Doing gender overnight?
Parenthood, gender and sleep quantity and quality in Australia
You are in an archived section of the AIFS website
March 2016
Download Family Matters article
Abstract
The importance of sleep cannot be underestimated, as sleep affects domains such as physical and mental health, work-related productivity, and longevity. Yet, we know surprisingly little about the social determinants of sleep in contemporary Australia. International evidence suggests that parenthood and gender are important factors influencing individuals' sleep quantity and quality, with parents sleeping less and worse than non-parents and mothers sleeping less and worse than fathers. We provide first-time evidence of these patterns in the Australian context using data from the 2013 wave of the Household, Income and Labour Dynamics in Australia Survey and multivariate regression models. Our findings are consistent with those from previous US and UK research, and indicate that sleep quantity and sleep quality are greater amongst (i) childless individuals than parents, (ii) parents of young children (ages 2 to 4) than parents of very young children (ages 0 and 1), and (iii) fathers than mothers. We take these results as evidence of gender-unequal sleep arrangements in Australian family households, whereby women take primary responsibility for the overnight care of children. Programs aimed at reducing the sleep debt experienced by parents, particularly mothers, are needed to reduce sleep inequalities that may compound with inequalities in other life domains.
Background
The importance of sleep for individuals in all life-course stages cannot be underestimated. Sleep affects physical and mental health, work-related productivity, and longevity, among other things (see e.g., Grandner, Hale, Moore, & Patel, 2010; Lamberg, 2004; Leproult and Van Cauter, 2010; Taheri, Lin, Austin, Young, & Mignot, 2004). Hence, the promotion of healthy sleeping habits is a fundamental pillar of public health strategies to improve population wellbeing (Altevogt & Colten, 2006). In Australia, the annual direct and indirect costs of poor sleep amount to over $5 billion (Hillman & Lack, 2013). Yet, we know surprisingly little about the social determinants of sleep in contemporary Australia.
Conventional wisdom, media discourses and emerging scholarly research agree that parenthood is an important factor reducing both the quantity and the quality of sleep. For example, US evidence demonstrates that parents struggle with increased fatigue and daytime sleepiness after the birth of children (Elek, Hudson, & Fleck, 2002; Hagen, Mirer, Palta, & Peppard, 2013; Medina, Lederhos, & Lillis, 2009). Lack of sleep or reduced sleep quality among parents is important for two reasons.
First, investments in children (be it economic resources or time spent with the child) are of critical importance during the first five years of life (Duncan, Yeung, Brooks-Gunn, & Smith, 1998; Heckman & Masterov, 2007). However, this period of time may coincide with the time in which parents are most sleep deprived. Sleep deprivation may restrict parental ability to spend quality time with their offspring and transfer human, social and cultural capital.
Second, parenthood is accompanied by an increasing need for economic resources to cover the costs of having young children, including special food and other items, increased access to health services, a larger or better located dwelling and childcare (Phillips & Taylor, 2013). However, parents who are "sleepy" and "tired", may be less productive workers (Lamberg, 2004) and have a greater tendency to miss work (Rahkonen et al., 2012), and consequently decrease their chances of doing well and advancing in their jobs and careers.
The first aim of this paper is to establish whether and how the number of young children people have and the age of their youngest child are associated with the quantity and quality of their sleep.
Sociologists are also beginning to look at these issues from a gender perspective. Becoming a parent, as well as having additional children, is known to bring about or exacerbate gender inequalities in household arrangements. For example, gender-unequal outcomes favouring men following from the transition to parenthood have been documented in Australia for participation in paid employment, work hours, housework hours, perceptions of housework fairness and exercise time (Baxter, Hewitt, & Haynes, 2008; Evans and Baxter, 2013; Perales, Baxter, & Tai, 2015; Perales, del Pozo-Cruz, & del Pozo-Cruz, 2015). Based on these well-known processes, some scholars have argued that sleep may be another life sphere in which gender inequalities emerge after increases in family size. While, on average, women sleep more than men, once they become mothers (and men fathers) the pattern reverses (Arber, Bote, & Meadows, 2009; Burgard & Ailshire, 2013; Meadows & Arber, 2012). These gender inequalities in sleep, whereby mothers sleep less and worse than fathers, have been referred to as women's "fourth shift" (Venn, Arber, Meadows, & Hislop, 2008), following from a first shift of paid or unpaid daily work, a second shift of evening work, and a third shift that involves thinking about the needs of other family members throughout the first two shifts (Hochschild, 1997).
