Parenting influences on adolescent alcohol use
You are in an archived section of the AIFS website
Overview
Alcohol use is widespread among Australian adolescents, and high risk use is a serious and growing problem.
A range of individual, family, peer, school and community characteristics have been shown to be risk factors for the development of adolescent alcohol use and misuse.
This report reviews and synthesises the research and interventions concerning the impact of parenting factors on adolescent alcohol use. It focuses particularly on recent Australian research and research with Indigenous and other cultural sub-groups, but also includes influential research conducted in other countries. It concludes with discussion of implications for research and policy, highlighting key conclusions that may be drawn from the findings reviewed.
Foreward
While there is widespread acknowledgement of the problem of adolescent abuse of alcohol, the pathways to it remain contentious. The influence of parents on these pathways has been unclear. This report, Parenting Influences on Adolescent Alcohol Use, provides invaluable new insights into the influences that parents exert on adolescent alcohol use.
The report's messages have an elegant clarity and answer a number of key questions. Among these are: Should parents delay adolescents' introduction to alcohol? What role do parents play in guiding responsible alcohol use? How do parents exert an influence? What other sources of influence are there - for example, from peers, the wider culture and the media? Which interventions have been demonstrated to work, and how widely available are these in Australia?
This report provides answers to these questions. For example, it demonstrates the long-term benefits of delaying adolescents' uptake of alcohol. It also shows the ways in which parents can guide patterns of use once adolescents have started consuming alcohol. It explodes a popular myth that parents have little impact in this area by showing that they can and do influence their offspring's alcohol use, especially through their supervision and monitoring behaviours, the closeness of their relationships with their children, and through positive behaviour management practices. While parents have a greater influence than many would admit, the peer group, cultural norms, and the law also play substantial roles. Successful modification of the patterns of teenage drinking will need to target all these spheres of influence.
While there is very little Australian research and very few intervention programs with proven success, this report shows some productive ways forward, both through investment in research and evaluation, and the implementation of evidence-based interventions.
The Australian Government Department of Health and Ageing is to be congratulated for this most valuable investment in addressing an issue of such widespread community concern. The authors of the report, Louise Hayes, Diana Smart, John Toumbourou and Ann Sanson, are to be especially commended on completing a significant and groundbreaking report.
This volume should provide an excellent resource for policy makers, practitioners, and researchers, to work together to address a social issue of urgent priority. I am delighted that the Australian Institute of Family Studies could contribute to such a productive collaboration and look forward to its impacts on policy and practice.
Professor Alan Hayes
Director
Australian Institute of Family Studies
Executive summary
This report is the fulfilment of a contract between the Australian Government Department of Health and Ageing and the Australian Institute of Family Studies. Alcohol use is widespread among Australian adolescents, and high risk use is a serious and growing problem. A range of individual, family, peer, school and community characteristics have been shown to be risk factors for the development of adolescent alcohol use and misuse. This report aims to review and synthesise the research and interventions concerning the impact of parenting factors on adolescent alcohol use.
To set the scene for the review, the patterns of alcohol use among Australian adolescents are described. Alcohol use is shown to be common among young Australians, with many experimenting with alcohol by the age of 14-15 years. Once adolescents begin drinking, most become regular consumers of alcohol. The evidence suggests that delaying the onset of drinking reduces long-term consumption levels into adulthood. A large proportion of Australian adolescents obtain alcohol from their parents.
Two theoretical models are used to provide a framework in which to understand the research on parenting influences on adolescent alcohol use. First, the Social Interactional model is used to describe the impact of parenting behaviours and skills such as monitoring, parental behaviour management, parent-adolescent relationship quality, and parenting norms, goals and values. Second, the Social Development model is used to understand the importance of broader environmental influences on adolescents and parents. Thus, parental consumption of alcohol, parental alcohol abuse and dependence, family structure, and family socio-economic background, the role of differing cultural norms and legal systems, and findings regarding Indigenous adolescents are examined.
Parental monitoring
Parental monitoring has been defined as parental awareness of the child's activities, and communication to the child that the parent is concerned about, and aware of, the child's activities (Dishion and McMahon 1998). The review demonstrates that adolescents who are poorly monitored begin alcohol consumption at an earlier age, tend to drink more, and are more likely to develop problematic drinking patterns. Australian parents are likely to be unaware of, or to underestimate, their adolescent's alcohol consumption and are more concerned about illicit drug use than alcohol use. Australian parents may feel pressured to accept alcohol use by adolescents as "normal". It appears that for many parents, knowing the "right age" to permit their adolescents to consume alcohol, or indeed if they should permit alcohol consumption at all, is a critical question that they feel ill equipped to answer.
Parental behaviour management
Parental behaviour management encompasses positive practices such as the use of incentives, positive reinforcement, setting limits for appropriate behaviour, providing consequences for misbehaviour, and negotiating boundaries and rules for appropriate behaviour, as well as less effective strategies such harsh and punitive discipline, high conflict, and lax, inconsistent or over-permissive approaches. Family standards and rules, rewards for good behaviour, and well developed negotiation skills were associated with lower initiation of alcohol use in early adolescence, and lower rates of alcohol abuse and dependence in early adulthood. Harsh discipline and high conflict were associated with higher rates of alcohol use. When parents were openly permissive toward adolescent alcohol use, adolescents tended to drink more.
Relationship quality
Parent-adolescent relationship quality underpins all aspects of parenting, and is the product of an ongoing interplay between parents and adolescents. For example, without a warm relationship, adolescents are more likely to resist monitoring, while authoritative parenting may contribute to and enhance strong parent-adolescent relationships. Warm and supportive parent-adolescent relationships were associated with lower levels of adolescent alcohol use, as well as lower rates of problematic use and misuse.
Parental norms
Parenting norms, values and goals reflect parents' belief systems, attitudes and conceptions concerning adolescent behaviour. Parental norms, attitudes, and beliefs with regard to adolescent alcohol use have an important influence on adolescent alcohol consumption. When parents show disapproval, their adolescents are less likely to drink, and conversely, when parents are tolerant or permissive, their adolescents are likely to drink more. Australian parents and adolescents differ in their perceptions of the appropriate age that adolescents should be permitted to consume alcohol, with studies showing that many parents believe 17 years is the appropriate age for adolescents to begin consuming alcohol at home, and many adolescents tending to believe this should occur earlier, at approximately 16 years.
Parental, family and broader environmental influences
Parents' own use of alcohol was found to increase the likelihood that adolescents would also consume alcohol. Biological links between parental alcohol dependence and adolescent alcohol use were evident. Adolescents from intact families were found to less often engage in heavy alcohol use, while adolescents from sole parent families were more often involved in heavy drinking.
In addition, social laws and norms were shown to exert a considerable influence on adolescent alcohol consumption, and parental attitudes toward adolescent alcohol use. International research has found that changes to policy or laws can influence adolescent consumption patterns.
Parenting and peer influences compared
The effect of peers was shown to mediate the influence of parenting on adolescents' alcohol use. Peer effects become particularly powerful when parent-adolescent relationships are of poorer quality. The influence of peers is thought to occur through peer modelling, peer pressure, or association with alcohol using peers. However, direct connections between parental monitoring and adolescent alcohol use remained after peer influences were taken into account.
Gaps and deficiencies in the research
There are a number of gaps and deficiencies in the literature. First, the research coverage is incomplete, Second, there is very little Australian data on this issue, and international research was relied upon to a large extent. When considering parent-adolescent relationships and parenting behaviours in general, international research reveals similar findings to Australian research. However, there are important social and cultural differences which may influence parenting behaviours and attitudes concerning adolescent alcohol use in differing countries. Third, much of the research has sought the views of adolescents only, and the findings need to be confirmed by parents and/or other informants. Fourth, while there was considerable consistency in the findings, on one important area - parental supply of alcohol - inconsistent findings were found. Finally, the possibility of gender differences has often been overlooked.
Promising intervention programs
Using randomised controlled trials as the "gold standard" for intervention programs, a small number of interventions conducted in other countries, which targeted changing parenting behaviours and parental education, have shown long term reductions in adolescent alcohol use. Several promising Australian interventions are currently underway, including PACE, Teen Triple P, and ABCD. However, Australian research using rigorous methodology and thorough evaluations is needed.
