisation measures a larger number of childhood victimisation experiences. This central difference has led to a number of divergences in the types of measurement tools and methods used. For instance, while it is feasible to measure five types of maltreatment using multiple questions for each type (which is important for measuring severity and understanding the sub-components of maltreatment types), it is much less feasible to include detailed measurement of 34 forms of victimisation (e.g., the JVQ has only one item per victimisation type, whereas the CCMS has between 2 and 11 items each).
| Multi-type maltreatment | Polyvictimisation |
|---|---|
| Developed to measure overlap in maltreatment experiences, and account for explainable variation in psychosocial outcomes associated with maltreatment | Developed to measure overlap in victimisation experiences (inc. maltreatment), and account for explainable variation in traumatic symptoms |
| Detailed measurement of five forms of maltreatment (i.e., sexual abuse, physical abuse, psychological maltreatment, neglect, and witnessing family violence) | Brief measurement of up to 34 forms of victimisation (e.g., conventional crime, child maltreatment, peer and sibling victimisation, sexual victimisation and witnessing and indirect victimisation) |
| Main measurement tool: Comprehensive Child Maltreatment Scale; adult or parent report; continuous scales | Main measurement tool: Juvenile Victimization Questionnaire; child self-report, caregiver, or adult report; dichotomous measures |
| Focuses on lifetime prevalence | Often focuses on 12-month incidence, although some recent studies on lifetime prevalence |
| Tends to focus on long-term psychosocial outcomes (e.g., internalising and externalising behaviour problems) | Tends to focus on short-term trauma symptoms (e.g., child anxiety, depressive symptoms and anger/aggression) |
Empirical comparison
One aim of this paper was to compare the utility of the multi-type maltreatment and polyvictimisation frameworks by using existing data collected as part of the Australian Temperament Project. To this end, three separate analyses were conducted. First, a measure of multi-type maltreatment was developed in order to examine its utility in explaining psychosocial outcomes in young adulthood. (See the "Group formation" section for a description of all the measures used in the current study). For the same purpose, a measure of polyvictimisation was developed; this measure contains the same forms of maltreatment as the multi-type maltreatment measure, but also includes three forms of peer victimisation, or bullying. Finally, a "victimisation type" measure was developed, which separates the different forms of maltreatment measured by multi-type maltreatment from the peer victimisation experiences specific to the polyvictimisation measure, in order to identify their unique influence on the outcomes.
The findings presented here come from the Australian Temperament Project, a longitudinal community study that has followed the development of a large group of Australians from infancy into adulthood.7 In the 2006-07 survey - conducted when study members were 23-24 years of age - young people were asked to reflect on their family experiences prior to age 18, both positive and negative. The findings presented in this paper are based on a sample of 1,000 study members (390 males, 610 females).
This empirical comparison was not intended to be exhaustive or definitive, but is perhaps best considered a demonstration of these frameworks, designed to accompany the above conceptual comparison. Nonetheless, the current analysis still adds to the limited evidence base of multi-type maltreatment and polyvictimisation in Australia, and effectively illustrates some of the differences between them.
Measures
The questions used to measure young peoples' experiences while growing up are shown in Box 1. Items 1-6 reflect differing forms of maltreatment, while items 7-9 indicate different types of bullying. The table also shows the five psychosocial outcome measures at 23-24 years. Following Price-Robertson, Smart et al. (2010), these measures were chosen as they have previously been shown to be associated with childhood experiences of abuse and neglect. All outcomes were composites of items, with the exception of "long-term health problems", which was measured with a single item.
Box 1: Questions used to measure young people's childhood victimisation experiences and psychosocial outcomes
Victimisation experiences a
1. Physical abuse: Your parent/s used harsh physical treatment (e.g., smacking, hitting) to discipline you > (If yes) > Did you ever suffer effects that lasted to the next day or longer (e.g., bruising, marking, pain, soreness)? (Note: "Yes" to second question was used to indicate physical abuse.)
2. Intra-familial sexual abuse: A family member did, or tried to do, sexual things to you.
3. Extra-familial sexual abuse: You had a sexual experience with a person who was not a family member before you were 16 > (If yes) > Was this consensual? (Note: "No" to second question was used to indicate sexual abuse.)
4. Emotional maltreatment: You experienced verbal treatment from your parent/s that made you feel embarrassed, humiliated, or scared (e.g., shouting, name calling, threats). (Note: Responses of "somewhat true" and "very true" were taken as indicating emotional maltreatment.)
5. Neglect: The care taken of you by your parent/s was the right amount (e.g., they watched out for you, fed you properly, gave you attention). (Note: Reverse scored; responses of "somewhat untrue" and "not at all true" were taken as indicating neglect.)
6. Witnessing family violence: There was physical violence between the adults caring for you. (Note: Responses of "somewhat true" and "very true" were taken as indicating witnessing family violence.)
You were bullied by schoolmates > (If yes) > In what way? (circle all that apply)
7. Bullying 1: Verbal abuse or insults
8. Bullying 2: Isolation or exclusion
9. Bullying 3: Physical bullying
Psychosocial outcomes at 23-24 years
1. Depression (e.g., "Over the past month I felt that life was meaningless"): 16% of ATP sample b
2. Anxiety (e.g., "Over the past month I felt scared without any good reason"): 16% of ATP sample b
3. Illicit substance use in the previous month (e.g., marijuana, ecstasy, amphetamines): 20% of ATP sample
4. Antisocial behaviour in past 12 months (e.g., "sold illegal drugs"): 7% of ATP sample c
5. Long-term health problems (the presence of a long-term health problem or disability, e.g., diabetes): 22% of ATP sample
Notes: a Question 1-3 and 7-9 were measured using dichotomous (yes/no) measures. Questions 4-6 were measured using a 5-point Likert scale (1 = very true, 5 = not at all true) and then converted into dichotomous variables. b From Lovibond & Lovibond (1995). c Adapted from Elliott & Ageton (1980), Self Report Delinquency Scale.