Such gender disparities in sleep outcomes are important because, given the consequences of unhealthy sleep outlined above, disproportionate sleepiness and tiredness among women with young children might compound or even drive well-known gender inequities in other life domains, for instance work and leisure.
The second aim of this paper is to establish whether and how the experience of parenthood is associated with gender unequal sleep outcomes.
While there is growing Australian research on the predictors of healthy sleeping habits among children and adolescents (see e.g., Cain, Gradisar, & Moseley, 2011; Olds, Maher, Blunden, & Matricciani, 2010; Short et al., 2011), evidence on the influence of parenthood and gender on sleep in Australia is lacking. Recent Australian research on the social determinants of sleep by Soltani et al. (2012), for instance, ignores the role of children. Perales and Plage (2015) find that young children substantially and significantly reduce sleep duration in Australia. Yet the focus of this research was not parenthood, and no consideration was given to the intersections between gender and parenthood. In this paper, this gap in knowledge will be filled by analysing data from the latest wave of the Household, Income and Labour Dynamics in Australia (HILDA) Survey.
Data and methods
Data from the HILDA Survey (Summerfield et al., 2014) is used to examine the intersections between sleep, parenthood and gender. The HILDA Survey is a household panel survey covering the period 2001 to 2013 that is largely representative of the Australian population. Information from all household members aged 15 and over is collected annually through a mix of face-to-face interviews and self-complete questionnaires. We use data from the most recent wave, Wave 13, in which a module on sleep was first introduced. The sample is restricted to individuals of typical child-rearing years, ages 20 to 55, with complete information on the analytical variables of interest.
Two outcome variables capturing different aspects of healthy sleep are examined. First, an indicator of sleep quantity is used. This is a continuous variable capturing respondents' self-reported hours of sleep in a usual week, considering night sleep and naps as well as differences between weekends and week days. Cases in which the values of this variable were implausible are excluded: less than 20 hours or more than 84 hours of sleep per week.
The second outcome is a self-reported measure of sleep quality. This comes from a question reading: "In the past month, how would you rate your sleep overall", with the following possible responses: "very good", "fairly good", "fairly bad" and "very bad". We reverse coded this variable so that high scores indicate better sleep quality (1 = very bad, 2 = fairly bad, 3 = fairly good, 4 = very good). Both outcome variables are treated as continuous variables in regression analyses. Nevertheless, results were very similar when using dichotomous and ordered versions of the outcome variables.
The key explanatory variables capture two dimensions of parenthood. First, a variable is used capturing the number of resident dependent children aged 0-4 (from hereafter referred to as "young children"). The 0-4 age range was chosen as a focus because this captures the ages in which children are most time demanding, and the time before children enter formal school. Second, for those individuals who have young children, a variable is used capturing the age of the youngest child (expressed in years). Categorical versions of the parenthood variables and polynomials of these variables were also considered to capture non-linear relationships with similar results.
Given the cross-sectional nature of the data, we use ordinary least squares (OLS) multivariate regression models to examine the associations between these two explanatory variables and each of the outcome variables. Regression models control for a range of possible confounders of the relationships between parenthood, gender and sleep, including age, relationship status, highest educational qualification, income, employment status, ethnic and migrant background and long-term health conditions. Means and standard deviations for all variables are presented in Table 1.
| Mean | SD | Min. | Max. | |
|---|---|---|---|---|
| Key explanatory variables | ||||
| Number of young children | 0.28 | 0.61 | 0 | 4 |
| Age of the youngest child † | 1.56 | 1.35 | 0 | 4 |
| Control variables | ||||
| Age | 36.93 | 10.61 | 20 | 55 |
| Relationship status | ||||
| Single; never married | 0.24 | 0 | 1 | |
| Single; divorced, separated, widowed | 0.08 | 0 | 1 | |
| Partnered; married or cohabiting | 0.68 | 0 | 1 | |
| Highest educational qualification | ||||
| Degree | 0.29 | 0 | 1 | |
| Professional qualification | 0.34 | 0 | 1 | |
| Year 12 | 0.18 | 0 | 1 | |
| Below year 12 | 0.18 | 0 | 1 | |
| Employment status | ||||
| Employed full-time | 0.51 | 0 | 1 | |
| Employed part-time | 0.14 | 0 | 1 | |
| Self-employed | 0.10 | 0 | 1 | |
| Unemployed | 0.05 | 0 | 1 | |
| Inactive | 0.15 | 0 | 1 | |
| Full-time student | 0.05 | 0 | 1 | |
| Annual household income, in $10,000s | 10.13 | 6.71 | 0 | 171 |
| Ethnic and migrant background | ||||
| Australian born, not Indigenous | 0.76 | 0 | 1 | |
| Australian born, Indigenous | 0.03 | 0 | 1 | |
| Migrant, English-speaking background | 0.08 | 0 | 1 | |
| Migrant, non-English-speaking background | 0.12 | 0 | 1 | |
| Long-term health condition | 0.21 | 0 | 1 |
Notes: Young children defined as children age 0-4 years. † Relates to the subsample of parents of young children.
