Elder abuse: Understanding issues, frameworks and responses
You are in an archived section of the AIFS website
Overview
This report provides an overview of elder abuse in Australia - including its characteristics, context, and prevention. First, it considers definitional issues and what is known about prevalence and incidence, risk and protective factors, and the dynamics surrounding disclosure and reporting. The report then sets out evidence on the demographic and socio-economic features of the Australian community that are relevant to understanding social dynamics that may influence elder abuse, including intergenerational wealth transfer and the systemic structures that intersect with elder abuse. Lastly, the report considers legislative and service responses and Australian and overseas approaches to prevention.
Key messages
-
Evidence about prevalence in Australia is lacking, though if international indications provide any guidance, it is likely that between 2% and 14% of older Australians experience elder abuse in any given year, with the prevalence of neglect possibly higher.
-
The available evidence suggests that most elder abuse is intra-familial and intergenerational, with mothers most often being the subject of abuse by sons, although abuse by daughters is also common, and fathers are victims too.
-
Financial abuse appears to be the most common form of abuse experienced by elderly people, and this is the area where most empirical research is available. Psychological abuse appears slightly less common than financial abuse, and seems to frequently co-occur with financial abuse.
-
The problem of elder abuse is of increasing concern as in the coming decades unprecedented proportions of Australia’s populations will be older: in 2050, just over a fifth of the population is projected to be over 65 and those aged 85 and over are projected to represent about 5% of the population.
-
Our federal system of government means that responses to elder abuse are complicated as they are contained within multiple layers of legislative and policy frameworks across health, ageing and law at Commonwealth and state level.
1. Introduction
This report provides a broad analysis of the issues raised by elder abuse in the Australian context. Elder abuse - which involves the physical, emotional, sexual or financial abuse or neglect of an older person by another person in a position of trust - presents a range of complex challenges for the Australian community. Although solid evidence about prevalence in Australia is lacking, the incidence of elder abuse will certainly increase as Australia's "baby boomer" generation reaches old age, with increased life expectancy meaning that the aged will, in coming years, comprise a greater proportion of the population than ever before. Fundamentally a human rights issue, responses to the management and prevention of elder abuse sit within a range of complex policy and practice structures across different levels of government, and various justice system frameworks within the private sector and across non-government organisations.
In this respect, the management of elder abuse has similar features to family and domestic violence, sexual assault and child protection. Recognition of the need for a national approach to family and domestic violence (and specifically violence against women and their children) and to child protection has seen the development in the past ten years of family and domestic violence national plans and child protection frameworks, all auspiced by the Council of Australian Governments. The structures and frameworks in the areas of ageing generally and elder abuse particularly have parallels with those that shape responses to family and domestic violence and child protection, but the range of frameworks is greater and more complex. From a policy perspective, Commonwealth, state and territory governments have intersecting responsibilities in relation to ageing, aged care and health. Local governments also have responsibility for the delivery of services to the aged. Many of the legal issues potentially raised by elder abuse - such as criminal justice responses and the legislative and organisational infrastructure that deals with matters including substituted decision making and wills and estates - are the preserve of the states and territories. A range of professions, disciplines and organisations interact with elders and their family members. Professionals from health, law, social work and the banking and financial industry potentially engage with elder abuse in their day-to-day practice, and a range of public, private and non-government organisations provide aged care services in private and public settings.
Against this complex structure and organisational background, this report provides an overview of the issues raised by elder abuse in Australia. It also draws on international material where relevant. The report first considers definitional issues in relation to elder abuse and what is known about prevalence and incidence, risk and protective factors and the dynamics surrounding disclosure and reporting. It then sets out some evidence on the demographic and socio-economic features of the Australian community that are relevant to understanding social dynamics that may influence elder abuse. Section 6 outlines some of the features of the systemic structures that intersect with elder abuse and section 7 considers prevention. Section 8 discusses international approaches.
2. What is elder abuse?
Varied conceptualisations of elder abuse are evident in different frameworks and disciplines (United Nations Department of Economic and Social Affairs [UNDESA], 2013). One of the dominant disciplines in the field has been social gerontology, which is concerned with the study of ageing. Human rights and public health perspectives are also evident, and intersecting fields of thinking and concern include those related to family violence, violence against women, and disability. An approach informed by an older adult protection philosophy arising from the discipline of geriatrics in medicine has influenced some approaches in the United States, including the establishment of adult protective services (UNDESA, 2013; also see section 8.2). In Australia, approaches of organisations concerned with elder issues, such as COTA Australia (the peak national organisation representing the rights, needs and interests of older Australians), tend to be informed by human rights conceptualisations that emphasis self-determination, autonomy and respect (Department of Health, Victoria, 2012).
The way in which elder abuse issues and responses are approached depends on the perspective adopted. The WHO takes a public health perspective, adopting a 1995 definition developed by Action of Elder Abuse UK to describe elder abuse as "a single or repeated act or lack of appropriate action, occurring within any relationship where there is an expectation of trust which causes harm or distress to an older person" (WHO, 2008, p. 6). This is the definition adopted in some Commonwealth frameworks in Australia (e.g., MyAgedCare). A working definition put forward by the US Centers for Disease Control and Prevention (CDC; 2015), again from a public health perspective, is more specific: "an intentional act or failure to act by a caregiver or another person in a relationship involving an expectation of trust that causes or creates a risk of harm to an older adult" (defined as someone age 60 or older). It also provides working definitions of specific types of abuse (see Appendix).
A commonly applied definition locally is that adopted by the Australian Network for the Prevention of Elder Abuse in 1999 (also based on the Action of Elder Abuse UK definition), which specifies that elder abuse is:
any act occurring within a relationship where there is an implication of trust, which results in harm to an older person. Abuse may be physical, sexual, financial, psychological, social and/or neglect.1
Although these definitions have similar elements, the absence of a precise agreed definition is considered problematic for a range of reasons, not the least of which is the difficulty in measuring elder abuse. One important area where this is evident is in relation to the age at which one might be considered an elder. For the purpose of the WHO and CDC definitions, 60 is the defining age. In Australia, however, for statistical and range of other purposes, including access to the pension (Australian Bureau of Statistics [ABS], 2012b), 65 is the starting point for status as an "elder", and 70 is the age for access to aged care services (Cotterell, Leonardi, Coward, Thomson, & Walters, 2015). The definition of "older" Australian used in this paper is consistent with that used by the ABS, which classifies people over 65 as "older". It should be noted, however, that some definitions, studies and services concerned with elder abuse use the age of 60 as a starting point. The literature on ageing also distinguishes between "old" people (65-84 years) and "old old" people, aged 85 and above (e.g., Wainer, Owada, Lowndes, & Darzins, 2011). The discussion in section 3 establishes that this is a useful distinction to make from a statistical viewpoint as there are significant differences in some areas between these age groups. For Aboriginal and Torres Strait Islander peoples, who have a substantially lower life expectancy than non-Indigenous peoples, a lower age for those who are "older" is considered appropriate (e.g., 45-50 years; Cotterell et al., 2015).
At a more complex level, as a "multi-faceted construct involving intentional and unintentional actions of both a passive and an active nature" (Clare, Blundell, & Clare, 2011, p. 44), consideration of the definition of elder abuse raises the fundamental question of what purpose the definition serves. A recent critique by a Western Australian research team (Clare et al., 2011) has raised several other concerns, arguing that, in addition to the age question, the term "elder abuse" needs to be fundamentally reconsidered. In addition to the operational complications arising from the application of different definitions in different legal, policy and practice frameworks in the Western Australian context, Clare and colleagues called for a debate on whether age should be the defining aspect of elder abuse, or whether it should be conceptualised on the basis of "an assessment of capacity for self-care and self-protection" (p. 40).
This analysis highlights an important issue in considering definitions, given that many of the behaviours captured by the definition may be experienced at any stage of the life course and are covered by various criminal and civil law frameworks. From a conceptual standpoint, this raises the question of whether harmful behaviours involving older people are distinguishable from harmful behaviours involving other adults because they involve older people or because they involve the exploitation of vulnerability. A further significant question that arises in this context is how, in such an analysis, issues such as the dynamics of dependence (section 3) should be dealt with.
Considering the phenomenon of elder abuse more broadly, theoretical models and approaches attribute its occurrence to a complex array of factors, including social and cultural attitudes to the aged. The international literature draws common links between the causes of and conditions for the occurrence of different kinds of abuse and maltreatment, including family violence, child abuse and neglect, and elder abuse (Wilkins, Tsao, Hertz, Davis, & Klevens, 2014; WHO, 2002b). Originally developed to support the conceptualisation of family violence prevention approaches, the socio-ecological model is also considered to be an apt approach in relation to elder abuse (WHO, 2002b). This model posits that interpersonal violence occurs as a result of interactions between factors at four levels of influence: individual, relationship, community and societal. In relation to violence against women across these four levels, attitudes inconsistent with the equality of women are associated with higher levels of family violence. An analogous approach is evident in relation to elder abuse, in which age discrimination and a lack of respect for elders are are societal factors associated with its occurrence (Gil et al., 2015; Hayslip, Reinberg, & Williams, 2015; Mann, Horsley, Barrett, & Tinney, 2014; WHO, 2002b). The authors of a recent prevalence study in Portugal noted that the findings of the study demonstrate that "prevalence rates vary by type of abuse, the victims socio-demographic characteristics, the victims' relationship with the perpetrator … The social responses toward victim protection and collective representations of this social problem, such as the belief systems, cultural norms, and social attitudes towards violence (e.g., higher or lower tolerance toward it) are structural dimensions that indirectly influence it" (Gil et al., 2015, p. 190).
Although different types of interpersonal violence are considered to have common elements in this theoretical model, a range of different theoretical and practice paradigms are applied in relation to each kind of violence. Responses to family violence, for example, have developed out of a feminist framework, and some Australian and American analyses have highlighted theoretical and practical tensions in responses to family violence involving women when feminist and gerontological approaches intersect internationally and locally (Bagshaw, Wendt, Zannettino, & Adams, 2013; Cramer & Brady, 2013). Similarly, analogies between child abuse and elder abuse are seen as problematic in some respects, as "making comparisons between elder abuse and child abuse, and drawing on responses used in child protection, is ageist and generally not appropriate" (Australian Association of Gerontology, 2015, p. 4). However, the structural and systemic issues raised by elder abuse, as highlighted in this and other reports, mean that recent experience in developing national approaches to child protection (the National Framework for Protecting Australia's Children) and family violence (the National Plan for the Reduction of Violence Against Women and Their Children) provide insight into the development of national approaches in relation to complex issues involving multiple levels of governments and a spread of different agencies.
Progress towards understanding elder abuse and developing effective response and prevention measures, are recognised to be considerably less well developed than in other areas of interpersonal violence, including family violence and child abuse (WHO, 2014). The following section outlines what is known about prevalence and risk factors internationally and locally.
1 See the Definition of Elder Abuse at: <www.arasagedrights.com/definition-of-elder-abuse.html>.
3. What is known about the prevalence and dynamics of elder abuse?
This section considers evidence on the prevalence and incidence of elder abuse generally and of the different types of elder abuse that occur. The discussion establishes that there is very limited evidence in Australia that would support an understanding of the prevalence of elder abuse, and there is emerging recognition of the need for systematic research in this area (e.g., Elder Abuse Prevention Unit [EAPU], n. d.). There is some limited evidence on the incidence of elder abuse, mainly based on data derived from calls to state-based elder abuse helplines. There is also some international research on prevalence in different countries - the United States, the United Kingdom and Portugal, for example - but these studies have used different definitions and methodologies.
The discussion in this section first sets out the international evidence on prevalence and then considers what is known about the phenomenon in Australia.
The available evidence suggests that prevalence varies across abuse types, with psychological and financial abuse being the most common types of abuse reported, although one study suggests that neglect could be as high as 20% among women in the older age group (Australian Longitudinal Study on Women's Health [ALSWH], 2014). Older women are significantly more likely to be victims than older men, and most abuse is intergenerational (i.e., involving abuse of parents by adult children), with sons being perpetrators to a greater extent than daughters. For some women, the experience in older age of family violence, including sexual assault, represents the continuation of a lifelong pattern of spousal abuse (Cramer & Brady, 2013; Mann et al., 2014; UNDESA, 2013). Evidence on elder abuse occurring outside of a familial context (e.g., in care settings) is particularly sparse.
At the international level, the WHO (2015) recently reported that estimated prevalence rates of elder abuse in high- or middle-income countries ranged from 2% to 14%, with the following prevalence rates for the most common types of elder abuse:
- physical abuse (0-5%);
- sexual abuse (0-1%);
- psychological abuse, above a threshold for frequency or severity (1-6%);
- financial abuse (1-9%)
- neglect (0-6%).
These prevalence estimates are based on data sources involving elderly people living in private and community settings and do not include those in institutional care or those with a cognitive impairment. These two latter limitations are characteristic of most prevalence studies, which therefore only reflect a partial view of the extent of elder abuse.
3.1 Prevalence studies
International
A US study based on 5,777 respondents (aged 60 and over), contacted through random-digit dialling in 2008, found that one in ten respondents had experienced elder abuse in the past year (Acierno, Hernandez, & Kilpatrick, 2010). The most common types of abuse were: financial abuse by a family member (5%), potential neglect (5%), and emotional abuse (5%). Physical abuse (2%) and sexual abuse (1%) were substantially less common.
A very different approach was taken in assessing prevalence in the UK Study of Abuse and Neglect of Older People (O'Keeffe et al., 2007). This study was based on face-to-face interviews with 2,111 people aged over 66 living in private settings across the UK in 2006. The study measured whether the participants had experienced mistreatment in the preceding 12 months at the hands of a family member, friend or care worker. Overall, 4% of the sample reported mistreatment in the defined period, comprising 4% of women and 1% of men. In this study, neglect (1%) and financial abuse (0.7%) were the most common forms of abuse, followed by psychological and physical abuse (each 0.4%). Sexual abuse was reported uncommonly (0.2% of women). The dominant relationship dynamic associated with abuse in this study was spousal, with 51% of perpetrators reported to be a spouse or partner, and married people more likely to report being abused compared to widows (9% cf. 1%). The other big perpetrator group was "another family member" (49%). Other reported perpetrators were care workers (13%) and close friends (5%).
A prevalence study from Portugal, based on a sample of 1,123 people aged over 60 living in private households, found that 12% had experienced elder abuse in the preceding twelve months (Gil et al., 2015). The relative distribution of the types of abuse were broadly consistent with the US findings, with financial and psychological abuse most common (6% each). Neglect was less common in the Portuguese sample (0.4%), though this may reflect the application of different definitions in the studies. Physical abuse was reported by 2% of participants, and sexual abuse by 0.2%. In this study, the largest group of defined perpetrators was ex-spouses or partners (14%), followed by sons and step-sons (13%), and daughters and step-daughters (6%). "Other relatives" accounted for incidents of abuse in 42% of cases, friends and neighbours in 16%, and paid professionals in 4%. One in five respondents refused to identify the perpetrators.
Australia
In Australia, there are two population-based studies that have yielded some insights into the extent to which older women experience violence, but there are limitations in the measures used and the extent to which they assess concepts relevant to elder abuse. One is a recently published, detailed analysis of data from the Personal Safety Survey (ABS, 2012a) by Australia's National Research Organisation for Women's Safety (ANROWS) (Cox, 2015). The age range for "older women" in that study was 55 plus, and the analysis was framed to assess violence against women, focusing on sexual assault by any perpetrator, and partner violence involving physical assault, physical threat, sexual assault and sexual threat by a cohabiting or intimate partner. In relation to cohabiting partner violence, 0.4% of women aged 55 and older reported this experience in the preceding 12 months (c. 12,800 women), compared with 3% of 25-34 year old women, the age group where this form of violence is most common. In relation to sexual assault, 0.2% of the sample aged 55 plus (c. 7,000 women) reported experiencing sexual assault in the preceding twelve months, against a national average rate across all age groups of 1%.
The other population-based study to yield approximations of prevalence of elder abuse (for women only) is the Australian Longitudinal Study of Women's Health (2014), which has measures relevant to vulnerability, coercion, dependence and dejection. This study is based on a random sample of women using a sampling frame from Medicare, with the oldest cohort (n = 5,561) being born between 1921 and 1926. When this cohort was surveyed in 2011 (at age 85-90), the findings suggested that 8% had experienced vulnerability to abuse, with name calling and put-downs being the most common forms. A similar level of prevalence was evident for this cohort in a preceding wave, conducted in 2008 (age 82-87), and slightly lower prevalence levels were found at younger ages (70-81 years). Measures the researchers used to assess neglect indicate a relatively stable prevalence rate of about 20% across waves, from ages 70-75 and 85-90 years.
Studies based on data from calls to helplines for elder abuse provide some further insights into the occurrence of elder abuse in Australia. There are three recently published sources from Queensland (Spike, 2015), Victoria (Joosten, Dow, & Blakey, 2015) and NSW (NSW Elder Abuse Helpline and Resource Unit, 2015). They reflect circumstances in which elder abuse is known or suspected and a person concerned has decided to seek advice on the situation.
In Queensland, calls to the EAPU helpline have increased substantially over the period that it has been operating, from just over 200 in 2000-01 to nearly 1,300 in 2014-15 (Spike, 2015; see further discussion in sections 3.2-3.4). The EAPU analysis of call data from the past five years provides a profile of the elder abuse concerns notified to the helpline. The calls were mostly in relation to female victims (68% female cf. 31 male cf. 1% unknown). The most common age group of victims was 80-84 years (23%), followed by 75-79 years (16%) and 85-89 years (15%). Perpetrators were male in 50% of calls and female in 45% (unknown: 5%). Where perpetrator age was known, the most common age group was 50-54 years (17%). Children were the largest groups of perpetrators reported (31% sons, 29% daughters). Otherwise, 10% were "other relatives", 9% a spouse/partner, and 21% fell into a combined category of neighbours, friends, workers and informal carers.
In 2014-15, the most commonly reported type of abuse to the EAPU helpline was financial abuse, accounting for 40% of reports, compared to 35% for psychological abuse, which had been the most common type up to 2012-13. The next most common types were neglect and social isolation, at about 10% each. Physical abuse was reported in just under 5% of calls, and sexual abuse was referred to in about 1% of calls. Where the perpetrator was a partner or spouse, the most likely form of abuse was psychological (41%). Where the perpetrators were adult children, financial abuse (39%) and psychological abuse (38%) were the most common types of abuse.
In Victoria, a recent study by the National Ageing Research Institute (Joosten et al., 2015), commissioned by Seniors Rights Victoria (SRV), was based on an analysis of data derived from records of calls to a helpline operated by SRV between July 2012 and June 2014. Of 755 calls, 455 involved discussion of a matter that raised elder abuse issues (including some that raised multiple types of abuse), and 236 raised issues not relating to elder abuse. The most common concerns raised in relation to elder abuse were about financial abuse (61%) and psychological or emotional abuse (59%). Physical abuse was raised much less frequently (16%), as were social abuse (9%), neglect (1%) and sexual abuse (0.4%). Elder abuse issues were most commonly reported in relation to female victims (73% females cf. 28% males) and the most commonly reported perpetrators were male (60% males cf. 40% females). The majority of perpetrators of the abuse reported to the SRV helpline were children of the victim (67%), with sons responsible for 40% of incidents reported, and daughters for 27%. Spouses were reported to be responsible in small proportions of cases (5% husbands and 3% wives).
In NSW, two years of call data (n = 3,388) to the NSW Elder Abuse hotline (NSW Elder Abuse Helpline and Resource Unit, 2015) reveal broadly similar patterns to the Queensland and Victorian data. Women were most commonly reported to be the victims (71% women cf. 28% men), and the most common age group of concern in the calls was 75-84 year olds (33%). In 71% of calls, the perpetrators were family members, and the largest group of perpetrating relatives were adult children (26% sons and 21% daughters). Just over one in ten (12%) of perpetrators were spouses. The most common abuse type reported in the calls was psychological abuse (57%), followed by financial abuse (46%), neglect (25%), physical abuse (17%) and sexual abuse (1%).
Three reports completed in the past five years (Clare et al., 2011; Miskovski, 2014; Wainer, Darzins, & Owada, 2010) have used data from a range of agencies to assess the extent and nature of elder abuse. The reports by Wainer, Darzins et al. and Miskovski specifically focused on financial abuse, and this kind of abuse emerged as the predominant concern in the report by Clare et al. Each of these reports illustrated the point that because responses to elder abuse are spread across different legal, policy and practice frameworks, the evidence available from these sources offers a piecemeal empirical understanding of elder abuse.
3.2 Risk factors and consequences
In the absence of systematic local research, insight into the factors that may mean older Australians are at higher risk of experiencing abuse, or the factors that may protect them against this risk is limited. As the discussion in the preceding section indicates, women are at higher risk of experiencing elder abuse than men (in part reflecting their greater representation in the older population; see further below). The literature indicates that there are different risk factors for different types of abuse. Among the common overall risk factors identified for which the empirical evidence is strong are when the older person has cognitive impairment or another disability, is isolated, or has a prior history of traumatic life events (Acierno et al., 2010; O'Keeffe et al., 2007; WHO, 2015). This section provides an overview of the main points that emerge from the literature on these issues.