Group formation
A multi-type maltreatment measure was developed by summing the six different types of reported abuse and neglect (i.e., physical abuse, intra-familial sexual abuse, extra-familial sexual abuse, emotional maltreatment, neglect, witnessing family violence). Three groups were formed:
- no maltreatment group, who did not report any experience of child maltreatment (n = 768, 77% of the sample);
- single maltreatment group, who reported one form of maltreatment (n = 153, 15% of the sample); and
- multi-type maltreatment group, who reported two or more forms of maltreatment (n = 79, 8% of the sample).8
A polyvictimisation measure was created by summing the number of types of victimisation experiences reported out of the nine provided (i.e., physical abuse, emotional maltreatment, neglect, witnessing family violence, intra-familial sexual abuse, extra-familial sexual abuse, bullying (verbal abuse), bullying (exclusion), and bullying (physical). Four groups were formed:
- no victimisation group, who did not report any form of maltreatment or bullying (n = 465, 47% of sample);
- single victimisation group, who reported one form of either maltreatment or bullying (n = 219, 22% of sample);
- low polyvictimisation group, who reported two types of maltreatment or bullying (n = 181, 18% of sample); and
- high polyvictimisation group, who reported three or more types of maltreatment or bullying (n = 135, 14% of sample).
Finally, a victimisation type measure was designed to compare the outcomes of those experiencing different types of victimisation (i.e., maltreatment, bullying or both):
- no maltreatment or bullying group, who reported neither maltreatment nor bullying (n = 456, 46% of sample);
- bullying only group, who reported at least one form of bullying but no forms of maltreatment (n = 306, 31% of sample);
- maltreatment only group, who reported at least one form of maltreatment but no forms of bullying (n = 89, 9% of sample); and
- maltreatment and bullying group, who reported at least one form of both maltreatment and bullying (n = 143, 14% of sample).9
Results
Rates of victimisation
Almost a quarter (23%) of participants had experienced one or more of the five forms of child maltreatment. Fifteen per cent reported experiencing a single type of maltreatment, while 8% had experienced multi-type maltreatment (i.e., two or more forms). The most common type of maltreatment was emotional maltreatment (17%), while neglect was the least common (3%).
Bullying was also prevalent, with 45% of participants indicating that they had been victims of bullying at least once during their school years. The most common form of bullying reported was verbal abuse or insults (39%), although social isolation or exclusion was also frequently reported (23%).
In total, 54% of participants had been bullied or maltreated prior to age 18. Almost a third (31%) had experienced bullying only, 9% experienced child maltreatment, but not bullying, and 14% reported both bullying and maltreatment (i.e., polyvictimisation).
Outcomes in early adulthood
The multi-type maltreatment, polyvictimisation and victimisation type groups described earlier were compared on a range of problematic outcomes at 23-24 years (i.e., depression, anxiety, illicit substance use, antisocial behaviour and long-term health problems) to determine whether they exhibited different profiles. Separate logistic regression analyses were used to compare groups (e.g., the no, single and multi-type maltreatment) on rates of each outcome (e.g., depression).
The results of these comparisons are described in terms of odds ratios (OR). Odds ratios can be used to estimate the likelihood of an outcome occurring (e.g., depression) if a particular factor is present (e.g., child maltreatment). Values close to 1 indicate that there is no relationship between a factor and an outcome, values greater than 1 suggest that as levels of a factor increase, so does the likelihood of the outcome occurring, while values less than one suggest that an outcome is less likely to occur as levels of a factor increase.
Table 2 summarises the results of these comparisons while Table A3 in the appendix provides more detailed statistical data. The crosses (X) in Table 2 indicate where groups that had experienced some form of maltreatment or victimisation significantly differed on a particular outcome from the groups that had not. The more crosses, the higher the OR, indicating a relatively higher likelihood of the outcome occurring. For example, the table shows that the single- and multi-type maltreatment groups were significantly more likely than the no maltreatment group to experience depression, with the multi-type maltreatment group being the most likely to do so.
Comparison of multi-type maltreatment groups
Significant associations were found between the number of forms of maltreatment a person experienced in childhood and his/her likelihood of becoming depressed and/or anxious in early adulthood (Table 2).
| Outcomes at 23-24 years | |||||
|---|---|---|---|---|---|
| Depression | Anxiety | Illicit substance use | Antisocial behaviour | Long-term health problems | |
| Multi-type maltreatment (ref. = no maltreatment) | |||||
| Single maltreatment | X | X | |||
| Multi-type maltreatment | XXX | XX | |||
| Polyvictimisation (ref. = no victimisation) | |||||
| Single victimisation | |||||
| Low polyvictimisation | X | ||||
| High polyvictimisation | XX | XX | XX | XX | |
| Victimisation type (ref. = no maltreatment or bullying) | |||||
| Bullying only | X | ||||
| Maltreatment only | XX | ||||
| Maltreatment and bullying | XXX | XX | XX | XX | |
Note: X = a significant positive association, p < .05; XX = OR > 2.0; XXX = OR > 3.0. See Table A3 for detailed data.