Source: HILDA Survey, 2013.
Empirical evidence
Raw associations
"Raw" (i.e., unadjusted, bivariate) associations between parenthood, gender and sleep are presented in Table 2. Sleep quantity, measured as the number of weekly sleep hours, decreases visibly with the number of young children: from 50 hours for people without young children to 46.2 hours for people with three young children. Looking at the data with a "gender lens", we can observe that, among individuals with no young children, mean sleep quantity is lower for men (49.5 hours) than women (50.4 hours). This gender gap in weekly sleep hours narrows with the birth of the first child (women = 48.8 hours; men = 48.4 hours), reverses with the birth of the second child (women = 45.8 hours; men = 48.3 hours), and continues to grow with the birth of the third child (women = 44.5 hours; men = 48.2 hours). Concerning the age of the youngest child, the data reveal that sleep quantity is particularly low among parents whose youngest child is age 0 (46 hours) or 1 (48.3 hours). The gender gap in sleep hours is more unbalanced at age 0, when men sleep on average 2.9 hours more than women per week. This gap narrows at age 1 (0.3 hours), and reverses to favour mothers at ages 2, 3 and 4 (-0.3, -0.4 and-1.3 hours, respectively).
| Sleep quantity (weekly hours) | Sleep quality (1-4) | |||||
|---|---|---|---|---|---|---|
| All | Women | Men | All | Women | Men | |
| Number of young children | ||||||
| None | 50.0 | 50.4 | 49.5 | 2.88 | 2.87 | 2.90 |
| One child | 48.6 | 48.8 | 48.4 | 2.79 | 2.73 | 2.86 |
| Two children | 47.0 | 45.8 | 48.3 | 2.68 | 2.60 | 2.76 |
| Three children | 46.2 | 44.5 | 48.2 | 2.69 | 2.64 | 2.75 |
| Age of the youngest child | ||||||
| 0 years | 46.0 | 44.6 | 47.5 | 2.65 | 2.51 | 2.80 |
| 1 year | 48.3 | 48.2 | 48.5 | 2.80 | 2.76 | 2.85 |
| 2 years | 49.0 | 49.2 | 48.9 | 2.75 | 2.71 | 2.81 |
| 3 years | 49.5 | 49.6 | 49.2 | 2.83 | 2.76 | 2.92 |
| 4 years | 49.2 | 49.7 | 48.4 | 2.82 | 2.83 | 2.80 |
Note: Young children defined as children age 0-4 years.
Source: HILDA Survey, 2013.
Altogether, the presence of young children in the household is associated with reduced sleep, and more so for women than men. Having babies of less than 1 year of age reduces parental sleep (especially maternal sleep) the most.
Similar patterns emerge for self-reported sleep quality. This is highest among individuals who have no young children (2.88 units), and decreases with the first (2.79 units), second (2.68 units) and third (2.69 units) child. The gender gap in sleep quality always favours men, but is wider among parents of one, two and three young children (0.13, 0.16 and 0.11 units, respectively) than among individuals with no young children (0.03 units). Parents whose youngest child is less than one year of age report the lowest sleep quality (2.65 units), with scores concentrated in the 2.75 to 2.83 range when the youngest child is age 1-4. The gender gap in sleep quality favouring men is most pronounced when the youngest child is age 0 (0.29 units).
Altogether, sleep quality is lowest and the gender gap in sleep quality is highest when there are young children in the household, particularly when they are babies.