Cognitive impairment or other disability
Cognitive impairment and other forms of disability are established in the research literature as having a strong association with being vulnerable to elder abuse (Acierno et al., 2010; Gil et al., 2015; WHO, 2015). The World Health Organization (2015) uses the term "intrinsic capacity" to refer to "all the physical and mental capacities" of an individual (p. 28), recognising that this varies across the life course and is influenced by a range of factors, including genetics (75%) and exposure to a variety of personal factors, such as socio-economic status. On average, intrinsic capacity peaks at age 20 and declines thereafter, with the rate of decline increasing from age 60. Compromised intrinsic capacity (as a result of conditions such as dementia or care dependence), which occur along a continuum ranging from low to severe, are associated with heightened risk of elder abuse, but are also a consequence of elder abuse (WHO, 2015). "Capacity", in a narrower sense, is a central concept in legal, medical and other responses to elder abuse, which recognises that there are degrees to which a person has capacity, and capacity may be present for some functions but not for others. In broad terms, capacity is the ability to make reasonable decisions. The link between cognitive impairment, which leads to reduced capacity, and elder abuse is well established (Acierno et al., 2010; Gil et al., 2015 & O'Keeffe, et al., 2007).
The Queensland EAPU analysis of helpline data (derived from calls made predominantly by family members and friends, but also from professionals) established that the incidence of abuse types observed varies according to whether the victim is reported to have dementia (Spike, 2015). Financial abuse is reported to occur at similar rates whether or not the victim has dementia, but psychological abuse (as a primary abuse type) occurs about half as often when the victim has dementia. This suggests that psychological abuse occurs to support financial abuse where dementia is not present, but is no longer necessary where dementia is present. Spike (2015) observed that "where financial motives are driving psychological abuse, once a victim has lost the capacity to manage their finances, psychological abuse becomes either: ineffectual as the victim no longer has the ability to direct their funds; or unnecessary because the perpetrator already has full access to the victim's assets". Miskovski (2014) observed the link between psychological abuse and financial abuse, noting that the former is a grooming behaviour for the latter.
Social isolation and traumatic life events
Social isolation has a well-established association with being vulnerable to elder abuse (Acierno et al., 2010; ALSWH, 2014; O'Keeffe et al., 2007; WHO, 2015). There are several dimensions to the connection between this condition and elder abuse. Isolation renders elders more vulnerable to exploitation for psychological, emotional and physical reasons, and it also means that abusive behaviour is less likely to be discovered due to the absence of social and other networks around the older person. Mariam, McLure, Robinson, and Yang (2015) explained the issues in this way:
As with most forms of abuse, access to the potential victim is a significant risk factor for the emergence of or continuation of elder abuse. Also in regard to living arrangements, social isolation has been shown to contribute to and result from ongoing abusive situations. Caregivers, family members and potential victims who lack substantial social networks experience increased demand on a limited number of caregivers and decreased social sanctions as a result of abusive behaviour, and they may avoid further social interactions out of shame or fear of discovery. (p. 20)
The association between experiences of elder abuse and previous traumatic events, including interpersonal and domestic violence, is evident in a range of sources (Acierno et al., 2010; Mann et al., 2014; UNDESA, 2013) and suggests elder abuse reflects the perpetuation of complex familial dynamics. Acierno et al. observed in their study that these experiences increased the risk of emotional, sexual and financial mistreatment. They suggested that:
there may be some shared variance between causes of these forms of mistreatment and precipitants of traumatic life events. On the most obvious level, interpersonal environments characterized by exposure to traumatic events are probably also more likely to contain abusive individuals over time. (p. 295)
There is a lack of detailed insight into the dynamics of intergenerational elder abuse in this context, and the extent to which elder abuse may be a response to the abusive adult child being abused or exposed to abuse in childhood involving the elder or other adults. Each of these dynamics is referred to in material emanating from practice perspectives on elder abuse,2 but empirical evidence is limited. A Canadian study examining prevalence and risk factors for "spouse abuse" at two different life stages (45-59 years, and 60 years and over) found slightly diminished rates of spousal abuse in the older sample, but a similar distribution between types of abuse (Yon, Wister, Mitchell, & Gutman, 2014). In the mid-age cohort, 9% experienced emotional/financial abuse, and 2% physical/sexual abuse. In the older cohort, the prevalence of emotional/financial abuse was 7%, and 1% for physical and emotional abuse.
Other factors
Other factors that have been established as risk factors for the perpetration of elder abuse include the perpetrator’s depression or alcohol and drug misuse, and the perpetrator being in a position of financial, emotional or relational dependence with the victim (WHO, 2015).
More generally, a theme that emerges from the analytic literature on elder abuse, but has not necessarily been directly measured in research, relates to attitudes and values (Gil et al., 2015; UNDESA, 2013; WHO, 2002a, 2015). As flagged at the outset, attitudes and values are associated with elder abuse in several different ways. Generally, social and individual values that fail to accord respect and consideration to elders and their human rights are considered to create an environment conducive to elder abuse (Peri, Fanslow, & Hand, 2009). Some literature points to an association between gender roles and elder abuse, particularly financial abuse, because under traditional gender role paradigms, women have not expected, or been expected, to take responsibility for financial matters. In this respect, norms that support women's relinquishment of financial control to others are also seen to be conducive to creating opportunities for elder abuse (Peri et al., 2009).
Consequences
Elder abuse has a range of physical, psychological and financial consequences. It can result in pain, injury and even death, and is associated with higher levels of stress and depression and an increased risk of nursing home placement and hospitalisation (WHO, 2015). Darzins, Lowndes, and Wainer (2009) referred to research suggesting that the effects of financial abuse on the elderly tend to be greater than on young people, as older people lack the capacity and time to recoup their financial losses, and those who suffer financial abuse experience "higher levels of psychological distress and depression than their peers … decline in physical health coupled with decreased resources for managing their healthcare" (p. 12).
Prevention
Preventative responses to elder abuse are generally seen to be underdeveloped in Australia. Directions in the themes underpinning thinking about prevention have two broad elements locally and internationally. The first is oriented toward changing the values and attitudes among the broader community and among professionals and individuals who interact with elders to address ageist (and sexist) assumptions and attitudes and to develop understanding of ageing processes, including potential cognitive decline. The second is oriented toward mitigating the risk factors for elder abuse, through measures to reduce social isolation, increase autonomy and empowerment, and support retention of control over financial affairs, or at the very least to help elders maintain knowledge of their financial affairs (e.g., Mariam et al., 2015; Wainer, Darzins et al., 2010). These issues are further discussed in section 7.
3.3 What is known about particular types of elder abuse?
Financial abuse
Of the different types of abuse identified in the preceding section, financial abuse is the most well researched in Australia. Evidence is sparse on the other kinds of abuse, although there is one recent qualitative study on sexual abuse and older women. There is little research on psychological abuse and neglect, although, as noted earlier, there is some evidence that suggests psychological and financial abuse often co-occur, and that psychological abuse may be a form of "grooming for financial abuse" (EAPU, n. d.; Miskovski, 2014; Wainer, Darzins et al., 2010).
The WHO (2002a) defines elder financial abuse as "the illegal or improper exploitation or use of funds or resources of the older person" (p. 3). Darzins et al. (2009) estimated that this experience affects between 0.5% and 5% of older Australians. The forms that financial abuse takes are varied, and it is this kind of abuse that is most likely to come to the attention of professionals across various areas (including banking, law and the welfare sector) because it may involve transactions and engagement with institutions and organisations. Financial abuse covers a spectrum of behaviours, and a guide published by Seniors Rights Victoria describes it as existing "in the grey area between thoughtless practice and outright theft" (Kyle, 2012, p. 7).
Several studies and analytic reports have raised concerns about financial management practices that are risky from the perspective of both the elder whose finances are being managed and the person managing them. Assistance in managing financial arrangements may be informal or formal in nature, ranging from informal responsibility for banking and bill payments, to substantial responsibility for financial arrangements being assumed. The frameworks and instruments governing formal transfers of financial responsibility are those relating to enduring power-of-attorney instruments, which are executed when a person has capacity, and allow another person (the attorney) to take responsibility for financial matters. If an enduring power of attorney has not been executed and it becomes necessary for someone else to exercise responsibility for an elder's financial affairs, then application must be made to a guardianship board or tribunal. It appears that anticipatory execution of enduring power-of-attorney instruments is common, with one study of supported asset management identifying 69% of a sample of 421 Victorians aged 65 and over using an enduring power of attorney (Tilse, 2007, as cited in Wainer, Darzins et al., 2010).
In 2010, Wainer, Darzins, and Owada observed that "supported asset management is a common experience for family members and there is much work to be done to understand the dynamics of this form of care, particularly in a multi-cultural society" (p. 6). In this area, varying societal values about the extent to which assets are considered communal or personal within a family are evident, and it is also evident that expectations are culturally determined (Miskovski, 2014; Wainer, Darzins et al., 2010). The study by Wainer, Darzins and Owada was based on an analysis of data from a range of agencies whose operations bring them into contact with elder financial abuse in Victoria. The findings of this study, consistent with the discussion in section 3.2, showed that, to the extent data were available, between one- and two-thirds of the elderly concerned were vulnerable because of dementia. The interviews with professionals also confirmed that financial abuse was accompanied by psychological abuse that was intimidating, controlling and fear inducing. Among the ways in which financial abuse was carried out were through misuse of powers of attorney, coerced changes to wills, unethical trading in title to property, and the coercion of people without capacity into signing documents in relation to assets that would result in financial gain for the perpetrator. Concerns were also raised, particularly by professionals from helplines, in relation to situations where adult children were dependent on aged parents for accommodation or financial support by reason of addiction or mental ill health, but failed to fulfil reciprocal expectations in relation to caregiving activities. Another area where financial abuse was identified was where an adult child held power of attorney and was also the beneficiary of a will and acted to preserve their inheritance by not selling the family home to release funds for an assisted accommodation bond, even though this was needed for their parent. Another analysis of the circumstances in which concerns about financial abuse arise indicated that in some circumstances adult children holding powers of attorney may use this power to gain pre-mortem control over heritable property and exhaust the resources in the estate, to the disadvantage of the other beneficiaries (Miskovski, 2014).
Wainer, Darzins et al. (2010) concluded that the legal system was rarely used and unhelpful when trying "to prevent or remedy financial abuse". There were a number of reasons for this, including privacy issues and the lack of an easily identifiable and accessible mechanism for reporting concerns. These findings are consistent with those of a multi-dimensional study by Tilse et al. (2005) on practices surrounding the management of older people's assets. The research found poor understanding of legal obligations and mechanisms in relation to assisted asset management among elder people and those caring for them. It also highlighted "attitudes that suggest entitlement" to the older person's assets, that together with risky asset management practices, created the conditions for financial elder abuse. Concluding that legal redress is often unattainable for practical reasons (assets are unrecoverable) or personal reasons (the older person decides that maintaining relationships is more important than pursuing justice), the researchers highlighted the need for a cross-sectoral approach involving financial institutions, advocacy organisations and agencies concerned with providing services to older people.
Bagshaw and colleagues (2013) examined in separate surveys the views of 209 service providers on the risk factors for elder financial abuse, and the concerns of 114 older people and their family members about financial abuse. Six risk factors were identified by majorities of services providers:
- a family member having a strong sense of entitlement to an older person's property or possessions (84%);
- an older person having diminished capacity (82%);
- an older person being dependent on a family member for care (81%);
- a family member having a drug or alcohol problem (73%);
- an older person feeling frightened of a family member (73%); and
- an older person lacking awareness of his or her rights and entitlements (72%).
About half of the sample of older people and their family members indicated they did not have concerns about financial management issues. The balance indicated they were "somewhat concerned" (30%), "concerned" (8%) or "very concerned (18%).
Sexual abuse
As the prevalence and helpline data set out in section 3.1 indicate, sexual abuse appears to be an uncommon form of elder abuse; however, the ANROWS analysis of Personal Safety Survey data suggests it is potentially experienced by thousands of older women annually.
Empirical evidence in this area is limited, but a recent study by researchers at La Trobe University has shed some light on the issue. Mann and colleagues (2014) conducted a study involving professionals concerned with sexual assault, service providers in aged care services, and women over 65 who had experienced sexual assault, their family members and friends. The findings showed that "the sexual assault of older women occurs in a wide range of contexts, settings and relationships. Older women remain vulnerable to sexual assaults by husbands/partners and family members. They can also face threats from service providers that they may rely on for general care, health care and intimate care. Assaults in such settings can be perpetrated by female as well as male staff" (p. 2). The research highlighted a lack of mechanisms to ensure that professionals such as personal care workers were fit for the responsibilities of working with the aged, and suggested a need for licensing of these workers and a way of conducting background checks analogous to the Working with Children Checks that are required for people who work with children (Child Family Community Australia, 2014). It also revealed mixed views on the question of reporting obligations, with evidence of some support among professionals for mandatory reporting. Concern was expressed in relation to gaps in reporting obligations. Most significantly, the research highlighted the fact that no statutory reporting obligations apply in aged care services that do not receive Commonwealth government funding. The researchers also expressed concern about the narrow statutory reporting obligations in the Aged Care Act 1997 (Cth) in relation to Commonwealth-funded facilities, and the implications of the discretion not to report (where reporting would otherwise be mandatory) in circumstances where the reportable act is committed by a person with cognitive impairment.
3.4 Elder abuse in particular contexts
As with elder abuse in general, insight into elder abuse in particular contexts is limited, including among Aboriginal communities, culturally and linguistically diverse (CALD) communities, rural communities, and gay, lesbian, bisexual, transsexual, intersex and queer (GLBTIQ) communities (Higgins, 2004). As the dynamics of elder abuse are context dependent, there remains much to be understood about the extent to which the dynamics of elder abuse are different or similar in varying contexts, and the extent to which different responses may be required.
In relation to elder abuse in Aboriginal communities, a 2005 report by the Office of the Public Advocate in Western Australia established that in the Aboriginal context, even at the level of terminology, the conceptualisation of the mainstream concept of elder abuse requires reconsideration. Both the terms "elder" and "abuse" were considered problematic, as "elder" has a specific meaning in Aboriginal communities, and "abuse" may be considered inapt and confrontational. The research indicates that, as in the non-Aboriginal context, the most common type of abuse is financial but that other types of abuse also occur. Two factors that were identified as having particular implications in the Aboriginal context were cultural obligations and the circumstances of grandparents. From a cultural perspective, Aboriginal norms in relation to reciprocity, the expectation that resources will be shared, and kinship (where a wide variety of relationships are involved in familial and community networks), are dimensions that complicate understandings of whether and how elder abuse is occurring. The extent to which calls on grandparent resources to care for grandchildren are culturally reasonable or unreasonable was also highlighted by the research. Substantially more work is required to understand and conceptualise elder abuse in the Aboriginal context, especially among different groups in different circumstances, given the diversity among Aboriginal and Torres Strait Islander communities.
In CALD communities, the literature suggests that a number of factors can heighten vulnerability to abuse, including language difficulties for those whose primary language is not English, social dependence on family members for support, and the potential conflict caused by cross-generational expectations in relation to care (Bagshaw et al., 2009). Two studies have shed some light on these issues, although of course the extensive range of cultures represented in our community, the spread of religious and cultural values, and the diverse range of settlement and migration pathways and timeframes mean that a complex range of dynamics will be relevant in different families and communities. A study by Wainer and colleagues (2011) examined practices in Greek, Italian and Vietnamese communities in relation to asset management, enduring power of attorney instruments and wills, and knowledge about elder abuse. The research highlighted similarities and differences between these groups in their awareness of and attitudes to elder financial abuse, and in relation to assisted asset management should that become necessary. All three groups had an awareness of elder financial abuse, and Italians were more likely than the other groups to know of examples of this. Greeks were most likely to believe elder financial abuse to be common, and the Italians and Vietnamese were least likely to believe this. All three groups intended to rely on family members for assistance with asset management should they be unable to manage this themselves. The use of wills and enduring powers of attorney was high among Italian and Greek participants, but not the Vietnamese.
In a focused case study exploration, Zannettino, Bagshaw, Wendt, and Adams (2015) documented one account where a mother, born in a northern European country, was reported by her son to have been isolated from her other children by her abusive daughter. One consequence of the abuse was that the mother was coerced into signing a will leaving the majority of the estate to the abusive daughter. The authors concluded that the case study demonstrates "the relationship between financial and emotional abuse in the context of CALD older people, whose isolation from the dominant culture may make them more dependent on family members and more vulnerable to abuse" (p. 82).
Some issues particularly pertinent to people resident in rural areas have been highlighted in the research (Tilse et al., 2006; Wainer, Lowndes, Owada, & Darzins, 2010). These include the complexity of assets held by families resident in rural areas such as farming properties; lack of access to services that may assist with asset management arrangements and responses to situation where elder abuse is occurring or expected; and the dynamics involved in reporting or disclosing elder abuse in rural communities, where shame and concern to protect the family name potentially play an inhibiting role. The rural participants in Wainer, Lowndes et al.'s study showed lower levels of confidence in their own ability to recognise whether an elder was experiencing financial abuse. Tilse et al.'s study highlighted the complex and potentially conflictual dynamics around farming properties with the multi-generational interests involved where the farm is the family business. These included complications about the treatment of farms as inheritance, and the balance between providing for children and maintaining the family business, placing one child in a different position from the others, and the treatment of labour and other contributions to the improvement of the farm in estates.
3.5 Dynamics in relation to disclosure and reporting
Complex dynamics and structures are relevant to consideration of the questions of disclosing, discovering and reporting elder abuse if it is disclosed or discovered. This section introduces some the issues raised in the empirical and analytic literature, with reporting obligations and mechanisms discussed more formally in section 6.
Empirical evidence on these issues is very limited in Australia. Elder abuse is generally considered to be remain hidden to a significant extent, and if it is disclosed or discovered, under-reported (Jackson & Hafmeister, 2015; UNDESA, 2013; WHO, 2002b). A range of issues is influential in this context, including difficulties in detecting and identifying elder abuse and the conditions within which it occurs. The same factors that are associated with vulnerability to elder abuse - social isolation and cognitive impairment - also militate against disclosure or discovery and reporting. Where abuse occurs in the context of familial or caregiver relationship dynamics (Jackson & Hafmeister, 2015), this may inhibit a parent disclosing mistreatment by a child and a spouse disclosing mistreatment by a partner. The dynamics of dependence are also relevant, since an aged person may be reluctant to disclose abuse by someone on whom they depend for care, since disclosure may mean withdrawal of the care and potentially an unchosen change in living circumstances. Cognitive impairment may also mean that an older person is unable to disclose or is not believed when they do disclose. Shame, embarrassment, fear of negative repercussions and/or a belief that disclosure and/or reporting may result in no consequences or negative consequences may also be relevant.
The question of reporting obligations in Australia is the subject of significant debate. Apart from limited obligations in relation to specific offences for Commonwealth-funded care facilities (Aged Care Act 1997 (Cth), s 63-1AA), there are no statutory mandatory obligations on professionals to report elder abuse (see section 6.1). Reporting pathways are acknowledged to be complex and confusing both for members of the community and professionals. Duties in relation to reporting depend on the professional context in which elder abuse is discovered. Some analyses have shown that even professionals providing care and other services to elders are unaware of reporting mechanisms (e.g., Miskovski, 2014).
There are a number of different perspectives on the question of whether mandatory reporting obligations should be introduced. One view is that mandatory reporting is paternalistic and detracts from the autonomy of the elder involved. This position is predicated on the view that the elder is in the best position to make a decision about whether abuse should be reported, and derogating from this position reflects an infringement of their human rights, particularly the right to self-determination (EAPU, 2006). Although some organisations and individuals suggest that mandatory reporting might be an appropriate response where elders have diminished capacity, the EAPU asserts that existing obligations arising from professional duty of care requirements already impose sufficient reporting requirements on professionals.
Research suggests mixed views among professionals. The Alzheimers Australia NSW (Miskovski, 2014) study found some support for mandatory reporting of financial abuse among professionals. The study by Mann et al. (2014) on sexual assault and older women also found support among some professionals for mandatory reporting of sexual assault in this context, but this was not a universal view. Mann and colleagues summarised the complex issues that arise in this context in this way:
Such accounts highlight complex ethical, legal, managerial and practical dilemmas and they point to tensions between rights and responsibilities. They also raise issues that extend beyond the residential care sector, suggesting the need for a wider response that encompasses the spectrum of settings in which older women live (p. 53).
A study from the US that interviewed victims and case workers from an adult protective service to examine the dynamics of detection and disclosure showed that relationship factors were an important influence in whether elder abuse was: (a) detected, and (b) reported (Jackson & Hafmeister, 2015). This indicates that where there is a close relationship between the victim and perpetrator, abuse tends to be reported only when it reaches a high threshold of severity. Abuse is more likely to be reported when the victim-offender relationship is not close; for example, when the abuse is being committed by a care worker. The study also found that the relationship between the victim and the person reporting the abuse is relevant, with superficial connections - such as when the reporter is a professional rather than a family member - resulting in reports occurring more readily.