Young people who experienced multi-type maltreatment were 3.7 times more likely than those who were not maltreated to be depressed at 23-24 years, and 2.7 times more likely to be anxious. Those who experienced one form of maltreatment prior to age 18 were also at heightened risk of subsequent depression and anxiety, although the odds of this occurring were lower than for the multi-type maltreatment group (ORs of 1.9 and 1.6, respectively).
The maltreatment groups did not significantly differ in their likelihood of engaging in illicit substance use, antisocial behaviour or having a long-term health problem.
Comparison of polyvictimisation groups
The number of victimisation experiences individuals faced prior to age 18 was significantly related to their likelihood of experiencing a range of problematic outcomes in early adulthood (Table 2). Young people who had experienced three or more forms of victimisation in childhood were almost three times as likely as those who had not been victimised to be depressed at age 23-24, and more than two and a half times as likely to be subsequently anxious, antisocial and have a chronic health problem. Young people who had experienced two different forms of victimisation were also at heightened risk of having chronic health problems (OR = 1.8).
No significant associations were found between polyvictimisation severity and later illicit substance use.
Comparison of victimisation type groups
Significant associations were found between the form of victimisation a person experienced in childhood and their likelihood of experiencing a range of negative outcomes in early adulthood (Table 2).
Young people who had been both bullied and maltreated prior to age 18 were more than three times as likely as those who had not been victimised to be depressed at 23-24 years, and approximately two and a half times as likely to be antisocial and/or have a long-term health problem. Furthermore, this group was more than twice as likely as those who had not been victimised to be anxious.
Study members who were bullied, but not maltreated (the bullied only group) were also more likely than those who were not victimised to have a chronic health problem in early adulthood (OR = 1.9), while those who were mistreated but were not bullied (the maltreatment only group) were at heightened risk of engaging in illicit substance use at 23-24 years (OR = 2.0).
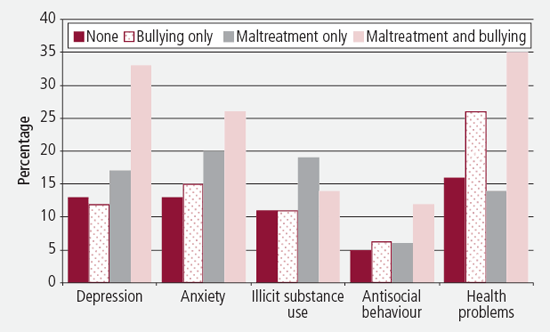
The comparison of the victimisation type groups revealed some interesting patterns. In general, rates of adverse outcomes among the bullying only group, were similar to those among the no victimisation group (an exception to this was the significant association with long-term health problems).10 On the other hand, there was a trend for a higher proportion of those in the maltreatment only group to experience adverse psychosocial outcomes than among the no maltreatment or the bullying only groups (see Figure 1).
Figure 1: Percentage of victimisation type groups reporting adverse outcomes at 23-24 years
Strengths and limitations of the current study
The current study has a number of strengths. Firstly, in contrast to many similar studies that use self-selected or clinical samples, the findings of this study are based on a relatively large community sample, which helps to decrease the biases that can arise from the former types of sampling. A further strength is that the ATP is a longstanding study in which a strong history of trust has been developed with study members. Such trust is particularly important when respondents are asked to disclose very sensitive information, such as whether or not they experienced child maltreatment. A third major strength is the breadth of data collected, allowing a range of childhood experiences and early adult outcomes to be examined, and cumulative measures of adverse experiences to be developed.
However, the research reported in this paper also has several limitations. As with many longitudinal studies, attrition over the course of the ATP has resulted in a slight under-representation of families from lower socio-demographic backgrounds or with a non-Australian-born parent. Thus, the current study's findings are likely to slightly underestimate the effects of growing up in a low socioeconomic status or immigrant family. Attrition has also resulted in there being a lower proportion of males in the ATP sample (i.e., 310 males compared to 610 females), which might have had some influence on the strengths of associations found. However, as the focus of this project was a comparison between two conceptual frameworks, an examination of gender differences was considered beyond its scope.
Secondly, the measures used to assess multi-type maltreatment and polyvictimisation were not as detailed as those used in some other studies. This is especially true of the polyvictimisation measure; although it measured aspects of four out of the five general categories covered by the JVQ, it was not nearly as extensive as the JVQ. The ATP is a life course study, collecting information on a wide range of aspects of child and youth development. Other more narrowly focused studies are able to include more in-depth measures than those used here. While it would have been preferable to use detailed measures such as the CCMS (for multi-type maltreatment) and the JVQ (for polyvictimisation), to our knowledge no studies have been conducted that used both of these measurement tools while also measuring adult outcomes.
It should also be noted that the measures used in the current study were not subjected to reliability or validity testing. However, the purpose of this paper was comparison, rather than original research into multi-type maltreatment and polyvictimisation per se. Although data from the ATP were considered sufficient for this purpose, these limitations affect the extent to which the findings from the current study can be extrapolated or be taken to represent rigorous new findings supporting either the multi-type maltreatment or polyvictimisation frameworks.
Finally, as in many other studies in this area, childhood family experiences were retrospectively reported in the current study. There has been debate about the accuracy of such reports, with memory loss and recall bias being commonly identified problems (Beckett, DaVanzo, Sastry, Panis, & Peterson, 2001). However, previous research with members of the current study has found high concordance between retrospective reports and other sources of data (e.g., between self-reports of contact with the police for offending and official police records; Smart et al., 2005), suggesting retrospective reports can provide useful and reliable information.