Multivariate regression models
More robust multivariate regression models that control for factors that may confound the relationships between parenthood, gender and sleep are presented in Table 3. Since we are interested in the intersections between gender and parenthood, the models include interaction terms between these sets of variables. These test the moderating effect of gender in the relationship between parenthood and sleep (and vice versa).
| Complete sample | Parents of young children | |||
|---|---|---|---|---|
| Sleep hours (i) | Sleep quality (ii) | Sleep hours (iii) | Sleep quality (iv) | |
| Female | 0.89*** | -0.01 | -3.04*** | -0.23*** |
| Number of young children | -1.07*** | -0.08*** | -0.66 | -0.05 |
| Female * Number of young children | -1.80*** | -0.06* | ||
| Age of the youngest child | 0.56** | 0.01 | ||
| Female * Age of the youngest child | 1.05*** | 0.06** | ||
| Age | -0.10*** | -0.00 | -0.19*** | -0.00 |
| Relationship status | ||||
| Single; never married (reference category) | ||||
| Single; divorced, separated, widowed | -1.47*** | -0.11** | -1.28 | -0.09 |
| Partnered; married or cohabiting | 0.44 | 0.01 | 3.97*** | 0.10 |
| Highest educational qualification | ||||
| Degree (reference category) | ||||
| Professional qualification | -1.02*** | -0.07*** | -1.24** | -0.06 |
| Year 12 | -0.74** | -0.06* | -0.85 | -0.08 |
| Below year 12 | -1.63*** | -0.11*** | -0.94 | -0.16** |
| Employment status | ||||
| Employed full-time (reference category) | ||||
| Employed part-time | 1.15*** | -0.01 | 0.96 | -0.02 |
| Self-employed | 1.32** | -0.15*** | 0.30 | -0.08 |
| Unemployed | 0.95*** | 0.06* | 0.78 | -0.02 |
| Inactive | 1.09** | -0.12*** | 1.40* | -0.02 |
| Full-time student | 1.56*** | 0.01 | 1.52 | 0.08 |
| Annual household income, in $10,000s | 0.01 | -0.00 | 0.03 | -0.01* |
| Ethnic and migrant background | ||||
| Australian born, not Indigenous (reference category) | ||||
| Australian born, Indigenous | -0.17 | -0.08 | 0.21 | 0.03 |
| Migrant, English-speaking background | -0.03 | 0.04 | 0.15 | 0.16* |
| Migrant, non-English-speaking background | -0.41 | 0.12*** | 1.26* | 0.20*** |
| Long-term health condition | -1.23*** | -0.31*** | -1.63** | -0.28*** |
| N | 10,706 | 9,211 | 2,216 | 1,876 |
| R2 | 0.05 | 0.06 | 0.07 | 0.06 |
Notes: Young children defined as children age 0-4 years. Standard errors adjusted for household clustering. Statistical significance: * p < 0.05, ** p < 0.01, *** p < 0.001.
Source: HILDA Survey, 2013.
Models (i) and (ii) are estimated on the complete sample of parents and non-parents and capture the associations between gender and the number of children aged 0-4 with sleep quantity and sleep quality, respectively. Since the gender and parenthood variables are interacted, they are substantially easier to interpret by inspection of the left-hand side of Figure 1. The top left graph shows that, all else being equal, the number of young children in the household is associated with reduced weekly sleep hours among both men (continuous line) and women (dashed line). The gradient is nevertheless more marked among women than men. Women with no young children sleep more per week than men with no young children, while women with young children sleep less than men with young children. The differences are generally statistically significant, as denoted by non-overlapping confidence intervals at the 95% level and a significant interaction effect in Table 3.