Synthesis of findings
To summarise the research reviewed, a conceptual model of parenting influences on adolescent alcohol use was developed. This model suggested that parental monitoring, parental norms for adolescent use, and parental behaviour management skills all have direct links to adolescent alcohol use. Parent-adolescent relationship quality has an overall effect on these parenting behaviours, as well as direct connections to alcohol use. Parental characteristics have an indirect effect on alcohol use, by way of their influence on the parenting behaviours described above. The parental characteristics depicted as having an indirect effect include parental alcohol use or abuse, as well as family factors, and broader cultural norms regarding alcohol use.
Conclusions
The evidence demonstrates that there is now a reasonable understanding of the processes by which parents influence adolescent alcohol use. In addition, there is also intervention evidence suggesting these principles can be translated into effective programs. Several specific conclusions are presented which highlight strategies to assist parents to more effectively guide adolescents towards responsible alcohol use.
Conclusion 1
Parents should be provided with information concerning the advantages of delaying the age at which young people begin using alcohol.
Based on the available research, there appear to be clear advantages in delaying the age at which young people begin using alcohol. Among these are the reduced likelihood of risky alcohol use and abuse in adulthood, averting the adverse impacts of alcohol on the developing adolescent body and brain, and avoiding the immediate risks to health and wellbeing conveyed by "normal" patterns of adolescent alcohol use (which are often at risky or high risk levels). It is unclear that parents are aware of this evidence, and efforts to publicise this information would appear highly worthwhile.
Conclusion 2
Parents should be provided with educative guidelines on the influence of parental attitudes and norms on adolescent alcohol use, as well as guidance in managing the social pressure they feel to allow their adolescents to consume alcohol.
Parents report feeling adverse social pressure and not having the confidence to assist children and adolescents to delay the initiation of alcohol use. However, the research evidence suggests that parental attitudes and norms can play a considerable role. Parents should be made aware of this research, and may also benefit from more information about the extent of high risk alcohol consumption among Australian adolescents, and distinctions between safe and risky levels of alcohol use. Additionally, knowledge that many Australian parents believe late adolescence to be the appropriate age at which adolescents should be introduced to alcohol might assist parents to resist pressure to permit their adolescent to commence use at an earlier age.
Conclusion 3
Once adolescents have commenced alcohol use, parents should be provided with educative guidelines which enable them to guide their adolescents in responsible alcohol use.
Once adolescents have commenced drinking, enhanced monitoring appears to be a key component of efforts to minimise harmful alcohol use. However, this first requires attention to the parent-adolescent relationship, and simply advising parents to ask more questions may have a detrimental effect in some families. Once a high quality parent-child relationship is in place, parents can then be educated on the importance of clear and consistent rules regarding alcohol use, setting age appropriate limits, and maintaining open communication about adolescents' use of free time.
Conclusion 4
Parent education and family intervention programs should be supported in Australia to assist parents to gain skills for encouraging their adolescents to delay initiation to alcohol use and to adopt less harmful patterns of use. Intervention and prevention programs should receive best practice evaluations.
Interventions that have shown promise in the North American context should be adapted, implemented and evaluated in Australia. Existing Australian interventions should also be evaluated for their potential to encourage a delayed age of first alcohol use and more moderate patterns of use. Prior to encouraging wider dissemination, evaluation funding should be provided to enable gold standard evaluations including randomised control trial designs and long-term follow-up evaluations. These best practice programs should promote the parent-adolescent relationship as a key starting point. As was demonstrated by this review, this aspect of parenting underpins the other elements shown to be important, for example monitoring and positive behavioural management techniques.
Conclusion 5
Given that broader social norms exert a considerable influence on adolescent alcohol use, strategies to reduce favourable cultural attitudes towards under-age alcohol consumption will be needed to support parental efforts.
An extensive educative effort, aimed at changing favourable societal attitudes towards adolescent alcohol use, appears necessary to assist parental efforts to delay adolescents' initiation of alcohol use and to guide responsible subsequent use. It will also be necessary to target broader adolescent attitudes regarding alcohol.
Conclusion 6
More Australian research is needed to promote understanding of the developmental processes and pathways to adolescent alcohol use. In particular, research on the development of adolescent alcohol use in Indigenous communities is seriously lacking.
At present, there is a critical lack of Australian data on the pathways to differing patterns of alcohol use, and the role that parents play. There is also a lack of Australian research evaluating promising intervention initiatives. Thus, the international research, and particularly the U.S. research, is relied upon to a large extent. Yet there are important differences, particularly relating to cultural norms and attitudes, which may dilute the transferability of the international research to the Australian context. In particular, there is almost no research on Indigenous communities on this issue. A greater investment in research in this area would appear to be vital.
1. Introduction
Alcohol use is widespread among Australian adolescents. The 2001 National Drug Strategy Household Survey, for example, found that two-thirds of 14-17 year olds had recently consumed alcohol, with approximately one-fifth reporting regular alcohol use. Similarly, longitudinal data from the Australian Temperament Project showed that 25 per cent of 13-14 year old adolescents had consumed alcohol within the past month, and noted a sharp escalation in alcohol use across adolescence, with 60 per cent of these adolescents consuming alcohol in the past month at 15-16 years and 85 per cent at 17-18 years (Smart, Vassallo, Sanson, Richardson, Dussuyer et al. 2003).
Adolescent alcohol misuse is a serious and growing problem. Although many adolescents experience no alcohol-related problems (Bonomo, Coffey, Wolfe, Lynskey, Bowes and Patton 2001), a large sub-group engage in risky drinking. For example, the Australian Institute of Health and Welfare (AIHW 2003) found that 35 per cent of Australian adolescents aged 14-17 years and 64 per cent of those aged 18-24 years were reported to drink at risky or high-risk levels in the short term. The incidence of risky alcohol use is reported to be even higher among Indigenous youth (AIHW 2003).
Numerous individual, family, school and community characteristics have been identified as risk factors for the development of adolescent alcohol use and misuse1 (Hawkins, Catalano and Miller 1992). This report aims to review and synthesise the research concerning the impact of parenting factors on adolescent alcohol use. It is anticipated that a better understanding of parenting influences on adolescents' uptake of alcohol and risky alcohol use will provide valuable guidance for prevention and intervention initiatives, enabling the provision of more effective family support services.
This report is in fulfilment of a contract between the Australian Government Department of Health and Ageing and the Australian Institute of Family Studies. The report aims to:
- Review and summarise the literature concerning parenting influences on adolescent alcohol use, focusing particularly on recent Australian research and research with Indigenous and other cultural sub-groups; but also including influential research conducted in other countries.
- Analyse the current body of knowledge concerning parenting influences on adolescent alcohol use, identifying gaps and weaknesses and detailing how such deficiencies might weaken the strength of conclusions that may be drawn and that may impact upon intervention strategies.
- Elucidate the implications emerging from the research findings for the development of policies and prevention/intervention initiatives directed towards adolescent alcohol use and alcohol harm minimisation, highlighting the ways in which parents can be assisted to guide adolescents more effectively in responsible alcohol use.
- Identify related issues that may affect the relationship between parenting and adolescent alcohol consumption.
Prior to the review of relevant research, an account of the study's search strategies is provided, and some of the critical methodological issues are discussed; these are covered in Section 2. Material is presented in Section 3 on the prevalence of alcohol use by Australian adolescents to provide a picture of the extent of normative and problematic alcohol use.
Discussion of the parenting factors linked to adolescent alcohol use is organised according to the parenting model developed by Dishion and McMahon (1998) (referred to as the "Parenting model" throughout). This model is nested within the Social Development Model developed by Catalano and Hawkins (1996), which was used to highlight the broader ecological framework in which parenting and parent-adolescent interactions take place. (For a broader discussion of parenting itself and the factors which influence parenting, the report Parenting Information Project: Volume Two: Literature Review, published by the Australian Government Department of Family and Community Services in 2004, provides a comprehensive review.)
Using these theoretical guides, a review of the parenting behaviours and beliefs that have been shown to influence adolescent alcohol use is provided in Section 4. These include: parental monitoring; parental behaviour management; parent-adolescent relationship factors; and parental norms, values and goals.
An emphasis has been placed on longitudinal research, although cross-sectional and clinical studies are also included, particularly those of importance to the Australian context. Cross-sectional studies examine connections between predictors and outcomes which are both measured at the same point in time, whereas longitudinal studies follow the progress of a particular sample over an extended period of time, exploring across-time connections between predictors and outcomes. Additionally, previously unpublished research findings from the Australian Temperament Project are included to augment the Australian database.