Implications for research
The current paper has demonstrated the value of using both the multi-type maltreatment and polyvictimisation frameworks for understanding child victimisation and its effects on wellbeing. Consistent with research on both multi-type maltreatment (e.g., Higgins & McCabe, 1998, 2003) and polyvictimisation (e.g., Finkelhor et al., 2009; Richmond, Elliott, Pierce, Aspelmeier, & Alexander, 2009), victimisation among ATP participants was found to be strongly associated with internalising behaviour problems (i.e., anxiety and depression) in adulthood. For example, compared to those who did not experience maltreatment, participants in the multi-type maltreatment group were almost four times more likely to be depressed, and almost three times more likely to be anxious. The high polyvictimisation group were also at heightened risk for depression and anxiety in early adulthood, as well as antisocial behaviour and long-term health problems.
An obvious question to ask, then, is: Which framework is the best to use in child victimisation research?
The answer to this appears to depend on the aims of the research in question. There are times when a broad measure of a wide variety of victimisation experiences will be most appropriate (i.e., polyvictimisation), and there are other times when detailed measurement of specific child maltreatment experiences will be preferable (i.e., multi-type maltreatment).
For instance, if the aim of research is to provide an accurate assessment of the immediate risk environment children are facing, polyvictimisation will likely be the best option. The current findings suggest that, when compared to measures of multi-type maltreatment, measures of polyvictimisation may capture a greater range, or at least different forms, of adversity. Compared to multi-type maltreatment, polyvictimisation was associated with a greater number of problematic outcomes in early adulthood. Specifically, those in the high polyvictimisation group were significantly more likely to engage in antisocial behaviour and experience chronic health problems, while those in the multi-type maltreatment group were not.11
The breadth of polyvictimisation makes it well suited to measurement of the short-term incidence of victimisation experiences and trauma. Some children will generally be at high risk of adversity in their lives. Although they may not have been maltreated (i.e., as measured by multi-type maltreatment) in the past year, they might have been subjected to a number of other victimisation experience (e.g., peer bullying, property crime), which polyvictimisation measures will be able to identify.
If researchers have the capacity to include in-depth measures of many of the adversities covered by polyvictimisation, then it appears that it would be sensible to do so. The current analysis suggests that the more child victimisation experiences that are measured, the more sensitively researchers will be able to detect relationships with later outcomes.
On the other hand, if the purpose of research is to identify those experiences (i.e., the different forms of child maltreatment) that tend to have the most profound long-term influences on individuals' lives, then measures of multi-type maltreatment may be preferable. Research by Finkelhor and colleagues (2009) found that when studying short-term outcomes (within 12 months), aggregated measures of victimisation (i.e., polyvictimisation) "eclipsed or greatly reduced the contribution of any particular type of victimization in the prediction of mental health symptoms" (p. 407). However, when investigating the lifetime prevalence of polyvictimisation, they found that any form of child maltreatment or sexual assault continued to be a significant predictor of later trauma symptoms, even after controlling for lifetime polyvictimisation. "This suggested", according to the authors, "that in the lifetime assessment of polyvictimization as a predictor of negative outcomes, child maltreatment and sexual assault had a particular traumatic salience, and therefore should be given additional weight in the summing of victimizations" (p. 408, emphasis added). The results of the current study would appear to offer some support for Finkelhor et al.'s (2009) observations, with those in the maltreatment only group being more likely to report a range of adverse long-term outcomes than those who experienced bullying only (see Figure 1 ).
When compared to the wide scope of polyvictimisation, the primary benefit of multi-type maltreatment's limited breadth is that it allows a much more in-depth measurement of maltreatment experiences. Research has demonstrated that multiple questions are required to accurately measure a subtype of abuse. For instance, the number of questions that researchers ask can have a strong effect on prevalence estimates. Peters, Wyatt, and Finkelhor (1986) found that studies that asked four or more questions on sexual abuse produced the highest estimates. Similarly, differences in the wording of questions can lead to dramatic differences in prevalence figures. For example, a question such as "Were you sexually abused as a child?" requires people to categorise themselves as "victims of sexual abuse". Many will resist this categorisation, even if they have been subjected to behaviours that constitute sexual abuse (Sorsoli, Kia-Keating, & Grossman, 2008). Alternatively, questions that involve behavioural descriptions (e.g., "When you were a child did an adult touch or fondle your body in an inappropriate way?") are more likely to elicit an accurate response, although multiple behavioural questions will often be required to cover the range of behaviours that constitute a particular form of maltreatment (Goldman & Padayachi, 2000).
Whether one chooses multi-type maltreatment, polyvictimisation, or some other framework that accounts for multiple experiences of victimisation, it is clear that the era in which researchers routinely measure only one form of child victimisation is drawing to a close. There is simply too much evidence suggesting that experiences of victimisation routinely co-occur. This evidence gives reason to question any research that only measures one form of maltreatment and attempts to draw conclusions about outcomes or risk factors associated with this form of maltreatment. For instance, if researchers only measure physical abuse, how can they be sure that any correlations they find with long-term psychosocial outcomes are not actually the effect of various other victimisation experiences that are likely to co-occur with physical abuse? The answer is: they cannot be sure.
Of course, this does not mean that all forms of child victimisation are the same, or that they should not be investigated separately. To be sure, research has identified some unique outcomes associated with specific forms of victimisation (e.g., greater sexualised behaviour among sexually abused young people). It does mean, however, that researchers investigating the consequences of a specific form of victimisation should at least control for the effects of other victimisation experiences, as well as for the effects of cumulative experiences of victimisation, such as by using measures of multi-type maltreatment or polyvictimisation.
