Impacts of caring for a child with chronic health problems on parental work status and security
A longitudinal cohort study
You are in an archived section of the AIFS website
Caring for a family member with chronic health problems is known to have an effect on carers' emotional and physical health as well as on household finances and engagement in paid employment (Edwards, Higgins, Gray, Zmijewski, & Kingston, 2008). There is broad agreement in the literature that caring for a child with chronic health problems impacts negatively on maternal paid employment (DeRigne 2012; Stabile & Allin, 2012). More severe conditions and those of longer duration (DeRigne, 2012; Stabile & Allin, 2012) increase the likelihood of mothers reducing working hours or stopping work all together. Caring for children with a range of conditions including asthma (Baydar, Joesch, Kieckhefer, Kim, & Greek, 2007), autism (Kogan et al., 2008), other developmental disorders (Parish, Seltzer, Greenberg, & Floyd, 2004) and attention deficit hyperactivity disorder (ADHD) (Kvist, Nielsen, & Simonsen, 2013) has been shown to affect maternal employment.
Australian studies (Bittman, Hill, & Thomson, 2007; Edwards et al., 2008; Lee & Gramotnev, 2007) have shown that caring for a person with chronic health problems impacts negatively on the participation of the carer in the labour force; however, these studies make no distinction between caring for adults and caring for children. Cuskelly, Pulman and Hayes (1998), in a small case-control study of the employment status of couples caring for a child with a disability, reported that there are "a disproportionate number of mothers of a child with a disability in part-time employment in comparison to the mothers of children who were developing normally" (p. 319). Bourke-Taylor, Howie, and Law (2011) surveyed mothers of school-aged children with disabilities and concluded that they were less likely to work fulltime when their children reached school age compared with the mothers of typically developing children. Using data from the Longitudinal Study of Australian Children (LSAC), Yamauchi (2012) found that labour force participation by mothers caring for children with long-term health problems varied by the age of the child at the onset of health problems. Mothers of children aged 0-4 years reduced their labour force participation when their child started to show long-term health problems but mothers of children aged 4-8 years did not change their labour force participation in response to the onset of long-term health problems in their child.
A major limitation of the literature on the effect of children's chronic health problems on parental labour force participation is the paucity of longitudinal studies able to account for parental labour force participation early in the child's life. Findings of the longitudinal studies (Baydar et al., 2007; Kvist et al., 2013; Powers, 2003; Seltzer, Greenburg, Floyd, Pettee, & Hong, 2001; Yamauchi, 2012) suggest that the onset of chronic health problems in a child precipitates a reduction in the parents' labour force participation, although this might vary by the child's age at the onset of the health problem (Kvist et al., 2013; Yamauchi, 2012), by marital status of the mother (Baydar et al., 2007; Powers, 2003), by the duration of the child's condition (Kvist et al., 2013), and by type (Seltzer et al., 2001) and severity (Baydar et al., 2007) of the child's condition.
Labour force participation, particularly of mothers, has been the main focus of the literature on the impact of children's chronic health problems on parents' work; however, it is not the only parameter of work which may be adversely affected by the increased caring resulting from a child's chronic health problems. Other aspects of parental work, such as job tenure and job security, might be affected. No studies were found that have explored the impact of child chronic health problems on these aspects of parental work status.
Using data from the birth cohort (B cohort) of LSAC, this paper examines the impact on both parents' labour force participation, job tenure and job security when their child was aged 6 years and had experienced chronic health problems between the ages of 2 and 6 years. It adds to existing literature by accounting for parents' prior work status and by studying the effects on job tenure and security in addition to labour force participation.
Methods
This study draws on data from LSAC, a major study funded and managed by the Australian Department of Social Services (DSS) following the development of 10,000 children and families from around Australia. A two-stage clustered design was employed, with Medicare enrolment and activity databases held by the Health Insurance Commission providing the sampling frame.