Section 5 provides a discussion of some specific parental characteristics, such as parental use of alcohol, the biological transmission of alcohol dependence, and other ecological and environmental factors which affect parents and their parenting practices. The implications of broader cultural norms and laws for adolescent alcohol use are discussed and a review of research conducted with Indigenous adolescents is also provided in Section 5.
The contrasting roles of parents and peers are examined in Section 6. Some gaps and deficiencies in the literature are discussed in Section 7.
Following the analysis of relevant research findings, Section 8 presents intervention research that has attempted to manipulate parenting factors to reduce adolescent alcohol initiation or consumption. These experimental studies play a pivotal role in understanding the importance of parenting for adolescent alcohol use, as they provide the most direct evidence of "cause and effect" relationships.
A synthesis of the findings is presented in Section 9, and the review concludes with a discussion, in Section 10, of implications for research and policy, highlighting key conclusions that may be drawn from the findings reviewed.
1. The term "adolescent" is used here to describe young people aged from 11 to 21 years, covering the age span from the onset of puberty to the early adulthood stage of development.
2. Literature review methodology
This section outlines the search strategy and selection criteria adopted for this review, and provides descriptions of the types of studies reviewed. The methodological foundations upon which the reviewed research rest are then discussed.
Search strategy
Relevant research concerning parenting influences on adolescent alcohol use was identified by searching the biomedical and social sciences databases for primary research material. A total of 18 research databases were searched for publications from 1990 through to the present (2004), with key articles obtained primarily from PsychINFO, MEDLINE, ERIC, and The Cochrane Library. A complete list of the databases searched is included in Appendix 1.
In order to ensure that relevant studies were not missed, the search terms remained broad. These were "parenting or family", plus "adolescent or youth", plus "alcohol" anywhere in the title or abstract. No language restrictions were employed. Studies were eligible for consideration in this review if: (a) the focus of the study was adolescent alcohol use, or substance use (providing alcohol use was measured separately); and (b) there was at least one parenting variable measured.
To capture unpublished Australian research, personal contact was made with key researchers at universities and research institutions across Australia. This included key personnel at the Australian Drug Foundation, the National Drug Research Institute, the National Drug and Alcohol Research Centre, and other research organisations. A complete list of the organisations contacted is included in Appendix 2.
Finally, a comprehensive search was made of Internet resources in Australia and internationally. A number of sites were searched, although the primary sites used were the Australian Drug Foundation's Drug Information Clearinghouse and the United States National Clearinghouse for Drug and Alcohol information. A complete list of the websites searched is provided in Appendix 3.
Selection criteria
The next step was a detailed examination of papers, and at this point studies were excluded if the parenting or adolescent measures were insufficiently described, or alcohol use was only a minor variable in the study, and therefore the study did not contribute important information to this review.
For the studies investigating direct associations between parenting and adolescent alcohol use, the review includes all peer reviewed longitudinal studies investigating parenting and adolescent alcohol use. Longitudinal studies were seen as a particularly valuable resource as they facilitate the testing of relationships between early events or characteristics and later outcomes, and enable the identification of developmental sequences and pathways, as well as the construction of theoretical models which can then be validated in future research. Cross-sectional studies which used large samples and methodologically sound research designs were also retained. Studies with methodological weaknesses arising from small convenience samples, few factors measured, or weak data analysis, were included only when they provided insights not available from more rigorous studies. For the qualitative studies, those studies that contributed new information or covered areas that had not been fully explored in quantitative studies were included. Due to the limited volume of Australian published studies, Australian quantitative and qualitative studies were included wherever possible.
For the review of intervention research, studies were retained if: they employed "control" or "no-treatment" groups; participants were randomly assigned to treatment and non-treatment groups; and the studies included pre-intervention measures as well as post-intervention or follow-up measures.
Study descriptions
As with much research in the area of parenting, the majority of studies were correlational - that is, they investigated statistical relationships between parenting factors and adolescent alcohol use, and interpreted the associations found as showing a direct impact of parenting on adolescent behaviour. The possibility of "mediated" effects, in which parenting impacts on adolescent alcohol use through the influence of an intervening variable (for example, peer influence), has been infrequently investigated. Thus, while most studies have investigated direct associations only, it should be noted that the findings reported may mask more complex relationships.
Overall, 26 cross-sectional and 30 longitudinal studies were included in this review. A small number of qualitative Australian studies were found, and these have been included in the text alongside the discussion of findings emerging from the quantitative studies. Only two intervention programs were found that met the eligibility criteria, that is, they had a treatment and control group; pre-test, posttest and follow-up stages; and positive outcomes. The results of these intervention studies follow the review of research studies. Due to the limited number of intervention studies available, a brief review of promising work has also been included.
Finally, this report includes data from the Australian Temperament Project. This is a large, longitudinal study which has followed children's psychosocial development from infancy into adulthood, investigating the contribution of personal, familial and broader environmental factors to adjustment and wellbeing. This project is one of very few large scale Australian longitudinal studies that contains data on parenting and adolescent alcohol use.2
Methodological considerations
Regarding the methodological foundations upon which the reviewed research rest, there are at least five key issues which must be kept in mind when considering the research outcomes. These are: (a) the nature of correlational research; (b) the measurement of parenting and adolescent variables; (c) the importance of considering the differing levels of alcohol use amongst adolescents; (d) the timing of data collections; and (e) the comparability of cross-cultural findings.
First, as noted previously, the majority of the research is correlational, and cannot therefore determine "cause and effect" relationships. To be confident about causal connections, research would require experimental manipulation of parenting factors under tightly controlled conditions - an approach not feasible in social research. Nevertheless, the correlational research is able to demonstrate significant statistical associations between adolescent alcohol use and parenting factors. Furthermore, the longitudinal studies are able to demonstrate the importance of parenting factors over time, and their weight and sheer volume make it clear that there are indeed significant across-time relationships between parenting behaviours and adolescent alcohol use. With regard to parent and adolescent programs designed to prevent adolescent alcohol use, a change in parental and/or adolescent behaviour patterns is considered essential to demonstrate program effectiveness.
Second, most research on parenting influences has used parent or adolescent reports, collected via self-completion questionnaires. A minority of studies have used observations to assess parenting behaviours. Parental reports reflect parental perceptions, and hence may provide only a partially accurate portrayal of parental behaviours, as they are affected by self-enhancing biases and social desirability. Thus, studies which include parental reports and observational measures often report relatively low rates of agreement between these two sources of information (for example, Smart, Sanson, Toumbourou, Prior and Oberklaid 2000). Equally, adolescent reports are affected by adolescents' perceptions, and research has demonstrated that adolescents generally have a more negative view of their families than do their parents, and they see their families as less cohesive (Noller 1994). Thus, in this review of mainly self-report studies, results should be tempered by the notion that parents tend to have a positive bias, while adolescents have a negative bias.
Few studies have collected parent and adolescent data together. Information from multiple informants can provide a more complete picture, although again, there may be relatively low rates of agreement between the differing respondents. It can be valuable to obtain information from both parents and adolescents because they generally do not report the same level of problems in their interactions and the views of one may counterbalance those of the other. The few studies that have gathered data from both parties suggest that the concordance between adolescent and parent reports tends to be quite low, even when using identical measures. There is also evidence that concordance between parent and adolescent reports decreases as adolescent age increases. Therefore, younger adolescents are likely to report greater parental involvement and more agreement with parents.
Third, it is also likely that if adolescent alcohol use reaches problem levels, adolescents' self-reports of parenting behaviours will be influenced by negative attributions in family interactions and these adolescents are likely to report that their parents are less involved. Thus, it is possible that a somewhat biased view of parental behaviours might be obtained from adolescents with entrenched patterns of risky alcohol use. The research looks at adolescent alcohol use at several levels, including initiation of use, the age at first use, the pattern of regular use, and high risk alcohol use and misuse. Where the level of adolescent alcohol use has been measured alongside a parenting factor, it has been highlighted in this report.
Fourth, it is not always clear in the research when the data were collected, but the timing of data collections, particularly of adolescent self-reports of alcohol use, may have an important bearing on the results. For example, in Australia the fourth term of the school year coincides with end-of-year parties and summer celebrations. It is highly likely that adolescents at this time of the year would report a greater use of alcohol than they would during other parts of the year. Unfortunately the timing of data collection is generally not included in the research studies.