Endnotes
1 For those unaware of this controversy, the opening night of a 2008 exhibition of prominent Australian photographer Bill Henson was cancelled after police received numerous complaints regarding a photograph of a nude 13-year-old girl, which was featured on the invitation to the exhibition. The police subsequently seized a number of photographs from the cancelled exhibition, with the intention of charging Henson with "publishing an indecent article". This incident catalysed an intense national debate over censorship and the depiction of children in art and advertising. For extended treatment of this controversy, see Marr (2008).
2 Following Finkelhor, Turner, and Hamby (2012), child victimisation can be broadly defined as "harm caused by other persons, in this case, peers, acting outside of the norms of appropriate conduct" (p. 273). In order to enhance readability, the terms "child maltreatment", "child abuse and neglect", "childhood adversity" and "victimisation" are generally used interchangeably in this paper. However, on some occasions "child maltreatment" is used to denote a limited subcategory (i.e., the five forms of abuse and neglect measured in multi-type maltreatment) of broader "victimisation" experiences (i.e., the 34 forms of victimisation measured in polyvictimisation). It should be clear from the context which type of use is intended.
3 One exception to this is the finding that sexually abused youth display greater sexualised behaviour (Miller-Perrin & Perrin, 2007).
4 Such large discrepancies in prevalence figures primarily reflect differences in sampling strategies (e.g., clinical samples versus representative community samples), but could also be related to differences in measurement (e.g., the continuous maltreatment scales of the CCMS versus dichotomous measures of maltreatment).
5 That is: exposure to war or ethnic conflict, sexual assault by peer, rape (attempted or completed), flashing/sexual exposure, verbal sexual harassment, nonspecific sexual assault, bias attack, witness to parent assault of sibling, kidnapping, witness to murder, exposure to random shootings etc., custodial interference/family abduction, physical abuse by caregiver, dating violence, robbery, gang or group assault, witness to assault with weapon, attempted assault, psychological/emotional abuse, nonsexual genital assault, murder of family member or friend, assault with weapon, personal theft, witness to assault without weapon, witness to domestic violence, vandalism, assault without weapon, sexual assault by known adult, burglary of family household, neglect, emotional bullying, bullying, peer or sibling assault.
6 For a full description of the different versions of the JVQ, see: <www.unh.edu/ccrc/juvenile_victimization_questionnaire.html>.
7 For more details, see Prior, Sanson, Smart, and Oberklaid (2000) or visit the ATP study website: <www.melbournechildrens.com/atp/>.
8 As two forms of child sexual abuse were measured in this study (i.e., intra- and extra-familial), it would have been possible for participants to be included in the multi-type maltreatment group when they had only experienced one of the five forms of abuse or neglect included in the multi-type maltreatment framework. Thus, participants who experienced both intra- and extra-familial sexual abuse but no other forms of maltreatment (N = 2) were included in the single maltreatment group.
9 As six participants were missing relevant data, the number of participants in these four groups equals 994. Percentages for the victimisation type groups were therefore calculated using a total of 994.
10 It was not possible from this finding to ascertain whether, or to what extent, bullying was a consequence, as opposed to simply a cause, of long-term health problems. In other words, it is possible that participants with long-term health problems may have been more likely to be targeted by peers.
11 As many of the multi-type maltreatment studies outlined in the introduction and in Table A1 have found connections between multi-type maltreatment and externalising behaviour problems, it is feasible that measurement or sample issues in the current study led to a lack of statistical sensitivity with which to detect such relationships.
References
- Anderson, K. L. (2010). Conflict, power, and violence in families. Journal of Marriage and Family, 72(3), 726-742.
- Arata, C. M., Langhinrichsen-Rohling, J., Bowers, D., & O'Farrill-Swails, L. (2005). Single versus multi-type maltreatment: An examination of the long-term effects of child abuse. Journal of Aggression, Maltreatment & Trauma, 11(4), 29-52.
- Beckett, M., DaVanzo, J., Sastry, N., Panis, C., & Peterson, C. (2001). The quality of retrospective data: An examination of long term recall in a developing country. Journal of Human Resources, 36(3), 593-625.
- Bevan, E., & Higgins, D. J. (2002). Is domestic violence learned? The contribution of five forms of child maltreatment to men's violence and adjustment. Journal of Family Violence, 17(3), 223-245.
- Briere, J., & Runtz, M. (1990). Differential adult symptomatology associated with three types of child abuse histories. Child Abuse and Neglect, 14, 357-364.
- Cawson, P., Wattam, C., Brooker, S., & Kelly, G. (2000). Child maltreatment in the United Kingdom: A study of the prevalence of child abuse and neglect. London: National Society for the Prevention of Cruelty to Children.
- Cuevas, C. A., Sabina, C., & Milloshi, R. (2012). Interpersonal victimization among a national sample of Latino women. Violence Against Women, 18(4), 377-403.
- Elliott, D. S., & Ageton, S. S. (1980). Reconciling race and class differences in self-reported and official estimates of delinquency. American Sociological Review, 45, 95-110.
- Ellonen, N., & Salmi, V. (2011). Poly-victimization as a life condition: Correlates of poly-victimization among Finnish children. Journal of Scandinavian Studies in Criminology and Crime Prevention, 12(1), 20-44.
- Feerick, M. M., & Snow, K. L. (2006). An examination of research in child abuse and neglect: Past practices and future directions. In M. M. Feerick, J. F. Knutson, P. K. Trickett, & S. M. Flanzer (Eds.), Child abuse and neglect: Definitions, classification, and a framework for research. Baltimore, MD: Paul H. Brooks Publishing Company.