Figure 1: Interactions between parenthood, gender and sleep
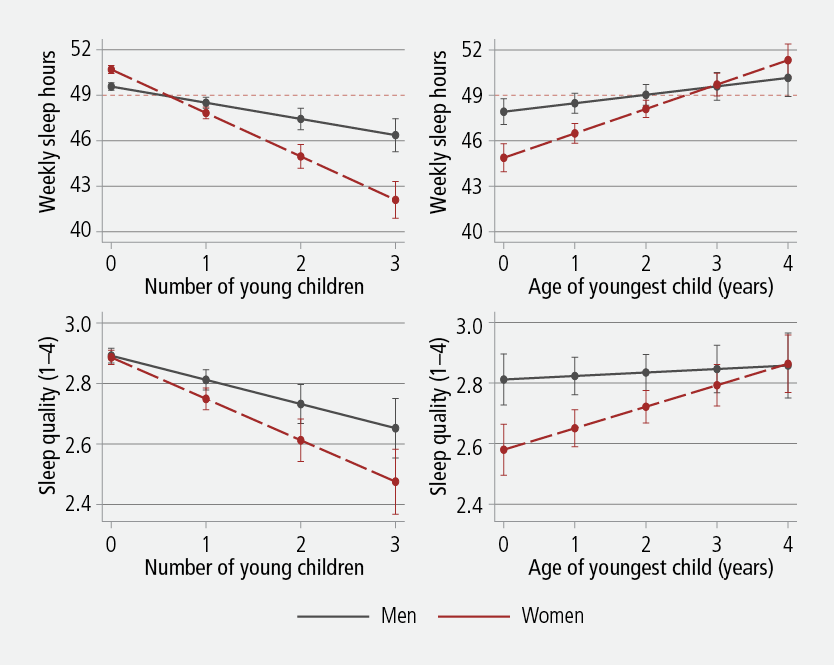
Notes: Based on the results of multivariate regression models presented in Table 3. Young children defined as children age 0-4 years. Models control for age, relationship status, highest educational qualification, income, employment status, ethnic and migrant background and the presence of long-term health conditions. Vertical bars denote 95% confidence intervals. Horizontal dashed lines represent the minimum weekly sleep time recommended by the US National Sleep Foundation (Hirshkowitz et al., 2015).
The bottom left graph portrays a similar relationship for sleep quality, which decreases with the number of young children for both men and women, all else being equal. However, the gender differences in sleep quality by the number of young children are small and generally not statistically significant at the 95% level (though the interaction effect in Table 3 is statistically significant).
Models (iii) and (iv) are estimated on the subsample of individuals who are parents of young children aged 0-4 and capture the associations between gender and the age of the youngest child with sleep quantity and sleep quality, respectively. These are again easier to interpret by visual means, looking at the right-hand side of Figure 1. The top right graph shows that predicted sleep quantity increases markedly and statistically significantly with the age of the youngest child, particularly among women. The gender gap in sleep quantity favours fathers and is statistically significant at the 95% level when the youngest child in the household is 1 year of age or younger, and fades as the youngest child grows older.
The bottom right graph shows analogous relationships for sleep quality. Mothers' sleep quality increases with the age of the youngest child, while the line representing fathers' sleep quality is almost flat. As a result, mothers experience significantly lower sleep quality than fathers up to when their youngest child is age 4, when they finally "catch up".
Altogether, these results confirm the patterns observed in bivariate analyses and demonstrate statistically significant and often large gaps in sleep quantity and quality between parents of young children and individuals without young children, parents of very young and young children, and mothers and fathers.
While not of key importance in this research, the model coefficients on the control variables offer interesting insights into the social determinants of sleep quantity and quality in contemporary Australia. In model (i) for the complete sample, sleep quantity is higher among individuals who are younger; are single (never married) rather than divorced, separated or widowed; have degree-level qualifications; are in any employment category other than employed full-time; and have no long-standing health impairments. Neither income nor ethnic/migrant status significantly predicted sleep quantity. The associations between the covariates and sleep quality in model (ii) are similar, with the exceptions that age and certain employment characteristics no longer feature statistically significant coefficients. Additionally, migrants from non-English speaking backgrounds report significantly better sleep quality than Australian-born, non-Indigenous individuals.
In the models for the subsample of parents of young children, the coefficients on the relationship status variables in model (iii) are particularly interesting. Single (never married) parents of young children in our sample, of which 92% are women, sleep an average of four hours per week less than partnered parents of young children, all else being equal. Parents who are single after a divorce, separation or widowhood sleep even less. This suggests that, for single parents, sleep disadvantage compounds with disadvantage in other life domains.
Discussion and conclusion
In this paper we have examined the associations between different dimensions of parenthood, gender and sleep quantity and quality using nationally representative Australian survey data. Key findings indicate that both sleep quantity and sleep quality are greater among (i) individuals without pre-school age children than parents of pre-school age children, (ii) parents of young children (ages 2 to 4) than parents of very young children (ages 0 and 1), and (iii) fathers of pre-school age children than mothers of pre-school age children. These results are consistent with those of previous studies from the USA (Elek et al., 2002; Hagen et al., 2013; Medina et al., 2009), and add to gender theory by providing first-time evidence of gender-unequal sleep arrangements in Australian households. These results are consistent with the notion that parenthood brings about a "fourth shift" into Australian women's lives (Venn et al., 2008), whereby women take primary responsibility for the overnight care of children.