Finally, this review aimed to summarise both the Australian and international literature, although because of the limited number of Australian studies which possess both parenting and adolescent alcohol use data, the international research was relied on quite heavily. Studies included in this review were conducted in Canada (for example, Williams, McDermitt and Bertrand 2003), New Zealand (for example, Ferguson, Horwood and Lynskey 1995), and Scandinavian countries (for example, Bjarnason et al. 2002), although research conducted in the United States predominates.
There are two key issues to consider when comparing Australian and United States research: first, whether adolescents in Australia display similar patterns of alcohol use when compared with adolescents in the United States and, second, the comparability of Australian and United States populations in terms of the mechanisms of parenting, the ways in which parents influence their adolescents, and parental and cultural norms concerning adolescent alcohol use. These issues are discussed further in Section 4 and Section 7.
2. The Australian Temperament Project (ATP), involving a representative sample of over 2400 Victorian families, commenced in 1983 at a child age of four to eight months. A total of 13 waves of data have been collected by mail surveys over the first 20 years of the children's lives, with information provided by parents, maternal and child health nurses, teachers and, from the age of 12 years onwards, the children themselves. The study has focused primarily on the children's development and wellbeing. From early adolescence onwards, adolescents have reported on their recent use of substances, along with many other aspects of life.
3. Alcohol: Age of initiation, levels of use, and risky use
Before proceeding with a discussion of parenting influences, it is necessary to set the scene by discussing rates and levels of alcohol use among Australian adolescents. This section provides an overview of information about: the age at which Australian adolescents commence drinking; levels of adolescent alcohol consumption, distinguishing between "moderate" and "risky" levels of use; the risks associated with alcohol consumption; adolescents' views of alcohol and their reasons for drinking; their source of access to alcohol; and the settings in which adolescent alcohol use takes place. The section ends with a brief comparison of Australian and United States trends in adolescent alcohol use.
Initiation and consumption levels
Alcohol consumption among Australian adolescents before the legal age of 18 years is the norm, rather than the exception. The Australian School Students' Alcohol and Drug Survey (hereinafter ASSAD) has provided repeated population-based data on the alcohol consumption patterns of Australian adolescents (White and Hayman, in press). The most recent survey on 24,403 secondary students aged 12-17 years shows that by the age of 14 years 90 per cent of Australian adolescents have tried a full glass of alcohol, and 95 per cent of 17 year olds have tried a full glass (White and Hayman, in press).
The 2001 National Drug Strategy Household Survey (hereinafter NDSHS) conducted by Australian Institute of Health and Welfare found that young people aged 14-24 years reported that their first glass of alcohol was consumed at around 14.6 years for males, and 14.8 years for females (AIHW 2003a). Other large surveys have also found that for the majority of adolescents, their first full glass of alcohol is consumed somewhere between their 14th and 15th year (Premier's Drug Prevention Council 2003). Therefore it seems that most adolescents begin experimenting with alcohol at approximately 14-15 years of age.
Once their first glass of alcohol is consumed, a sizeable proportion of adolescents appear to progress to regular drinking. With regard to repeated consumption, the NDSHS showed that 20 per cent of males and 17 per cent of females aged 14-17 years were classified as regular weekly drinkers (AIHW 2003a), and two-thirds of adolescents aged 14-17 years had consumed a full glass of alcohol in the past 12-months.
As shown in Table 1, there are differences in adolescent consumption between the NDSHS and ASSAD data. The rates of regular drinking are considerably higher in the ASSAD data which show that 34 per cent of adolescents had consumed alcohol in the past week, with the rates being slightly higher rates for males (37 per cent) than females (31 per cent). These differences are likely to be attributable to survey content and methodology. For example, there were differences between the two studies in the phrasing of the questions, the age of respondents, and the place where the data were collected (at home versus at school).
| NDSHS survey 2001: 14-17 years | Males % | Females % |
|---|---|---|
| Regular (weekly) | 19.8 | 17.1 |
| Occasional (past year) | 44.3 | 51.6 |
| Ex-drinker | 6.6 | 4.3 |
| Never a full glass of alcohol | 29.2 | 27.0 |
| ASSAD survey 2002: 12-17 years | Males % | Females % |
| In past week | 37 | 31 |
| In past month | 15 | 16 |
| In past year | 23 | 25 |
| Never | 11 | 13 |
Source: AIHW (2003a); White and Hayman (in press).
Comparisons between the 1999 and 2002 ASSAD survey data show that there was no significant change in adolescent alcohol use in the past three years. Longer-term comparisons show that while consumption among 12-15 year olds was similar in 2002 and 1999, these rates were significantly higher than in 1996 and 1993. For the 16-17 year age group, the proportion of drinkers in 2002 was slightly lower than in 1999, but overall the rate has remained relatively stable since the early 1990s (White and Hayman, in press). In both age groups (12-15 and 16-17 years), the proportion of adolescents who drank at risky levels remained relatively stable from the 1990s survey period through to the current 2002 survey wave (White and Hayman, in press).
Delayed onset
There is some evidence to suggest that the later adolescents delay their first alcoholic drink, the less likely they are to become regular consumers. Adolescents who start later are more likely to report that they are light or occasional drinkers, and they are less likely to binge (Premier's Drug Prevention Council 2003). In the United States, the National Longitudinal Epidemiologic Survey of 27,616 young people (cited in Spoth, Lopez Reyes, Redmond, and Shin 1999) shows that the lifetime alcohol dependence rates of those people who initiate alcohol use by age 14 are four times as high as those who start at age 20 years or older. Furthermore, the odds of dependence decrease by 14 per cent with each additional year of delayed initiation (cited in Spoth et al. 1999).
Longitudinal data from New Zealand also demonstrate that the commencement of alcohol use in early adolescence increases the likelihood of the subsequent development of high risk use, independent of other influences (Fergusson, Horwood and Lynskey 1995). Young people who begin using alcohol at a younger age are more likely to progress to regular use in adolescence (Fergusson, Lynskey and Horwood 1994). Australian longitudinal studies have demonstrated that regular drinking in adolescence is an important risk factor for the development of abusive, dependent (Bonomo et al. 2001) and risky (Toumbourou Williams, White et al. 2004) patterns of use in young adulthood.
Risky adolescent alcohol use
The 2001 National Health and Medical Research Council (NHMRC) guidelines for alcohol use recommend that males should, on average, drink no more than four standard drinks per day and on any particular day, no more than six standard drinks; females should drink no more than two standard drinks per day on average, and four standard drinks on any one day. As well, this level of use should occur on no more than three days per week. Definitions are also provided of "risky" and "high risk" patterns of alcohol use, which are further separated into short-term and long-term harms (see Table 2 for description).
| Type of risk | Risky alcohol use | High risk alcohol use |
|---|---|---|
| Short-term harms | ||
| Males | 7-10 drinks on any one day | 11+ drinks on any one day |
| Females | 5-6 drinks on any one day | 7+ drinks on any one day |
| Long-term harms - Males | ||
| - on an average day | 5-6 drinks per day | 7+ drinks per day |
| - overall weekly level | 29-42 drinks per week | 43+ drinks per week |
| Long-term harms - Females | ||
| - on an average day | 3-4 drinks per day | 5+ drinks per day |
| - overall weekly level | 15-28 drinks per week | 29+ drinks per week |
Source: NHMRC (2001).
It is important to note that these Australian guidelines were developed for healthy adults, not adolescents. In fact, adolescents' physical immaturity (for example, smaller body size), and inexperience with alcohol make young people more susceptible to the harmful effects of alcohol than adults. Thus, for the same dose of alcohol, more harm can result for an adolescent than an adult.
The NDSHS reports that for the Australian population as a whole, alcohol is the second greatest cause of drug-related deaths and hospitalisations (AIHW 2002). Amongst adolescents, one-third (34.4 per cent, or 387,400) of 14-17 year olds had put themselves at risk of alcohol-related harm in the past 12 months on at least one occasion, and this is similar to the overall population rate of 34.4 per cent (AIHW 2002).
