Assessing the effectiveness of school-based sexual abuse prevention programs
You are in an archived section of the AIFS website
Background
Child sexual abuse is a serious problem for children worldwide with prevalence estimated at between 10-20% for girls and 5-10% for boys when sexual abuse is measured on a continuum from exposure through unwanted touching to penetrative assault prior to 18 years of age (Barth, Bermetz, Heim, Trelle, & Tonia, 2013; Ji, Finkelhor, & Dunne, 2013; Pereda, Guilera, Forns, & Gómez-Benito, 2009; Stoltenborgh, Van Ijzendoorn, Euser, & Bakermans-Kranenburg, 2011). Many individuals, however, do not ever disclose their abuse (London, Bruck, Ceci, & Shuman, 2005) nor report it to authorities (Wyatt, Loeb, Solis, & Carmona, 1999); the data available, therefore, may underestimate the true prevalence.
Child sexual abuse is associated with a range of adverse short- and long-term consequences. School-aged children who have experienced sexual abuse report higher rates of emotional and behavioural problems including patterns of inappropriate sexual behaviour (Berliner & Elliott, 2002; Putnam, 2003); social withdrawal, isolation and dissociation (Macdonald, 2001); deliberate self-harm and attempted suicide (Kendall-Tackett, Williams, & Finkelhor, 1993); and poor academic performance (Paolucci, Genius, & Violato, 2001). Health effects can include physical injury, teenage pregnancy and sexually transmitted infections (Kendall-Tackett et al., 1993). In adulthood, adjustment difficulties are evident including risky sexual behaviours and sexual revictimisation (Andrews, Corry, Slade, Issakids, & Swanston, 2004; Van Roode, Dickson, Herbison, & Paul, 2009); substance misuse (Kendall-Tackett, 2002); and mental health problems such as depression (Briere & Runtz, 1993), anxiety and phobias, post-traumatic stress disorder, dissociation and suicidal behaviours (Berliner & Elliot, 2002). There are also long-term effects on adult physical wellbeing including increased rates of cardiac disease, arthritis, chronic pain (Scott et al., 2011) and problems with gastrointestinal and reproductive health (Irish, Kobayashi, & Delahunty, 2010).
Owing to its complexity, prevalence and serious consequences, comprehensive public health approaches are required in child sexual abuse prevention efforts. Multiple types of interventions are required, targeting: (i) offenders and potential offenders; (ii) children and adolescents; (iii) situations in which child sexual abuse is known to occur; and (iv) communities (Smallbone, Marshall, & Wortley, 2008). School-based sexual abuse prevention programs target children and adolescents, typically by providing developmentally appropriate information about personal safety generally, and sexual abuse prevention specifically, including disseminating messages about appropriate help seeking and disclosure in the event of abuse or attempted abuse, and emphasising that children are not to blame (Duane & Carr, 2002). Consistent with a public health approach, schools have been considered a logical conduit for the provision of these prevention efforts because their primary function is to educate (Wurtele, 2009), programs can be delivered universally at comparatively little cost without stigmatising those at greater risk (Wurtele & Kenny, 2010), and the content of prevention programs aligns with school health curricula (Walsh et al., 2013).
School-based programs for prevention of child sexual abuse first appeared in the USA in the 1970s (Berrick & Gilbert, 1991; Briggs, 2012; Plummer, 1986) where program development was encouraged with an injection of funds via the Child Abuse Prevention and Treatment Act in 1974. A decade later, in 1984, the state of California was providing $11 million annually for school-based child sexual abuse prevention programs beginning in preschool (Berrick & Gilbert, 1991; Gilbert, Berrick, LeProhn, & Nyman, 1989) and a further decade later, approximately two-thirds of 10 to 16 year olds recalled their exposure to a child sexual abuse prevention program at some time during school (Finkelhor, Asdigian, & Dzuiba-Leatherman, 1995). Australia has followed suit but at a slower rate. Today, more than 30 programs are delivered in Australian primary schools reaching approximately one-fifth of school-aged children (Walsh, Brandon, Berthelsen, & Nicholson, under review).
The purpose of this paper is to introduce readers to the importance of systematic reviewing for understanding the effectiveness of school-based programs for the prevention of child sexual abuse. The most recent approaches to research synthesis are presented using findings from our recent systematic review of school-based child sexual abuse prevention interventions (Walsh, Zwi, Woolfenden, & Shlonsky, 2015). This work is situated within the dearth of strong evidence for the effectiveness of prevention interventions in the field of sexual violence generally (World Health Organization [WHO] & London School of Hygiene and Tropical Medicine, 2010), and child maltreatment specifically (WHO & International Society for Prevention of Child Abuse and Neglect, 2006). For the purpose of the review, child sexual abuse is defined as "the involvement of a child in sexual activity that he or she does not fully comprehend, is unable to give informed consent to, or for which the child is not developmentally prepared and cannot give consent, or that violates the laws or social taboos of society" (WHO, 1999, p. 15). The paper begins with a description of the features of rigorously conducted evaluation studies and a discussion of the differences between systematic reviews and more traditional literature reviews. A selection of key findings from the review are then presented, the complete details of which can be found in the freely accessible Cochrane Library online at <www.cochranelibrary.com/>.
Assessing evidence of effectiveness
Research methods can be used to answer many questions, including those that enquire about the effectiveness of treatment and prevention efforts. For these types of questions, there is a well-established hierarchy of design referring to the extent to which causality can be established (i.e., the extent to which we can say that the delivered program resulted in improved outcomes). In general, this hierarchy proceeds from anecdotal evidence (e.g., experience, practice wisdom, opinion) through to observational studies that do not have control or comparison groups, to well-controlled studies that include a control group (see Figure 1).