What mechanisms might be driving the observed associations? Both parents and non-parents may experience sleep loss associated with worry (e.g., financial stress), but this may be more acute among parents because they have the financial responsibility to ensure that their children's basic needs are met. While we control for household income in the models, other aspects of wealth such as debt, assets or financial commitments are not included in this measure. Parents of young children may also sleep less due to the tendency of young children to wake up in the early morning, or may willingly use their sleep time to undertake paid work, domestic work or leisure activities once their children are in bed. Some parents may co-sleep with their young children, which might disrupt their sleep or reduce comfort due to diminished bed space. Most importantly, parents are likely to experience worsened or reduced sleep because of their responsibility to tend to children's overnight needs, such as changing their nappies, breast- or bottle feeding, accompanying them to the toilet, dealing with night terrors or fetching food and water. Some of these needs will be heightened when children feel unwell or fall sick, including natural developmental stages such as teething.
The reasons why women may be more willing or able to undertake these night activities, and the ways in which the tasks are negotiated within the family, are less clear. From the economic perspective of household specialisation, women may have a comparative advantage in performing these tasks (Becker, 1985, 1991). For example, women can better fulfil the biological imperative of breastfeeding, and it has been argued that young children may display a preference for being in close proximity to their mothers when it comes to night activities. An alternative sociological perspective is that men and women "do gender" overnight (West and Zimmerman, 1987); that is, fathers and mothers reaffirm their gendered identities by engaging or not engaging in the overnight care of children (Venn et al., 2008). This is because, under a traditional gender division of labour, dealing with children (and caring for others more generally) is typically considered a "female" task. Further research that untangles these processes is warranted.
The US National Sleep Foundation recommends that adults sleep no less than seven hours a day; that is, 49 hours per week (Hirshkowitz et al., 2015). This threshold is denoted by a dashed horizontal line in the graphs pertaining to sleep quantity in Figure 1. On average, mothers and fathers of young children in Australia fall short of this figure. The situation is particularly alarming for mothers and fathers of two or three young children, who incur a weekly sleep debt of two to seven hours. Fathers and mothers of young children in Australia only begin to meet the National Sleep Foundation sleep quantity recommendations after their youngest child turns 2 and 3 years old, respectively.
Given the well-established association between unhealthy sleep and ill health, these results indicate that policy planners should devise interventions that increase the agency of parents of young children to increase and improve their sleep. What could such interventions look like?
Government initiatives such as the provision of a generous and flexible paid parental leave scheme might help, since parents would not be as pressured to perform at work while they are at the peak of their "sleepiness". To prevent potentially harmful career breaks among parents of young children, such schemes may involve flexi-time and reduced work hours instead of long spells of time away from the workplace. It is important that any such policy extends to fathers as well as mothers, both because they suffer from sleep debt themselves and because their presence in the home could help mothers find the time to sleep.
Since sleep affects productivity, employers also have good reasons to combat sleep deprivation among working parents. Providing parents with flexi-time, enabling parents to work from home, and maintaining a strong commitment to equal opportunity policies that consider parenthood (not just motherhood) are potential strategies for employers to reduce parental sleep debt. More creative options include the provision of sleep pods at workplaces to enable short, restorative naps, and the establishment of a system of payments or tax deductions to relatives who help care for young children so that parents can allocate more time to sleep (Brady & Perales, 2014).
However, if gender gaps in sleep among parents of young children are a product of men and women's gender beliefs, then gender differences in sleep debt among parents would remain even if the above interventions are put to practice. Information campaigns about the benefits of sleep and the need for fathers to support mothers' sleep would help in this regard.
While important and innovative, our findings must nevertheless be interpreted with some caution, given some data-driven limitations of the research design. First and foremost, our data are cross-sectional and so we are unable to track the same individuals over time, before and after their children are born and as their youngest child ages. As a result, the reported relationships remain associational rather than causal.
Second, our measures of sleep are self-reported, which may lead to measurement error. Sleep quantity may be recorded differently by parents and non-parents. Parents of babies and young children, in particular, may have difficulty quantifying the time that they spend awake in the middle of the night caring for their children. As sleep quality is a subjective measure, it is possible that some people have greater aspirations and expectations than others (Tomaszewski & Perales, 2014). Parents, for example, may have different standards or reference points when evaluating what constitutes "a good night's sleep". Mothers and fathers who experienced significant difficulties with sleep in the first years of their child's life might rate suboptimal sleep more positively than individuals who were never exposed to troubled sleep.