According to a recent report from the National Drug Research Institute on drinking patterns among 14-17 year olds, 85 per cent of adolescent alcohol consumption is consumed at a risky or high-risk level for acute harm (Chikritzhs, Catalano, Stockwell, Donath, Ngo, Young and Matthews 2003). These findings suggest that when Australian adolescents consume alcohol, most do so at risky levels. Furthermore, this risk of harm occurs regularly, with 18 per cent of young people reporting drinking at levels of risk for short-term harms on a weekly basis (increased from 15 per cent in 2002), and 50 per cent drinking at these levels on a monthly basis (as compared with 42 per cent in 2002) (Premier's Drug Prevention Council 2003).
The rate of long-term risky alcohol consumption has recently increased among females aged 14-17 years, rising from 1 per cent in 1998 to 9 per cent in 2001 (Chikritzhs et al. 2003). However, the rate of risky long-term alcohol use among males aged 18-24 years has decreased, falling from 9 per cent in 1998 to 6 per cent in 2001. These findings might reflect fluctuations rather than long-term trends, and it will be important to continue measuring consumption trends to establish whether more enduring shifts in alcohol use are taking place.
Harms associated with adolescent alcohol use
Binge drinking can cause bowel, central nervous system, and psychological problems, and is also related to a high risk of injury, assault, road accidents, fights, other violence, sexual assault, and unprotected sex (AIHW 2003a). Serious binge drinking may result in alcohol poisoning, and can lead to coma or death (AIHW 2003a). While under the influence of alcohol, 26 per cent of young people reported verbally abusing someone, 13 per cent had driven a car, and 12 per cent had created a public disturbance (Premier's Drug Prevention Council 2003). In this Victorian survey, 41 per cent of young people reported being abused by someone under the influence of alcohol, while 20 per cent had been fearful of a person who was under the influence of alcohol (Premier's Drug Prevention Council 2003).
According to the Australian Institute of Health and Welfare (AIHW 2002), alcohol-induced memory lapses, where alcohol was consumed and events were unremembered afterwards, were more prevalent in adolescents aged 15-19 years than in adults. The NDSHS found that 4.4 per cent of adolescents reported alcohol-induced memory lapses occurred at least weekly, and 10.9 per cent reported this occurred at least monthly. The comparison rates for adults are considerably lower, with adults aged 20-29 years at 3.6 per cent for weekly rates and 7.7 per cent monthly. The prevalence of memory lapses following alcohol abuse continues to decline further with age (AIHW 2002). It has also been suggested that risky levels of alcohol use during adolescence can have deleterious effects on the developing brain (Scott and Grice 1997), and this is exacerbated by faster absorption rates and a less efficient metabolic system during this stage of development.
The ASSAD report shows that in both age groups (12-15 and 16-17 years) the proportion of adolescents who drink at high risk levels has remained relatively stable from the surveys conducted in the 1990s through to the current 2002 data collection wave (White and Hayman in press).
Adolescents' reasons for drinking
Alcohol remains a socially acceptable drug in Australia. The report produced by the Australian Institute of Health and Welfare, entitled Australia's Young People: Their Health and Wellbeing (AIHW 2003a) shows that young Australians aged 14-24 years perceive that heroin and cannabis are problem drugs, but that alcohol, amphetamines, tobacco and ecstasy are not. Among young Victorians aged 16-17 years, 26 per cent describe alcohol use as "not wrong at all" for them, and 48 per cent described it as "a little bit wrong" (Premier's Drug Prevention Council 2003).
Of concern are recent survey results showing that adolescents' expectations of alcohol consumption are different from adults'. According to the Victorian Drug and Alcohol use survey of 6052 young people aged 18-24 years, 20 per cent of young people intended to get drunk when they drink (Premier's Drug Prevention Council 2003). Further, Chikritzhs et al. (2003) suggest the percentage of adolescents who intend to get drunk might in fact be considerably higher than these rates.
Where do adolescents consume alcohol? Where do they obtain it?
The location of adolescent consumption of alcohol is shown in Table 3, which again displays NSDHS and ASSAD data. The NSDHS data show that for adolescents aged 14-19 years who had consumed alcohol in the past 12 months, the most common location was private parties (males 67.8 per cent, females 70.2 per cent), followed by friends' homes (males 62.9 per cent, and females 63.9 per cent), or their own homes (males 61.5 per cent, females 61.1 per cent). The ASSAD data, which describes adolescent alcohol consumption within the past week, shows a similar pattern of consumption at home or parties, although consumption at friends' homes or in public places is lower. The relatively high rate of consumption in public places and in cars shown in the NSDHS data is of concern. (AIHW 2002)
These data do not clarify the social milieu in which alcohol is consumed. For example, when alcohol is consumed at home, it is probable (but not certain) that parents are present, but it remains unknown whether parents actively supervise their adolescent's alcohol consumption. Likewise, when alcohol is consumed outside the home, presumably this occurs in social settings with peers and may, or may not, involve adult supervision. These are important considerations, but generally, this information has not been supplied.
The legal age for purchasing alcohol in retail outlets in Australia is 18 years, yet the majority of adolescents begin drinking before this. The ASSAD survey of 24,403 students in Years 7-12, found that parents were the most common source of alcohol, with 38 per cent of students reporting their parents gave them their last drink (White and Hayman, in press). Furthermore, this survey found that it was more likely that parents would provide alcohol to younger rather than older students, with rates of 42 per cent in the 12-15 year group compared with 32 per cent in 16-17 year group. It appears that older students may be able to obtain alcohol from other sources.
| NSDHS 2001 14-19 years (in past year) | ASSAD 2002 12-17 years (in past week) | |||
|---|---|---|---|---|
| Location | Males % | Females % | Males % | Females % |
| In my home | 61.5 | 61.1 | 36 | 34 |
| At friend's house | 62.9 | 63.9 | 14 | 15 |
| At private parties | 67.8 | 70.2 | 29 | 32 |
| At rave/dance parties | 22.9 | 24.5 | ||
| At restaurants/cafes | 22.4 | 25.5 | ||
| At licensed premises | 37.1 | 38.8 | ||
| At school/TAFE/Uni | 6.2 | 3.4 | ||
| At workplace | 5.8 | 2.7 | ||
| In public places | 14.1 | 10.6 | 4 | 4 |
| In a car | 12.2 | 7.0 | ||
| Somewhere else | 8.3 | 7.2 | ||
Source: AIHW (2002);White and Hayman (in press).
Other surveys also report that a considerable number of adolescents obtain alcohol through their parents. The 2003 Victorian Youth Alcohol and Drug Survey found that parents had purchased alcohol for half of the adolescents who had drunk alcohol and were under 18 years (51 per cent) (Premier's Drug Prevention Council 2003). The NSDHS data showed that just over two-thirds of persons aged 14-17 years obtained their alcohol through a friend or relative (69.2 per cent) (AIHW 2002). Similarly, Taylor and Carroll (2001) found that 29 per cent of adolescents aged 15-17 years reported that their parents had provided alcohol. These surveys show that between 30 per cent and 50 per cent of adolescents who drink obtain their alcohol from their parents.
Australian and United States trends compared
One methodological issue noted earlier was whether Australian patterns of adolescent alcohol use are similar to those of the United States. Epidemiological research has shown that at a population level, alcohol consumption patterns in Australia and the United States are not dissimilar, but there can be some variation in use. International comparisons of alcohol consumption for the total population (adults, adolescents and children) reveal that Australians consume more alcohol, with consumption rates of 7.8 litres per capita, compared with the United States at 6.7 litres, Canada at 6.6, and the United Kingdom at 8.4 (AIHW 2003b). Assessing behavioural differences between young people in the different countries is more complicated.
A major source of data concerning American trends in youth substance use is the Monitoring the Future (MTF) youth survey. This study has provided annual estimates of high school student substance use since 1975. Additionally, the MTF survey was extended in 1995 and 1999 to countries in Europe. In general, rates of alcohol and tobacco use were considerably higher for European students than students in the United States, while rates of illicit drug use were higher in the United States (Hibell et al. 2000).
In one of the few matched studies comparing Australia and America, Beyers and colleagues (2004) reported clear differences across the two countries in students' levels of substance use. At the same age, there were markedly higher levels of youth alcohol and tobacco use in the Victorian sample and slightly higher marijuana and other illicit drug use among the United States sample. Similar inter-country differences were reported in the early 1990s in a comparison presented by Makkai (1994). Similarly, Toumbourou (2004) presented findings from carefully matched large state surveys conducted in 2002 which compared students in Victoria and Washington State. This comparison revealed, once again, a pattern of markedly higher rates of alcohol use for students in Victoria relative to Washington State in Grade 5 (primary school) and Years 7 and 9 (secondary school).