An independently-conducted randomized controlled trial (RCT) is the most rigorous research design that can be used to evaluate a program's effect upon program participants. There are other types of research designs that are valid for different types of questions (e.g., qualitative interviews with clients in order to ascertain how they might experience an intervention), but not all methods are equally valid for determining program effectiveness (Shlonsky & Mildon, 2014). An RCT measures a program's effect by randomly assigning individuals (or other units, such as schools, or classes within schools) into an intervention group, which receives the program, and a control group, which does not. A quasi-RCT differs slightly in that intervention and control groups are not randomly assigned and other strategies are used to minimise group differences. In both designs, data are collected before and after program participation, and compared. Research rigour is a constant challenge. Even within the design of seemingly rigorous RCT and quasi-RCT program evaluation studies, there are potential sources of bias, such as flawed randomisation methods, failing to account for attrition, and selective outcome reporting wherein only results demonstrating positive effects are reported (Higgins & Green, 2011). Thus, any assessment of whether a program or intervention is "effective" needs to consider carefully not just that there was an RCT but also the quality of the study and its applicability across contexts (Shlonsky & Benbenishty, 2014).
Systematic reviews
But what if there are numerous evaluation studies, conducted across many different contexts, using diverse methods? This poses a major problem for those trying to understand the research. A more traditional approach would be to conduct a narrative-style literature review, moving from one paragraph to another and describing the studies and their findings, and then coming up with an overall conclusion. Typically, narrative literature reviews do not use systematic and transparent methods to locate all of the evidence, nor do they use impartial methods for extracting findings and combining results to reach conclusions. Narrative reviews thus carry a high risk of author bias (Littell, 2008) and can amount to opinion pieces based on material that is readily available and supports what authors' believe. To address this shortcoming in narrative reviews, the field has turned to more systematic and rigorous approaches to reduce the risk of author bias (Shlonsky, Noonan, Littell, & Montgomery, 2011).
As shown in Table 1, systematic reviews differ from traditional narrative reviews on a number of dimensions and these variances are centred on the goal of reducing potential for author bias in the conduct of evidence reviews. Systematic reviews have several advantages over narrative reviews for research questions focusing on "what works" and for informing evidence-based decision-making. For example, systematic reviews use methods that are pre-defined, explicit and open to scrutiny. Systematic reviews attempt to identify all available evidence, and synthesise the totality of that evidence, both positive and negative. All evidence is assessed for methodological quality, such that conclusions about effectiveness can be drawn from the most reliable studies. In doing so, systematic reviews provide a high-level view from which to judge program effectiveness, hence their position at the top of the evidence hierarchy as shown in Figure 1.
| Systematic review | Narrative review |
|---|---|
| Pre-defined objectives | May or may not have defined objectives |
| Clear inclusion/exclusion criteria | Inclusion/exclusion criteria likely to be emergent |
| An explicit, replicable, exhaustive search strategy (including searches for unpublished studies to address publication bias) | Study selection depends on author selection and subjectivity |
| Systematic coding and analysis of included studies | Databases searched as required/preferred/available |
| Quality appraisal | Studies not appraised for quality |
| Meta-analysis (where possible to combine findings from a large number of studies) | Narrative synthesis, may be based on a subset of studies in a field |
| Protocol (project plan) for the review is developed in advance and undergoes peer review | Methodology not usually reported; difficult to replicate review |
| Review decisions are undertaken by at least two reviewers who work independently and compare results | Studies may be screened but criteria are not reported |
| Peer and editorial review | Peer and editorial review |
Source: Summarised from Gough, Oliver, & Thomas (2012); Higgins & Green (2011); and Torgerson (2003).
Figure 1: Levels of evidence for effectiveness questions
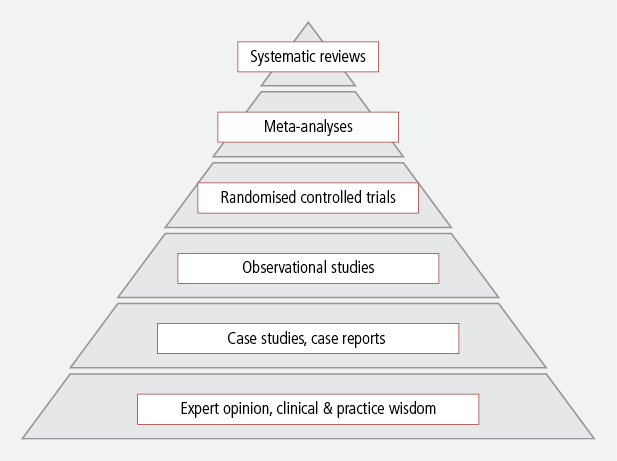
Source: Adapted from National Health and Medical Research Council (2009) and Puddy & Wilkins (2011).
Criticisms of systematic reviews have focused on paradigmatic claims that they are grounded in the positivist or scientific research traditions (Hammersley, 2001) and legitimacy claims that they are cannot provide clear answers to questions about the effectiveness of interventions that are often complex and have not yet been thoroughly evaluated (Petticrew, 2003). There are criticisms, also, that systematic reviews privilege evidence from experimental studies, which are known to be difficult to conduct, especially for the community-based, non-government organisations who deliver the bulk of prevention interventions in many fields (Flood, 2013; Kwok, 2013). However, as Courtney, Pergamit, Woolverton, & McDaniel (2014) assert, if the research question is about the effectiveness of a program or intervention that will be provided to children, it is our responsibility to know whether or not there is strong evidence that the program is effective, including how effective it might be, and for whom, and whether or not there are any negative impacts. This requires systematic, transparent and impartial methods. While we may want to know a great deal more about interventions, such as their underlying theories, driving paradigms and socio-cultural relevance, program effectiveness itself is not an ideological question. What is done with information about program effectiveness may be ideologically driven but at the very least we must start with what we know is likely to produce positive outcomes based on evidence produced with high levels of objective scrutiny.