2 See, for example, the EAPU web page on risk factors: <www.eapu.com.au/elder-abuse/risk-factors>.
4. Australia's older population: Demography and health statistics
This part of the discussion focuses on two important aspects of the social, demographic and health backdrop to the issues considered in this paper. It profiles the demographic characteristics of older Australians on the basis of ABS data derived from the 2011 Census (in particular ABS, 2012b, 2013c) and sets out projections in relation to ageing. The discussion also highlights a range of issues, including relationship status, living circumstances, cultural background and disability status that are relevant to a range of considerations in relation to risk factors and response opportunities for elder abuse, as identified in the preceding section. The discussion also uses Australian Institute of Health and Welfare (AIHW) data to identify the health implications of our ageing population, which again provides insight into the extent of some risk factors and response opportunities for elder abuse.
4.1 Older Australians
Older Australians have increased significantly as a proportion of the total population, reaching 15% (15% women, 14% men) in June 2014 (ABS, 2015a), compared with 7% in 1941 (n = 3 million). The proportion of people aged 85 years and older tripled between 1971 and 2014, from 0.5% to 2%. Population projections indicate that these trends are set to continue, due to a combination of improved life expectancy and fall in fertility rate since the late 1960s. The ABS has projected that persons aged 65 years and older will account for 20-21% of the Australian population by 2040, and 21-23% by 2050 (Figure 1). The projections indicate that from less than 2% in 2011, persons aged 85 years and older will represent about 4% of the Australian population by 2040, and 4-5% by 2050.
4.2 Relationship status
In terms of relationship status, 73% of men and 63% of women in the 65-69 year age bracket were recorded as being married in the 2011 Census (ABS, 2012b), with this differential broadening in the older age brackets due to the lower life expectancy of men compared to women (80.3 years for men cf. 84.4 years for women in 2014) (ABS, 2015b). The proportions of men and women who reported being widowed peaked in the 90+ age group, at 49% of men and 85% of women. Widowhood was most common for men when they were in the 90+ age bracket, with 49% having this status, whereas for women, 85% in this age group were widowed. Widowhood was common for women in 75-79 year age bracket (40%), compared with just 5% of men.
In the 85-89 year old age bracket, 59% of men were married, compared to 19% of women (ABS, 2012b). The proportion of divorced men in the 65-69 year old age bracket was 13%, compared with 15% of women.
4.3 Cultural background
In the 2011 Census, Aboriginal and Torres Straight Islander peoples made up 3% of the population under 64 years, and only 1% in the 65 years and over group (ABS, 2012b).
Australia's older population reflects significant cultural diversity due to post-war immigration policies, with 36% of 65+ year olds having been born overseas (compared to 24% of people under 65 years old) (ABS, 2012b). Among the older immigrants, 25% in 2011 were from non-Anglo countries, compared with 12% from the UK and Ireland. The country of origin with the largest representation of older Australians, after the UK and Ireland, was Italy, followed by Greece. Australia's older population will become increasingly culturally diverse, with weakening dominance of immigrants from European countries. Indeed, while 5% of people aged 65 years and over were from Asian countries in 2011, the proportions were 8% of people aged 50-64 years, and 11% of those aged 35-49 years.
Figure 1: Proportion of projected population aged 65+ years and aged 85+ years, based on three alternative sets of assumptions, 2011-2101
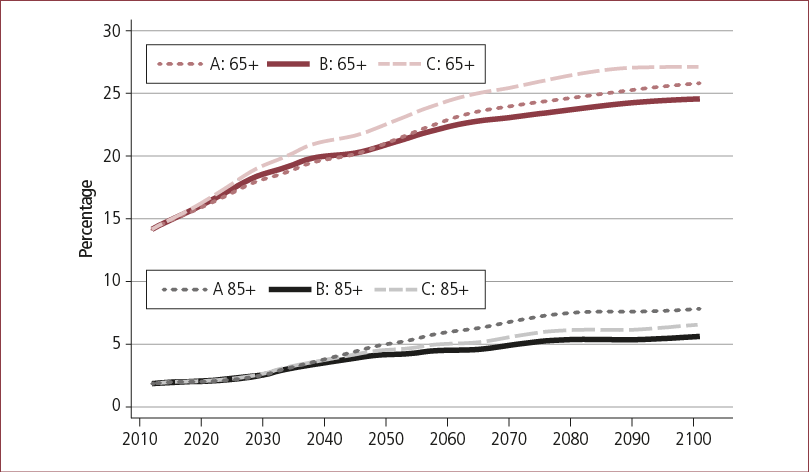
Notes: Series A: total fertility rate = 2.0 births per women from 2026; net overseas migration = 280,000 from 2021; life expectancy = 92.1 and 93.6 for men and women from 2061. Series B: total fertility rate = 1.8 births per women from 2026; net overseas migration = 240,000 from 2021; life expectancy = 85.2 and 88.3 for men and women from 2061. Series C: total fertility rate = 1.6 births per women from 2026; net overseas migration = 200,000 from 2021; life expectancy = 85.2 and 88.3 for men and women from 2061.
Source: ABS (2013b).
4.4 Disability
Increasing increments of older Australians are classified as having a profound or severe disability across the 65+ year age brackets, standing at 9% for 65-69 year olds, and rising to 67% in the 90+ age group according to 2012 Survey of Disability, Ageing and Carers (ABS, 2013a).
AIHW estimates indicate that 342,800 Australians had dementia in 2015, with this reflecting a rate of one in ten in the 65+ age group, and three in ten for the 85+ age group.3 AIHW projections indicate that the number of people with dementia will grow to 400,000 in 2020 and 900,000 in 2050. More than 50% of permanent residents in Australian Government-funded aged care facilities in 2013-14 had a diagnosis of dementia.
4.5 Where do older Australian live?
In 2011, the two states with the highest concentrations of older Australians were Tasmania and South Australia (16% each; ABS, 2013c), followed by NSW, Victoria, Queensland and WA, which were close to the national average of 14%. The two territories had noticeably lower proportions, especially the Northern Territory, with 6%, reflecting the higher proportion of Aboriginal people in that territory, who typically have a younger age profile than non-Indigenous Australians.
Most older Australians, like most Australians, lived in major urban areas in 2011 (65%; ABS, 2013c). About a quarter of older Australians (23% men and 24% of women) lived in other urban areas (smaller cities and towns). Bounded localities, classified as areas with between 200 and 900 people, were home to 3% of older men and 4% of older women. Of older people, 10% of men and 7% of women lived in rural areas.
For the 65-74 year old age bracket, the most common living arrangement was living in a private dwelling with a spouse or partner, with 67% in these circumstances (74% men and 60% women; ABS, 2013c). In the 75-84 and 85+ age brackets, the gender differential increased, with 46% of men and 11% of women aged 85 years and older living in this situation. A quarter of all older Australians lived alone (32% of women and 17% of men), while 8% lived with other relatives, including their siblings or children.
The higher life expectancy of women is reflected in the patterns in their living circumstances among older men and women. Thirty-two per cent of older women lived alone in 2011, compared to 17% of older men (ABS, 2013c). More older women than men lived with family members other than a partner (65-74: 10% women cf. 4% men; and 85+ years: 15% women cf. 7% men). Most commonly, people in these arrangements were living with one or their children.
Most people aged 65 years and over lived in private dwellings (94%; ABS, 2013c). The most common other living circumstance was non-private dwellings (covering a range of non-self-contained, mostly supported, arrangements). By the age of 85 and older, the proportion of people living in non-private dwellings was 18% (men) and 31% (women), compared with 2% (men) and 1% (women) aged 65-74.
3 See the AIHW's information on dementia: <www.aihw.gov.au/dementia/>.
5. Socio-economic context and intergenerational wealth transfer
The socio-economic characteristics of Australia's ageing population raise some significant issues when considering and developing policy responses to elder abuse. The management of the financial resources and assets of older Australians in particular raises significant challenges. This section considers the socio-economic backdrop to the forms of financial abuse described in section 3, and the likely increase in the coming decades in the numbers of Australians with cognitive decline. It also sets out what is known about attitudes to and the dynamics of inter-generational wealth transfers before and after death, and community practices in relation to will-making, bequests and estate contestation.
As a result of the strong economic conditions that have characterised the baby boom generation's life cycle, the aggregated value of the assets that they hold is significant. Baby boomer wealth profiles are characterised by high levels of home ownership and the rewards of the periods of economic prosperity that have occurred throughout their adult lives. One estimate indicates that the total household wealth that may be subject to transfer by bequest (largely due to high rates of home ownership) may be as high as $70 billion in 2030 (Kelly, Harding, AMP, & NATSEM, 2003), up from $8.8 billion in 2000. In addition to home ownership, the introduction of the Superannuation Guarantee system in 1993 has seen substantial growth in levels of superannuation holdings, which in turn has increased the amount of potentially heritable assets. The 2015 Intergenerational Report: Australia in 2055 predicted that superannuation assets - which stood at $1.84 trillion at the end of 2013-14 - could rise to $9 trillion by 2040 (Treasury, 2015). Depending on how retirement income streams are managed, this may mean that in the future substantial levels of superannuation residues may be transferred to beneficiaries posthumously, given the evidence that some retirees manage fears about outliving their income streams by taking a frugal approach to expenditure (Wu, Asher, Meyricke, & Thorp, 2015).
The implications of the home ownership profile of the now ageing baby boomer generation have been studied by human geographers for some time. Writing in 2001, O'Dwyer noted that:
the transfer of housing wealth which will occur when the baby boom cohorts (currently the inheriting generation) reach the end of their life cycles in 20-30 years time may indeed represent a significant transfer of wealth. We already know that home ownership among this generation is very high and they tended to have fewer children than their parents' generation. Thus the pie of wealth will not only be larger, but will be divided between fewer persons. (p. 96)
The extent to which this prediction eventuates will depend on how the baby boomer generation manages its wealth, the extent to which assets are decumulated prior to death, and the extent to which assets are exhausted in meeting financial and care needs over an extended life span (Olsberg & Winters, 2005). Whether distribution of wealth (housing, investments, retirement income streams and residues) occurs posthumously or not, the socio-economic profile of the baby boomer generation means that the emerging generations of older Australians have much greater levels of assets than those that preceded them.
A further influence arises from the disparities in wealth and access to housing between the baby boomer generation and the generations that follow (Barrett, Cigdem, Whelan, & Wood, 2015; Birrell & McCloskey, 2015). The extent to which, through pre- or post-mortem distribution of assets, this will mean that the intergenerational transfer of wealth will support access to home ownership for the children and grandchildren of the baby boom generation has been the subject of some debate in the academic literature. Uncertainties in this context arise in relation to the attitudes of the older generation, the extent to which they voluntarily preserve or transfer assets for and to their children, and the extent to which assets are not exhausted by the need to meet care and health needs in the face of longer life expectancy (Tomlinson, 2012). The concept of "inheritance impatience" has been developed, meaning: "a situation where family members deliberately or recklessly prematurely acquire their ageing relatives' assets that they believe will, or should, be theirs one day" (Miskovski, 2014, p. 18).
Researchers have highlighted the tensions that arise in relation to wealth preservation or dispersal, the care needs of older generations and the wealth transfer expectations of younger generations (Darzins et al., 2009; Wilson, Tilse, Setterlund, & Rosenman, 2009). This is an area where private interests and public policies intersect in multiple and complex ways, particularly in the context of aged care policies being oriented toward developing a self-funded aged care system, and access to the aged pension being means tested. Wilson et al. analysed the issues raised in this way:
older people's assets can be a site of competing interests. Families have an interest in protecting potential inheritances; the market has interests in promoting lifestyle, care and accommodation options, as well as financial products, such as reverse mortgages; the state is concerned with self-provision and financial independence in older age, and, with service providers, also has an interest in preserving assets to pay user charges for health, care and accommodation in older age. (p. 156)
In this context, generational attitudes and expectations in relation to asset transfers before or after death, and the broader question of attitudes and expectations in relation to mutual or non-mutual intergenerational support in terms of material resources and care, form an important part of the backdrop to the social and economic dynamics that may influence the conditions in which elder abuse occurs. Research based on a sample of 7,000 Australians aged 50 and over reveals a significant amount of complexity in some of these dynamics (Olsberg & Winter, 2005). The authors suggested that the findings showed an erosion in the concept "of a strong and supporting family structure" among the participants, with the emergence of a shift away from "self-sacrifice" to "self-interest" in relation to attitudes to obligations by adult children. In part, this was underpinned by a realisation among participants that their resources would need to remain available to fund their own care and would probably be exhausted by the end of their own lives. But the research also highlighted the prevalence of attitudes negating the observation of continuing obligations to provide financial support for older children, on the basis of a perception that the participants had made enough sacrifices in their children's interests and that the younger generation had "had it all". One third of the sample had already provided support for their children to purchase homes, mostly in the form of an informal loan, often interest free. Particular indications of negative intergenerational dynamics were evident among participants who had experienced relationship breakdowns and re-formations, and there was concern among participants about the implications of these dynamics for potential conflicts over inheritance.
The study by Olsberg and Winter (2005) is one of a very limited number of studies on intentions and actions in relation to pre-mortem transfers of wealth, and the dynamics in this area remain little understood. This is particularly so where such a transfer is part of a "family agreement" in which access to housing, or support to obtain housing, is part of a familial (usually intergenerational) arrangement in which it is exchanged for care and support so that a parent may avoid assisted living or aged care arrangements. These agreements may have various degrees of formality, but evidence considered by the House of Representatives Standing Committee on Legal and Constitutional Affairs on Older People and the Law (2007) raised concern about the lack of specific mechanisms regulating them (para. 4.40). The limited evidence available in relation to such arrangements indicates that some may be disadvantageous to the older adult, such as in circumstances where expectations about care are not fulfilled, but the material part of the agreement is irreversible or would take significant effort to reverse (Miskovski, 2014). The House of Representatives (2007) report concluded that "the potentially disastrous consequences that can be suffered by parties to family agreements due to uncertainty, dispute or abuse warrant some form of regulation, particularly if the use of family agreements increases in the future" (para. 4.40). Case studies presented in various reports, including that published by Miskovski, suggest that, in some cases, family agreements and the exercise of powers under enduring power-of-attorney instruments may provide scope for assets to be stripped out of estates.
The available empirical evidence in relation to the post-mortem transfers of assets demonstrates that most people in the older age groups have wills, and that intestacy (not having a will) is rare. In the 50+ year cohort surveyed by Olsberg and Winter (2005), 96% had a will. A more recent study by Tilse, Wilson, White, Rosenman, and Feeney (2015) also evidences an increased emphasis on will-making from middle age onwards. In their community sample of 2,400 people, having a will became more common than not having a will in the 40-49 age group, with 62% of this sub-sample having a will. Increasing increments of participants in the older age groups had a will, rising to 93% in the 70+ age group. The research by Tilse et al. and another study in the same research program on court judgments in will disputes over a one-year period, shed some light on the dynamics surrounding inheritance and will disputes. The analysis suggests that norms and practices in these areas are shifting in line with some social attitudes. From a socio-legal perspective, the context for this has been shifts in some Australian jurisdictions that have weakened longstanding principles in support of testamentary freedom in favour of strengthened recognition of obligations to provide for dependents. In some areas the class of person who may claim entitlement to provision from an estate has also widened (Tilse et al., 2015; White et al., 2015). Consistent with the findings of Olsberg and Winter (2015), Tilse et al. found that participants were not necessarily preserving wealth to ensure a substantial inheritance. Providing for dependents while alive, as well as living comfortably in old age and retirement were seen as just as important. The most common approaches to bequests were providing for spouses and distributing estates equally among children (consistent with Baker & Gilding, 2011). The study indicates that pre-mortem material support for adult children, where the same values in relation to the equal treatment of children in relation to pre-mortem wealth transfers were not evident, is not interconnected to any great extent with approaches to bequests in wills.
The study by White et al. (2015) analysed 195 judgments from 2011 (sourced from AustLII) in relation to disputes over wills, and sheds light on some of the dynamics underlying situations where wills, and the arrangement made in them, are disputed. The analysis showed that the most common class of cases in the sample reflected circumstances where a person with eligibility under the relevant state legislation was seeking to gain or increase a share of the estate (family provision claims, 99 cases). Where the contests involved a partner of the deceased person, 17 (out of 27) involved challenges to provisions made for children of a previous relationship of the deceased, and only one involved a case against the current partner's own child. Where claims were being made by children (73 cases), they most commonly reflected a contest between siblings (43 cases), but challenges by children against provisions made for partners were not uncommon (20 cases). In considering the contests involving siblings, the published account of the research does not shed light on the circumstances that underlie such disputes. In terms of the issues considered in this section, the study findings indicated, consistent with the concerns expressed by the participants in Olsberg and Winter's (2005) sample, that family re-formation is associated with disputes over wills, indicating that complex family dynamics continue to be manifested even at this life stage. White et al. observed that disputes between siblings and those between children of a former marriage and subsequent partner of the deceased are the "fiercest" (p. 902). The authors also observed that the study showed that "competent, financially comfortable adult children are making claims" against estates (p. 906), in contrast to the original intention of family provision law to ensure that widows and children of the deceased were not left financially destitute.
In the study by White et al. (2015), validity was the legal ground most likely to indicate circumstances where elder abuse may have occurred. In the study, two distinct legal categories were grouped together under this heading: circumstances where it was claimed the will-maker did not have the capacity to make the will; and undue influence, where it is claimed that the will is the result of the will-maker's intention being overborne. These grounds were raised in 43 out of 195 cases in the sample.
6. Structures, frameworks and organisation
The discussion in this chapter will identify a range of intersecting frameworks and structures that potentially engage with elder abuse across a range of areas, laws and jurisdictions. Following an examination of the Commonwealth legislative and policy frameworks, examples from the range of state and territory frameworks will be considered, prior to an examination of financial systems focusing on measures encouraging financial literacy and protecting against financial abuse. The chapter will conclude with a brief discussion of a range of advice and advocacy services available through non-government organisations and community bodies that facilitate protection against, and response to, the perpetration of elder abuse.
6.1 Commonwealth legislative and policy frameworks
Legislative frameworks
In spite of the “myth of an all-encompassing federal legal and policy dominance in the ageing portfolio" (Lacey, 2014, p. 101), the Commonwealth Parliament has limited sources of power with which to legislate specifically with respect to elderly Australians and aged care. The Commonwealth of Australia Constitution Act (the Constitution) contains the following heads of power which may provide a basis for the Commonwealth to legislate on matters for this population:
- s 51(xxiii): invalid and old-age pensions;
- s 51(xxiiiA): … widows' pensions … pharmaceutical, sickness and hospital benefits, medical and dental services …;
- s 51(xiii): banking…;
- s 51(xx): foreign corporations, and trading or financial corporations formed within the limits of the Commonwealth;
- s 51(xiii): banking …;
- s 51(xxix): external affairs; and
- s 51(xxxix): matters incidental to the execution of these powers.
Also of note in the context of potential authority to provide for elderly Australians are s 61 of the Constitution, which relates to the executive power of the Commonwealth, and s 96, which enables the Commonwealth Parliament to grant financial assistance to any state on such terms and conditions as the Parliament thinks fit.
While relevant, the provisions enumerated above do not specifically enable the Commonwealth to legislate or otherwise provide for protection against elder abuse. Nevertheless, s 61 and s 96, in addition to s 51(xxix) of the Constitution, have been identified as providing potential bases for the enactment of a national framework for protection against elder abuse, albeit that s 96 would authorise the funding of a scheme to be administered by the states and territories (Lacey, 2014, p. 103). In particular, the external affairs power in s 51(xxix) has been identified as holding the greatest prospect of enabling a human-rights-based approach to underpin a national protective framework, and this avenue will be discussed further below.
Current Commonwealth programs and legislation regulating aged care
While there is no comprehensive adult protection legislation at present in Australia, of particular relevance among the current legislative instruments in the Commonwealth jurisdiction is the Aged Care Act 1997 (Cth), which provides the regulatory framework for the provision of aged care.4 This Act, which is primarily based on the pensions/benefits power in s 51(xxiii) and on the corporations power in s 51(xx), governs both residential care and home care, making provision for the Commonwealth to provide financial support “through payment of subsidies for the provision of aged care" and “through payment of grants for other matters connected with the provision of aged care" (s 3-1(1)).
Commonwealth responsibility for the provision of aged care was recently expanded following the introduction of the National Partnership Agreement on Transitioning Responsibilities for Aged Care and Disability Services (Council of Australian Governments, 2012) and the Living Longer, Living Better program, which extended Commonwealth funding of home and community care (now “home care") support for elderly Australians and initiated program reform intended to provide improved service provision (Department of Social Services, 2013). As a result, from 1 July 2012, the Commonwealth Home and Community Care program (now the Commonwealth Home Support Programme) took on full funding, policy and operational responsibility for Australians in all states and territories aged 65 years and over (and Aboriginal and Torres Strait Islanders aged 50 years and older),5 save for Victorian and Western Australian older persons.6
The regulatory system in the Aged Care Act 1997 (Cth) provides for the accreditation of service providers, the imposition of obligations on these service providers and the establishment of the Aged Care Complaints Scheme.