- Finkelhor, D. (1983). Common features of family abuse. In D. Finkelhor, R. J. Gelles, G. T. Hotaling, & M. A. Straus (Eds.), The dark side of families: Current family violence research (pp. 17-28). Beverly Hills, CA: Sage Publishing.
- Finkelhor, D., Ormrod, R. K., & Turner, H. A. (2007a). Poly-victimization: A neglected component in child victimization. Child Abuse and Neglect, 31(1), 7-26.
- Finkelhor, D., Ormrod, R. K., & Turner, H. A. (2007b). Re-victimization patterns in a national longitudinal sample of children and youth. Child Abuse and Neglect, 31(5), 479-502.
- Finkelhor, D., Ormrod, R. K., & Turner, H. A. (2009). Lifetime assessment of poly-victimization in a national sample of children and youth. Child Abuse and Neglect, 33(7), 403-411.
- Finkelhor, D., Ormrod, R. K., Turner, H. A., & Hamby, S. L. (2005). Measuring poly-victimization using the Juvenile Victimization Questionnaire. Child Abuse and Neglect, 29(11), 1297-1312.
- Finkelhor, D., Turner, H., & Hamby, S. (2012). Let's prevent peer victimization, not just bullying. Child Abuse & Neglect, 36(4), 271-274.
- Finkelhor, D., Turner, H., Hamby, S., & Ormrod, R. (2011). Polyvictimization: Children's exposure to multiple types of violence, crime, and abuse. Washington, DC: Department of Justice.
- Ford, J. D., Wasser, T., & Connor, D. F. (2011). Identifying and determining the symptom severity associated with polyvictimization among psychiatrically impaired children in the outpatient setting. Child Maltreatment, 16(3), 216-226.
- Goldman, J. D. G., & Padayachi, U. K. (2000). Some methodological problems in estimating incidence and prevalence in child sexual abuse research. Journal of Sex Research, 37(4), 305-315.
- Herrenkohl, R. C., & Herrenkohl, T. I. (2009). Assessing a child's experience of multiple maltreatment types: Some unfinished business. Journal of Family Violence, 24(7), 485-496.
- Higgins, D. J. (2003). The relationship of childhood family characteristics and current attachment styles to depression and depressive vulnerability. Australian Journal of Psychology, 55(1), 9-14.
- Higgins, D. J. (2004a). Differentiating between child maltreatment experiences. Family Matters, 69, 50-55.
- Higgins, D. J. (2004b). The importance of degree versus type of maltreatment: A cluster analysis of child abuse types. Journal of Psychology: Interdisciplinary and Applied, 138(4), 303-324.
- Higgins, D. J., & McCabe, M. P. (1998). Parent perceptions of maltreatment and adjustment in children. Journal of Family Studies, 4(1), 53-76.
- Higgins, D. J., & McCabe, M. P. (2000a). Multi-type maltreatment and the long-term adjustment of adults. Child Abuse Review, 9(1), 6-18.
- Higgins, D. J., & McCabe, M. P. (2000b). Relationships between different types of maltreatment during childhood and adjustment in adulthood. Child Maltreatment, 5(3), 261-272.
- Higgins, D. J., & McCabe, M. P. (2001a). The development of the Comprehensive Child Maltreatment Scale. Journal of Family Studies, 7(1), 7-28.
- Higgins, D. J., & McCabe, M. P. (2001b). Multiple forms of child abuse and neglect: Adult retrospective reports. Aggression and Violent Behavior, 6(6), 547-578.
- Higgins, D. J., & McCabe, M. P. (2003). Maltreatment and family dysfunction in childhood and the subsequent adjustment of children and adults. Journal of Family Violence, 18(2), 107-120.
- James, M. (1994). Domestic violence as a form of child abuse: Identification and prevention. Melbourne: National Child Protection Clearinghouse.
- James, M. (2000). Child abuse and neglect: Part 1. Redefining the issues. Canberra: Australian Institute of Criminology.
- Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335-343.
- Marr, D. (2008). The Henson case. Melbourne: Text Publishing.
- McGee, R. A., Wolfe, D. A., & Wilson, S. K. (1997). Multiple maltreatment experiences and adolescent behavior problems: Adolescents' perspectives. Development and Psychopathology, 9(1), 131-149.
- Miller-Perrin, C., & Perrin, R. (2007). Child maltreatment: An introduction. Thousand Oaks, CA: Sage Publications.
- Ney, P. G., Fung, T., & Wickett, A.R. (1994). The worst combinations of child abuse and neglect. Child Abuse & Neglect, 18, 705-714.
- Peters, S. D., Wyatt, G. A., & Finkelhor, D. (1986). Prevalence. In D. Finkelhor (Ed.), A sourcebook on child sexual abuse. Beverly Hills, CA: Sage Publications.
- Price-Robertson, R. (2012). What is child abuse and neglect? (CFCA Resource Sheet). Melbourne: Australian Institute of Family Studies.
- Price-Robertson, R., Bromfield, L., & Vassallo, S. (2010). Prevalence matters: Estimating the extent of child maltreatment in Australia. Developing Practice, 26, 12-20.
- Price-Robertson, R., Smart, D., & Bromfield, L. (2010). Family is for life: Connections between childhood family experiences and wellbeing in early adulthood. Family Matters, 85, 7-17.