Comparative studies in older age groups have also tended to show higher rates of alcohol use in Australia relative to the United States (Makkai 1994), however there has been at least one comparison inconsistent with this trend. A comparison of alcohol use for young people aged 14-17 years responding to the Australian National Survey of Mental Health and Wellbeing Survey (NSMHWB) and the United States Youth Risk Behaviour Survey on which the Australian survey was modelled, revealed differences in consumption for adolescent females but not for males. For adolescent males the lifetime prevalence of alcohol use was 73 per cent for Australians, and this was similar to the United States rate of 79 per cent. However, there was a significant difference for females, with prevalence of lifetime alcohol use for Australian female adolescents at 70.6 per cent, compared with American females at 80.7 per cent (Pirkis, Irwin, Brindis, Patton and Sawyer 2003).
Despite this apparent similarity between adolescent alcohol use in Australia and the United States, Pirkis and colleagues (2003) cautioned that errors can occur when cross-cultural comparisons are based on survey data that had not been matched in content and context. To demonstrate the errors that can occur with these comparisons, Pirkis et al. compared the prevalence rates as shown on the Australian NSMHWB, with the American Youth Risk Behaviour Survey, and the American NHSDA survey. They found that when the NHSDA survey data was used, the rates of alcohol use appeared much lower in the United States than Australia whereas, as described earlier, results were quite similar when the Australian NSMHWB trends were compared to the American Youth Risk Behaviour Survey data (Pirkis et al. 2003). Therefore, for the cross-cultural comparisons, caution is always required.
There has been limited investigation of inter-country differences in the harms associated with alcohol use and findings are mixed. Jernigan (2001) presented inter-country comparisons across a range of indicators that are known to be influenced by youth alcohol use. With respect to mortality related to motor vehicle crashes, the death rates for people aged under 25 in 1997 were higher in the United States (5.79 per 100,000) than in Australia (3.92 per 100,000). However, suicide rates were higher in Australia (3.14 per 100,000) than in the United States (2.06 per 100,000).
Summary
This brief overview has shown that alcohol use is common among young Australians, and that most begin experimenting with alcohol by the age of 14-15 years. Once they begin drinking, a large proportion become regular consumers of alcohol. The evidence suggests that delaying the onset of drinking reduces longterm consumption levels into adulthood. Adolescents reported that they tended to drink to get drunk, and that they put themselves at considerable risk when they drank. Adolescents tend to drink at home, at parties, or at friends' homes. Finally, it was shown that a considerable proportion of adolescents (up to one half) obtain their alcohol from parents.
With regard to cross-national comparisons, the available evidence suggests that school age adolescents in the United States have lower rates of alcohol and tobacco use but higher illicit drug use by comparison with youth of similar ages in Australia and the majority of Europe. Although differences in the young adult age group may be less pronounced at a population level, alcohol consumption rates appear lower in the United States. One would expect that cultural and social norms might contribute to consumption patterns, and these differences should be considered when interpreting overseas studies within an Australian context.
4. Parenting influences on adolescent alcohol use
It is widely believed that parents have little influence on adolescents' alcohol use, and there has been a common assumption that the influence of peers is more important than parental influence (Johnson and Johnson 2000). The research to be reviewed here does not support this notion. The findings reviewed are consistent with those of many other studies which have investigated associations between parenting behaviours or parental characteristics and a range of child and adolescent problems, and have shown links between several parenting factors and internalising and externalising behaviour problems in children and adolescents.
Framework for reviewing parenting literature
The purpose of this review is to identify the particular parenting factors that are linked to adolescent alcohol use. To do this, a theoretical model of parental influence developed by Dishion and McMahon (1998) will be used. This is a Social Interactional model of parenting and it provides a framework to demonstrate the relevance of parenting characteristics to adolescent behaviours. This conceptual model of parenting is developed from a large body of research, which has shown that several key parenting factors influence child and adolescent behaviour (for example the body of work in the Oregon Youth study, Patterson, Reid and Dishion 1992).
The Social Interactional model is shown in Figure 1. At the centre of the model is the parent-child relationship, which forms the foundation of effective parenting. Therefore, research that considers how parents may influence adolescent alcohol use should consider the contribution of quality of parent-adolescent relationships. The apex of this model is represented by a parent's motivations, and this is a compilation of parental beliefs, norms, values, and goals. It has been shown that parent's expectations of parenting, along with their expectations of their child, are critical to parenting behaviours (Patterson 1982). Finally, the social interactional model of parenting depicts the role of parental monitoring and parents' management of adolescent behaviour, but they are interrelated with parent-adolescent relationship quality and parental motivation, goals, values and beliefs. Using this framework, it becomes evident that parenting factors are dynamically interrelated, for example, parental values are likely to influence parenting behaviour management skills.
While Dishion and McMahon's model is used as a tool to organise the diverse array of findings, it should be noted that relationships are dynamic, and the importance of examining parent-adolescent interactions within a bi-directional paradigm should also be considered. Research has shown that parents influence the behaviour of their adolescents, but the reverse also occurs, with adolescents exerting influence that changes the behaviour of their parents. The longitudinal body of work by Capaldi (2003), Capaldi and Patterson (1989), Dishion, Capaldi, Spracklen, and Fuzhong (1995), Patterson et al. (1992), and Patterson and Stouthamer-Loeber (1984), over an 11-year period, provides substantial evidence of the multi-faceted nature of parenting, and the bi-directionality of influences. Other researchers have also demonstrated the bi-directional nature of parent-adolescent relationships (Brody 2003), and more recently this has also been demonstrated in intervention work using rigorous experimental methodology (Dishion, Nelson and Kavanagh 2003).
In addition to the bi-directional nature of parent-adolescent relationships, the ecology of the family is also crucial, and the Social Development model (Hawkins, Catalano and Miller 1992) is used as a framework for understanding broader family and environmental influences.
This model is a general theoretical model of behaviour which integrates social learning theories and control theory, and has been developed to provide a framework for understanding the role of family, peers, and community in the development of various adolescent behaviour problems (Catalano and Hawkins 1996; Hawkins et al. 1992). Thus, the model proposes that adolescents who are poorly attached to families, schools and community, but are more strongly attached to antisocial peers, are more likely to engage in problem behaviours such as substance use and antisocial behaviour.
This model has been used to measure positive and negative influences using a risk and protective conceptual framework. Therefore, throughout this review, where parenting factors are examined, there is an underlying assumption that adolescents can and do change the behaviour and attitudes of their parents, and that the ecology surrounding the adolescent and parent exerts further influence.
Figure 1. Social interactional parenting model
Source: Dishion and McMahon (1998)
Summary
Two theoretical models are used to provide a framework in which to understand parenting influences on adolescent alcohol use.
First, the Social Interactional model of Dishion and McMahon (1998) is used to understand the importance of a range of parenting skills and behaviours, in particular parent-adolescent relationship quality, parental monitoring, parents' management of adolescent behaviour, and parents' norms, goals and values.
Second, the Social Development model of Catalano and Hawkins (1996) is used to highlight the ecological context surrounding the parent and adolescent, focusing on broader aspects of family environment and the influence of peers.
Overview of findings
Tables 4 and 5 summarise the findings regarding the most consistent associations found between aspects of parenting and adolescent alcohol use. Other findings which emerged less frequently are described in the text, rather than displayed. Table 4 displays the results emerging from the cross-sectional studies, and Table 5 the results from the longitudinal studies. These tables present an overview of the results, and each parenting factor is discussed subsequently in this review.
In the tables, the arrows depict the effect that the parenting factor was shown to have on adolescent alcohol use. For example, in the parental monitoring column, the downward arrows indicate that high levels of this factor are associated with lower adolescent alcohol use. The final column in each table denotes whether the study was conducted with Australian participants, and reveals that there has been little Australian research on this issue to date. Following the Dishion and MacMahon (1998) model, the review begins with a discussion of the findings concerning parental monitoring, which is followed by a review of findings relating to parents' behaviour management, parent-adolescent relationship quality, and parental norms and attitudes. Broader aspects of the family environment are then reviewed, such as parental alcohol use and abuse, family structure, and family socio-economic background. The impact of cultural norms and laws, and findings emerging from indigenous samples, are described. Parenting influences are compared with peer influences, and gaps and deficiencies in the research are discussed. Finally, the results of intervention studies are reviewed.