More specifically, Division 54 of the Aged Care Act 1997 (Cth) makes provision for determination of quality care and accommodation standards. Part 4.1 makes provision for Quality of Care Principles (currently the Quality of Care Principles 2014), and s 54-4 indicates that such principles may include accreditation standards for the quality of care and quality of life for the provision of residential care and home care respectively. Section 55-2 provides for User Rights Principles to be made, with the relevant minister making these principles pursuant to s 96-1 (currently the User Rights Principles 2014, made by the Assistant Minister for Social Services). Schedule 1 of the current User Rights Principles provides the Charter of Care Recipients' Rights and Responsibilities - Residential Care, and Schedule 2 provides the Charter of Recipients' Rights and Responsibilities - Home Care. These Quality of Care Principles and User Rights Principles will be considered further in the next section in the context of a broader discussion of the Aged Care Principles made under the Aged Care Act 1997 (Cth).
Division 63 of Part 4.3 of the Aged Care Act 1997 (Cth) relates to accountability, and outlines the responsibilities of approved providers in this regard. Specifically, in relation to the protection of elder Australians from abuse, this division of the Act requires approved providers to report allegations or suspicions based on reasonable grounds of “reportable assaults"7 in residential care settings to the police and to the department. This mandatory reporting provision is limited to physical assault and does not extend to such abuse of the elderly receiving care outside federally funded aged care facilities (s 63-1AA(2)). For a discussion of mandatory reporting obligations more generally, see section 3.4. General responsibilities of approved providers of residential care (s 56-1) and of approved providers of home care (s 56-2) are also enumerated. These provisions relate to compliance with rules; fees to be charged for both residential and home care services; management of refundable deposits, accommodation bonds and entry contributions for residential care; provision of security of tenure with respect to residential care; compliance with complaints resolution requirements (s 56-4); and the obligation on the provider “not to act in a way which is inconsistent with any rights and responsibilities of care recipients that are specified in the User Rights Principles" (s 56-1(m) and s 56-2(k)).
Part 4.4 of the Aged Care Act 1997 (Cth) outlines the consequences of non-compliance, with provisions relating to the nature and operation of sanctions. Section 65-1(a) provides that where an approved provider “has not complied, or is not complying, with one or more of its responsibilities under Part 4.1, 4.2 or 4.3", the secretary may impose a sanction if satisfied that it is appropriate to do so, and imposes this sanction in accordance with the procedures and requirements for imposing sanctions in Division 67. Section 67-1 in this division provides that unless the secretary is satisfied that the non-compliance gives rise to an immediate and severe risk to the safety, health or wellbeing of care recipients, sanctions must not be imposed unless the secretary has given the approved provider a notice of non-compliance, a notice of intention to impose sanctions or to remedy the non-compliance, and a notice of their decision regarding whether to impose sanctions. The sanctions that may be imposed include revocation, suspension or restriction of providers' approvals to provide aged care services; prohibition on charging or accrual of relevant fees or bonds; and such other sanctions enumerated in the Sanctions Principles.
Of particular note, s 53-2 provides that if an approved service provider fails to meet the responsibilities outlined in Chapter 4 of the Act (including under the User Rights Principles), such a failure does not give rise to an offence, and the failure has no consequence under any law other than the Aged Care Act unless the relevant act or omission “constitutes a breach of an obligation under another law". In her recent overview of applicable Australian law relevant to elder abuse, Lacey (2014) identified numerous shortfalls arising from this approach to sanctions, noting in particular that the Charters of Rights and Responsibilities (discussed further below) are not enforceable in their own right as there is no process within the legislation for individuals such as care recipients to seek remedies for breaches, save for the Aged Care Complaints Scheme (discussed below), with penalties relating to the implications for service providers' accreditation. In the event that elder abuse is identified, as captured by this Commonwealth framework, reliance on state and territory bodies (e.g., state and territory criminal justice systems) would nevertheless be required by way of implementation (Lacey, 2014).
As noted above, the Aged Care Act 1997 (Cth) also establishes the Aged Care Complaints Scheme (s 94A-1(1) and (2)) and the offices of the Aged Care Commissioner (Division 95A) and Aged Care Pricing Commissioner (Division 95B).
The Aged Care Complaints Scheme enables any person to report complaints about the quality of the care or service provided by an aged care service that is funded or subsidised by the Commonwealth. The scheme applies the Complaints Guidelines and they are resolved using a framework established in accordance with the Complaints Principles 2014. This involves consideration of whether the approved provider is meeting their responsibilities under all principles covered by the Aged Care Act 1997 (Cth), such as whether there has been a breach of any rights set out in the Charter of Care Recipients' Rights and Responsibilities - Residential Care and Home Care. The amended scheme has nevertheless been identified by some commentators as focusing on the resolution of complaints rather than the enforcement of the rights of care recipients (Barnett & Hayes, 2010; Lacey, 2014). The 2009 Walton review of the predecessor to the current complaints scheme had been critical of the scheme's lack of independence, being situated within the government department that administers aged care.8
The Aged Care Commissioner is a statutory appointment operating independently of the Accreditation Agency, the Aged Care Complaints Scheme and the department, with provisions made for the Commissioner to consider complaints about the operation of the Accreditation Agency or the Complaints Scheme, and more broadly to consider issues on their own initiative. The Commissioner's role includes examining the decisions of the Complaints Scheme, if necessary recommending that the scheme reconsider decisions, nominating matters to be included in the process, and developing measures to improve the complaint handling process. The Commissioner may also direct the Complaints Scheme to undertake a new complaints resolution process (see Part 6.6, Division 95A of the Aged Care Act 1997 (Cth)).
Section 63-2 of the Aged Care Act 1997 (Cth) requires the relevant minister to report to Parliament about the Aged Care Complaints Scheme, and the Aged Care Standards and Accreditation.
Commonwealth Aged Care Principles and other policies and best practice guidelines
Numerous Commonwealth Aged Care Principles guiding service provision have been made under s 96-1 of the Aged Care Act 1997 (Cth). Of these principles, the Quality of Care Principles, the Users Rights Principles and the Accountability Principles are of particular relevance. These Aged Care Principles, together with the Aged Care Determinations,9 are legislative instruments in accordance with the Legislative Instruments Act 2003 (Cth).
The Quality of Care Principles 2014 specify the Accreditation Standards (Schedule 2) and Home Care Common Standards (Schedule 4) to be met by residential care providers and home care providers respectively, as well as the care and services to be provided by these providers.
The User Rights Principles 2014 set out the responsibilities of approved providers in the provision of residential or home care services. These include describing the required content of agreements between approved providers and care recipients, and the information that approved providers are required to provide to care recipients, although notably, information about fee and charges were recently moved to the Fees and Payments Principles 2014 and the Aged Care (Transitional Provisions) Principles 2014. Importantly, Schedule 1 of the current User Rights Principles provides the Charter of Care Recipients' Rights and Responsibilities - Residential Care and Schedule 2 provides the Charter of Recipients' Rights and Responsibilities - Home Care. These charters are of particular relevance and are extracted in full in Box 1 and Box 2.
Box 1: Charter of Care Recipients' Rights and Responsibilities - Residential Care
Care recipients' rights - residential care
Each care recipient has the following rights:
(a) to full and effective use of his or her personal, civil, legal and consumer rights;
(b) to quality care appropriate to his or her needs;
(c) to full information about his or her own state of health and about available treatments;
(d) to be treated with dignity and respect, and to live without exploitation, abuse or neglect;
(e) to live without discrimination or victimisation, and without being obliged to feel grateful to those providing his or her care and accommodation;
(f) to personal privacy;
(g) to live in a safe, secure and homelike environment, and to move freely both within and outside the residential care service without undue restriction;
(h) to be treated and accepted as an individual, and to have his or her individual preferences taken into account and treated with respect;
(i) to continue his or her cultural and religious practices, and to keep the language of his or her choice, without discrimination;
(j) to select and maintain social and personal relationships with anyone else without fear, criticism or restriction;
(k) to freedom of speech;
(l) to maintain his or her personal independence;
(m) to accept personal responsibility for his or her own actions and choices, even though these may involve an element of risk, because the care recipient has the right to accept the risk and not to have the risk used as a ground for preventing or restricting his or her actions and choices;
(n) to maintain control over, and to continue making decisions about, the personal aspects of his or her daily life, financial affairs and possessions;
(o) to be involved in the activities, associations and friendships of his or her choice, both within and outside the residential care service;
(p) to have access to services and activities available generally in the community;
(q) to be consulted on, and to choose to have input into, decisions about the living arrangements of the residential care service;
(r) to have access to information about his or her rights, care, accommodation and any other information that relates to the care recipient personally;
(s) to complain and to take action to resolve disputes;
(t) to have access to advocates and other avenues of redress;
(u) to be free from reprisal, or a well-founded fear of reprisal, in any form for taking action to enforce his or her rights.
Source: User Rights Principles 2014, Schedule 1
Box 2: Charter of Care Recipients' Rights and Responsibilities - Home Care
Care recipients' rights - home care
General
(1) Each care recipient has the following rights:
(a) to be treated and accepted as an individual, and to have his or her individual preferences respected;
(b) to be treated with dignity, with his or her privacy respected;
(c) to receive care that is respectful of him or her, and his or her family and home;
(d) to receive care without being obliged to feel grateful to those providing the care;
(e) to full and effective use of all human, legal and consumer rights, including the right to freedom of speech regarding his or her care;
(f) to have access to advocates and other avenues of redress;
(g) to be treated without exploitation, abuse, discrimination, harassment or neglect.
Participation
(2) Each care recipient has the following rights:
(a) to be involved in identifying the home care most appropriate for his or her needs;
(b) to choose the care and services that best meet his or her assessed needs, from the home care able to be provided and within the limits of the resources available;
(c) to participate in making decisions that affect him or her;
(d) to have his or her representative participate in decisions relating to his or her care if he or she does not have capacity.
Care and services
(3) Each care recipient has the following rights:
(a) to receive reliable, coordinated, safe, quality care and services which are appropriate to his or her assessed needs;
(b) to be given before, or within 14 days after he or she commences receiving care, a written plan of the care and services that he or she expects to receive;
(c) to receive care and services as described in the plan that take account of his or her other care arrangements and cultural, linguistic and religious preferences;
(d) to ongoing review of the care and services he or she receives (both periodic and in response to changes in his or her personal circumstances), and modification of the care and services as required.
Personal information
(4) Each care recipient has the following rights:
(a) to privacy and confidentiality of his or her personal information;
(b) to access his or her personal information.
Communication
(5) Each care recipient has the following rights:
(a) to be helped to understand any information he or she is given;
(b) to be given a copy of this Charter;
(c) to be offered a written agreement that includes all agreed matters;
(d) to choose a person to speak on his or her behalf for any purpose.
Comments and complaints
(6) Each care recipient has the following rights:
(a) to be given information on how to make comments and complaints about the care and services he or she receives;
(b) to complain about the care and services he or she receives, without fear of losing the care or being disadvantaged in any other way;
(c) to have complaints investigated fairly and confidentially, and to have appropriate steps taken to resolve issues of concern.
Fees
(7) Each care recipient has the following rights:
(a) to have his or her fees determined in a way that is transparent, accessible and fair;
(b) to receive invoices that are clear and in a format that is understandable;
(c) to have his or her fees reviewed periodically and on request when there are changes to his or her financial circumstances;
(d) not to be denied care and services because of his or her inability to pay a fee for reasons beyond his or her control.
Source: User Rights Principles 2014, Schedule 2
While the charters are laudable in their content, the Aged Care Act 1997 (Cth) has been described as “primarily intended to operate as a regulatory framework for the accreditation and monitoring of residential aged care facilities" (Lacey, 2014, p. 126). The relegation of the Charter of Rights to schedules rather than being in the body of the Aged Care Act 1997 (Cth) is emblematic of the “lack of priority given to those rights under the legislative framework" (Lacey, 2014, p. 125).
The Accountability Principles 2014 make provision for access to residential aged care facilities by the aged care certification assessors, the Aged Care Commissioner and the Australian Aged Care Quality Agency established by the Australian Aged Care Quality Agency Act 2013 (Cth). These principles also outline requirements in relation to police certificates prepared by the Australian Federal Police, CrimTrac or the police force or police service of a state or territory, for staff and volunteers, as well as the provision of information (including financial reports and information relating to service provision) by approved providers to the relevant secretary or minister. Notably, Part 7 of these principles outlines the circumstances in which the requirement to report allegations or suspicions of reportable assaults (described above) does not apply.
Other Aged Care Principles include the Approved Provider Principles 2014, which enumerate the matters that the secretary is required to consider when determining whether an applicant is suitable to provide aged care; the Allocation Principles 2014, which deal with the process for allocating aged care places to approved providers; the Approval of Care Recipients Principles 2014, which deal with the eligibility requirements for care recipients; and the Sanctions Principles 2014, which relate to the administration of sanctions.
The Commonwealth Government has also established and published an extensive array of policies and guidelines to facilitate best practice in the provision of aged care services.10 These include:
- guidelines about aged care assessments (e.g., Aged Care Assessment Programme Guidelines);
- best practice guides and user guides relating to fees and funding (e.g., Best Practice Guide to the Publication of Accommodation Prices);
- program, policy and law guides (e.g., the Home Care Standards Guide, the National Aged Care Advocacy Program Policy Guide and the Community Visitors Scheme Policy Guide 2013-2016); and
- quality and compliance statements and guides (e.g., the Compulsory Reporting Guidelines for Approved Providers of Residential Care, the Better Practice Guide to Complaint Handling in Aged Care Services, the Guidelines for the Aged Care Complaints Scheme, and the Guide to Aged Care Law).
In response to the current Commonwealth position, suggestions for reform have ranged from calls for the introduction of comprehensive adult protection legislation (e.g., Lacey, 2014; Office of the Public Advocate [OPA], & University of South Australia, 2011) to proposals for the reform of guardianship and related laws (e.g., Australian Law Reform Commission, 2014; Chesterman, 2013; Victorian Law Reform Commission, 2012), each of which will be discussed below.
International human rights treaties and the external affairs power
While important Commonwealth legislative measures have been outlined in the discussion in this chapter so far, these measures discussed are limited to elderly Australians accessing Commonwealth-funded services and do not enable comprehensive national legislation protecting against elder abuse. As noted earlier, the external affairs power in s 51(xxix) of the Constitution provides a potential basis for the enactment of a national framework for the protection of Australians against elder abuse.
International human rights laws that have been ratified by Australia to date - including, for example, the International Covenant on Civil and Political Rights, and the International Covenant on Economic, Social and Cultural Rights - do extend to the protection of elder persons against abuse and neglect,11 and implied rights for the protection of the elderly have also been identified in seminal treaties, including the right to live free from abuse, exploitation and neglect. For example, the Universal Declaration of Human Rights 1947 enshrines a specific right to security for the elderly (Article 25(1)), but also, more generally, provides that all people are “born free and equal in dignity and rights".
Other relevant documents endorsed by Australia include non-binding international instruments such as the United Nations Principles for Older Persons, which specifies 18 rights covering the independence, participation, care, self-fulfilment and dignity of elderly people.12 Nevertheless, specific reference in treaties to the protection of the rights of the elderly has been uncommon to date, and concerns have been raised in relation to the “patchy and aspirational nature" of the relevant international human rights treaties and instruments (Lacey, 2014, pp. 103, 104 & 114).13
An international convention on the rights of older persons (currently under consideration by the UN General Assembly Open-ended Working Group on Ageing, 2015), if ratified, may provide broader scope to frame a national approach to protect against elder abuse, although practical if not legal implementation would necessarily involve cooperation with the state and territory governments (Lacey, 2014, pp. 103 & 122).
At a policy level, the international human rights instruments, together with the Age Discrimination Act 2004 (Cth), and the Office of the Age Discrimination Commissioner at the Australian Human Rights Commission, also serve to raise greater awareness of “the human rights implications of elder abuse, and to encourage the use of rights as the basis for all corrective policies and programs" (Ryan, 2015).
6.2 State/territory-based frameworks
At present, the states and territories have, to varying degrees, provided for the prevention of elder abuse through varying policies, practice guidelines, legislative frameworks, and different levels of coordinated interagency approaches (Lacey, 2014, pp. 102-103). The discussion in this section will focus on power-of-attorney and guardianship laws, following a discussion of examples of state/territory-based policy and practice guidelines, and concluding with a brief discussion of examples of state-based justice systems.
Health and aged care policy frameworks and practice guidelines
At present there exist a range of state/territory-based elder abuse response strategies, policies and practice guidelines that generally outline the various forms of elder abuse, how it can be identified, the action to be taken when elder abuse is suspected or identified, and the relevant services that can be approached for assistance. These policy frameworks and practice guidelines are detailed in Table 1.
| State/territory | Organisation/department | Policies and guidelines |
|---|---|---|
Source: Chesterman, (2015a), p. 2 | ||
| Victoria | Department of Health and Human Services | Elder Abuse Prevention and Response Guidelines for Action 2012-14 (2012); and With Respect to Age Practice Guidelines (2009) |
| South Australia | SA Health | Strategy for the Safeguarding of Older South Australians Action Plan 2014-21 (2015) |
| New South Wales | Department of Ageing, Disability and Home Care | Interagency Protocol for Responding to the Abuse of Older People (2007) |
| Tasmanian | Department of Health and Human Services | Responding to Elder Abuse: Tasmanian Government Practice Guidelines for Government and Non-Government Employees (2012) |
| ACT | ACT Government | ACT Elder Abuse Prevention Program Policy (2012) |
| Western Australia | Alliance for the Prevention of Elder Abuse | Elder Abuse Protocol: Guidelines for Action (2013) |
| Queensland | - | Strategy not publicly available, but note Elder Abuse website and Elder Abuse Prevention Unit (UnitingCare) |
| NT | - | - |
These policy frameworks and practice guidelines vary in scope and detail, with some, such as Victoria's Elder Abuse Prevention and Response Guidelines for Action identified as a “high level guideline document aimed at encouraging sector collaboration and coordination", in contrast with the detailed protocols and practice guidelines released by New South Wales and Tasmania (Chesterman, 2015a, p. 2). Victoria had, however, previously established detailed practice guidelines described in With Respect to Age (2009), which provides guidance for health services and community agencies for the prevention of elder abuse with both “multi-sector and multi-discipline application".14
Despite the variability, key common limitations have been identified, including an emphasis on the vulnerability of victims of elder abuse, with responses where there is significant impairment involving the appointment of a substitute decision maker via a guardianship application across the various jurisdictions (e.g., Tasmania, New South Wales, Western Australia) (Chesterman, 2015a, pp. 3-4). A lack of emphasis on service improvement, the development of expertise, and facilitating collaborative practices have also been identified (Chesterman, 2015a, pp. 4-5). A lack of clarity around the relevant primary point of contact in cases of elder abuse has also emerged as a shortcoming, although the complexities associated with this were acknowledged in the New South Wales, South Australian and Tasmanian strategies, with varying agencies nominated to address particular issues (Chesterman, 2015a, p. 6). Notably, Chesterman argued that state/territory government policies and guidelines should be improved to provide greater priority to the views and best interests of the relevant person, and to identify lead agencies to be empowered to facilitate collaborative responses.
State/territory legislative frameworks
Each state and territory has its own laws in relation to powers of attorney and guardianship. By way of illustration, the discussion in this section will focus on provisions in Victoria, with a brief discussion of legislative arrangements in some other states and territories.
Following an Inquiry into Powers of Attorney by the Victorian Parliamentary Law Reform Committee, reforms were introduced in Victoria, which implemented many of the committee's recommendations. On 1 September 2015, the Powers of Attorney Act 2014 (Vic.) came into operation and introduced various elements aimed at preventing the misuse of enduring powers of attorney. These changes included:
- the simplification and consolidation of Victoria's power-of-attorney laws, such that the legislative provisions for enduring powers of attorney and enduring powers of guardianship were consolidated into a single enduring power of attorney, with powers for financial and/or personal affairs;15
- improvements in the legislative protections against abuse of enduring powers of attorney, including:
- the introduction of indictable offences of dishonestly obtaining or dishonestly using an enduring power of attorney, with penalties of up to five years' imprisonment (s 135 and s 137);
- setting out more clearly the duties of enduring attorneys in the legislation and including the duty to act honestly, diligently and in good faith, and to exercise reasonable skill and care (s 63-s 70);
- the introduction of a new definition of decision-making capacity and guidance about how to assess decision-making capacity, with s 4(2) clearly stating that a person is presumed to have decision-making capacity unless there is evidence to the contrary;
- the inclusion of principles to better guide decision-making, including that decisions are to be made in a manner that is least restrictive, with the attorney to ensure that the principal is provided with “practicable and appropriate support" to enable their participation in decisions affecting them to the extent possible, and with the attorney required to give effect to the principal's wishes, encourage participation in decision making and promote the principal's social and personal wellbeing (s 21);
- the extension of the power of the Victorian Civil and Administrative Tribunal (VCAT), including to order compensation (s 71-s 72; s 77-s 80);
- the introduction of new provisions prohibiting conflict-of-interest transactions, unless authorised or ratified by the principal or VCAT (s 64-s 65), and provisions regulating an enduring power of attorney's ability to give gifts from the principal's property (s 67);
- the introduction of more stringent execution requirements for the making or revocation of enduring powers of attorney (s 23; s 32-s 36; s 44-s 50); and
- a new amendment to create the role of supportive attorney, which enables (Part 7 of the Act):
- a principal to appoint a person to support them in making and giving effect to certain or all of their own decisions, while still retaining their own decision-making authority (the first provision for a supportive attorney in Australia); and
- the supportive attorney to be authorised to communicate or assist the principal to communicate supported decisions, and to do such things as are required to give effect to supported decisions (other than decisions regarding significant financial transactions), but may not make decisions on behalf of the principal.