The study commenced in 2004 with two cohorts: families with 0-1 year old infants (the B cohort) and families with 4-5 year old children (the K cohort). Interviews took place in the family home with the main respondent, usually the mother (99%). This study used data from Waves 2, 3 and 4 of the LSAC B cohort when the children were 2-3 years, 4-5 years and 6-7 years of age, respectively. The initial response rate for the B cohort was 64%, of whom 90% were present at Wave 2, 85% at Wave 3 and 80% at Wave 4 (Daraganova & Sipthorp, 2011). Only children with two resident parents at Waves 2 and 4 were included in the analysis. Wave 1 was not included, as there were insufficient data on chronic health problems in the children's first year of life.
It was predicted that caring for a child with chronic health problems would have a gendered effect on parents' employment. Among fathers, little difference in workforce participation, job tenure or job security was expected. Among mothers, it was expected that, compared with mothers whose child did not have a chronic health condition, mothers whose child did, would be less likely to be: (a) employed at Wave 4; and, if employed would be more likely to be: (b) working in casual jobs; and (c) more concerned about their job security.
Parental work status variables
The following measures of maternal and paternal work status and security at Wave 4 were analysed separately:
- labour force participation (yes/no) - unemployment and not available for work both treated as no;
- job tenure - casual vs permanent, fixed contract and other; and
- job security - very insecure, not very secure vs secure and very secure.
Childhood chronic health problems
Defined as the parental report of one or more of the following at more than one wave:
- child has chronic problem lasting or likely to last > 6 months based on the question: "Does the child have a condition or disability that has lasted, or is likely to last, for 6 months or more?";
- functional restriction based on the question: "Is the child restricted in everyday activities because of any of the following? - shortness of breath or breathing difficulties; chronic or recurring pain or discomfort; nervous or emotional condition; mental illness or condition requiring help or supervision; long-term effects of head injury, stroke or other brain damage; any other long-term conditions; receiving treatment or medication for any long-term conditions or ailments and still restricted";
- condition difficulties (Waves 3 and 4 only) based on the following question: "Does the child have a difficulty or delay in any of the following areas compared to children of a similar age? - communication (understanding or being understood by others); mobility (getting out of bed, moving around at home or at places away from home); self-care (eating, drinking, dressing, bathing); interacting or playing with others; coping with feelings or emotions; managing his/her behaviour; difficulty learning; other (everyday activities)";
- parents report needing more help with caring (Waves 3 and 4 only) based on the following question: "Does the child ever need more help or care than other children his/her own age for any problem?";
- child has a score on the Strengths and Difficulties Questionnaire of greater than the 95th centile for the whole cohort (Waves 3 and 4 only); and
- moderate/severe special health care needs (Wave 4 only) due to the following problems: eczema; vision problems; hearing problems; bone, joint or muscle problems; ADHD; anxiety disorder, depression; autism, Asperger's syndrome; diabetes; epilepsy or seizure disorder; chronic fatigue; hospitalisation for asthma.
Potential explanatory variables
Maternal and paternal work status measures at Wave 4 were analysed separately using the following variables:
- maternal or paternal work status measures at Wave 2;
- family material hardship at Wave 2 based on the following situations (with yes = 1, no = 0 responses, and responses summed to give a hardship score of 0-3 where 3 = 3 or more yes responses): difficulty raising $2,000 in a week; couldn't pay bills on time; couldn't pay mortgage on time; gone without meals; been unable to heat or cool home; pawned or sold something; sought assistance from welfare/community organisation.
- maternal or paternal chronic illness/disability at Wave 2 based on the following question: "Does mother/father have a condition or disability that has lasted, or is likely to last, for 6 months or more?" and
- maternal or paternal age.
Analysis
For the calculation of frequencies of included variables, sample weighting between Waves 2, 3 and 4 was used to reduce bias associated with attrition between waves (Daraganova & Sipthorp, 2011). To test the association of caring for a child with chronic health problems with a change in parents' work status between Waves 2 and 4, models were tested separately for the mother and father. Separate models were tested for each parental work status measure. Child with a chronic health problem (yes/no) was entered into the first model (Model 1 in Tables 1 and 2) to test the association with parental work status measures at Wave 4 before other potential explanatory variables were added. Next, to test if child chronic health problems were associated with a change in parental work status measures between Waves 2 and 4, parental work status measures at Wave 2 were added to the model (Model 2 in Tables 1 and 2). For each of the work status measures at Wave 4, the same measure at Wave 2 was added to the model.