The most rigorous systematic reviews are published by the Cochrane Collaboration (Cochrane Systematic Reviews), producing systematic reviews of health care interventions, and their social science counterpart, the Campbell Collaboration (Campbell Systematic Reviews), producing systematic reviews of social interventions in the areas of education, international development, justice, knowledge translation and implementation, and social welfare. Using the Cochrane and Campbell approach to systematic reviews, we conducted two systematic reviews (one original review, and a review update) on school-based child sexual abuse prevention programs.
The original Cochrane review of school-based programs for prevention of child sexual abuse (Zwi et al., 2007) was undertaken to provide an objective, rigorous and comprehensive assessment of all the evaluation studies in the area and to present this in a format accessible to policy-makers, practitioners and the general public. Several previous high-level reviews had been conducted including four meta-analytic studies (Berrick & Barth, 1992; Heidotting, Keiffer, & Soled, 1994; Rispens, Aleman, & Goudena, 1997; and Davis & Gidycz, 2000), but these reviews used less extensive search strategies and diverse inclusion criteria, rendering the varied findings incomparable between studies and across time. A Cochrane review, in contrast, is intended as a living document to be continually updated to maintain currency and relevance, and to reflect the growing literature base on a specific intervention (Higgins & Green, 2011).
For the review update we were aware that new studies had been published in the intervening years, and these needed to be assessed for inclusion in the review. The Cochrane risk of bias tool had been introduced (Higgins, Altman et al., 2011), synthesis methods had further evolved (e.g., Borenstein, Hedges, Higgins, & Rothstein, 2009), new databases had become available, and existing databases had extended their historical reach, meaning that a range of older studies were now readily available in electronic form.
The remainder of this paper is dedicated to reporting on the findings from the review update to demonstrate the strength of this approach to research synthesis.
Cochrane review process and methods
The methods for Cochrane reviews are set out in detail in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins & Green, 2011). The objective of the review was to systematically assess the effectiveness of school-based education programs for the prevention of child sexual abuse. Electronic searches of 15 major databases were conducted (see Box 1) using a pre-defined search strategy yielding almost 13,000 records. Hand searching of journals, grey literature and trial registers yielded a further 58 records (13,027 in total and 10,218 after duplicates were removed).
Box 1: Databases searched
1.Cochrane Central Register of Controlled Trials (CENTRAL), searched to September 2014
2.Ovid MEDLINE(R), searched 1946 to August 2014
3.EMBASE (OVID), searched 1980 to September 2014
4.PsycINFO (OVID), searched 1967 to September 2014
5.CINAHL (EBSCOhost), searched 1937 to September 2014
6.Social Science Citation Index (SSCI), searched 1970 to August 2014
7.Sociological Abstracts (ProQuest), searched 1952 to September 2013 (not available in September 2014)
8.Conference Proceedings Citation Indexes (CPCI-S and CPCI-SSH), searched to August 2014
9.ERIC (EBSCOhost), searched 1966 to September 2014
10.ERIC (ProQuest), searched 1966 to September 2013 (not available in September 2014)
11.Database of Abstracts of Reviews of Effects (DARE, via The Cochrane Library), searched to September 2014
12.Networked Digital Library of Theses and Dissertations (NDLTD via SCIRUS), searched to September 2013 (not available in September 2014 and no longer available via SCIRUS)
13.ClinicalTrials.gov, searched to September 2014
14.International Clinical Trials Registry Platform (ICTRP), searched to September 2014
15.Australasian Theses (via TROVE) searched to September 2014
Two study authors independently screened these search results according to pre-specified criteria (see Table 2) and discussed the findings with a third author. After discussion, it was agreed that 55 records merited full-text review. These records were reviewed by two authors, with 29 records (comprising 24 studies) meeting all inclusion criteria. Owing to the rigorous selection process and the very specific procedures used in Cochrane reviews to examine risk of study bias, it is reasonable to suggest that the studies included in this review are the most rigorous studies undertaken in this field to date.
| Criteria | Study inclusion details |
|---|---|
| Types of studies | Randomised controlled trails (RCTs); cluster RCTs, quasi-RCTs where participants were randomly allocated to intervention or control groups |
| Types of participants | Children (aged 5-12) and adolescents (aged 13-18) attending primary (elementary) or secondary (high) schools |
| Types of interventions | School-based programs primarily focusing on prevention of child sexual abuse (i.e., excluded relationship and dating violence prevention programs1) |
| Types of outcome measures | 1. Protective skills; 2. Knowledge; 3. Retention of skills over time; 4. Retention of knowledge over time; 5. Child anxiety or fear; 6. Disclosure |
A fundamental component of a Cochrane review is assessing risk of bias in included studies (Higgins & Green, 2011). The Cochrane Collaboration distinguishes study "bias" from study "quality" by taking the position that a particular study may be conducted to the highest possible standards, yet still carries a substantive risk of bias. For example, in the conduct of school-based trials, it is often unworkable to ensure that study participants are blinded to study conditions, as study participants will usually know if they are receiving an intervention program or not. In a Cochrane review, a specific tool is used for assessing risk of bias in included studies. Each study is subject to detailed review by two study authors with a third author called upon to adjudicate differences. Risk of bias is assessed for six domains, guided by key questions, and response options are recorded as "low risk", "high risk", or "unclear" as shown in Table 4. Unclear risk of bias is assigned when detail presented in the published studies was missing or limited (see Higgins & Green, 2011, Section 8.5).