The Victorian Guardianship and Administration Act 1986 (Vic.), was introduced to provide for substitute decision making where people with disabilities are unable to make legal and financial decisions (administrator), or personal decisions such as those relating to medicine and housing (guardian). The Victorian Office of the Public Advocate (OPA) is Victoria's “adult guardian of last resort", with statutory duties to “protect and promote the rights of people with disabilities" (Chesterman, 2015b, p. 1). Public advocates or adult guardians may be appointed as guardians or substitute decision makers where the principal lacks capacity, or appointed to investigate complaints or allegations relating to the abuse, neglect or exploitation of a principal by an attorney, guardian or administrator. The Victorian OPA undertakes a variety of tasks pursuant to the Guardianship and Administration Act 1986 (Vic.), including to investigate “complaint(s) or allegation(s) that a person is under inappropriate guardianship, or is being exploited or abused or in need of guardianship". The OPA hosts five volunteer programs and also plays an important educative role in relation to powers of attorney (Chesterman, 2015b, pp. 1-2), providing access to relevant publications and hosting the new online forms introduced by the legislative amendments. Other important legislation and agencies in Victoria include the Disability Act 2006 (Vic.) and the Disability Services Commissioner, the Ombudsman Act 1973 (Vic.) and the Victorian Ombudsman. The Chief Psychiatrist and the Health Services Commissioner may also play an investigatory role in the Victorian context, and the Aged Care Assessment Service and Department of Health and Human Services Intake and Response service may also identify elder abuse when investigating a person's eligibility to access services, although this is not their primary role (Chesterman, 2013, p. 23).
Some aspects of the Victorian approach to guardianship legislation have been reflected across other states and territories, and each now have guardians of last resort in the form of OPAs in South Australia, ACT, Western Australia; Public Guardians in New South Wales and Tasmania; and an Adult Guardian in Queensland. The investigative powers of these OPAs do, however, vary (Chesterman, 2013, p. 72) and variations in guardianship practices have given rise to calls for greater involvement by the Commonwealth in state and territory guardianship systems, including calls for the development of national guardianship principles (Chesterman, 2013, p. 35). In Queensland, the Communities, Disability Services and Domestic and Family Violence Prevention Committee inquiring into the adequacy of existing financial protections for Queensland's seniors recommended the adoption of strategies to regulate and record the appointment of attorneys, to amend the Powers of Attorney Act 1998 (Qld) to require attorneys to demonstrate knowledge of attorneys' duties and responsibilities prior to their appointment, and to amend the Public Trustee Act 1978 (Qld) to enable the Public Trustee to investigate and prosecute attorneys where there is evidence of financial abuse (Communities, Disability Services and Domestic and Family Violence Prevention Committee, 2015, p. 147). Also of note in relation to powers of attorney, the Advance Care Directives Act 2013 (SA) was amended to enable South Australians, from 1 July 2014, to better protect their interests by appointing a substitute decision maker.
Potential responses to instances of elder abuse via the legal system more generally may involve criminal proceedings for fraud pursuant to state or territory criminal law (see directly below), or the pursuit of remedies through civil law (e.g., contracts or torts) or in equity, including claims for breach of fiduciary duty, unconscionable conduct or undue influence. However, civil law or equity may not capture relevant aspects of elder abuse, such action may be expensive and time consuming to pursue, and it may require the appointment of a litigation guardian, which for financial and other reasons may limit access to legal remedies for elderly victims of abuse (OPA (Qld) & Queensland Law Society, 2010). In some jurisdictions there may also be restrictions in relation to the damages that may be sought (OPA (Qld) & Queensland Law Society, 2010). Indeed, Wainer, Darzins and Owada (2010) observed that the legal system is rarely invoked by the elderly in response to abuse.
Criminal justice system
Various forms of elder abuse, including physical violence and financial abuse, may constitute crimes under state and territory law, and include offences such as assault, theft and obtaining property by deception. However, these criminal offences can be difficult to identify because they are often perpetrated in the context of relationships where the opportunity exists for coercion and where evidence of wrongdoing may be weak, even in circumstances where victims feel able to initiate or facilitate police investigations in the context of a relationship of dependence (Chesterman, 2015a; OPA (Qld) & Queensland Law Society, 2010). Also, the primary goal of the criminal justice system is the prosecution of the perpetrator rather than the facilitation of a remedy for the victim, although crimes compensation may be available. In relation to financial abuse more specifically, the criminal justice system's response to the perpetration of fraud, and in particular online fraud, is an issue commanding increased attention at present. The Communities, Disability Services and Domestic and Family Violence Prevention Committee, in their report from their inquiry into the adequacy of existing financial protections for Queensland's seniors, identified the potential failure to identify this financial exploitation as a crime. They nominated feelings of shame and embarrassment as factors contributing to high levels of underreporting, with federal and state-based police services able to offer only limited assistance where the fraud is undertaken by an overseas-based offender, due to investigatory and enforcement challenges. Training of police and consumer protection agencies was also a measure identified as enabling “empathetic and appropriate service responses" (Communities, Disability Services and Domestic and Family Violence Prevention Committee, 2015, pp. 101, 103).
Laws relating to family violence also offer potential protection for vulnerable elderly people. For example, s 5 of the Family Violence Protection Act 2008 (Vic.) provides an expansive definition of family violence, including economic abuse (Box 3). Section 8 of the Act provides that a family member for the purposes of this Act includes spouses, domestic partners, persons in intimate personal relationships, and relatives, but may also include persons “regarded as being like a family member if it is or was reasonable to regard the other person as being like a family member having regard to the circumstances of the relationship" (Box 3). Section 8(3) references a broad range of circumstances to consider when assessing family relationships, and also provides the example where a person with a disability and their carer “may over time have come to approximate the type of relationship that would exist between family members". There are provisions made for family violence safety notices (ss 24-39) and family violence intervention orders (Part 4), both of which may include conditions for exclusion from the residence (s 81 and s 82). Relevant legislation in other states and territories include the Domestic and Family Violence Protection Act 2012 (Qld); Crimes (Domestic and Personal Violence) Act 2007 (NSW); Intervention Orders (Prevention of Abuse) Act 2009 (SA); Restraining Orders Act 1997 (WA); Family Violence Act 2004 (Tas); Domestic Violence and Protection Orders Act 2008 (ACT) and Domestic and Family Violence Act 2007 (NT).
Box 3: Family Violence Protection Act 2008 (Vic.)
Section 5
Meaning of family violence
(1) For the purposes of this Act, family violence is -
(a) behaviour by a person towards a family member of that person if that behaviour -
(i) is physically or sexually abusive; or
(ii) is emotionally or psychologically abusive; or
(iii) is economically abusive; or
(iv) is threatening; or
(v) is coercive; or
(vi) in any other way controls or dominates the family member and causes that family member to feel fear for the safety or wellbeing of that family member or another person; or
(b) behaviour by a person that causes a child to hear or witness, or otherwise be exposed to the effects of, behaviour referred to in paragraph (a).
Examples
The following behaviour may constitute a child hearing, witnessing or otherwise being exposed to the effects of behaviour referred to in paragraph (a) -
- overhearing threats of physical abuse by one family member towards another family member;
- seeing or hearing an assault of a family member by another family member;
- comforting or providing assistance to a family member who has been physically abused by another family member;
- cleaning up a site after a family member has intentionally damaged another family member's property;
- being present when police officers attend an incident involving physical abuse of a family member by another family member.
(2) Without limiting subsection (1), “family violence" includes the following behaviour -
(a) assaulting or causing personal injury to a family member or threatening to do so;
(b) sexually assaulting a family member or engaging in another form of sexually coercive behaviour or threatening to engage in such behaviour;
(c) intentionally damaging a family member's property, or threatening to do so;
(d) unlawfully depriving a family member of the family member's liberty, or threatening to do so;
(e) causing or threatening to cause the death of, or injury to, an animal, whether or not the animal belongs to the family member to whom the behaviour is directed so as to control, dominate or coerce the family member.
(3) To remove doubt, it is declared that behaviour may constitute family violence even if the behaviour would not constitute a criminal offence.
Section 8
Meaning of family member
(1) For the purposes of this Act, a “family member", in relation to a person (a “relevant person"), means -
(a) a person who is, or has been, the relevant person's spouse or domestic partner; or
(b) a person who has, or has had, an intimate personal relationship with the relevant person; or
(c) a person who is, or has been, a relative of the relevant person; or
(d) a child who normally or regularly resides with the relevant person or has previously resided with the relevant person on a normal or regular basis; or
(e) a child of a person who has, or has had, an intimate personal relationship with the relevant person.
(2) For the purposes of subsections (1)(b) and (1)(e), a relationship may be an intimate personal relationship whether or not it is sexual in nature.
(3) For the purposes of this Act, a “family member" of a person (the “relevant person") also includes any other person whom the relevant person regards or regarded as being like a family member if it is or was reasonable to regard the other person as being like a family member having regard to the circumstances of the relationship, including the following -
(a) the nature of the social and emotional ties between the relevant person and the other person;
(b) whether the relevant person and the other person live together or relate together in a home environment;
(c) the reputation of the relationship as being like family in the relevant person's and the other person's community;
(d) the cultural recognition of the relationship as being like family in the relevant person's or other person's community;
(e) the duration of the relationship between the relevant person and the other person and the frequency of contact;
(f) any financial dependence or interdependence between the relevant person or other person;
(g) any other form of dependence or interdependence between the relevant person and the other person;
(h) the provision of any responsibility or care, whether paid or unpaid, between the relevant person and the other person;
(i) the provision of sustenance or support between the relevant person and the other person.
Example
A relationship between a person with a disability and the person's carer may over time have come to approximate the type of relationship that would exist between family members.
(4) For the purposes of subsection (3), in deciding whether a person is a family member of a relevant person the relationship between the persons must be considered in its entirety.
6.3 Financial systems: Measures encouraging financial literacy and protecting against financial abuse
Measures encouraging financial literacy
The Australian Securities and Investments Commission (ASIC) regulates financial advice and financial products and has national responsibility for coordinating financial literacy among Australians. To this end, ASIC's (2014) National Financial Literacy Strategy (currently 2014-17) identifies the importance of improving financial literacy and financial wellbeing via informed financial decision-making, including those financial decisions that are made at retirement and in old age.
The National Financial Literacy Strategy highlights programs that are aimed at building financial literacy, and nominates Australians aged 65 years and over as a key target audience, with this group identified as being “least likely to consult a range of information sources to stay informed" and as having “gaps in their knowledge and engagement and declining cognitive skills" (ASIC, 2014, p. 23; ASIC, 2015, p. 7). This vulnerability is reflected in recent research, such as Earl, Gerrans, Asher and Woodside's (2015) quantitative and qualitative study of the relationship between financial literacy, financial judgement and retirement self-efficacy, which identified a link between cognitive functioning and financial judgement. Participants in their study had relatively high levels of financial literacy, scoring well on general mental ability and lower on self-rated symptoms of dementia.
Of particular relevance to the improvement of financial literacy among older people is ASIC's MoneySmart program, which provides free and impartial literacy tools and resources, including guidance in relation to seeking financial advice, and accessible information to assist with financial decision making, such as retirement planning and budgeting (ASIC, 2015, p. 9). MoneySmart provides access to online calculators, including a budget planner, a superannuation and pension age calculator, an account-based pension calculator, a reverse mortgage calculator and a retirement planner (ASIC, 2015, p. 9). MoneySmart also provides access to a wide range of online content, such as information about choosing a financial advisor, together with access to a suite of MoneySmart publications. For example, Financial Decisions at Retirement: How to Make the Most of Your Money and Avoid Costly Mistakes, is a MoneySmart publication that provides guidance about the funds required for retirement, available entitlements, information about withdrawing superannuation, and options dealing with these funds and income stream choices, as well as alerts to potential risks associated with investment decisions. ASIC also consults regularly and widely with government, community and not-for-profit agencies to facilitate access to their educative and guidance materials (ASIC, 2015, p. 13). The National Information Centre on Retirement Investments is also able to provide older Australians with general financial advice, and Centrelink's Financial Information Service provides information about the receipt of pensions and benefits, and the effects on such payments of the receipt of income or the gifting of financial assistance.
In relation to financial literacy, the Queensland Disability Services and Domestic and Family Violence Prevention Committee's (2015) report recommended that the Queensland Government investigate the establishment of a dedicated, 24-hour financial advice helpline, reinstate funding for financial counselling, and “investigate ways to better facilitate vulnerable seniors' access to, and uptake of, free and independent financial advice" (p. 90). It recommended that the Queensland and Commonwealth governments work together to explore options to reduce complexity in aged care contracts and to educate consumers about reasonable charges for aged care services (p. 90).
While important, “financial literacy is not a panacea" (ASIC, 2015, p. 14). ASIC has emphasised that a strong, regulatory framework - including legislative mechanisms such as the Future of Financial Advice reform package,16 the national regulatory regime for consumer credit,17 and dispute resolution mechanisms for clients dealing with financial institutions, as well as non-legislative codes of conduct - is required to protect against financial abuse. Measures specifically relevant to the prevention of financial abuse of the elderly are considered directly below.
Measures protecting against financial abuse of the elderly
As discussed earlier, financial abuse takes many and varied forms. It may include exerting pressure to transfer funds or other assets, taking out or guaranteeing loans to the benefit of others, or not acting in the best interests of the relevant elderly persons when authorised to manage funds or other assets on their behalf.
Information and advocacy services available in each state and territory aim to educate elderly people about the varied forms of financial abuse and the steps that can be taken to protect against such abuse. For example, groups such as Seniors Rights Victoria and the Elder Abuse Prevention Unit, Queensland (see below) provide relevant legal, education and advocacy services. Information to support awareness about scams relating to investments, superannuation, banking, credit, lotteries or dating, and identity theft is provided by groups such as the ASIC Scamwatch information centre, and are an important means of protecting elderly Australians against such scams.
The financial institution sector in Australia also provides information about the nature of financial abuse and means of protection against such abuse, together with industry guidelines facilitating financial institutions to both prevent and identify financial abuse among their clients. For example, the Australian Bankers Association (ABA)18 has developed the following tools to facilitate both the prevention and identification of elder abuse in the financial institution context:
- Protecting Vulnerable Customers From Potential Financial Abuse - guidelines for the banking industry, outlining the indicators of financial abuse and how it may “impact customers and banks' relationships with their customers", together with a framework to enable banks to “raise awareness and promote consistent arrangements to deal with suspected cases of financial abuse" (ABA, 2014a, p. 1).
- Protecting Yourself From Financial Abuse - a consumer fact sheet to raise awareness about the nature and consequences of financial abuse and measures that can be taken to protect against such abuse (ABA, 2014b).
- Responding to Requests From a Power of Attorney or Court-Appointed Administrator - a guideline to industry outlining “how powers of attorney and court-appointed administrators arrangements apply to banks' relationships with their customers" and providing a framework that banks can use to consistently deal with requests from attorneys and administrators (ABA, 2014c, p. 1)
- Setting up a Power of Attorney to Help Manage Your Banking Needs - a consumer fact sheet providing information about powers of attorneys and the circumstances in which it may be appropriate to appoint one to manage financial and legal issues (ABA, 2014d).
While the above industry guidelines are voluntary, they were “developed with input from, and agreed to by, member banks" and the ABA encourages member banks to adhere to them and to incorporate them into their internal policies, processes and procedures (ABA, email communication, 30 November 2015).
In addition, Capacity Australia (a not-for-profit charity), with the support of the ABA, has devised an online education and assessment tool that bank staff can use to identify financial abuse or the risk of financial abuse, and respond appropriately (ABA, email communication, 30 November 2015). This online tool was introduced following its trial with the Commonwealth Bank of Australia and the National Australia Bank. Financial institutions also provide regular staff training, with an emphasis on escalating customer issues and concerns to those with appropriate authority, including hardship teams who are likely to have received specialist training with regard to the identification of financial abuse and implementing appropriate measures to raise concerns with clients (ABA, email communication, 30 November 2015). The Cognitive Decline Partnership Centre recently published a report recommending thorough training and ongoing education for senior managers through to frontline staff about cognitive decline, and how to deal with clients with dementia, their attorneys and agents (Field, Matkovic, & Bhatia, 2015, p. 6).
From the perspective of financial institutions, formal arrangements are preferred as they provide clear instructions to the relevant bank and are directed at eliminating the client's exposure to financial risk (ABA, email communication, 30 November 2015). When managing and responding to instances, or potential instances, of financial abuse, institutions are required to be particularly mindful not to breach their obligations pursuant to privacy laws, to respect the autonomy of their clients, and not to discriminate against clients based on their age or disability (ABA, email communication, 30 November 2015). These considerations can be difficult to balance where there are concerns, for example, about the exertion of undue influence, as the bank must act on their clients' instructions and “must assume that a customer can transact until a point to which the law, and medical profession, say this is not the case" (ABA, email communication, 30 November 2015). Complexities may also arise where the suspected or actual financial abuse is perpetrated by someone who has the legal authority to make decisions on behalf of the elderly client, particularly given the importance of not undermining the trust that an elderly client has in an agent who is “acting in good faith and in their best interests" (ABA, email communication, 30 November 2015) and to this end, measures to facilitate supported decision-making rather than substituted decision-making may be preferred. These measures include two-to-sign, co-signatory and linked accounts, clients obtaining independent legal advice prior to applying for various lending products (ABA, email communication, 30 November 2015). Field et al. (2015) also recommended that financial institutions require clients to produce valid enduring powers of attorney when authorising third party signatories or co-signatories, as well as tighter online banking restrictions for attorneys accessing their principals' accounts (pp. 6-7).
Where substituted decision-making arrangements are in place, financial institutions generally require these arrangements to be noted on the client's file and the institution's database, and the relevant instruments are usually required to be registered where property transactions are taking place (ABA, email communication, 30 November 2015). The ABA and Field et al. (2015) indicated that uniform national legislation regarding attorneys, agents and administrators, and a national register of relevant instruments would “reduce regulatory and administrative complexity", with varying state and territory laws at present giving rise to confusion and delay, which in turn may expose elderly clients to financial abuse if appropriate safeguards are not in place, or to financial loss if arrangements are not established in a timely manner (ABA, email communication, 30 November 2015; see also Field et al., 2015, p. 5-6).
Collaborative approaches are also recommended, with the Queensland Disability Services and Domestic and Family Violence Prevention Committee (2015), for example, recommending that the state government continue to work together with the Commonwealth Government and enforcement agencies to “promote responsible lending and other ethical business practices to better safeguard the interests and assets of vulnerable seniors", to develop more formal protocols for financial institutions with regard to elder abuse, including options for financial reporting, and to create options to improve remedies and compensation for victims of financial elder abuse (pp. 114, 172, 156).
6.4 Non-government service provision and advocacy
Independent and confidential advocacy services are available free of charge to care recipients in each state and territory. These advocates may provide information about care recipients' rights and responsibilities, listen to their concerns, assist in the resolution of issues or complaints raised in relation to aged care service providers, liaise directly with these service providers and may also refer care recipients to other relevant agencies where appropriate (Department of Social Services, 2015).19 A 1800 National Aged Care Advocacy helpline is also available in addition to the state/territory-based advocacy services.
Other consumer groups and community organisations, such as COTA and National Seniors Australia, as well as informal alliances are essential to effective aged care advocacy and for monitoring the implementation and review of aged care service provision. At a state and territory level, a broad range of services have been established. For example, since 2008, Seniors Rights Victoria has been funded by the Victorian Government to provide information, legal and other advice, and short-term support and advocacy, as well as referrals for those experiencing elder abuse in Victoria. Its services include a free and confidential helpline and an online e-learning portal for professionals, and extend to performing educative and policy and law reform roles. For example, its online Elder Abuse Tool Kit provides guidance about facilitating older people to make their own decisions, how to work respectfully with older people, and how to enable them to receive the services that they need, including working respectfully with older gay, lesbian, bisexual, transgender and intersex people. Similar agencies in other states and territories specialise in providing information and advocacy services aimed at preventing elder abuse. These include the Queensland Seniors Legal and Support Service and the Queensland Elder Abuse Prevention Unit, the Aged Rights Advocacy Service in South Australia, Advocare in Western Australia, Tasmanian Elder Abuse Helpline and Advocacy Tasmania, Aged and Disability Rights Team, Darwin Community Legal Centre, the Older Persons Abuse Prevention Referral and Information Line and the New South Wales Aged Rights Service and the New South Wales Elder Abuse Helpline and Older Person's Legal Service.
In addition to the Centrelink Financial Information Service (noted at 6.3) provided through the Department of Human Services, advisory services in relation to social security entitlements for seniors are also available in each state and territory, including Social Security Rights Victoria, Adelaide Welfare Rights Centre, Welfare Rights Centre Sydney, Welfare Rights Centre Brisbane, Welfare Rights and Advocacy Service Western Australia, Social Security and Tenant's Advice Line, Welfare Rights and Legal Centre ACT, and the Darwin and Hobart Community Legal Services.