Family hardship is known to be associated with chronic health problems in childhood (Blackburn, Spencer, & Read, 2010) and is also likely to be associated with non-participation in the labour force, casual job tenure and job insecurity. To test if this might explain associations noted in Models 1 and 2, family hardship at Wave 2 was added (Model 3 in Tables 1 and 2). There is a known association between parental chronic illness and chronic health problems in their children (Blackburn et al., 2010), and this potential explanatory variable was added in Model 4. The age of the mother or the father was added to create the final model (Model 5 in Tables 1 and 2), as parental age might impact on labour force participation, job tenure or job security.
Logistic regression modelling was undertaken using SPSS Version 20 (IBM Inc.). Logistic regression modelling produces estimates of the size of the impact of a variable on the outcome (in this study, parental work status at Wave 4). These are expressed as odds ratios. For clarity, in this paper these are referred to as "likelihoods".
Ethics approval
LSAC was approved by the Australian Institute of Family Studies Ethics Committee (Gray & Sanson, 2005).
Results
As shown in Figure 1, of 4,606 children present at Wave 2 of the LSAC B cohort, 3,309 were present at all three waves studied. Of these, 2,665 children were living with both parents at Waves 2 and 4. There were complete data for both maternal and paternal labour force participation but variable numbers of missing data for job tenure and security. Of the 2,665 children living with both parents at Waves 2 and 4, 218 (8%) were reported to have chronic health problems.
Figure 1: Participant flow diagram
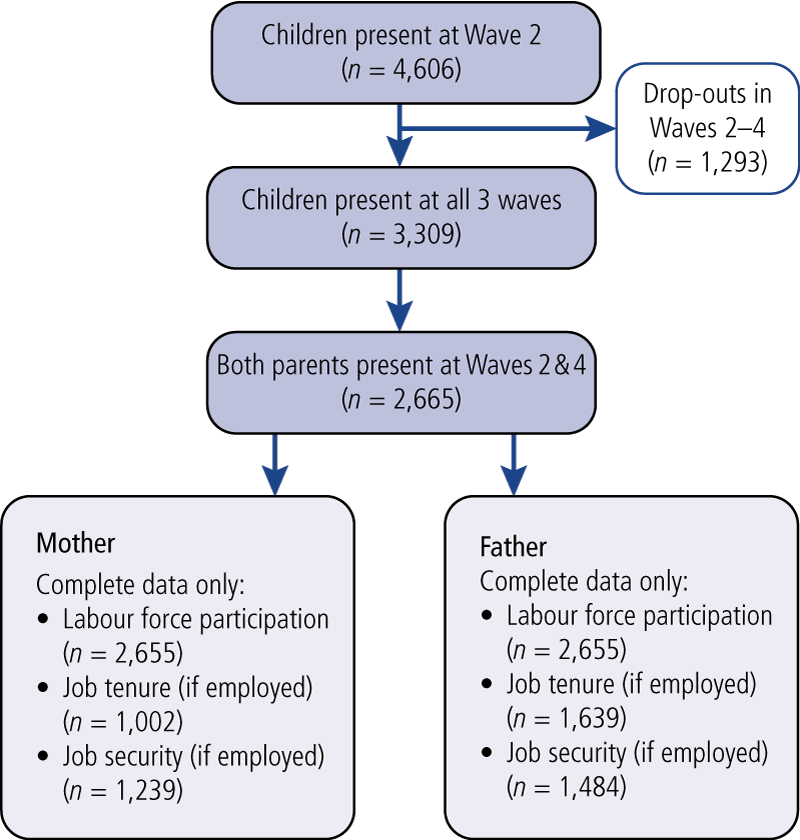
Table 1 shows that, before other explanatory variables were accounted for, mothers in households caring for children with chronic health problems were 1.5 times more likely to be not participating in the labour force, three times more likely to be in insecure employment and two times more likely to be in casual employment (Model 1). These associations were all reduced by the addition of all the explanatory variables to the model (Model 5), and only insecure employment remained statistically significant (that is less than a 5% likelihood that the statistical association had occurred by chance).