Third, sample sizes for some subgroups of parents of young children may be small, and so some of our predicted effects are relatively imprecise. Further collection of sleep-related information within the HILDA Survey (or other panel studies) will aid in overcoming some of these methodological limitations by increasing subsample sizes and enabling more robust and precise longitudinal analyses.
Nevertheless, our findings are important and provide first-time evidence that the sleep quantity and quality of parents of young children, particularly mothers, are a cause for concern in contemporary Australia. New studies examining the specific mechanisms that link parenthood and gender to unhealthy sleep in Australia are necessary to inform efficient and effective evidence-based policy responses.
References
- Altevogt, B. M., & Colten, H. R. (Eds.). (2006). Sleep disorders and sleep deprivation: An unmet public health problem. Institute of Medicine (US) Committee on Sleep Medicine and Research. Washington, D.C.: National Academies Press.
- Arber, S., Bote, M., & Meadows, R. (2009). Gender and socio-economic patterning of self-reported sleep problems in Britain. Social Science & Medicine, 68(2), 281-289. doi: 10.1016/j.socscimed.2008.10.016.
- Baxter, J., Hewitt, B., & Haynes, M. A. (2008). Life course transitions and housework: Marriage, parenthood and time on housework. Journal of Marriage and Family, 70(2), 259-272.
- Becker, G .S. (1985). Human capital, effort and the sexual division of labour. Journal of Labor Economics, 3, S33-58.
- Becker, G. S. (1991). A treatise on the family. Cambridge, MA: Harvard University Press.
- Brady, M. & Perales, F. (2014). Hours of paid work among single and partnered mothers in Australia: The role of childcare packages. Journal of Family Issues, 1-23. doi: 10.1177/0192513x14531416.
- Burgard, S. A., & Ailshire, J. A. (2013). Gender and time for sleep among US adults. American Sociological Review, 78(1), 51-69. doi: 10.1177/0003122412472048.
- Cain, N., Gradisar, M., & Moseley, L. (2011). A motivational school-based intervention for adolescent sleep problems. Sleep Medicine, 12(3), 246-251.
- Duncan, G. J., Yeung, W. J., Brooks-Gunn, J., & Smith, J. R. (1998). How much does childhood poverty affect the life chances of children? American Sociological Review, 63(3), 406-423.
- Elek, S. M., Hudson, D. B., & Fleck, M. O. (2002). Couples' experiences with fatigue during the transition to parenthood. Journal of Family Nursing, 8(3), 221-240. doi: 10.1177/107484070200800305.
- Evans, A., & Baxter, J. (2013). Negotiating the life course: Stability and change in life pathways. Dordrecht, The Netherlands: Springer.
- Grandner, M. A., Hale, L., Moore, M., & Patel, N. P. (2010). Mortality associated with short sleep duration: The evidence, the possible mechanisms, and the future. Sleep Medicine Reviews, 14(3), 191-203. doi: 10.1016/j.smrv.2009.07.006.
- Hagen, E. W., Mirer, A. G., Palta, M., & Peppard, P. E. (2013). The sleep-time cost of parenting: Sleep duration and sleepiness among employed parents in the Wisconsin Sleep Cohort Study. American Journal of Epidemiology, 177(5), 394-401. doi: 10.1093/aje/kws246.
- Heckman, J. J., & Masterov, D. V. (2007). The productivity argument for investing in young children. Applied Economic Perspectives and Policy, 29(3), 446-493. doi: 10.1111/j.1467-9353.2007.00359.x
- Hillman, D. R., & Lack, L. C. (2013). Public health implications of sleep loss: the community burden. Medical Journal of Australia, 199(8), S7-10.
- Hirshkowitz, M., Whiton, K., Albert, S. M., Alessi, C., Bruni, O., DonCarlos, L., et al., (2015) National Sleep Foundation's sleep time duration recommendations: Methodology and results summary. Sleep Health, 1(1), 40-43. doi: 10.1016/j.sleh.2014.12.010.
- Hochschild, A. (1997). The time bind. When work becomes home and home becomes work. New York: Owl Books.
- Lamberg, L. (2004). Promoting adequate sleep finds a place on the public health agenda. Journal of the American Medical Association, 291(20), 2415-2417. doi: 10.1001/jama.291.20.2415.
- Leproult, R., & Van Cauter, E. (2010). Role of sleep and sleep loss in hormonal release and metabolism. Endocrine Development, 17, 11-21. doi: 10.1159/000262524.