The discussion in this section has identified the legal complexities associated with current measures for the protection of elder Australians against abuse. Commentators (including Barnett & Hayes, 2010; Chesterman, 2015a; Field et al., 2015; Lacey 2014), have identified shortcomings associated with legal avenues and policy responses as well as current levels of coordinated interagency approaches. Calls for the introduction of a comprehensive, national approach to elder abuse and for leadership to be shown in this area have been made (Chesterman, 2015a). More specifically, Chesterman has suggested that the best way to promote leadership in this sector would be through the introduction of standalone elder abuse prevention and response units to be established within key state/territory departments (Chesterman, 2015a, p. 7).
4 Anti-discrimination legislation [in the Commonwealth jurisdiction the Age Discrimination Act 2004 (Cth)] may be identified as providing some protection against discrimination on the basis of age, whereby the Australian Human Rights Commission may investigate complaints and attempt conciliation. However, limitations associated with the definition of human rights and enforcement have been identified in relation to this avenue, with the underuse of this legislation in part linked to the restrictive definitions (Barnett & Hayes, 2010, p. 73-74).
5 As of 1 July 2015, the Home and Community Care Programme, the National Respite for Carers Programme, Day Therapy Centres and the Assistance with Care and Housing for the Aged, together became known as the Commonwealth Home Support Programme. See the program website at: <www.myagedcare.gov.au/aged-care-services/commonwealth-home-support-programme> for more information.
6 In May and August 2013, the Victorian and Western Australian Governments each agreed to transfer responsibility (Victoria) or to commence negotiations to transfer responsibility (Western Australia) for the provision of these services to the Commonwealth.
7 Section 63-1AA(9) of the Aged Care Act 1997 (Cth) defines a reportable assault as “unlawful sexual contact, unreasonable use of force, or assault specified in the Accountability Principles (currently the Accountability Principles 2014) and constituting an offence against a law of the Commonwealth or a State or Territory, that is inflicted on a person when: (a) the person is receiving residential care in respect of which the provider is approved; and (b) either (i) subsidy is payable for provision of the care to the person; or (ii) the person is approved under Part 2.3 as the recipient of that type of residential care".
8 See the Department of Social Services web pages: Aged Care Complaints Scheme <agedcarecomplaints/govspace.gov.au/about-us/about-the-scheme/#.VjAuDenF85Q>; Commonwealth Home Support Programme <www.myagedcare.gov.au/aged-care-services/commonwealth-home-support-programme>; and Commonwealth guides, advice and policies <www.dss.gov.au/our-responsibilities/ageing-and-aged-care/publications-articles/guides-advice-policy>.
9 The Aged Care Determinations primarily relate to the calculation of subsidies and supplements.
10 See the list of Commonwealth guides, advice and policies at: <www.dss.gov.au/our-responsibilities/ageing-and-aged-care/publications-articles/guides-advice-policy>.
11 Note also the Universal Declaration of Human Rights, the Convention on the Elimination of All Forms of Discrimination Against Women, the Convention on the Rights of Persons With Disabilities, and the Convention Against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment.
12 Lacey (2014) noted, though, that the aspirational nature of the 1991 United Nations Principles for Older Persons does not enshrine legally enforceable rights to the benefit of the elderly (p. 115). These 18 principles were adopted by General Assembly resolution 46/91 of 16 December 1991.
13 Lacey (2014) noted the examples of the Office of the High Commission for Human Rights (2012) Normative Standards in International Human Rights Law in Relation to Older Persons: Analytical Outcome Paper, the Migrant Workers Convention, and the Convention on the Rights of Persons with Disabilities, which refers specifically to age.
14 See the Preventing Elder Abuse web page: <www2.health.vic.gov.au/ageing-and-aged-care/wellbeing-and-participation/preventing-elder-abuse>.
15 Note that enduring powers of attorney and guardianship made prior to 1 September 2015 remain valid.
16 Corporations Amendment (Future of Financial Advice) Act 2012 (Cth) and the Corporations Amendment (Further Future of Financial Advice Measures) Act 2012 (Cth).
17 National Consumer Credit Protection Act 2009 (Cth).
18 The ABA provides advice, analysis and advocacy for the banking industry.
19 See <www.myagedcare.gov.au/how-make-complaint/advocacy-services> for details of the advocacy services in each state and territory.
7. Prevention approaches
As noted in section 3.2, directions in the themes underpinning thinking about prevention have two broad elements, with the first oriented toward changing the values and attitudes among the broader community and among professionals and individuals who interact with elders, and the second oriented toward mitigating the risk factors for elder abuse.
Many of the provisions of the Aged Care Act 1987 (Cth) outlined in section 6.1 are directed at identifying and preventing elder abuse in the aged care context by facilitating the oversight of the quality of aged care. Relevant measures include the Aged Care Principles (e.g., the Quality of Care Principles, the Accountability Principles and the User Rights Principles and Charter of Care Recipients Rights), as well as the establishment of a regulatory system comprising accreditation and aged care standards, non-compliance provisions and the establishment of a more robust Aged Care Complaints Scheme and an Independent Aged Care Commissioner. Broader Commonwealth- and state/territory-based policy frameworks and practice guidelines also involve a preventative, educative function by outlining approaches to identifying and effectively responding to instances of elder abuse. In relation to financial abuse in particular, measures encouraging financial literacy and advocacy for elderly Australians (e.g., ASIC's National Financial Literacy Strategy and MoneySmart program), together with strong regulatory regimes and industry codes of conduct that are aimed at encouraging awareness of elder abuse among both financial institution professionals and clients, are in turn directed at putting safeguards in place to prevent elder financial abuse. State/territory-based laws governing powers of attorney and guardianship also play an important role in the prevention of elder abuse, with legislative protections in place against the abuse of enduring powers of attorney, and the introduction in some jurisdictions of the new role of a supportive attorney, which operates to preserve a principal's decision-making role. Criminal justice responses, including family violence provisions, are also directed at the prevention of elder abuse via intervention/protection order mechanisms.
In terms of prevention approaches more broadly - in the public health sense that has been applied to family violence (e.g., VicHealth, 2007) and other issues, such as smoking, in recent decades - prevention and early intervention approaches are in the early phases locally and internationally. The WHO (2011) has observed that there is limited knowledge on prevention and amelioration approaches, and a number of recent Australian analyses have called for a greater focus in this area (e.g., Clare et al., 2011). One example of a local initiative is a campaign by the Queensland Elder Alder Abuse Prevention Unit, which conducted an elder abuse awareness campaign in 2010 (Sparkes & Jackson, 2011). The campaign was based on the theme: Is it Happening to Someone You Know? It involved posters displayed in shopping centres and cinemas, advertising on television and the supply of announcements for community services slots on radio stations, together with press releases and media interviews. The campaign was targeted at the family and friends of older people and was intended to encourage greater awareness of elder abuse and reports to the Elder Abuse Helpline. An evaluation of the campaign found that notifications of elder abuse to the helpline rose by 64%, with an increase of 6% in notifications from family and friends.
8. What can we learn from international approaches?
International responses to elder abuse have generally been shaped around the evidence of risk factors for perpetration and victimisation (discussed in section 3.2), including the issues of care dependence, poor physical and mental health, low income and isolation (WHO, 2015). More particularly, responses have tended to reflect the recommendations of the WHO (2002b) World Report on Violence and Health, which called for stronger laws and policies and effective prevention strategies.
It is worth noting in this regard the WHO (2002a) Missing Voices report, which canvassed the views of older adults on ways in which to combat elder abuse. That report identified widespread agreement among participants that the prevention of elder abuse is a public responsibility. Strategies proposed by participants to address this issue included:
- the provision of health services and supervision of care institutions;
- the enactment of strong protective laws;
- the development of awareness-raising campaigns to enhance respect for older people, and education strategies to empower older adults (particularly in relation to the management of their financial affairs);
- the provision of training for professionals to recognise and respond to signs of elder abuse; and
- the conduct of longitudinal research to improve knowledge of elder abuse.
The lack of research on the effectiveness of particular prevention strategies is a common theme in the elder abuse literature (e.g., Davidson, Rossall, & Hart, 2015). However, the WHO (2015) noted a number of case study examples supporting the effectiveness of several strategies, including:
- using multidisciplinary teams where professionals pooled expertise to resolve cases of alleged elder abuse;
- providing helplines and websites that provide information to potential victims;
- monitoring by financial institutions for suspicious patterns to identify older adults at risk of financial abuse; and
- conducting public campaigns to raise awareness of elder abuse and enhance respect for older adults.20
The following sections provide some international illustrations of these strategies.
8.1 Legislative responses
The WHO (2002b) noted that, at that time, few countries in the world had enacted specific legislation on elder abuse. Little appears to have changed in the intervening years. In its 2014 Global Status Report on Violence Prevention, which reported on the progress that countries had made in implementing the recommendations of the 2002 report,21 the WHO noted that of all types of violence, laws in relation to elder abuse were the least commonly reported, with only around 40% of countries reporting having enacted laws to prevent elder abuse.
More commonly, the abuse of older adults is addressed through provisions in general criminal laws and laws governing property rights and mental health (WHO, 2002b). A typical example in relation to property rights is Part 9 of the New Zealand Protection of Personal Property Rights Act 1988, which deals with enduring powers of attorney. This part includes sections that impose a duty on those with a power of attorney to "use the donor's property in the promotion and protection of the donor's best interests, while seeking at all times to encourage the donor to develop the donor's competence and to manage his or her own affairs in relation to his or her property" (s 97A(2)).
A number of jurisdictions also have provisions in their criminal law statutes that cover elder abuse. For example, New Zealand's Crimes Act 1961 imposes a legal duty on the carer of a "vulnerable adult" to "take reasonable steps to protect the that person from injury" (s 151). A vulnerable adult for this purpose is "a person unable, by reason of detention, age, sickness, mental impairment, or any other cause, to withdraw himself or herself from the care or charge of another person" (s 2).
More recently, some jurisdictions have enacted legislation to criminalise the abuse of vulnerable older adults. For example, Chapter 13 of the California Penal Code creates a number of elder abuse offences that can be prosecuted as a felony or misdemeanour, with penalties of up to four years' imprisonment on conviction.22 This includes the offences of willfully causing or permitting an elder or dependent adult "to suffer unjustifiable physical pain or mental suffering" and willfully causing or permitting an elder or dependent adult "to be placed in a situation in which his or her person or health is endangered".23 Section 368(a) contextualises the basis for these offences as follows:
The Legislature finds and declares that crimes against elders and dependent adults are deserving of special consideration and protection, not unlike the special protections provided for minor children, because elders and dependent adults may be confused, on various medications, mentally or physically impaired, or incompetent, and therefore less able to protect themselves, to understand or report criminal conduct, or to testify in court proceedings on their own behalf.
The criminal laws of some countries also contain provisions that require the courts to consider evidence that the offence had a significant effect on the victim due to their age, or that the offender in committing the offence abused a position of trust or authority in relation to the victim, as an aggravating factor for sentencing purposes. Canada's Criminal Code (s 718.2) is a case in point.
Another area of legislative intervention in the elder abuse field involves mandatory or permissive reporting laws. For example, in Canada, a number of provinces have laws that require community care facility staff to notify relevant authorities if they witness or become aware of an older adult who is residing in a long-term care home being abused or neglected,24 while some provinces have mandatory notification procedures in relation to older adults living anywhere in the community.25 In a similar vein, the recently enacted Social Services and Well-being (Wales) Act 2014, which will come into force in April 2016, imposes a duty on health services staff to report suspected neglect or abuse of an adult who "has needs for care and support" to a local authority (ss 126, 127).
Some jurisdictions have also enacted laws providing for the reporting of suspected financial abuse (sometimes referred to as "senior fraud"). For example, the Canadian Government recently introduced amendments to the Personal Information Protection and Electronic Documents Act 2000 to allow banks and other financial institutions to notify officials if they suspect that an elderly client is the victim of financial abuse.26
However, as the WHO (2015) report noted, some countries have introduced specific adult protection laws. A recent example is England's Care Act 2014, which came into effect in April 2015.27 Sections 42-46 of this Act deal with safeguarding adults at risk of abuse and neglect. Together with Schedule 2 of the Act and accompanying statutory guidance (Department of Health [DOH], 2014, chapter 14), these provisions create a legal framework to guide a range of relevant organisations and individuals with responsibilities for older adults. In particular, the Care Act requires local authorities, which also have statutory responsibility for child protection, to make "whatever enquiries it thinks necessary" when notified of suspected abuse or neglect of an adult with care and support needs in their area, with a view to determining what, if any, action may be needed (s 42). The statutory guidance makes it clear that these provisions are intended to cover a wide range of abuse and neglect, including domestic violence, physical and sexual abuse, psychological harm, financial abuse, organisational abuse (poor care practices within an institution) and self-neglect (DOH, 2014, paras 14.16-14.26).
8.2 Adult protective services
The WHO (2014) report noted that the countries furthest along in efforts to protect and support older adults include dedicated adult protective services as part of their national policy. However, it also reported that in terms of responses to elder abuse, implementing adult protective services was the least commonly reported initiative, with only a third of respondent countries indicating they had such services in place.
The elder abuse literature suggests that the United States is generally regarded as having the most longstanding and fully developed system for reporting and treating cases of elder abuse (WHO, 2014). Central to this system are state-based adult protective services, which employ dedicated adult protection workers to investigate and prosecute substantiated allegations of elder abuse. Like child protection agencies, adult protective services in many US states are supported by mandatory reporting laws,28 while others have developed specialist risk assessment tools, such as the Elder Abuse Suspicion Index, to screen for elder abuse (Hoover & Polson, 2014). Some states also have elder fatality review teams, convened by a coroner or medical examiner, to identify and examine systemic issues raised by these cases (Stiegel, 2005).
Adult protective services agencies in the Unites States are supported by the National Adult Protective Services Association (NAPSA), a not-for-profit organisation established in 1989 to provide program administrators and their staff with a forum for sharing information and professional development.29 NAPSA also conducts national research on issues relating to the delivery of adult protective services, provides training and technical assistance to adult protective services professionals, and provides information to the public on issues relating to elder and vulnerable adult abuse, exploitation and neglect.
As noted above, England has recently added investigations of elder abuse to the range of statutory responsibilities of local authorities, which currently investigate referrals of suspected child abuse and neglect.30 The Care Act 2014, which came into effect in April 2015, provides that where a local authority has reasonable cause to suspect that an adult in its area has needs for care and support, is experiencing or is at risk of abuse or neglect, and is unable to protect himself or herself against the abuse or neglect or the risk of it, the local authority must make (or cause to be made) "whatever enquiries it thinks necessary to enable it to establish whether any action needs to be taken to prevent or stop the abuse or neglect" (s 42). Abuse and neglect for this purpose cover a wide range of behaviours, including misusing medication, using physical restraints, misappropriating property or benefits, providing poor care practice in a hospital or aged care facility, and withholding nutrition or heating (DOH, 2014, para. 14.17). It also includes self-neglect, such as neglecting one's personal hygiene or health. The legislation is supported by statutory Care Act guidance for relevant professionals and organisations. At present this does not include a framework for risk assessment but it does provide a list of "potential indicators" of abuse, including financial abuse (DOH, 2014, para. 14.23).
As noted, a local authority is not obliged to investigate a notification itself if it decides that others are better placed to conduct the enquiry (Care Act 2014, s 42; DOH, 2014, para. 14.84). For example, where the alleged abuse involves poor care practice within a care home, an employer-led investigation may be more appropriate (DOH, 2014, para. 14.33). The Care Act guidance (DOH, 2014) suggests that in many cases a professional such as a social worker, housing support worker or GP who already knows the adult will be the best person to conduct the enquiry (para. 14.84). Where a crime is suspected (such as sexual assault, fraud, or unlawful imprisonment), the matter should be referred to the police to lead the investigation with the local authority's support (para. 14.85). However, the local authority retains overall responsibility for ensuring the enquiry is acted upon and must assure itself that the investigation satisfies its duty under the Care Act to decide what action (if any) is necessary to protect the adult, and that such action is taken. The local authority also has a responsibility to challenge the agency making the enquiry if it considers the process or outcome is unsatisfactory (para. 14.84).
The English model does not prescribe any particular form of investigation, allowing a flexible approach that accommodates the person's circumstances (DOH, 2014). For example, the enquiry itself could range from a conversation with the affected adult or, if they lack capacity or have substantial difficulty in understanding the enquiry, with his or her representative or advocate, through to a more formal multi-agency course of action (para. 14.64). The Care Act guidance provides that the process should be "person-led and outcome-focused", ensuring the affected adult is involved in the decision about how best to respond to the safeguarding situation, with a decision that reflects the adult's wishes wherever possible (para. 14.15). More particularly, the guidance provides that the affected adult "should experience the safeguarding process as empowering and supportive" (para. 14.79).
Safeguarding enquiries may result in a range of outcomes (DOH, 2014). The investigation might lead to a review of the existing care plan, to disciplinary action, and/or to prosecution if the abuse or neglect is substantiated (para. 14.89). The guidance provides that the outcome should be proportionate to the level of concern, with priority given to ensuring the person's safety and wellbeing (paras 14.66, 14.78). The local authority must also ensure that any action taken that restricts the person's rights or freedoms is the "least restrictive necessary" in the circumstances (para. 1.14).
In a similar fashion to child protection investigations, the Care Act requires the convening of Safeguarding Adults Reviews (SARs) whenever an adult in the local authority's area dies as a result of abuse or neglect and there is concern that the local authority or a partner agency (such as a health service or the police) could have worked more effectively to protect the adult (s 44). The aim of the SAR is to "promote effective learning and improvement action to prevent future deaths or serious harm occurring again" by identifying what the relevant agencies and individuals in the case might have done differently that could have prevented harm (DOH, 2014, para. 14.135, 14.139).
In contrast to England and the US, specialist responses to suspected elder abuse in some other countries are located within the primary health care sector. Ireland, for example, has a dedicated Elder Abuse Service (EAS) located within the Health Service Executive (HSE) to investigate allegations of elder abuse (O'Donnell et al., 2012). The EAS was established in 2007 to provide a coordinated community-based approach to elder abuse. This model centres on a National Elder Abuse Steering Group, which oversees the provision of HSE services for older adults, and designs and delivers elder abuse training for health services staff and the voluntary sector (HSE Elder Abuse Services, 2013). In practice, investigations are conducted by qualified social workers, known as Senior Case Workers, who are based within primary community care services. Senior Case Workers follow up suspected cases of abuse involving people aged 65 and over that are notified to the HSE through its dedicated HSE Information Line (which allows victims and people who are concerned about elder abuse to make a complaint). The Senior Case Worker's investigatory role includes working with the older person and their family and carers to resolve the concerns, and develop a plan that will support the person's safety and care needs (HSE Elder Abuse Services, 2013; O'Donnell et al., 2012). In doing so, the Senior Case Worker's response is guided by a presumption that the older person has mental capacity and a right to self-determination (HSE Elder Abuse Services, 2013).
A more recent international approach to adult protection is one that situates the issue of elder abuse within a broader family violence framework. This is the model used in New Zealand. New Zealand has an Office for Senior Citizens, established in 1990, and a Minister for Senior Citizens. However, responsibility for adult protective services is located within the Department of Family and Community Services, which has responsibility for delivering the country's range of family violence prevention programs. This includes funding for 24 specialist elder abuse and neglect prevention services across the country. Age Concern, a long-standing charitable organisation (founded in the 1940s) dedicated to people over the age of 65, delivers 19 of New Zealand's 24 specialist elder abuse and neglect prevention services.31 The New Zealand Government also contracts Age Concern to provide national training on elder abuse to professionals in the family violence, primary health and aged care sectors.
8.3 Multidisciplinary and multi-agency responses
As the discussion above indicates, the prevention of elder abuse affects a range of different areas of government responsibility. A report published by the National Centre for the Protection of Older People in Ireland, for example, noted the "ongoing debate as to whether it is primarily an issue of human rights, domestic violence, public health, adult protection, criminal justice or empowerment" (O'Donnell et al., 2012, p. 3). In fact, a key theme in the international literature concerns the multi-faceted nature of the issue, and the associated need for multidisciplinary and multi-agency responses. However, a recent US report noted that while there is broad agreement that elder abuse requires a multisystem response, such efforts are often poorly coordinated (Connolly, Brandil, & Breckman, 2014, p. 24).
This recognition has led to growing efforts to develop coordinated responses across the key organisations that provide services for older adults. For example, in June 2015 the New Zealand Minister for Senior Citizens announced a new umbrella initiative called Connects that will see a number of community-based agencies work together to help prevent social isolation and abuse of older adults in that country (Barry, 2015). Similarly, some countries have looked at increasing collaboration and reducing overlaps between the main areas of government responsibility for senior citizens. For example, a 2013 report by the US Government Accountability Office (GAO) identified leadership and coordination as being critical to ensuring the efficient use of limited government resources in the elder justice area (US GAO, 2013). In particular, the report recommended that the Department of Health and Human Services and the Department of Justice (which at that time separately administered 12 overlapping programs affecting elder justice) work to identify common objectives and outcomes and develop a coordinated elder justice approach, including a national public awareness campaign.