| Models a | Non-participation in labour force | Casual job tenure | Insecure job | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Model 1 | 1.5 | (1.1, 2.0) | 1.9 | (1.0, 3.8) | 2.9 | (1.6, 5.2) |
| Model 2 | 1.2 | (0.9, 1.7) | 1.8 | (0.9, 3.8) | 2.3 | (1.3, 4.3) |
| Model 3 | 1.2 | (0.8, 1.6) | 1.9 | (0.9, 3.9) | 2.4 | (1.3, 4.3) |
| Model 4 | 1.2 | (0.8, 1.6) | 1.8 | (0.9, 3.8) | 2.4 | (1.3, 4.3) |
| Model 5 | 1.1 | (0.80, 1.6) | 1.8 | (0.9, 3.7) | 2.4 | (1.3, 4.4) |
Notes: OR = odds ratio; CI = confidence interval. a Model 1 - child has chronic health problem only; Model 2 - Model 1 plus maternal work status variable at wave 2; Model 3 - Model 2 plus family hardship at wave 2; Model 4 - Model 3 plus maternal chronic illness at wave 2; Model 5 - Model 4 plus maternal age.
Unexpectedly, caring for a child with a chronic health problem also impacted on paternal work status (Table 2). Fathers in households caring for a child with a chronic health problem were two times more likely to not be participating in the labour force and 2.5 times more likely to be in casual employment at Wave 4 before other explanatory variables were added to the model (Model 1 in Table 2). With the potential explanatory variables added into the model (Model 5 in Table 2), fathers remained two times more likely to be in casual employment at Wave 4 and two times more likely to be non-participants in the labour force, although the latter became non-significant (greater than 5% likelihood that the association occurred by chance). The father's job security was unaffected by caring for a child with chronic health problems.
| Models a | Non-participation in labour force | Casual job tenure | Insecure job | |||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Model 1 | 1.9 | (1.1, 3.4) | 2.5 | (1.2, 5.4) | 1.0 | (0.5, 2.0) |
| Model 2 | 2.1 | (1.1, 4.1) | 2.3 | (1.0, 5.2) | 1.0 | (0.5, 2.0) |
| Model 3 | 1.9 | (1.0, 3.7) | 2.3 | (1.0, 5.1) | 1.0 | (0.5, 2.0) |
| Model 4 | 1.8 | (0.9, 3.5) | 2.3 | (1.0, 5.1) | 1.0 | (0.5, 2.0) |
| Model 5 | 1.9 | (1.0, 3.8) | 2.3 | (1.0, 5.3) | 1.0 | (0.5, 2.0) |
Notes: OR = odds ratio; CI = confidence interval. a Model 1 - child has chronic health problem only; Model 2 - Model 1 plus paternal work status variable at wave 2; Model 3 - Model 2 plus family hardship at wave 2; Model 4 - Model 3 plus paternal chronic illness at wave 2; Model 5 - Model 4 plus paternal age.
Discussion
The findings do not confirm the prediction that caring for a child with chronic health problems would negatively affect maternal but not paternal work status. Instead, the results indicated that the work status of both parents was adversely affected, albeit in different ways. For parents caring for a child with chronic health problems, the likelihood of maternal job insecurity and paternal labour force non-participation and casual job tenure when the child was 6 years old (LSAC B cohort, Wave 4) remained statistically significant after accounting for the same work status variables and other potential explanatory variables when the child was 2 years old (LSAC B cohort, Wave 2). Although the likelihood of mothers being in casual employment did not reach statistical significance, nonetheless, the result suggests that caring for a child with chronic health problems affects this aspect of maternal work status. The likelihood of maternal non-participation in the labour force at Wave 4 associated with caring for a child with chronic health problems became non-significant when maternal non-participation in the labour force was added into the model. Fathers' job security at Wave 4 was unaffected by caring for a child with chronic health problems.