A selection of results from the Cochrane review
In this section we provide a selection of results from the updated Cochrane review (see Walsh et al., 2015). As noted above, 24 program evaluation studies met the inclusion criteria. Research designs used in the studies were: randomised controlled trails where randomisation was undertaken at the individual student level (seven studies), cluster randomised controlled trials where randomisation took place at the school or classroom level, not at the individual student level (11 studies), and quasi-randomised controlled trials where randomisation may not have occurred for control groups, but other strategies were used to monitor group differences (e.g., in studies where wait-list control groups were used) (six studies).
The 24 studies included a total of 5,802 participants (99% of primary school age) with studies ranging in size from 74 to 1,269 participants. Trials evaluated the effectiveness of 15 distinct programs delivered in school settings in the USA (16 studies), Canada (three studies), China (one study), Germany (one study), Spain (one study), Taiwan (one study) and Turkey (one study). No Australian studies met the inclusion criteria. Only one rigorous Australian evaluation study has ever been conducted (Michaelson, 2001), and this was a PhD study, which we classified as a controlled before- after study (see Higgins & Green, 2011, Section 13.1.2). However, because participants were not randomised to intervention or control groups, it did not meet the inclusion criteria for this review.2
Although the majority of studies were conducted in the USA, the participant samples were not limited to those from white or Anglo-European backgrounds. Two studies included 100% Chinese participants, and six studies had diverse samples including participants from African-American, Asian, Hispanic, Latin-American and Middle-Eastern backgrounds. Ethnicity data were not reported in 10 studies. Important sample demographics such as parental socio-economic position, religious affiliation and school achievement data were not reported in any study. Mean age at baseline was in the range 5.8 to 13.44 years, indicating that the studies were conducted with children at the ages of greatest risk (i.e., 7-12 years) (Finkelhor & Baron, 1986).
Key features of programs in the studies are shown in Table 3. Programs typically had multiple components including the teaching of body safety rules and prevention concepts such as body ownership, public and private body parts, types of touches, types of secrets and who to tell. Programs did not focus narrowly on "self-protective skills" (also known as "protective behaviours") such as the "no-go-tell" sequence, although this was practised in some programs as part of an array of content. The teaching methods used in the programs were sound, comprising the kinds of strategies typically observed in effective primary school classrooms and based on social learning theories, such as modelling, social reinforcement, shaping and feedback (Hattie, 2009). These program characteristics were not well reported in some studies. Hence, future program evaluation studies should include standardised data collection tools for program contents, methods, delivery formats, duration and frequency.
| Key feature | Components common to programs |
|---|---|
| Program contents or topics (curriculum) | Safety or body safety rules (average of 2-6 rules)
Prevention concepts (body ownership, private body parts, distinguishing appropriate and inappropriate touches, distinguishing types of secrets, whom to tell). |
| Program teaching methods (pedagogy) | Instruction, rehearsal, practice, role play, modelling, social reinforcement, shaping, feedback, group mastery, review |
| Program delivery formats | Film, video, DVD, theatrical play/performance, multimedia presentation, songs, puppets, workbooks, comics, storybooks, games |
| Program duration | Mostly brief interventions of less than 90 minutes in total duration (a minimum of 1 x 45-minute session through to a maximum of 8 x 20-minute sessions) |
| Program frequency | Frequency of program presentation was poorly reported in all studies. |
The overall quality of evidence of studies in this review was assessed as moderate as a result of unclear risk of selection bias (in some studies we were unsure that proper randomisation was achieved), high or unclear risk of detection bias (in some studies, we were unsure that outcome assessors had been adequately blinded to study conditions), and high or unclear risk of attrition bias (in some studies we were unsure whether drop-out rates affected study outcomes) (see Table 4). We found that many studies did not apply appropriate statistical analyses to properly account for the "clustering" or grouping of students in classes or schools.
| Risk of bias domain | Example of key questions | Our judgement |
|---|---|---|
| Random sequence generation (selection bias) | Do study authors make an explicit statement about random assignment? | Low risk = 2/24 studies
High risk = 0/24 studies Unclear = 22/24 studies |
| Allocation concealment (selection bias) | Do study authors report a method for concealing allocation of children to intervention and control groups? | Low risk = 0/24 studies
High risk = 2/24 studies Unclear = 22/24 studies |
| Blinding of participants and personnel (performance bias) | Do study authors report procedures for blinding so that children, parents, teachers do not know whether intervention or control condition is received? | Low risk = 3/24 studies
High risk = 14/24 studies Unclear = 7/24 studies |
| Blinding of outcome assessment (detection bias) | Do study authors report procedures for blinding of staff responsible for outcome assessment (i.e., pre- and post-testing of children)? | Low risk = 10/24 studies
High risk = 7/24 studies Unclear = 7/24 studies |
| Incomplete outcome data (attrition bias) | Do study authors report study attrition (drop out) and exclusion? | Low risk = 5/24 studies
High risk = 6/24 studies Unclear = 12/24 studies |
| Selective reporting (reporting bias) | Do study authors report complete data for all study outcomes? | Low risk = 19/24 studies
High risk = 5/24 studies Unclear = 0/24 studies |
A detailed presentation of our meta-analysis for the Cochrane review is beyond the scope of this paper; however, in Table 5 we summarise the findings of the outcome measures that were the focus of our data synthesis and key findings are presented below.