A concern to encourage collaboration and multi-agency responses also underpinned the passage of the Care Act 2014 in England, described in the previous section. The adult safeguarding provisions of this legislation grew out of a 2011 Law Commission report, which recommended the creation of a partnership approach to the issue of elder abuse, with local authorities having lead coordinating responsibility. To this end, the Care Act requires every local authority to set up a multi-agency Safeguarding Adults Board (SAB) in their local area. The legislation provides that membership of an SAB must include the local authority, the chief officer of police and a local representative of the National Health Service. The inclusion of the police recognises the critical role they play in investigating crimes and bringing perpetrators to justice where an older adult has been abused. The statutory guidance also encourages local authorities to invite other relevant agencies (such as housing providers, carer groups, general practitioners, and ambulance and fire services) to be a member of the SAB to the extent needed to effectively carry out the SAB's duties (Care Act, Schedule 2; DOH, 2014, paras 14.117-14.118).
The purpose of establishing SABs is to facilitate a "timely and effective" coordinated response by all relevant agencies work to the abuse and neglect of older adults (DOH, 2014, para. 14.7). Early sharing of information is central to this, and the Care Act supports this aim through a statutory information-sharing requirement: an organisation or individual who is likely to have information of relevance to the SAB's functions must share it with the SAB when requested to do so (s 45(1)). The Care Act also requires all organisations involved to have arrangements in place that clearly set out the process for sharing information between each other (s 6). In addition, local authorities and their partner agencies are required to collaborate with each other, to have clear protocols of understanding about how they will share information with one another, and to have mechanisms in place to enable early identification and assessment of risk (DOH, 2014, paras 14.108 & 14.53-14.55).
Each of the three core partners of the SAB (the local authority, the police and the health service) is required to make a resource contribution to ensure the SAB can carry out its functions and oversight role (DOH, 2014, para. 14.105). The Care Act also requires the SAB to publish:
- a strategic plan for each financial year that sets out how it will meet its main objective (to help and protect older adults in its area), and what each member is to do to implement that strategy; and
- an annual report detailing what the SAB has done during the year to achieve its objective, and what it and each member has done to implement its strategy (Care Act, s 44 & Schedule 2).
In addition to these obligations, the Care Act requires SABs to conduct a Safeguarding Adults Reviews (SAR) whenever "there is reasonable cause for concern about how the SAB, members of it or others worked together" to safeguard an older adult and "death or serious harm arose from actual or suspected abuse" (s 44(1)). The purpose of these reviews is to learn lessons and improve practice and interagency working. Agencies are expected to cooperate with the review, and the Care Act also gives SABs the power to require organisations and individuals to provide relevant information.
8.4 Awareness-raising campaigns and public education strategies
The WHO (2014) Global Status Report on Violence Prevention noted that in most cases where laws have led to a change in attitudes and behaviours, the enactment of legislation has been accompanied by widespread awareness-raising initiatives and public education campaigns, as well as capacity building for relevant professionals. However, while cultural norm-change strategies were a commonly reported approach to address violence against women, only 23% of countries had reported implementing public information campaigns on elder abuse.
One country with a long history of using national awareness-raising campaigns in relation to elder abuse is Ireland. Since 2004, Ireland has run a "Say No to Ageism Week" public awareness campaign about discrimination against older adults each year, using advertising, social media and radio to showcase older employees and emphasise the benefits of inclusiveness (WHO, 2015). Awareness raising is also one the Canadian Government's keys strategies for preventing elder abuse. One aspect of this strategy is the New Horizons for Seniors Program (NHSP), which funds community organisations across Canada for projects that focus on elder abuse awareness. Each year, the NHSP invites organisations to apply for funding for community-based projects that will empower older adults to share their knowledge, skills and experiences and to address social isolation among seniors (Employment and Social Development Canada, 2015). The Canadian Government also developed an advertising campaign, "Elder Abuse - It's Time to Face the Reality", launched in 2009, which airs regularly on television, with print and online components. A 2011 public opinion survey indicated that this campaign had significantly increased awareness of elder abuse among Canadians (Government of Canada, 2014).
The WHO has also instituted an Instagram campaign with the hashtag #YearsAhead to combat ageism. It is designed to convey the idea of expenditure on older populations being an investment, rather than a cost, that can yield significant dividends, both for the health and wellbeing of older people and for society as a whole, through increased participation, consumption, and social cohesion.
Around 26% of countries worldwide reportedly have implemented education campaigns to address elder abuse (WHO, 2014). Many of these involve the provision of online information aimed at assisting older adults to navigate financial issues and understand their legal rights, while others provide advice and links to support services for carers who have responsibilities for an older person.
The United States, for example, has an Office of Financial Protection for Older Americans within its national Consumer Financial Protection Bureau, whose website offers services along these lines.32 The New Zealand Government, which has a Minister for Senior Citizens, has also recently established a new SuperSeniors website,33 which provides information and advice about financial management, entitlements to social security benefits, and enduring powers of attorney, along with online support and information programs for carers (Barry, 2015). The Canadian government provides a similar website,34 which has information for older adults, including links to resources on fraud prevention and how to improve financial literacy,35 links to a Senior's Abuse Support Line in each Province,36 and an information portal for caregivers covering topics such as self care,37 and the legal obligations of employers of people with care responsibilities.38
8.5 National action plans
A final initiative that has been adopted by a number of countries is the development of a national action plan. The WHO (2014) emphasised the importance of having comprehensive data-driven national action plans to ensure effective violence prevention. However, it noted that while many of the surveyed countries reported having national action plans for child maltreatment (71%) and intimate partner violence (68%), fewer than half (41%) had addressed elder abuse. The report noted that such plans are an important "way for countries to articulate how violence impacts the health, economic viability and safety and security of a nation", and provides direction for policy makers about what needs to be done, including the identification of objectives, priorities, assigned responsibilities, a timetable and an evaluation mechanism (WHO, 2014, p. 24).
It is worth noting that the WHO is in the process of developing a Global Strategy and Action Plan on Ageing and Health. The public consultation period for this initiative ended on 30 October 2015 and will be considered by the 69th World Health Assembly in May 2016.
20 The WHO (2015) report also noted the importance of providing access to social security benefits for older adults, along with protection from the costs of health care and social care.
21 It contains data collected from 133 countries, representing 88% of the world's population.
22 Note that the Los Angeles District Attorney's Office has a specialist Elder Abuse Unit to prosecute elder abuse offences.
23 California Penal Code § 368(b)(1). These offences are punishable by a fine not exceeding US$6,000, or by both that fine and imprisonment, or by imprisonment in the state prison for two, three or four years.
24 See for example, the British Columbia Community Care and Assisted Living Act 2002, c 75, and the Ontario Long-Term Care Homes Act 2007, c 8.
25 Adult Protection Act, RS, Nova Scotia, c 2.
26 The amendments were enacted by the Digital Privacy Act, which received royal assent on 18 June 2015.
27 The passage of the Care Act places on a statutory footing the duties imposed on local authorities by Article 5 of the European Convention on Human Rights to intervene where adult abuse is suspected (see A Local Authority v A [2010] EWHC 978 (Fam), per Munby J). Similar legislative changes were enacted in Wales. See Part 7 of the Social Services and Well-being (Wales) Act 2014, which will come into force in April 2016.
28 There are some exceptions (such as New York) that have resisted this out of concerns about the civil liberties of older adults (see Brownell, 2010, pp. 1-15).
29 See the NAPSA website: <www.napsa-now.org>.
30 See the National Society for the Prevention of Cruelty to Children, Child protection in England: Referrals and investigation web page: <www.nspcc.org.uk/preventing-abuse/child-protection-system/england/referrals-investigations>.
31 See contact details at Age Concern: <www.ageconcern.org.nz/ACNZPublic/Local_Age_Concerns/ACNZ_Public/AroundNZ.aspx?hkey=189abbc5-0199-4204-b7f6-582dc8804305>.
32 See Financial Protection for Older Americans web page: <www.consumerfinance.gov/older-americans>.
33 See the SuperSeniors website: <superseniors.msd.govt.nz>.
34 See the Government of Canada Seniors website: <seniors.gc.ca>.
35 See Banks and Financial Literacy we page: <yourmoney.cba.ca/seniors/banks_financial_literacy>.
36 See Senior's Abuse Support Line website: <www.seniorsabusesupport.ca>.
37 See Self-Care for Caregivers web page: <www.phac-aspc.gc.ca/publicat/oes-bsu-02/caregvr-eng.php>.
38 See Canadian Employers for Caregivers Plan web page: <www.esdc.gc.ca/eng/seniors/cecp/index.shtml>.
9. Summary and discussion
This report has examined the issues that elder abuse raises in the context of Australia's ageing population and complex jurisdictional frameworks. A feature of the policy backdrop to the issues covered in this report is a ten-year period that has seen momentum for national approaches to child protection and family violence build to the extent that frameworks in both of these areas have been developed through Council of Australian Government processes. The National Framework for Protecting Australia's Children 2009-2020 is now supported by its Third Action Plan 2015-2018. The National Plan to Reduce Violence Against Women and Their Children 2010-2022 is half-way through its Second Action Plan 2013-2016. In each of these areas, the driving concerns have been to find improved responses to complex social problems in the context of Australia's federal system, which sees responsibility for policy and legislative frameworks spread across various levels of government. Both child protection and family violence have a much longer history of knowledge development than elder abuse, with research about these issues gathering pace from the 1960s onwards. In each of these areas, royal commissions are currently underway, reflecting community and government concern about historical institutional responses to child sexual abuse, and contemporary policy and practice responses to family violence in Victoria. The recommendations of each of these royal commissions have the potential to substantially re-shape the policy and legislative landscape in each of these areas (Australian Government, 2014; Victorian Government, 2015).
The material considered in this report establishes that calls for a national consideration of elder abuse are gaining pace (e.g., see Chesterman, 2015a; Lacey, 2014), with widespread recognition among experts in the field that both the existing knowledge base concerning elder abuse and approaches to preventing, identifying and addressing such abuse, however defined, have significant limitations (Clare et al., 2011; Wainer et al., 2010). Community concern is also increasingly evident, reflected in the NSW Parliamentary Inquiry Into Elder Abuse currently underway, and the House of Representative Inquiry Into Older People and the Law in 2007.
The discussion in this report has established that elder abuse is a complicated construct, with varying conceptualisations, in part depending on the theoretical and disciplinary lens through which it is approached (section 2). From a definitional perspective, the lack of an agreed approach in various legislative, policy and practice frameworks is seen to inhibit the development of a coherent approach from the perspectives of both measurement and response. The absence of a consistent approach to elder abuse from a chronological standpoint is emblematic of a deeper need to consider how elder abuse and neglect should be conceptualised, and why it raises questions of public policy that are not dealt with adequately within existing private and public law frameworks (Clare et al., 2011). Considerations in relation to human rights principles and obligations are relevant in this respect; so too are considerations in relation to professional, institutional and personal accountability.
Evidence about prevalence in Australia is lacking, though if international indications provide any guidance, it is likely that between 2% and 14% of older Australians experience elder abuse in any given year, with the prevalence of neglect possibly higher (section 3). In the absence of systematic empirical data, the dynamics, circumstances and effects of elder abuse are difficult to assess. However, the available evidence suggests that most elder abuse is intra-familial and intergenerational, with mothers most often being the subject of abuse by sons, although abuse by daughters is also common, and fathers are victims too. Financial abuse appears to be the most common form of abuse experienced by elderly people, and this is the area where most empirical research is available. Psychological abuse appears slightly less common than financial abuse, and seems to frequently co-occur with financial abuse, suggesting a pattern of behaviour analogous to grooming in the sexual abuse context. For some women, abuse in older age reflects the continuation of a long-term pattern of spousal abuse. Unlike other countries, such as America, the UK, Portugal and Israel, Australia does not have a strategy for measuring prevalence. In the absence of systematic data to shed light not only on prevalence but also on dynamics and effects among different groups and in different circumstances, the evidence base to support further development of policy and practice initiatives is underdeveloped.
The statistical evidence on Australia's age profile is clear (section 4): in the coming decades unprecedented proportions of Australia's populations will be aged. In 2050, just over a fifth of the population is projected to be over 65 (compared with 15% in 2015), and those aged 85 and over are projected to represent about 5% of the population (compared with less than 2% in 2011).39 With three in ten people over 85 having dementia, the numbers of aged people with a primary risk factor for elder abuse are likely to increase substantially. There will be significant cultural diversity among this population. Given that women tend to outlive men, it seems reasonable to suggest that a substantial number of widowed women will be living alone in 2050, a circumstance that again reflects a key risk factor for elder abuse. The numbers of aged people with dementia living in assisted care will also be substantial, underlining the need to consider this context in the development both of prevalence assessment strategies and future policy responses.
With the first annual cohort of the baby boomer generation turning 70 in 2016 (section 5), the evidence on intergenerational wealth and inheritance dynamics raises some challenging issues. In aggregate, the baby boomer generation holds higher levels of wealth than preceding generations due to higher home ownership rates and rising house prices. They, and the annual cohorts that follow them until 1980, are also the generation that was forming and unforming families when no-fault divorce was introduced in 1975. The five years after the introduction of the Family Law Act 1975 (Cth) saw the divorce rate rise substantially, with 63,230 divorces in 1976, a rate of 4.6 per thousand of the resident population, an increase from 1 per thousand of the population in 1970.40 While the highest number of divorces recorded was in 1976, since then the crude divorce rate has remained higher than that apparent prior to 1976, fluctuating between 2.5 and 2.9 for several years, then falling slightly in more recent years (from 2.3 in 2009 and 2010 to 2.1 in 2013), which partly reflects a decline in the marriage rate.41 The research discussed in section 5 suggests that complex family dynamics, including those arising from re-partnering, are associated with conflict in relation to wealth transfer and estates. One implication of such dynamics may be reflected in an escalation of disputes over pre- and post-mortem wealth transfers in the next two or three decades. A relevant social factor in this respect is housing affordability dynamics among the grandchildren of baby-boomers.
Another relevant factor potentially associated with elder abuse warrants mention in light of recent empirical evidence about levels of family violence among separated parents. In section 3, the association between traumatic life events and elder abuse was discussed, with complex family dynamics (including a history of trauma and/or family violence) being a predictor of elder abuse. In the past five years, three nationally representative cohorts of separated parents participating in AIFS research examining the experiences of separated families have demonstrated consistent levels of reports of experiences of family violence in each annual cohort studied.42 These findings suggest that stable and relatively high proportions of separated parents experience complex family dynamics, including family violence. The implications of these findings for future vulnerability to elder abuse among parents (and step-parents or partners) who have experienced separation merit further examination in any future research program.
The discussion in section 6 outlines an array of structures, frameworks and organisations that engage with issues related to ageing and potential elder abuse, with a particular focus on Commonwealth areas of concern. As with child protection and family violence, but to an even greater extent, our federal system of government means that responses to elder abuse are contained within multiple layers of legislative and policy frameworks across health, ageing and law at Commonwealth and state level, with intersections in some areas (health and ageing) and parallel operation in others (state/territory criminal and civil law frameworks). Several international conventions and treaties that establish human rights obligations relevant to elder abuse are also outlined in that section. The discussion of Commonwealth aged care provisions outline measures associated with the oversight of the quality of aged care that enable the identification of, and response to, elder abuse, although shortcomings associated with the absence of a comprehensive national framework for protection against elder abuse, and the current "patchy and under-resourced" (Barnett & Hayes, 2010, p. 57) legal and policy approaches were noted. Important efforts directed at encouraging financial literacy and an effective regulatory framework for elderly clients dealing with financial institutions have also been acknowledged, although calls for improvements in integrated and collaborative responses in this sector are also acknowledged.
A varied range of legislative and policy approaches are evident internationally, and in some countries, including America, the development of response strategies to elder abuse reflect a process of systematic policy and practice engagement with a history exceeding two decades. Among the approaches described in section 8 are legislative responses specific to a legally recognised and defined concept of elder abuse (e.g., the California Penal Code) and the establishment of Adult Protective Services in the US. In common with developments in the area of child protection and family violence in Australia, the discussion of international approaches also highlights international recognition of the need for multidisciplinary, multi-agency approaches, awareness raising campaigns and national action plans.
39 According to one set of projections developed by the ABS (2013b), the proportion of the total Australian population that is aged 65 years and over would increase from 14% in mid-2012 to 22% in mid-2061, while the proportion aged 85 years and over would increase from 2% to around 5%. As the ABS explains, population projections are not predictions. They are based on sets of assumptions concerning future changes occurring in the total fertility rates, mortality (and hence life expectancy) and net immigration. The projections quoted here are based on the ABS' "Series B" set of assumptions.
40 See the AIFS Divorce in Australia web page: <aifs.gov.au/facts-and-figures/divorce-australia>.
>41 See the Australian Bureau of Statistics series Marriages and divorces, Australia (various years) (Cat. No. 3310.0).
42 These studies were conducted by AIFS on behalf of the AGD and DSS in 1998, 2012 and 2014. See: Kaspiew et al. (2009); Qu & Weston (2010); and Qu, Weston, Moloney, Kaspiew, & Dunstan (2014).
References
- Acierno, R., Hernandez, M., & Kilpatrick, D. (2010). Prevalence and correlates of emotional, physical, sexual and financial abuse and potential neglect in the United States: The National Elder Mistreatment Study. American Journal of Public Health, 100(2), 292-297.
- Australian Association of Gerontology. (2015). Inquiry Into Elder Abuse in New South Wales: Submission to Legislative Council Inquiry Into Elder Abuse in New South Wales (Submission No. 23). Sydney: NSW Legislative Council.
- Australian Bankers' Association. (2014a). Protecting vulnerable customers from potential financial abuse (Industry Guideline). Sydney: ABA.
- Australian Bankers' Association. (2014b). Protecting yourself from financial abuse (Consumer fact sheet). Sydney: ABA.
- Australian Bankers' Association. (2014c). Responding to requests from a power of attorney or court-appointed administrator (Industry Guideline). Sydney: ABA.
- Australian Bankers' Association. (2014d). Setting up a power of attorney to help manage your banking needs (Consumer fact sheet). Sydney: ABA.
- Australian Bankers' Association. (2015, 12 February). New tool to help detect financial abuse of Australians (media release). Sydney: ABA. Retrieved from <www.bankers.asn.au/media/media-releases/media-release-2015/New-tool-to-help-detect-financial-abuse-of-Australians>.
- Australian Bureau of Statistics. (2012a). Personal Safety Survey 2012 (Cat. No. 4906.0). Canberra: ABS. Retrieved from <www.abs.gov.au/ausstats/[email protected]/mf/4906.0>.
- Australian Bureau of Statistics. (2012b). Who are Australia's older people? (Cat. No. 2071.0; Reflecting a Nation: Stories from the 2011 Census, 2012-2013). Canberra: ABS.
- Australian Bureau of Statistics. (2013a). Disability, ageing and carers, Australia: Summary of findings 2012 (Cat. No. 4430.0). Canberra: ABS. Retrieved from <www.abs.gov.au/ausstats/[email protected]/PrimaryMainFeatures/4430.0>.
- Australian Bureau of Statistics. (2013b). Population projections, Australia, 2012 (base) to 2101 (Cat. No. 3222.0). Canberra: ABS. Retrieved from <www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/
- 3222.02012%20(base)%20to%202101?OpenDocument>.
- Australian Bureau of Statistics. (2013c). Where and how do Australia's older people live? (Cat. No. 2071.0; Reflecting a Nation: Stories from the 2011 Census, 2012-2013). Canberra: ABS.
- Australian Bureau of Statistics. (2015a). Australian demographic statistics, March 2015 (Cat. No. 3101.0). Canberra: ABS. Retrieved from <www.abs.gov.au/ausstats/[email protected]/mf/3101.0>.
- Australian Bureau of Statistics. (2015b). Deaths, Australia 2014 (Cat. No. 3302.0). Canberra: ABS.
- Australian Government. (2014). Royal Commission Into Institutional Responses to Child Sexual Abuse Terms of Reference 1(d). Canberra: Australian Government. Retrieved from: <www.childabuseroyalcommission.gov.au/about-us/terms-of-reference>.
- Australian Law Reform Commission. (2014). Equality, Capacity and Disability in Commonwealth Law. Melbourne: Justice Connect.
- Australian Longitudinal Study on Women's Health. (2014). 1921-26 cohort: Summary 1996-2013. Callaghan, NSW & Herston, Qld: University of Newcastle and the University of Queensland.
- Australian Securities and Investments Commission. (2014). National Financial Literacy Strategy 2014-17. Melbourne: ASIC.
- Australian Securities and Investments Commission. (2015). Submission to the Queensland Parliamentary Inquiry: The Adequacy of Existing Financial Protections for Queensland Seniors. Brisbane: Queensland Government.
- Bagshaw, D., Wendt, S., & Zannettino, L. (2009). Preventing the abuse of older people by their family members (Stakeholder Paper 7). Sydney: Domestic Violence Clearing House.
- Bagshaw, D., Wendt, S., Zannettino, L., & Adams, V. (2013). Financial abuse of older people by family members: Views and experiences of older Australians and their family members. Australian Social Work, 66(1), 86-103.
- Baker, C., & Gilding, M. (2011). Inheritance in Australia: Family and charitable distributions from personal estates. Australian Journal of Social Issues, 46(3), 273-289.
- Barnett, M., & Hayes, R. (2010). Not seen and not heard: Protecting elder human rights in aged care. University of Western Sydney Law Review, 14, 45-83.