Yamauchi (2012) reports on the effects of caring for a child with chronic health problems on parental labour force participation and job tenure; however, this appears to be the first study to report on job security in addition to labour force participation and job tenure. These findings indicate that a focus only on labour force participation is likely to underestimate the effects of caring for a child with chronic health problems on parental work. The existing literature is consistent in showing that mothers caring for children with chronic health problems are at increased risk of non-participation in the labour force. This study shows that mothers caring for children with chronic health problems were at increased risk of non-participation in the labour force, but the association was reduced and became non-significant once labour force participation, family hardship and maternal chronic illness earlier in the child's life were taken into account.
The longitudinal design of this study, with adjustment for prior labour force participation, may explain some of the differences with cross-sectional studies; however, published longitudinal studies that account for prior maternal labour force participation (Baydar et al., 2007; Kvist et al., 2013; Yamauchi, 2012), report a significant association of caring for a child with chronic health problems and maternal participation in the labour force. The contrast in findings may relate to the use of a different definition of chronic health problems (Yamauchi, 2012) or specific diagnoses rather than all-cause chronic problems (Baydar et al., 2007; Kvist et al., 2013), as well as a wider range of ages of children studied (Baydar et al., 2007; Kvist et al., 2013). Yamauchi (2012) reports mothers of children aged 4-8 years do not adjust their labour supply and Kvist et al. (2013) report no significant effect on maternal labour market participation (what they refer to as "extensive labour supply") before the age of 8 years when caring for a child with ADHD. The exclusion of lone parent households in our study may also partly explain different findings; Yamauchi (2012) and Baydar et al. (2007) include lone and couple households and Kvist et al. (2013) report on parental separation as well as labour force participation over the first 10 years of the life of the children in the study.
Strengths and limitations
The main strength of this study was the longitudinal data. With this data, the study could identify children with reported chronic health problems on more than one occasion at ages 2, 4 and 6 years, and account for prior parental work status in the analysis of the effects of child chronic health problems on parental work status when the child was 6 years of age. The analysis was limited to households with both parents present at the beginning and end of the period studied. This was both a strength and a limitation: a strength because the assumption that the impact on parental work status would be gendered could be tested; and a limitation as it excluded lone parent households. Caring for a child with chronic health problems has been shown in some studies to be more likely to reduce the mother's labour market participation in a lone parent household than in couple households (Powers, 2003; Baydar et al., 2007).
The main limitation of the study was the high proportion of missing data, especially for the analyses of job tenure and security. The reduced sample sizes resulted in a loss of power in the analysis, with wide confidence intervals around the likelihood estimates and consequent difficulties in interpreting the significance of some of the findings. Loss of data on some households may have biased the results if these households had characteristics systematically different from those included in the study. Adding parental work status at Wave 2 (the study baseline) may have led to an underestimate of the effects of caring for a child with chronic health problems if these problems were already established when the child was 2 years old; however, the underestimate is likely to be small as the proportion of children with chronic health problems increased between Waves 2 and 4. Change in parental work status may have been confounded by inclusion of health problems at Wave 2 in the definition of chronic health problems if parental work patterns had already been disrupted at baseline; however, the effect of this potential confounding is likely to be small as health problems had to be reported in more than one wave to meet the definition. If parental work patterns had changed by Wave 2, adjustment for parental work status at Wave 2 is likely to have further reduced the potential effect of confounding.
Conclusions
This study is consistent with published literature in that it finds there is an impact on parental work status of caring for a child with chronic health problems in the early years of life. The results further suggest an effect on job security and tenure as well as paternal labour force participation. The study did not confirm the prediction of a gendered effect on the mother rather than the father. The work status of both parents was adversely affected, although in different ways. The contrast of these findings with those of other longitudinal studies indicates the need for further research into this aspect of caring for a child with chronic health problems, using longitudinal datasets with large sample sizes.
References
- Baydar, N., Joesch, J. M., Kieckhefer, G., Kim, H., & Greek, A. (2007). Employment behaviors of mothers who have a child with asthma. Journal of Family Economic Issues, 28, 337-355.
- Bittman, M., Hill, T., & Thomson, C. (2007). The impact of caring on informal carers' employment, income and earnings: A longitudinal approach. Australian Journal of Social Issues, 42(2), 255-277.