Because there are, as yet, no Australian evaluation studies meeting the standard for inclusion in this review, it is important that we make a strong caveat. As previously noted, many school-based child sexual abuse prevention programs are currently delivered in Australian primary schools. It was beyond the scope of this systematic review to assess the extent to which programs delivered in Australian schools are similar to or different from those in this review. The Cochrane review contains a very detailed examination of the contents of the programs in the "Characteristics of Included Studies" tables (Walsh et al., 2015, pp.43-87) and the findings reported here apply only to the types of programs included in the review, and are condensed for this paper in Table 3.
| Outcome | Measurement | Meta-analysis (yes/no), number of studies, number of participants | Finding | |
|---|---|---|---|---|
| 1. Skills (protective behaviours) | Simulated risk situation | Yes, 3 studies (n = 102) | School-based programs were effective in increasing participants' skills. | |
| 2. Knowledge (factual knowledge) | Questionnaire | Yes, 18 studies (n = 4,657) | School-based programs were effective in increasing participants' knowledge. | |
| 3. Knowledge (applied knowledge) | Vignettes | Yes, 11 studies (n = 1,688) | ||
| 4. Retention of skills over time | Simulated risk situation | No | There were insufficient studies with follow-up data to enable assessment of retention over time. | |
| 5. Retention of knowledge over time | Questionnaire | Yes, 4 studies (n = 929) | Knowledge gains were not significantly eroded 1-6 months after program participation. | |
| 6. Harm (child anxiety or fear) | Parent or child report | Yes, 3 studies (n = 795) | Programs do not increase or decrease children's anxiety or fear. | |
| 7. Disclosure | Records of reports at school or statutory level | Yes, 3 studies (n = 1788) | Children exposed to programs had greater odds of disclosure; however, the result was not significant and incorrect analyses were used in some studies. | |
Summary of findings
1. We found clear evidence of improvements in self-protective skills (measured using a role-play scenario). Children who received a program had a significant five times greater odds of using the skills they learned in the program when confronted with a role-play of a potential risk situation that was conducted immediately after program completion.
2. School-based programs were effective in increasing participants' factual knowledge of program concepts (measured via questionnaire), irrespective of the program type. Children who received a program had mean knowledge scores significantly higher than children who did not receive a program.
3. School-based programs were effective in increasing participants' applied knowledge of program concepts (measured via vignettes). Again, children who received a program, had mean knowledge scores significantly higher than children who did not receive a program. Effect sizes for both types of knowledge gains as a result of program participation were within the "zone of desired effects" for school-based interventions, that is 0.40 effect size and above (Hattie, 2009, p. 18). Program effects were therefore comparable to other educational interventions using sound teaching methods, and exceeded the knowledge effects found for other primary prevention programs such as relationship and dating violence prevention programs (Fellmeth et al., 2013).
4. Analysis of data on retention of participants' self-protective skills over time was not able to be conducted, as complete data were unavailable.
5. Knowledge gains (measured via questionnaires) seemed to persist in the short term and were not significantly eroded one to six months after the intervention.
6. School-based programs did not appear to cause harm (as measured by anxiety or fear questionnaires completed by children or parents). Children who experienced a program also experienced slightly less anxiety or fear than children who had not experienced a program but the result was not significant. None of the included studies measured parental anxiety or fear, hence there is a need for ongoing monitoring of both positive and negative short- and long-term effects.
7. Children who had participated in school-based programs had greater odds of disclosing their abuse than children who had not received a program; however, the result was not significant and there was substantial uncertainty around this result as the data were gathered differently in different studies, and many studies used incorrect analytical methods that did not take account of the clustering of children in classes and schools. We noted that there is need for future program evaluations to routinely collect disclosure data and/or to conduct data linkage to statutory child protection records so that studies can assess actual prevention of child sexual abuse in the longer term.
Conclusions
Our systematic review and meta-analysis set out to assess the evidence of effectiveness of school-based education programs for the prevention of child sexual abuse.
Strengths and limitations of the review
The most obvious strengths of a Cochrane review are its comprehensive and replicable search strategy, and objective approach to screening and study inclusion. We searched widely for studies in peer-reviewed journals, dissertations and theses, and grey literature, which enabled us to make equitable assessment of the most rigorous studies in the field rather than selecting studies based on our ideological, professional or empirical preferences. We included only studies using RCT, cluster RCT or quasi-RCT research designs where participants were allocated to intervention or control groups via a documented randomisation process.
Strengths and weaknesses of the available evidence
The available evidence is skewed somewhat towards studies conducted in North America mainly during the 10-year period from 1986-1996. However, participant samples within the studies were diverse enough for us to be comfortable that their findings have broader applicability. There were no Australian studies included in this review, however we are aware that an Australian program trial is currently underway and has been registered with the Australian New Zealand Clinical Trials Registry.3 We noted many oversights in the reporting of findings for individual studies including: failure to adequately report on demographic characteristics of study samples, poor reporting of study attrition, incomplete reporting of program characteristics, inadequate baseline comparisons of intervention and control groups, use of a wide range of measurement instruments (e.g., questionnaires), inappropriate statistical analysis techniques, and lack of longitudinal follow-up of study participants. We suggest that the reporting of future evaluation studies can be substantially improved if study authors use the Consolidated Standards of Reporting Trials (CONSORT) statement (Shulz, Altman, & Moher, 2010) as a standard checklist for reporting on trials of school-based interventions.