- Barrett, G., Cigdem, M., Whelan, S., & Wood, G. (2015). The relationship between intergenerational transfers, housing and economic outcomes (AHURI Final Report, Vol. 250). Melbourne: Australian Housing and Urban Research Institute.
- Barry, M. (Minister for Senior Citizens). (2015, 15 June). New research and community programmes to combat elder abuse (media release). Wellington: New Zealand Government.
- Bay of Plenty District Health Board. (2012). Health of older people: Strategic plan 2012-2017. Tauranga, NZ: Bay of Plenty District Health Board.
- Birrell, B., & McCloskey, D. (2015). The housing affordability crisis in Sydney and Melbourne: Report one. The demographic foundations. Melbourne: Australian Population Research Institute.
- Brownell, P. (2010). Social issues and social policy response to abuse and neglect of older adults. In G. Gutman, & C. Spencer (Eds.), Aging, ageism and abuse: Moving from awareness to action. London: Elsevier.
- Centers for Disease Control and Prevention. (2015). Elder abuse: Definitions. Atlanta, GA: CDC. Retrieved from <www.cdc.gov/violenceprevention/elderabuse/definitions.html>.
- Chesterman, J. (2013). Responding to violence, abuse, exploitation and neglect: Improving our protection of at-risk adults (Churchill Fellowship Report 2013). Canberra: Winston Churchill Memorial Trust. Retrieved from <www.churchilltrust.com.au/media/fellows/Chesterman_John_2012_Report.pdf>.
- Chesterman, J. (2015a). Taking control: Putting older people at the centre of elder abuse response strategies. Australian Social Work, 1-10.
- Chesterman, J. (2015b). Submission to the Parliamentary Inquiry Into Elder Abuse in New South Wales. Sydney: Parliament of New South Wales.
- Child Family Community Australia. (2014). Pre-employment screening: Working with Children Checks and Police Checks Melbourne: AIFS.
- Clare, M., Blundell, B., & Clare, J. (2011). Examination of the extent of elder abuse in Western Australia: A qualitative and quantitative investigation of existing agency policy, service responses and recorded data. Crawley, WA: Crime research Centre
- Communities, Disability Services and Domestic and Family Violence Prevention Committee. (2015). Inquiry Into the Adequacy of Existing Financial Protections for Queensland's Seniors (Parliamentary Committees Report No. 2, 55th Parliament). Brisbane: Queensland Parliament.
- Connolly, M., Brandil, B., & Breckman, R. (2014). Elder justice roadmap: A stakeholder initiative to respond to an emerging health, justice, financial and social crisis. Alhambra, CA: National Center on Elder Abuse. Retrieved from <ncea.acl.gov/Library/Gov_Report/docs/EJRP_Roadmap_and_Appendices.pdf>.
- Cotterell, E., Leonardi, S., Coward, D., Thomson, J., & Walters, A. (2015). Elder abuse in the ACT: A literature review. Canberra: Council on the Ageing ACT.
- Council of Australian Governments. (2012). National Partnership Agreement on Transitioning Responsibilities for Aged Care and Disability Services. Canberra: Council on Federal Financial Relations. Retrieved from <www.federalfinancialrelations.gov.au/content/npa/health_reform/transitioning_responsibilities/national_partnership.pdf>.
- Cox, P. (2015). Violence against women: Additional analysis of the Australian Bureau of Statistics' Personal Safety Survey 2012 (Horizons No. 1). Sydney: Australia's National Research Organisation for Women's Safety.
- Cramer, E., & Brady, S. (2013). Competing values in serving older and vulnerable adults: Adult protective services, mandated reporting and domestic violence programs. Journal of Elder Abuse and Neglect, 25(5), 453-468.
- Darzins, P., Lowndes, G., & Wainer, J. (2009). Financial abuse of elders: A review of the evidence. Melbourne: Faculty of Medicine, Nursing and Health Sciences, Monash University. Retrieved from < www.eapu.com.au/uploads/research_resources/VIC-Financial_Elder_Abuse_Evidence_Review_JUN_209-Monash.pdf>.
- Davidson, S., Rossall, P., & Hart, S. (2015). Financial abuse evidence review. London: Age UK.
- Department of Health. (2014). Care and support statutory guidance issued under the Care Act 2014. London: Department of Health.
- Department of Health, Victoria. (2012). Elder abuse prevention and response guidelines for action 2012-14. Melbourne: Department of Health.
- Department of Social Services. (2013). Living longer, living better: Aged care in Australia is changing. Canberra: DSS. Retrieved from <www.dss.gov.au/sites/default/files/documents/06_2014/a_-_aged_care_in_australia_is_changing.pdf>.
- Department of Social Services. (2015). My Aged Care: Advocacy services. Canberra: DSS. Retrieved from <www.myagedcare.gov.au/how-make-complaint/advocacy-services>.
- Earl, J., Gerrans, P., Asher, A & Woodside, J. (2015). Financial literacy, financial judgement, and retirement self efficacy of older trustees of self-managed superannuation funds. Australian Journal of Management, 40(3), 435-458.
- Elder Abuse Prevention Unit. (n. d.). Final summary: A "wishlist" for a prevalence study. Queensland: EAPU.
- Elder Abuse Prevention Unit. (2006). Position statement on mandatory reporting of elder abuse. Queensland: EAPU.
- Employment and Social Development Canada. (2015, 15 June). Government of Canada announces project promoting social inclusion of seniors and marks World Elder Abuse Awareness Day (media release). Ottawa: Employment and Social Development Canada.
- Field, S., Matkovic, L., & Bhatia, S. (2015). Final report: The policies and practices of financial institutions around substitute decision making. Sydney: Cognitive Decline Partnership Centre.
- Gil, A., Kislaya, I., Santos, A., Nunes, B., Nicolau, R., & Fernandes, A. (2015). Elder abuse in Portugal. Journal of Elder Abuse and Neglect, 27, 174-194.
- Government of Canada. (2014). Action for seniors report. Ottawa: Government of Canada. Retrieved from <www.seniors.gc.ca/eng/report/index.shtml>.
- Hayslip, B., Reinberg, J., & Williams, J. (2015). The impact of elder abuse education on young adults. Journal of Elder Abuse and Neglect, 27(3), 233-253.
- Health Service Executive Elder Abuse Services. (2013). Open your eyes: There is no excuse for elder abuse. Dublin: HSE Elder Abuse Services. Retrieved from <www.hse.ie/eng/services/publications/olderpeople/elderabuse2013.pdf>.
- Higgins, D. (ed.) (2004). About time! GLBT Seniors ALSO Matter Strategic Plan. South Yarra: The ALSO Foundation.
- Hoover, R. M., & Polson, M. (2014). Detecting elder abuse and neglect: Assessment and intervention. American Family Physician, 89(6), 453-460.
- House of Representatives Standing Committee on Legal and Constitutional Affairs. (2007). Older people and the law. Canberra: Parliament of Australia.
- Jackson, S., & Hafmeister, T. (2015). The impact of relationship dynamics on the detection and reporting of elder abuse occuring in domestic settings. Journal of Elder Abuse, 27(2), 121-145.
- Joosten, M., Dow, B., & Blakey, J. (2015). Profile of elder abuse in Victoria: Analysis of data about people seeking help from Seniors Rights Victoria. Summary report. Melbourne: National Ageing Research Institute & Seniors Rights Victoria. Retrieved from <seniorsrights.org.au/wp-content/uploads/2014/03/Summary-Report_Profile-of-Elder-Abuse-in-Victoria_Final.pdf>.
- Kaspiew, R., Gray, M., Weston, R., Moloney, L., Hand, K., Qu, L., & the Family Law Evaluation Team. (2009). Evaluation of the 2006 family law reforms. Melbourne: Australian Institute of Family Studies
- Kelly, S., Harding, A., AMP, & NATSEM. (2003). AMP-NATSEM income and wealth report. Sydney: AMP.
- Kyle, L. (2012). Assets for care: A guide for lawyers to assist older clients at risk of financial abuse. Melbourne: Seniors Rights Victoria.
- Lacey, W. (2014). Neglectful to the point of cruelty? Elder abuse and the rights of older persons in Australia. Sydney Law Review, 36, 99-130.
- Law Commission. (2011). Adult social care (Law Com. No. 326). London: Law Commission.
- Mann, R., Horsley, P., Barrett, C., & Tinney, J. (2014). Norma's Project: A research study into the sexual assault of older women in Australia (ARCSHS Monograph Series No. 98). Melbourne: Australian Research Centre in Sex, Health and Society, La Trobe University.
- Mariam, L., McLure, R., Robinson, J., & Yang, J. (2015). Eliciting change in at-risk elders (ECARE): Evaluation of an elder abuse intervention program. Journal of Elder Abuse and Neglect, 27(1), 19-33.
- Miskovski, K. (2014). Preventing financial abuse of people with dementia. Sydney: Alzheimers Australia NSW. Retrieved from <nsw.fightdementia.org.au/sites/default/files/20140618-NSW-Pub-DiscussionPaperFinancialAbuse.pdf>.
- NSW Elder Abuse Helpline and Resource Unit. (2015). Submission to the Parliamentary Inquiry into Elder Abuse in New South Wales. Sydney: Parliament of New South Wales.
- O'Donnell, D., Treacy, M. P., Fealy, G., Lyons, I., Phelan, A., Lafferty, A. et al. (2012). Managing elder abuse in Ireland: The senior case worker's experience. Dublin: National Centre for the Protection of Older People, University College Dublin.
- O'Dwyer, L. A. (2001). The impact of housing inheritance on the distribution of wealth in Australia. Australian Journal of Political Science, 36(1), 83-100.
- Office for Senior Citizens. (2015). Towards gaining a greater understanding of elder abuse and neglect in New Zealand. Wellington: Office for Senior Citizens.
- Office of the Public Advocate, & University of South Australia. (2011). Closing the gaps: Enhancing South Australia's response to the abuse of vulnerable older people. Adelaide: Australian Guardianship and Administration Council.
- Office of the Public Advocate (Qld), & Queensland Law Society. (2010). Elder abuse: How well does the law in Queensland cope? Qld: OPA (Qld) & Queensland Law Society.
- O'Keeffe, M., Hills, A., Doyle, M., McCreadie, C., Scholes, S., Constantine, R. et al. (2007). UK Study of Abuse and Neglect of Older People: Prevalence survey report. London: National Centre for Social Research.
- Olsberg, D., & Winters, M. (2005). Ageing in place: Intergenerational and intrafamilial housing transfers and shifts in later life (AHURI Final Report, Vol. 88). Melbourne: Australian Housing and Urban Research Institute.
- Peri, K., Fanslow, J., & Hand, J. (2009). Keeping older people safe by preventing elder abuse and neglect. Social Policy Journal of New Zealand, 35, 159-172.
- Qu, L., & Weston, R. (2010). Parenting dynamics after separation: A follow-up study of parents who separated after the 2006 family law reforms. Canberra: Attorney-General's Department.
- Qu, L., Weston, R., Moloney, L., Kaspiew, R., & Dunstan, J. (2014). Post-separation parenting, property and relationship dynamics after five years. Canberra: Attorney-General's Department.
- Ryan, S. (2015, 13 October). Elder Abuse Forum: A human rights perspective. Presentation to the Elder Abuse Forum, Auburn. Retrieved from <www.humanrights.gov.au/news/speeches/elder-abuse-forum-human-rights-perspectives>.
- Sparkes, D., & Jackson, L. (2011). Elder abuse: Effectiveness and outcomes of an awareness campaign. Fortitude Valley, Qld: Elder Abuse Prevention Unit.
- Spike, C. (2015). The EAPU helpline: Results of an investigation of five years of call data. Report for the International Association of Gerontology and Geriatrics Asia & Oceania Regional Congress 2015. Chermside Central, Qld: Elder Abuse Prevention Unit, UnitingCare Community.
- Stiegel, L. A. (2005). Elder abuse fatality review teams: A replication manual. Washington, DC: Office for Victims of Crime & American Bar Association. Retrieved from <www.americanbar.org/content/dam/aba/migrated/aging/publications/docs/fatalitymanual.authcheckdam.pdf>.
- Tilse, C., Rosenman, L., Peut, J., Ryan, J., Wilson, J., & Setterlund, D. (2006). Managing older people's assets: Does rurality make a difference? Rural Society, 16(2), 169-185.
- Tilse, C., Wilson, J., Setterlund, D., & Rosenman, L. (2005). Older people's assets: A contested site. Australasian Journal on Ageing, 24(Supplement), 51-156
- Tilse, C., Wilson, J., White, B., Rosenman, L., & Feeney, R. (2015). Will-making prevalence and patterns in Australia: Keeping it in the family. Australian Journal of Social Issues, 50(3), 319-338.
- Tomlinson, M. (2012). Gen Y and housing inheritance in Australia. Urban Policy and Research, 30(3), 327-337.
- Treasury. (2015). 2015 intergenerational report: Australia in 2055. Canberra: Commonwealth of Australia.
- United Nations Department of Economic and Social Affairs. (2013). Neglect, abuse and violence against older women. New York: United Nations.
- United Nations General Assembly Open-Ended Working Group on Ageing. (2015). Report of the Open-Ended Working Group on Ageing (A/AC.278/2015/2). New York: UN Department of Economic and Social Affairs. Retrieved from: http://daccess-dds-ny.un.org/doc/UNDOC/GEN/N15/235/92/PDF/N1523592.pdf?OpenElement.
- United States Government Accountability Office. (2013). Elder justice: More federal coordination and public awareness needed (Report to Congressional Requesters No. GAO-13-498). Washington, DC: GAO. Retrieved from <www.gao.gov/assets/660/655820.pdf>.
- VicHealth. (2007). Preventing violence before it occurs: A framework and background paper to guide the primary prevention of violence against women in Victoria. Melbourne: VicHealth.
- Victorian Government. (2015).Royal Commission into Family Violence Terms of Reference. Melbourne: Premier of Victoria. Retrieved from <www.premier.vic.gov.au/wp-content/uploads/2015/01/150119-Proposed-Terms-of-Reference2.pdf>
- Victorian Law Reform Commission. (2012). Guardianship final report. Melbourne: VLRC.
- Wainer, J., Darzins, P., & Owada, K. (2010). Prevalence of financial elder abuse in Victoria: Protecting Elders' Assets Study. Melbourne: Monash University. Retrieved from <www.eapu.com.au/uploads/research_resources/VIC-Prevalence_of_FInancial_Elder_Abuse_MAY_2010-Monash.pdf>
- Wainer, J., Lowndes, G., Owada, K., & Darzins, P. (2010). Staying safe with money: The experience of older English speaking Victorians. Protecting Elders' Assets Study. Melbourne: Monash University.
- Wainer, J., Owada, K., Lowndes, G., & Darzins, P. (2011). Diversity and financial elder abuse in Victoria: Protecting Elders' Assets Study. Melbourne: Faculty of Medicine, Nursing and Health Sciences, Monash University. Retrieved from <eccv.org.au/library/file/projects/Monash_University_Diversity_and_financial_elder_abuse_in_Victoria.pdf>.
- Western Australia, Office of the Public Advocate. (2005). Mistreatment of older people in Aboriginal communities project: An investigation into elder abuse in Aboriginal communities. Perth: OPA.
- White, B., Tilse, C., Wilson, J., Rosenman, L., Purser, K., & Coe, S. (2015). Estate contestation in Australia: An empirical study of a year of caselaw. University of New South Wales Law Journal, 38(3), 880-910.
- Wilkins, N., Tsao, B., Hertz, M., Davis, R., & Klevens, J. (2014). Connecting the dots: An overview of the links among multiple forms of violence. Atlanta, GA: National Centre for Injury Prevention and Control, Centers for Disease Control and Prevention. Retrieved from <www.cdc.gov/violenceprevention/pdf/connecting_the_dots-a.pdf>.
- Wilson, J., Tilse, C., Setterlund, D., & Rosenman, L. (2009). Older people and their assets: A range of roles and issues for social workers. Australian Social Work, 62, 155-167.
- World Health Organization. (2002a). Missing voices: Views of older persons on elder abuse. Geneva: WHO. Retrieved from <www.who.int/ageing/projects/elder_abuse/missing_voices/en/>.
- World Health Organization. (2002b). World report on violence and health. Geneva: WHO. Retrieved from <www.who.int/violence_injury_prevention/violence/world_report/en/>.
- World Health Organization. (2008). A global response to elder abuse and neglect: Building primary health care capacity to deal with the problem worldwide. Geneva: WHO.
- World Health Organization. (2011). European report on preventing elder maltreatment. Geneva: WHO.
- World Health Organization. (2014). Global status report on violence prevention. Geneva: WHO. Retrieved from <www.who.int/violence_injury_prevention/violence/status_report/2014/en/>.
- World Health Organization. (2015). World report on ageing and health. Geneva: WHO. Retrieved from <www.who.int/ageing/publications/world-report-2015/en/>.
- Wu, S., Asher, A., Meyricke, R., & Thorp, S. (2015). Age pensioner profiles: A longitudinal study of income, assets and decumulation. Sydney: ARC Centre of Excellence in Population Ageing Research.
- Yon, Y., Wister, A. V., Mitchell, B., & Gutman, G. (2014). A national comparison of spousal abuse in mid- and old age. Journal of Elder Abuse and Neglect, 26(1), 80-105. doi 10.1080/08946566.2013.784085
- Zannettino, L., Bagshaw, D., Wendt, S., & Adams, V. (2015). The role of emotional vulnerability and abuse in the financial exploitation of older people from culturally and linguistically diverse communities in Australia. Journal of Elder Abuse Neglect, 27(1), 74-89.
Appendix
Centres for Disease Control and Prevention
Injury Prevention and Control: Division of Violence Prevention
Elder abuse: Definitions
Elder abuse is any abuse and neglect of persons age 60 and older by a caregiver or another person in a relationship involving an expectation of trust.
Forms of elder abuse include:
- Physical Abuse occurs when an elder is injured (e.g., scratched, bitten, slapped, pushed, hit, burned, etc.), assaulted or threatened with a weapon (e.g., knife, gun, or other object), or inappropriately restrained.
- Sexual Abuse or Abusive Sexual Contact is any sexual contact against an elder's will. This includes acts in which the elder is unable to understand the act or is unable to communicate. Abusive sexual contact is defined as intentional touching (either directly or through the clothing), of the genitalia, anus, groin, breast, mouth, inner thigh, or buttocks.
- Psychological or Emotional Abuse occurs when an elder experiences trauma after exposure to threatening acts or coercive tactics. Examples include humiliation or embarrassment; controlling behavior (e.g., prohibiting or limiting access to transportation, telephone, money or other resources); social isolation; disregarding or trivializing needs; or damaging or destroying property.
- Neglect is the failure or refusal of a caregiver or other responsible person to provide for an elder's basic physical, emotional, or social needs, or failure to protect them from harm. Examples include not providing adequate nutrition, hygiene, clothing, shelter, or access to necessary health care; or failure to prevent exposure to unsafe activities and environments.
- Abandonment is the willful desertion of an elderly person by caregiver or other responsible person.
- Financial Abuse or Exploitation is the unauthorized or improper use of the resources of an elder for monetary or personal benefit, profit, or gain. Examples include forgery, misuse or theft of money or possessions; use of coercion or deception to surrender finances or property; or improper use of guardianship or power of attorney.
Source: Centres for Disease Control and Prevention (2015)
Dr Rae Kaspiew is a Senior Research Fellow and Dr Rachel Carson is a Research Fellow, both at the Australian Institute of Family Studies. Professor Helen Rhoades is an academic from the Melbourne Law School, The University of Melbourne.
Views expressed in this publication are those of the authors and may not reflect those of the Australian Institute of Family Studies or the Australian Government.
This report was commissioned and funded by the Australian Government Attorney-General's Department (AGD).
The authors would like to acknowledge the support and assistance provided by the AGD, in particular by AGD officers Emma Swinbourne and Genevieve Schulz, and to thank the Australian Bankers Association (ABA) and the Australian Securities and Investments Commission (ASIC) for their contributions to this research.
We also extend our thanks to the AIFS librarian Carole Jean for her research assistance and to our editor Lan Wang for her invaluable assistance, including for her insight and attention to detail in editing this report.
We would also like to thank Anne Hollonds, Director of AIFS, and Associate Professor Daryl Higgins, Deputy Director (Research), together with AIFS Assistant Director, Ruth Weston, and Senior Research Fellow, Dr Lixia Qu, for their advice and support throughout this research.
An earlier version of this report was published on the Attorney-General’s Department’s website.
Correction (2 November 2018)
In one instance in an earlier version of this report, on page 46 of the PDF, it is stated: “Evidence about prevalence in Australia is lacking, though if international indications provide any guidance, it is likely that between 2% and 10% of older Australians experience elder abuse in any given year, with the prevalence of neglect possibly higher. “ This should have read “…it is likely that between 2% and 14% of older Australians experience elder abuse in any given year…”
Cover photo: © iStockphoto/KatarzynaBialasiewicz
Kaspiew, R., Carson, R., & Rhoades, H. (2015). Elder abuse: Understanding issues, frameworks and responses (Research Report No. 35). Melbourne: Australian Institute of Family Studies.
978-1-76016-082-1
25 February 2016