- Prior, M., Sanson, A., Smart, D., & Oberklaid, F. (2000). Pathways from infancy to adolescence: Australian Temperament Project 1983-2000. Melbourne: Australian Institute of Family Studies.
- Richmond, J. M., Elliott, A. N., Pierce, T. W., Aspelmeier, J. E., & Alexander, A. A. (2009). Polyvictimization, childhood victimization, and psychological distress in college women. Child Maltreatment, 14(2), 127-147.
- Sesar, K., Zivcic-Becirevic, I., & Sesar, D. (2008). Multi-type maltreatment in childhood and psychological adjustment in adolescence: Questionnaire study among adolescents in Western Herzegovina Canton. Croatian Medical Journal, 49(2), 243-256.
- Smart, D., Richardson, N., Sanson, A., Dussuyer, I., Marshall, B., Toumbourou, J. W., et al. (2005). Patterns and precursors of adolescent antisocial behaviour: Outcomes and connections. Third report. Melbourne: Australian Institute of Family Studies and Crime Prevention Victoria.
- Sorsoli, L., Kia-Keating, M., & Grossman, F. K. (2008). "I keep that hush-hush": Male survivors of sexual abuse and the challenges of disclosure. Journal of Counseling Psychology, 55(3), 333-345.
- Tseloni, A., & Pease, K. (2003). Repeat personal victimization: "Boosts" or "flags"? British Journal of Criminology, 43(1), 196-212.
- Vranceanu, A. M., Hobfoll, S. E., & Johnson, R. J. (2007). Child multi-type maltreatment and associated depression and PTSD symptoms: The role of social support and stress. Child Abuse and Neglect, 31(1), 71-84.
Appendix
| Authors | N | Age (years) | Sample | Measure | Childhood prevalence | Outcomes associated with MM | Predictors of MM |
|---|---|---|---|---|---|---|---|
| Higgins & McCabe (1998) (Australia) | 50 (43 females) | M = 40.6 ( SD = 16.0) | Self-selected parents of primary-school-aged children | FLEQ-P (including items that form the later CCMS-P) | MM = 42% (30% for 3 forms) | MM > externalising, internalising | N/A |
| Higgins & McCabe (2000b) (Australia) | 175 (128 females) | M = 31.46 ( SD = 11.01) | Self-selected community | CCMS-A | N/A | MM > trauma symptomatology, self-deprecation | Family background (gender, quality of childhood relationships, physical and verbal affection, parental divorce, family adaptability, family cohesion, parental sexual punitiveness, quality of interpersonal relationship, traditionality of father/mother) |
| Bevan & Higgins (2002) (Australia) | 36 males | M = 41.9 ( SD = 9.45) | Self-selected (from counselling agency, history of domestic violence) | CCMS-A | N/A | MM > physical spouse abuse, trauma symptomatology | N/A |
| Higgins (2003) (Australia) | (a) 50 (43 females) | (a) M = 39.6 ( SD = 7.2) | (a) Self-selected caregivers | (1) CCMS-P | N/A | (1) MM > externalising, internalising, sexual behaviour problems (in children) | (1) Family background (family adaptability, family cohesion, sexual punitiveness, divorce) |
| (b) 138 (119 females) | (b) M = 46.1 ( SD = 11.17) | (b) Self-selected community | (2) CCMS-A | N/A | (2) MM > psychological adjustment problems | (2) Family background (gender, quality of childhood relationships, physical and verbal affection, parental divorce, family adaptability, family cohesion, parental sexual punitiveness, quality of interpersonal relationship, traditionality of father/mother) | |
| (c) 95 | (c) Self-selected community | (3) CCMS-A | N/A | (3) MM < positive relations with others, purpose in life | (3) N/A | ||
| Vranceanu, Hobfoll, & Johnson (2007) (USA) | 100 females | M = 28.92 ( SD = 10.52) | Recruited from gynaecological treatment centre for low-income women | CCMS-A | N/A | MM > stress, PTSD symptoms MM < social support | N/A |
| Sesar et al. (2008) (Bosnia-Herzegovina) | 458 (61% females) | 15-20 ( M = 17) | Third grade high-school students | Based on CCMS-A | MM = 57% | N/A | N/A |
| Price-Robertson, Bromfield, & Vassallo (2010) (Australia) | 1,000 (610 females) | 23-24 | Representative community sample | Self-developed scale, adapted from Cawson, Wattam, Brooker, & Kelly (2000) | MM = 8% | MM > depression, anxiety | N/A |
Notes: M = mean; SD = standard deviation; MM = multi-type maltreatment; FLEQ-P = The Family and Life Experience Questionnaire - Parent Version; N/A = not applicable; CCMS-A = Comprehensive Child Maltreatment Scales for Adults; CCMS-P = Comprehensive Child Maltreatment Scales for Parents; PTSD = post-traumatic stress disorder.