Implications for policy and practice
In undertaking this review of prevention programs directed towards children of school age, we are not suggesting that such programs can be a substitute for adults' and society's responsibility to ensure child safety. We emphasise that "increasing children's knowledge in this area does not mean they are in any way responsible for abuse which might then occur by their not being able to apply this knowledge in an actual abuse situation" (Walsh et al., 2015, p. 32). In keeping with Smallbone et al.'s (2008) theory of integrated prevention, programs directed towards children must be part of comprehensive prevention efforts encompassing multiple prevention targets such as offenders and potential offenders, risk environments and situations, and wider communities. Risk environments include online settings, and we noted that in our searches of thousands of papers, only a small handful had addressed web-based, electronic or multimedia prevention programs conducted with children in schools. Very few evaluations had been published and none were of sufficient quality to be included in this review.
Unanswered questions and future research
Research must be undertaken to more rigorously evaluate programs generally, and in Australia, in particular. Further research is needed to address the relationship between program participation and prevention of child sexual abuse. This implies the need for longitudinal studies with research designs enabling long-term follow-up of program participants beyond the point in childhood at which programs are received and, ideally, into adulthood. However, even if such longitudinal studies are conducted, they may not provide conclusive evidence regarding the ability of programs to prevent child sexual abuse because child sexual abuse often remains undisclosed (London et al., 2005).
The Cochrane review reported here provides the most comprehensive and rigorous evidence to date of the combined effects across the highest quality studies. As such the results are likely to represent a conservative estimate of program effects. We conclude that "even if successful in only a small proportion of situations, given the prevalence of child sexual abuse, it is possible that the skills and knowledge learned in prevention programs may be of assistance to a considerable number of children" (Walsh et al., 2015, p. 32). For a copy of the review, please see the Cochrane Database of Systematic Reviews via the Cochrane Library at <www.cochranelibrary.com>.
Endnotes
1 These programs are addressed in a separate Cochrane Review by Fellmeth, Heffernan, Nurse, Habibula, & Sethi (2013).
2 We are aware that an Australian cluster RCT is currently underway (Zimmer-Gembeck, Shanley, Walsh, Hawkins, & Lines, 2013, see <www.sdrs.info/research.php>).
3 See <tinyurl.com/gnbzqcb>.
References
- Andrews, G., Corry, J., Slade, T., Issakids, C., & Swanston, H. (2004). Child sexual abuse. In M. Ezzati, A. D. Lopez, A. Rodgers & C. J. L. Murray (Eds.), Comparative quantification of health risks: Global and regional burdens of disease attributable to selected major factors (Vol. 2, pp. 1851-1940). Geneva: World Health Organization.
- Barth, J., Bermetz, L., Heim, E., Trelle, S., & Tonia, T. (2013). The current prevalence of child sexual abuse worldwide: A systematic review and meta-analysis. International Journal of Public Health, 58(3), 469-483.
- Berliner, L., & Elliott, D. (2002). Sexual abuse of children. In J. Myers, L. Berliner, J. Briere, C. Hendrix, C. Jenny & T. Reid (Eds.), The APSAC handbook on child maltreatment (2nd ed.) (pp. 55-78). Thousand Oaks, CA: Sage Publications.
- Berrick, J. D., & Barth, R. P. (1992). Child sexual abuse prevention: Research review and recommendations. Social Work Research & Abstracts, 28(4), 6-16.
- Berrick, J. D., & Gilbert, N. (1991). With the best of intentions: The child sexual abuse prevention movement. New York: The Guilford Press.
- Borenstein, M., Hedges, L. V., Higgins, J. P. T., & Rothstein, H. R. (2009). Introduction to meta-analysis. Chichester, UK: Wiley.
- Briere, J., & Runtz, M. (1993). Childhood sexual abuse: Long-term sequelae and implications for psychological assessment. Journal of Interpersonal Violence, 8(3), 312-330.
- Briggs, F. (2012). Child protection: The essential guide for teachers and other professionals whose work involves children. Docklands, Vic: JoJo Publishing.
- Courtney, M. E., Pergamit, M., Woolverton, M., & McDaniel, M. (2014). Challenges to learning from experiments: Lessons from evaluating independent living services. In A. Shlonsky & R. Benbenishty (Eds.), From evidence to outcomes in child welfare: An international reader (pp.117-132). New York: Oxford University Press.
- Davis, M. K., & Gidycz, C. A. (2000). Child sexual abuse prevention programs: A meta-analysis. Journal of Clinical Child Psychology, 29(2), 257-265. doi: 10.1207/S15374424jccp2902_11.
- Duane, Y., & Carr, A. (2002). Prevention of child sexual abuse. In A. Carr (Ed.), Prevention: What works with children and adolescents? A critical review of psychological prevention programmes for children, adolescents and their families (pp. 181-204). New York: Brunner-Routledge.
- Fellmeth, G. L. T., Heffernan, C., Nurse, J., Habibula, S., & Sethi, D. (2013). Educational and skills-based interventions for preventing relationship and dating violence in adolescents and young adults. Cochrane Database of Systematic Reviews 2013, Issue 6. Art. No.:CD004534. doi: 10.1002/14651858.CD004534.pub3.
- Finkelhor, D., & Baron, L. (1986). Risk factors for child sexual abuse. Journal of Interpersonal Violence, 1(1), 43-71.
- Finkelhor, D., Asdigian, N., & Dziuba-Leatherman, J. (1995). Victimization prevention programs for children: A follow-up. American Journal of Public Health, 85(12), 1684-1689.
- Flood, M. (2013). Evaluation capacity building in the Respect, Responsibility and Equality program: Report on Stage 1 (2008-2010). Melbourne, Vic: Victorian Health Promotion Foundation. Retrieved from <www.vichealth.vic.gov.au/search/pvaw-evaluation-trends>.