- Blackburn, C. M., Spencer, N. J., & Read, J. M. (2010). Prevalence of childhood disability and the characteristics and circumstances of disabled children in the UK: Secondary analysis of the Family Resources Survey. BMC Pediatrics, 10, 21. doi:0.1186/1471-2431-10-21.
- Bourke-Taylor, H., Howie, L., & Law, M. (2011). Barriers to maternal workforce participation and relationship between paid work and health. Journal of Intellectual Disability Research, 55(5), 511-520.
- Cuskelly, M., Pulman, L., & Hayes, A. (1998). Parenting and employment decisions of parents with a preschool child with a disability. Journal of Intellectual & Developmental Disability, 23(4), 319-332.
- Daraganova, G., & Sipthorp, M. (2011). Wave 4 weights (LSAC Technical Paper No. 9).Melbourne: Australian Institute of Family Studies. Retrieved from <www.growingupinaustralia.gov.au/pubs/technical/index.html>.
- DeRigne, L. (2012). The employment and financial effects on families raising children with special health care needs: An examination of the evidence. Journal of Pediatric Health Care, 26(4), 283-290.
- Edwards, B., Higgins, D. J., Gray, M., Zmijewski, N., & Kingston, M. (2008). The nature and impact of caring for family members with a disability in Australia (Research Report No. 16). Melbourne: Australian Institute of Family Studies.
- Gray, M., & Sanson, A. (2005). Growing Up in Australia: The Longitudinal Study of Australian Children. Family Matters, 72, 4-9.
- Lee, C., & Gramotnev, H. (2007). Transitions into and out of caregiving: Health and social characteristics of mid-age Australian women. Psychology and Health, 22, 193-209.
- Kogan, M., Strickland, B., Blumberg, S., Singh, G., Perrin, J., & Van Dyck, P. (2008). A national profile of the health care experiences and family impact of autism spectrum disorder among children in the United States, 2005-2006. Pediatrics, 122, 1149-1158.
- Kvist, A. P., Nielsen, H. S., & Simonsen, M. (2013). The importance of children's ADHD for parents' relationship stability and labor supply. Social Science and Medicine, 88, 30-38.
- Parish, S. L., Seltzer, M. M., Greenberg, J. S., & Floyd, F. (2004). Economic implications of caregiving at midlife: Comparing parents with and without children who have developmental disabilities. Mental Retardation, 42(6), 413-426.
- Powers, E. T. (2003). Children's health and maternal work activity: Estimates under alternative disability definitions. Journal of Human Resources, 38(3), 522-556
- Seltzer, M., Greenburg, J., Floyd, F., Pettee, Y., & Hong, J. (2001). Life course impacts of parenting a child with a disability. American Journal on Mental Retardation, 106, 265-286.
- Stabile, M., & Allin, S. (2012). The economic costs of childhood disability. The Future of Children, 22(1), 65-96.
- Yamauchi, C. (2012). Children's health and parental labour supply. The Economic Record, 88(281), 195-213.
Nick Spencer is Emeritus Professor of Child Health at Warwick Medical School, University of Warwick in Coventry in the United Kingdom and Visiting Fellow at the National Centre for Epidemiology and Population Health, Australian National University in Canberra.
Acknowledgements: I am indebted to Dr Lyndall Strazdins, Associate Professor, National Centre for Epidemiology and Population Health (NCEPH) at the Australian National University, for sponsoring my application for a Visiting Fellowship at NCEPH and for her valuable contribution to the conception of this paper. This paper uses confidentialised unit record data from Growing Up in Australia: the Longitudinal Study of Australian Children. The study is conducted by the Department of Social Services (DSS, formerly Department of Families, Housing, Community Services and Indigenous Affairs), the Australian Institute of Family Studies (AIFS) and the Australian Bureau of Statistics (ABS). The findings and views reported in this paper are those of the author and should not be attributed to DSS, AIFS or ABS and cannot be taken in any way as expressions of government policy.
Spencer, M. (2014). Impacts of caring for a child with chronic health problems on parental work status and security: A longitudinal cohort study. Family Matters, 95, 24-29.
11 December 2014