The table can also be viewed on page 34 of the PDF.
| Cross-sectional studies | Biological history of alcoholism | Familial alcohol abuse | Parents regular drinkers | Parents disapprove or negative norms | Parents provide alcohol | Higher parental monitoring | Parents permissive | Good parent-child relationship | Positive behaviour management | Harsh parenting or high conflict | Mother and father together | Responder | Australian participants |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baker et al. (1999) | ? | A | |||||||||||
| Beck,Boyle & Boekeloo (2003) | ? | ? f | A | ||||||||||
| Beck, Ko & Scaffa (1997) | ? | P | |||||||||||
| Bjarnason et al. (2002) | ? | A | |||||||||||
| Bonomo et al. (2001) | ? | A | 3 | ||||||||||
| Borawski, et al. (2003) | ? | ? | ? | A | |||||||||
| Brown et al. (1999) | ? | ? | AP | ||||||||||
| Chassin et al. (1993) | ? | ? | AP | ||||||||||
| DiClemente et al. (2001) | ? | A | |||||||||||
| Epstein, Botvin & Spoth (2003) | ? g | A | |||||||||||
| Flannery, Vazsonyi, Torquati & Fridrich (1994) | ? | A | |||||||||||
| Hawthorne (1996) | ? | A | 3 | ||||||||||
| C. Jackson (2002) | ? | A | |||||||||||
| Keefe (1994) | ? | A | |||||||||||
| Letcher et al. (in press) | ? | ns | AP | 3 | |||||||||
| X. Li, Feigelman & Stanton (2000) | ? | A | |||||||||||
| Neighbors, Clark, Donovan & Brody (2000) | ? ? g | AP | |||||||||||
| Quine & Stephenson (1990) | ? | A | 3 | ||||||||||
| Rai et al. (2003) | ? | A | |||||||||||
| Sale, Sambrano, Springer & Turner (2003) | ? | ? | A | ||||||||||
| Smith & Rosenthal (1995) | ? | A | 3 | ||||||||||
| Svensson (2000) | ? | A | |||||||||||
| Vicary, Snyder & Henry (2000) | ? | A | |||||||||||
| White & Hayman (in press) | ? | A | 3 | ||||||||||
| P.S. Williams & Hine (2002) | ? | ? | ? | A | 3 | ||||||||
| Wood, Read,Mitchell & Brand (2004) | ? | ? | ? ? | A | |||||||||
| J.Yu (2003) | ns | ? | A | ||||||||||
| Note: ? or ? = direct predictive effect of parenting variable, ? or ? = indirect (mediational) effect of parenting variable, ? ? or ? ? = variable has direct effect and also an indirect effect by interacting with another factor (moderator). g = gender differences, a = age effects, f = father only, m = mother only, ns = not significant, P = Parent respondent, A = Adolescent respondent, 3 = Australian sample | |||||||||||||
The table can also be viewed on page 35 of the PDF.
| Longitudinal studies | Biological history of alcoholism | Familial alcohol abuse | Parents regular drinkers | Parents disapprove or negative norms | Parents provide alcohol | Higher parental monitoring | Parents permissive | Good parent-child relationship | Positive behaviour management | Harsh parenting or high conflict | Mother and father together | Responder | Australian participants |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ary, Duncan, Biglan et al. (1999) | ? ? | ? | ? | AP | |||||||||
| Ary, Duncan, Duncan & Hops (1999) | ? ? | ? | ? | AP | |||||||||
| Barnes & Farrell (1992) | ? | ? | ? | ? | AP | ||||||||
| Barnes, Reifman, Farrell & Dintcheff (2000) | ? | ? | ? | A | |||||||||
| Baumrind (1991) | ? | ? | AP | ||||||||||
| Bray, Adams, Getz & Baer (2001) | ? | A | |||||||||||
| Bray, Adams, Getz & Stovall (2001) | ? ? | ? ? | ? ? | A | |||||||||
| Brody, Ge, Katz & Ileana (2000) | ? | AP | |||||||||||
| Brody & Ge (2001) | ? | ? | ? | AP | |||||||||
| Chilcoat & Anthony (1996) | ? | A | |||||||||||
| Dishion, Capaldi & Yoerger (1999) | ? | ns | ? | AP | |||||||||
| Duncan, Duncan, Biglan & Ary (1998) | ? | ? | A | ||||||||||
| Ennett, Bauman, Foshee et al. (2001) | ? | AP | |||||||||||
| Guo, Hawkins, Hill & Abbott (2001) | ? | ? | ns | A | |||||||||
| Jackson, Henriksen & Dickinson (1999) | ? | ? | A | ||||||||||
| Kosterman, Hawkins, Guo, Catalano & Abbott (2000) | ? | ? | ? | A | |||||||||
| F. Li, Duncan & Hops (2001) | ? | ? | A | ||||||||||
| C. Li, Pentz & Chih-Ping (2002) | ? ? | A | |||||||||||
| X. Li, Stanton & Feigelman (2000) | ? | A | |||||||||||
| Ouellette, Gerrard, Gibbons & Reis-Bergan (1999) | ? | ? | AP | ||||||||||
| Oxford, Harachi, Catalano & Abbott (2001) | ? | ? | A | ||||||||||
| Pedersen (1995) | ns | ? | ? g | A | |||||||||
| Prior, Sanson, Smart & Oberklaid (2000) | ? | AP | 3 | ||||||||||
| Reifman, Barnes, Dintcheff et al. (1998) | ? | A | |||||||||||
| Rodgers-Farmer (2000) | ? ? | A | |||||||||||
| Steinberg, Fletcher & Darling (1994) | ? | A | |||||||||||
| Stice, Barrara & Chassin (1998) | ? | ? | ns | ? | ns | AP | |||||||
| Thomas, Reifman, Barnes & Farrell (2000) | ? | ? | A | ||||||||||
| Webb, Bray, Getz & Adams (2002) | ? g | A | |||||||||||
| B. Williams, Sanson, Toumbourou & Smart (2000) | ? | ? | AP | 3 | |||||||||
| Note: ? or ? = direct predictive effect of parenting variable, ? or ? = indirect (mediational) effect of parenting variable, ? ? or ? ? = variable has direct effect and also an indirect effect by interacting with another factor (moderator). g = gender differences, a = age effects, f = father only, m = mother only, ns = not significant, P = Parent respondent, A = Adolescent respondent, 3 = Australian sample | |||||||||||||
Parental monitoring
The most widely accepted definition of parental monitoring is: parental awareness of the child's activities, and communication to the child that the parent is concerned about, and aware of, the child's activities (Dishion and McMahon 1998). Thus, the term "parental monitoring" describes parental efforts to influence adolescents' independent use of free time via the establishment of boundaries for appropriate behaviour and communications with adolescents about their activities when away from parents.
More recently the definition of monitoring has been fiercely debated in the literature with two opposing views presented. This debate centres on the direction of effects, and whether the greatest influence in monitoring is driven by parenting behaviours, or by adolescent willingness to be monitored. However, the complexities of this debate are beyond the scope of this present report (see Hayes, 2003 for a review), and the Dishion and McMahon view has been used because it provides a sound definition with an influential research base.
There are numerous cross-sectional and longitudinal studies linking poor parental monitoring with adolescent alcohol and substance use. Thus, 14 of the 26 cross-sectional studies, and 17 of the 30 longitudinal studies reported connections between parental monitoring and adolescent alcohol use. A recent review of 113 studies where parental monitoring was a key variable (Hayes 2004) revealed that lower monitoring has been correlated with externalising problem behaviours in adolescents, including antisocial behaviour, "deviant" peer associations3, substance use, and sexual risk-taking. Internalising problems and related behaviours have also been linked to poor monitoring, including psychological maladjustment, lowered self-esteem, and poor academic achievement. Furthermore, in studies of family functioning, poor monitoring is associated with parent-adolescent relationship difficulties, family dysfunction, and social disadvantage (Dishion and McMahon 1998, Patterson et al. 1992). The following studies have the most rigorous and relevant findings in relation to adolescent alcohol use and the role of parental monitoring.