- Gilbert, N., Berrick, J. D., LeProhn, N., & Nyman, N. (1989). Protecting children from sexual abuse: Does preschool training work? New York: Lexington Books.
- Gough, D., Oliver, S., & Thomas, J. (2012). An introduction to systematic reviews. London: Sage.
- Hammersley, M. (2001). On 'systematic' reviews of research literatures: A 'narrative' response to Evans & Benefield. British Journal of Educational Research, 27(5), 543-554.
- Hattie, J. (2009). Visible learning: A synthesis of over 800 meta-analyses relating to achievement. New York: Routledge.
- Heidotting, T., Keiffer, S., & Soled, S. W. (1994). A quantitative synthesis of child sexual abuse prevention programs. Paper presented at the American Educational Research Association, New Orleans.
- Higgins, J. P. T., Altman, D. G., Gøtzsche, P., Jüni, P., Moher, D., Oxman, A.D. et al. (2011). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. British Medical Journal, 343(7829), 889-893.
- Higgins, J. P. T., & Green, S. (2011). Cochrane handbook for systematic reviews of interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. Retrieved from <handbook.cochrane.org>.
- Irish, L., Kobayashi, I., & Delahunty, D. L. (2010). Long-term physical health consequences of childhood sexual abuse: A meta-analytic review. Journal of Pediatric Psychology, 35(5), 450-461.
- Ji, K., Finkelhor, D., & Dunne, M. (2013). Child sexual abuse in China: A meta-analysis of 27 studies. Child Abuse & Neglect, 37(9), 613-622.
- Kendall-Tackett, K. (2002). The health effects of childhood abuse: Four pathways by which abuse can influence health. Child Abuse & Neglect, 26(6-7), 715-730.
- Kendall-Tackett, K. A., Williams, L. M., & Finkelhor, D. (1993). Impact of sexual abuse on children: A review and synthesis of recent empirical studies. Psychological Bulletin, 113, 164-180.
- Kwok, W. L. (2013). Evaluating preventing violence against women initiatives: A participatory and learning-oriented approach for primary prevention in Victoria. Melbourne, Vic: Victorian Health Promotion Foundation. Retrieved from <www.vichealth.vic.gov.au/search/pvaw-evaluation-trends>.
- Littell, J. H. (2008). Evidence-based or biased? The quality of published reviews of evidence-based practices. Children & Youth Services Review, 30(11), 1299-1317. doi:10.1016/j.childyouth.2008.04.001.
- London, K., Bruck, M., Ceci, S. J., & Shuman, D. W. (2005). Disclosure of child sexual abuse: What does the research tell us about the ways that children tell? Psychology, Public Policy, and Law, 11(1), 194-226.
- Macdonald, G. (2001). Effective interventions for child abuse and neglect: An evidence-based approach to planning and evaluating interventions. Chichester: John Wiley & Sons.
- Michaelson, R. (2001). Development, evaluation and revision of the school-based child sexual abuse prevention program (CSAPP Project). Unpublshed PhD thesis, Victoria University of Technology, St Alban's, Vic.
- National Health and Medical Research Council (NHMRC). (2009). NHMRC additional levels of evidence and grades for recommendations for guideline developers. Canberra: National Health and Medical Research Council. Retrieved from <www.nhmrc.gov.au/_files_nhmrc/file/guidelines/developers/nhmrc_levels_grades_evidence_120423.pdf>.
- Paolucci, E. O., Genius, M. L., & Violato. (2001). A meta-analysis of the published research on the effects of child sexual abuse. The Journal of Psychology, 135(1), 17-36.
- Pereda, N., Guilera, G., Forns, M., & Gómez-Benito, J. (2009). The international epidemiology of child sexual abuse: A continuation of Finkelhor (1994). Child Abuse & Neglect, 33(6), 331-342.
- Petticrew, M. (2003). Why systematic reviews reach uncertain conclusions. British Medical Journal, 326, 756-758.
- Plummer, C. A. (1986). Prevention education in perspective. In M. Nelson, & L. Clark, (Eds.). An educator's guide to preventing child sexual abuse. Santa Cruz, CA: Network Publications.
- Puddy, R. W., & Wilkins, N. (2011). Understanding evidence part 1: Best available research evidence. A guide to the continuum of evidence of effectiveness. Atlanta, GA: Centers for Disease Control and Prevention (National Center for Injury Prevention and Control, Division of Violence Prevention). Retrieved from <www.cdc.gov/violenceprevention/pdf/understanding_evidence-a.pdf>.
- Putnam, F. W. (2003). Ten-year research update review: Child sexual abuse. Journal of the American Academy of Child and Adolescent Psychiatry, 42(3), 269-278.
- Rispens, J., Aleman, A., & Goudena, P. P. (1997). Prevention of child sexual abuse victimisation: A meta-analysis of school programs. Child Abuse & Neglect, 21(10), 975-987. doi: 10.1016/S0145-2134(97)00058-6.
- Schulz, K. F., Altman, D. G., & Moher, D. for the CONSORT Group. (2010). CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. British Medical Journal, 340, 698-702.
- Scott, K. M., Von Korff, M., Angermeyer, M. C., Benjet, C., Bruffaerts, R., de Girolamo, G. et al. (2011). Association of childhood adversities and early-onset mental disorders with adult-onset chronic physical conditions. Archives of General Psychiatry, 68(8), 838-844.
- Shlonsky, A., & Benbenishty, R. (2014). From evidence to outcomes in child welfare. In A. Shlonsky & R. Benbenishty (Eds.), From evidence to outcomes in child welfare: An international reader (pp. 3-23). New York: Oxford University Press.