| Authors | N | Age (years) | Sample | Measure | 12-month incidence/childhood prevalence | Outcomes associated with PV | Predictors of PV |
|---|---|---|---|---|---|---|---|
| Finkelhor et al. (2005) (USA) | 2,030 | 10-17 ( N = 1,000); caregivers of 2-9 year olds ( N = 1,030) | Representative community sample | JVQ | Incidence: PV (4+ forms of victimisation) = 22% | PV > trauma symptomology (depression, anxiety, anger/aggression) | Low socioeconomic status, one-parent household, residing in large city |
| Finkelhor et al. (2007a) (USA) | 2,030 | 10-17 ( N = 1,000); caregivers of 2-9 year olds ( N = 1,030) | Representative community sample | JVQ | Incidence: PV (4+ forms of victimisation) = 22% | PV > trauma symptomology, re-victimisation in following year | Low socioeconomic status, gender (boys), race (African-American), one-parent household, residing in large city |
| Finkelhor, Ormrod, & Turner (2007b) (USA) | 1,467 | 10-17 (children 10-17 and caregivers of 2-9 year olds) | Representative community sample | JVQ | Incidence: PV (4+ forms of victimisation) = 23% | PV > re-victimisation in following years | Family problems (alcohol misuse, homelessness, family member imprisonment) |
| Richmond et al. (2009) (USA) | (a) 311 female | (a) 18-23 ( M = 19.1, SD = 1.33) | Female undergraduates | JVQ adult retrospective | (a) Prevalence: 97% (at least 1 type of PV); 40% (at least one type of victimisation in at least 5 of the 6 main PV categories) | (a) PV > psychological symptomology and distress (e.g., depression, anxiety, phobic anxiety, psychoticism), relationship quality, trauma symptomology | N/A |
| (b) 321 female | (b) 18-23 ( M = 19; SD = 1.32) | Female undergraduates | JVQ adult retrospective | (b) Prevalence: 98% (as above); 49% (as above) | (b) As above | N/A | |
| Finkelhor et al. (2009) (USA) | 1,467 | 10-17 (children 10-17 and caregivers of 2-9 year olds) | Representative community sample | JVQ adult Retrospective | Prevalence: 80% (at least 1 type of PV). Mean: 3.7 types of victimisation of lifetime. | PV > trauma symptomology | One-parent household, step-families |
| Ellonen & Salmi (2011) (Finland) | 13,459 (50% female) | 12-13 (sixth graders) and 15-16 (ninth graders) | Representative sample of students from mainland Finland | Modified JVQ | Incidence: PV (4 forms of victimisation) = 7% | PV > externalising, internalising, and social behaviour problems | Individual characteristics (e.g., factors of health, ways of spending free time, delinquency, alcohol, and drug use), family characteristics (e.g., family's socioeconomic situation, parental social control, and alcohol use) |
| Ford, Wasser, & Connor (2011) (USA) | 295 (38% female) | 5-17 ( M = 11.5, SD = 3.5) | Recruited from adolescent outpatient psychiatry clinic | Self-developed measure, using clinic admissions data | Incidence: PV (2+ of 7 forms of victimization) = 8% | PV > clinically severe externalising behaviour problems, psychiatric impairment, and PTSD diagnosis | N/A |
| Cuevas, Sabina, & Milloshi (2012) (USA) | 2,000 | 18-95 ( M = 47.76, SD = 16.24) | National sample of Latino women living in USA | LTVH | 40.3% reported at least one childhood victimisation experience | Re-victimisation in adulthood | N/A |
Notes: PV = polyvictimisation; JVQ = the Juvenile Victimization Questionnaire; M = mean; SD = standard deviation; PTSD = post-traumatic stress disorder; LTVH = Lifetime Trauma and Victimization History questionnaire.
| Groups | Depression | Anxiety | Illicit substance use | Antisocial behaviour | Long-term health problems | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Multi-type maltreatment (ref. = no maltreatment) | ||||||||||
| Single maltreatment | 1.95 ** | [1.26-3.02] | 1.58 * | [1.01-2.47] | 1.54 | [0.94-2.51] | 1.70 | [0.91-3.19] | 1.37 | [0.91-2.05] |
| Multi-type maltreatment | 3.75 *** | [2.26-6.23] | 2.72 *** | [1.61-4.58] | 1.63 | [0.86-3.07] | 1.90 | [0.86-4.20] | 1.52 | [0.90-2.56] |
| Polyvictimisation (ref. = no polyvictimisation) | ||||||||||
| Single victimisation | 1.06 | [0.67-1.69] | 1.14 | [0.72-1.80] | 1.30 | [0.79-2.12] | 1.26 | [0.64-2.48] | 1.48 | [0.99-2.22] |
| Low polyvictimisation | 0.99 | [0.59-1.63] | 1.08 | [0.66-1.77] | 1.24 | [0.73-2.10] | 1.08 | [0.50-2.29] | 1.77 ** | [1.16-2.68] |
| High polyvictimisation | 2.92 *** | [1.86-4.60] | 2.63 *** | [1.66-4.16] | 1.39 | [0.79-2.46] | 2.65 ** | [1.38-5.09] | 2.58 *** | [1.67-3.99] |
| Victimisation type (ref. = no victimisation) | ||||||||||
| Bullying only | 0.85 | [0.54-1.33] | 1.13 | [0.74-1.72] | 1.06 | [0.67-1.69] | 1.18 | [0.62-2.22] | 1.85 ** | [1.30-2.65] |
| Maltreatment only | 1.32 | [0.71-2.44] | 1.68 | [0.94-3.02] | 2.01 * | [1.09-3.68] | 1.12 | [0.41-3.03] | 0.82 | [0.42-1.58] |
| Maltreatment and bullying | 3.18 *** | [2.05-4.95] | 2.31 *** | [1.46-3.68] | 1.38 | [0.79-2.42] | 2.54 ** | [1.32-4.90] | 2.72 *** | [1.78-4.17] |
Note: OR = odds ratios; CI = 95% confidence intervals; * p < .05; ** p < .01; *** p < .001. See Table 2 for summary.
Price-Robertson, R., Higgins, D., & Vassallo, S. (2013). Multi-type maltreatment and polyvictimisation: A comparison of two research frameworks. Family Matters, 93, 84-98.
17 December 2013