- Meadows, R., & Arber, S. (2012). Understanding sleep among couples: Gender and the social patterning of sleep maintenance among younger and older couples. Longitudinal and Life Course Studies, 3(1), 66-79.
- Medina, A. M., Lederhos, C. L., & Lillis, T. A. (2009). Sleep disruption and decline in marital satisfaction across the transition to parenthood. Families, Systems, & Health, 27(2), 153-160. doi: 10.1037/a0015762.
- Olds, T., Maher, C., Blunden, S., & Matricciani, L. (2010). Normative data on the sleep habits of Australian children and adolescents. Sleep, 33(10), 1381-1388.
- Perales, F. and Plage, S. (2015). Losing ground, losing sleep: Economic vulnerability, local economic conditions and sleep quantity. LCC Working Papers 2015-06. Institute for Social Science Research: The University of Queensland.
- Perales, F., Baxter, J., & Tai, T. O. (2015). Gender, justice and work: A distributive approach to perceptions of housework fairness. Social Science Research, 51, 51-63.
- Perales, F., del Pozo-Cruz, J., & del Pozo-Cruz, B. (2015). Long-term dynamics in physical activity behaviour across the transition to parenthood. International Journal of Public Health, 60(3), 301-308. doi: 10.1007/s00038-015-0653-3.
- Phillips, B., Li, J., & Taylor, M. (2013). Cost of kids: The cost of raising children in Australia. NATSEM Income and Wealth Report, Issue 33, May 2013, Sydney, AMP.
- Rahkonen, O., Lallukka, T., Kronholm, E., Vahtera, J., Lahelma, E., & Laaksonen, M. (2012). Sleep problems and sickness absence among middle-aged employees. Scandinavian Journal of Work, Environment & Health, 38(1), 47-55. doi: 10.5271/sjweh.3186.
- Short, M. A., Gradisar, M., Wright, H., Lack, L. C., Dohnt, H., & Carskadon, M. A. (2011). Time for bed: parent-set bedtimes associated with improved sleep and daytime functioning in adolescents. Sleep, 34(6), 797-800.
- Soltani, M., Haytabakhsh, M., Najman, J., Williams, G., O'Callaghan, M., Bor, W., et al. (2012). Sleepless nights: The effect of socioeconomic status, physical activity, and lifestyle factors on sleep quality in a large cohort of Australian women. Archives of Women's Mental Health, 15(4), 237-247. doi: 10.1007/s00737-012-0281-3.
- Summerfield, M., Freidin, S., Hahn, M., Li, N., Macalalad, N., Mundy, L., et al. (2014). HILDA user manual: Release 13. Melbourne: Melbourne Institute of Applied Economic and Social Research, University of Melbourne.
- Taheri, S., Lin, L., Austin, D., Young, T., & Mignot, E. (2004). Short sleep duration is associated with reduced Leptin, elevated Ghrelin, and increased Body Mass Index. PLoS Medicines, 1(3), e62. doi: 10.1371/journal.pmed.0010062.
- Tomaszewski, W., & Perales, F. (2014) Who settles for less? Subjective dispositions, objective circumstances, and housing satisfaction. Social Indicators Research, 118(1), 181-203. doi: 10.1007/s11205-013-0420-x.
- Venn, S., Arber, S., Meadows, R., & Hislop, J. (2008). The fourth shift: Exploring the gendered nature of sleep disruption among couples with children. The British Journal of Sociology, 59(1), 79-97. doi: 10.1111/j.1468-4446.2007.00183.x.
- West, C., & Zimmerman, D. H. (1987). Doing gender. Gender & Society, 1(2), 125-151. doi: 10.1177/0891243287001002002.
Stefanie Plage is from the School of Social Science, The University of Queensland, Francisco Perales and Janeen Baxter are from the ARC Centre of Excellence for Children and Families over the Life Course, Institute for Social Science Research, The University of Queensland.
Acknowledgements: This research was supported by the Australian Research Council Centre of Excellence for Children and Families over the Life Course (project number CE140100027). The views expressed herein are those of the authors and are not necessarily those of the Australian Research Council. This paper uses unit record data from the HILDA survey. The HILDA Project was initiated and is funded by the Australian Government Department of Social Services (DSS) and is managed by the Melbourne Institute of Applied Economic and Social Research (Melbourne Institute). The findings and views reported in this paper, however, are those of the authors and should not be attributed to either DSS or the Melbourne Institute. The authors would like to thank Sofia, Oliver and Marc Perales Plage for valuable insights on practical aspects of the research.