- Shlonsky, A., & Mildon, R. (2014). Methodological pluralism in the age of evidence-informed practice and policy. Scandinavian Journal of Public Health, 42(13), 18-27. doi: 10.1177/1403494813516716.
- Shlonsky, A., Noonan, E., Littell, J. H., & Montgomery, P. (2011). The role of systematic reviews and the Campbell Collaboration in the realization of evidence-informed practice. Clinical Social Work Journal, 39(4), 362-368. doi: 10.1007/s10615-010-0307-0.
- Smallbone, S. W., Marshall, W. L., & Wortley, R. K. (2008). Preventing child sexual abuse: Evidence, policy and practice. Cullompton, UK: Willan Publishing.
- Stoltenborgh, M., Van Ijzendoorn, M. H., Euser, E. M., & Bakermans-Kranenburg, M. J. (2011). A global perspective on child sexual abuse: Meta-analysis of prevalence around the world. Child Maltreatment, 16(2), 79-101.
- Torgerson, C. (2003). Systematic reviews. London: Continuum.
- Van Roode, T., Dickson, N., Herbison, P., & Paul, C. (2009). Child sexual abuse and persistence of risky sexual behaviors and negative sexual outcomes over adulthood: Findings from a birth cohort. Child Abuse & Neglect, 33(3), 161-172.
- Walsh, K., Brandon, L., Berthelsen, D., & Nicholson, J. (under review). Prevention programs targeting child sexual abuse prevention in primary schools: Current content and strategies.
- Walsh, K., Berthelsen, D., Nicholson, J.M., Brandon, L., Stevens, J., & Rachele, J.N. (2013) Child sexual abuse prevention education: A review of school policy and curriculum provision in Australia. Oxford Review of Education, 39(5), 649-680.
- Walsh, K., Zwi, K., Woolfenden, S., & Shlonsky, A. (2015). School-based programmes for prevention of child sexual abuse (Review). Cochrane Database of Systematic Reviews 2015, Issue 4. Art. No.: CD004380. doi: 10.1002/14651858.CD004380.pub3.
- World Health Organization. (1999). Report of the consultation on child abuse prevention (document WHO/HSC/PVI/99.1). Geneva, Switzerland: World Health Organization. Retrieved from <apps.who.int/iris/handle/10665/65900>.
- World Health Organization and International Society for Prevention of Child Abuse and Neglect. (2006). Preventing child maltreatment: A guide to taking action and generating evidence. Geneva, Switzerland: World Health Organization. Retrieved from <www.who.int/violence_injury_prevention/publications/violence/child_maltreatment/en/>.
- World Health Organization and London School of Hygiene and Tropical Medicine. (2010). Preventing intimate partner and sexual violence against women: Taking action and generating evidence. Geneva, Switzerland: World Health Organization. Retrieved from <www.who.int/reproductivehealth/publications/violence/9789241564007/en/>.
- Wurtele, S. K. (2009). Preventing sexual abuse of children in the twenty-first century: Preparing for challenges and opportunities. Journal of Child Sexual Abuse, 18(1), 1-18.
- Wurtele, S. K., & Kenny, M. C. (2010). Primary prevention of child sexual abuse: Child- and parent-focused approaches. In K. L. Kaufman (Ed.), The prevention of sexual violence: A practitioner's sourcebook (pp. 107-134). Holyoke, MA: NEARI Press.
- Wyatt, G. E., Loeb, T. B., Solis, B., & Carmona, J. V. (1999). The prevalence and circumstances of child sexual abuse: changes across a decade. Child Abuse & Neglect, 23(1), 45-60.
- Zimmer-Gembeck, M., Shanley, D., Walsh, K., Hawkins, R., & Lines, K. (2013). Empowering and protecting children by enhancing knowledge, skills and well-being: A randomised controlled trial of Learn to BE SAFE with Emmy TM. Proposal for Australian Research Council Linkage Project Funding Commencing 2013.
- Zwi, K. J., Woolfenden, S. R., Wheeler, D. M., O'Brien, T. A., Tait, P., & Williams, K. W. (2007). School-based education programs for prevention of child sexual abuse (Review). Cochrane Database of Systematic Reviews, 3(1), 1-30. doi: 10.1002/14651858.CD004380.pub2.
Kerryann Walsh is at the School of Early Childhood, Faculty of Education, Queensland University of Technology, Karen Zwi is at the School of Women's and Children's Health, University of New South Wales & Sydney Children's Hospital Network, Susan Woolfenden is at the School of Women's and Children's Health, University of New South Wales & Sydney Children's Hospital Network, and Aron Shlonsky is at the School of Health Sciences, University of Melbourne.
Acknowledgements: A version of this paper was presented at the 13th Australian Institute of Family Studies Conference. The authors acknowledge the original review team: Karen Zwi, Susan Woolfenden, Danielle M Wheeler, Tracey O'Brien, Paul Tait, and Katrina J. Williams. Searches for this review were conducted by Margaret Anderson, Trials Search Coordinator for the Cochrane Developmental, Psychosocial and Learning Problems Group. In-kind support for the review was provided by our respective institutions. The research was supported by an ARC Discovery Project grant (DP1093717). We are especially grateful for the comments of external Cochrane reviewers and statisticians, and for the expert advice from the Cochrane Developmental, Psychosocial and Learning Problems Group editorial base: Prof. Geraldine MacDonald (Coordinating Editor), Joanne Wilson (Managing Editor), and Gemma O'Loughlin (Assistant Managing Editor).
17 March 2016