The relationship between increased adolescent alcohol use and lower parental monitoring has been demonstrated consistently in several large longitudinal studies (Barnes and Farrell 1992; Barnes et al. 2000; Guo et al. 2001; Reifman et al. 1998; Thomas et al. 2000). Barnes and colleagues (2000) found high parental monitoring was associated with lower alcohol use across a 6-wave longitudinal study of randomly sampled adolescents, commencing with measures taken at 13 years of age. They also found higher monitoring reduced the upward trajectory of alcohol misuse across adolescence. Guo et al. (2001) followed 755 adolescents from age 10-21 years, and found high monitoring, as well as clearly defined rules at ten years of age, predicted lower alcohol abuse and dependence at 21 years. In this study higher monitoring was associated with lower rates of alcohol abuse (odds ratio of 0.78) using odd ratios4 adjusted for internalising and externalising behaviours at age ten years (Guo et al. 2001).
DiClemente et al. (2001) reported female adolescents, aged 14-18 years, with poor parental monitoring were 1.4 times more likely those who received closer monitoring to have a history of alcohol use. They also found lower parental monitoring increased the risk of alcohol use in the past 30 days by 1.9 times. In a cross-sectional analysis of the Australian Temperament Project dataset, Letcher and colleagues (Letcher, Toumbourou, Sanson, Prior, Smart and Oberklaid, in press) investigated the separate and combined influence of differing facets of temperament style and types of parenting behaviours in the prediction of adolescent problem behaviours.
With regard to multi-substance use, adolescents who were temperamentally low in persistence or high in negative reactivity were found to be at a greater risk if monitoring was low, indicating that low monitoring was particularly influential for those who were temperamentally at-risk. However, even when optimal parenting was evident (for example, high monitoring), prevalence of behaviour problems was generally higher among those at greatest temperamental "risk" or vulnerability (such as high volatility, reactivity, intensity). However, for adolescents with an easier temperament style, optimal compared with adequate parenting seemed to have little impact and "good enough" parenting appeared to suffice. These findings suggest that it was particularly important for monitoring to be of high quality rather than merely adequate for more difficult adolescents, whereas the presence of high versus adequate monitoring was not so crucial for less difficult adolescents.
A four-year longitudinal study with a sample of 926 children of eight to ten years of age, used survival analysis to test the sustained impact of monitoring over time (Chilcoat and Anthony 1996). (Survival analysis investigates the time that elapses between the first point of measurement and the occurrence of a subsequent event, and allows an exploration of the factors that might influence the timing of the subsequent event). Estimates from this research indicated that children in the lowest quartile of monitoring began alcohol use at a younger age than children in the higher quartiles of monitoring. Children receiving the poorest monitoring were found to be two years ahead in terms of the commencement of alcohol use (Chilcoat and Anthony 1996). This study provided strong evidence that effective monitoring of pre-adolescents can delay the onset of alcohol initiation.
In a series of longitudinal studies, parental monitoring was shown to have a direct effect on problem behaviours (including alcohol use), but also to have an important indirect effect through deviant peers (Ary, Duncan, Biglan et al. 1999; Ary, Duncan, Duncan and Hops 1999). Duncan and colleagues (1998) used sophisticated modelling techniques (multivariate latent growth curve modelling) in a two-year longitudinal study to examine the relationship between monitoring, peer associations, and problem behaviours. They found that high levels of parent-child conflict and low levels of parental monitoring were associated with deviant peer relationships and a greater likelihood of adolescent substance use. In these studies the use of substances was found to co-vary, so that an increase in one substance over time also increased the likelihood of other substance use. Individuals who experienced increasing levels of conflict with parents over an 18- month period had faster acceleration of substance use. Additionally, increases in deviant peer associations over the two-year period were associated with faster increases in substance use. Other researchers have also found the interplay between monitoring and peer association is important (Baker et al. 1999; Dishion et al. 1999; Rai et al. 2003), and this research will be examined in detail later.
Parental awareness of adolescent alcohol use
While much of the research into parental monitoring has focused on parents' knowledge of their child/adolescent's whereabouts and activities, another important aspect of monitoring in relation to adolescent alcohol use is parental awareness of their adolescent's alcohol consumption. Findings regarding parental awareness of alcohol use are now reviewed.
Research has shown that adolescents tend to spend less time with their family than when they were children, and therefore there is a greater opportunity for them to consume alcohol without parental knowledge. From age of 10 to 18 years there is a dramatic drop in the time adolescents spend in family activities, with time typically decreasing from 35 per cent to 14 per cent across this age span (Larson, Richards, Moneta, Holmbeck, and Duckett 1996).
It appears that parents do not always know the level of alcohol consumed by their adolescent children; parents also consistently underestimate their children's level of alcohol use, and they tend to underestimate adolescents' smoking and other problem behaviours too. Data from the Australian Temperament Project on this issue are shown in Figure 2. These reveal that most parents (53.6 per cent) were very sure that their 17-18 year old children had not used alcohol to excess in the past month, there were 12.6 per cent of parents who were very sure their adolescent had drunk to excess, and 11.8 per cent who were somewhat sure they had.
Parental reports of how certain they were that their adolescent had consumed alcohol to excess in the past month were then compared with their adolescent children's own reports of their alcohol consumption. These comparisons, shown in Table 6, reveal a significant difference between parental reports and adolescent consumption patterns. The table shows that 84 per cent of 17-18 year old adolescents who were abstainers also had parents who reported that they were very sure their adolescents had not drunk to excess. Of note is the data from adolescents who reported they were consuming at very high levels (on 15 or more days in the past month). In total, almost half of their parents reported they were either "very sure" or "somewhat sure" that their adolescent had not consumed alcohol to excess in the past month (26.1 per cent and 17.2 per cent respectively), although it should be noted that the information sought was not identical and hence not expected to be entirely consistent.
Figure 2. How certain are you that your teenager used alcohol to excess within the past month?
Source: Reproduced with permission of the Australian Temperament Project (2004)
| How certain are you that your teenager used alcohol to excess in past month?*** | Pattern of alcohol use in past month reported by 17-18 year old adolescents (%) | ||||
|---|---|---|---|---|---|
| No | Low | Moderate | High | Very high | |
| Has - very sure | 1.4 | 8.2 | 18.0 | 27.6 | 20.3 |
| Has - somewhat sure | 4.3 | 8.7 | 15.7 | 16.4 | 21.9 |
| Unsure/don't know | 0.0 | 5.0 | 5.5 | 5.2 | 12.5 |
| Hasn't - somewhat sure | 10.0 | 18.5 | 21.6 | 17.2 | 17.2 |
| Hasn't - very sure | 84.3 | 59.6 | 39.2 | 33.6 | 26.1 |
*** = p <.001 No use = no alcohol consumption in past month (N = 149, 13.1%). Low use = consumed alcohol on 1-4 days in past month (up to once a week) (N = 557, 48.8%). Moderate use = consumed alcohol on 5-8 days in past month (more than weekly, up to twice a week) (N = 256, 22.4%). High use = consumed alcohol on 9-14 days in past month (more than twice a week - that is,more than weekend use) (N = 116, 10.2%). Very high use = consumed alcohol on 15-30 days in past month (that is, every second day or more often) (N = 63, 5.5%)
Source: Australian Temperament Project (2004).
A recent Canadian cross-sectional study compared the responses of a large sample of 854 parents and their adolescents, aged 12-18 years. It was found that of the adolescents who reported alcohol use, only 34 per cent of their parents were aware that their adolescent had consumed alcohol (Williams, McDermitt and Bertrand 2003). The difference in agreement was very powerful (p < .00001). Further investigation of the factors that might contribute to or detract from parental awareness of alcohol use showed that greater parental awareness occurred with increased adolescent age, increased communication, and increased parental alcohol use, perhaps indicating that parental tolerant attitudes towards alcohol enabled parents to gain knowledge of their adolescents' use.
In a series of quantitative and qualitative Australian studies, it was found that parents tend to be more concerned about illicit drug use than they are about alcohol use (Taylor and Carroll 2001). Reporting on data from 404 telephone interviews with parents of teenagers, this study showed that only half the parents considered underage drinking to be a problem. Approximately half the parents reported that they found it difficult to talk with their adolescents about alcohol use, but most agreed that it is the parent's responsibility to teach their children about sensible alcohol consumption (Taylor and Carroll 2001). It was suggested by these authors that there may be a reluctant acceptance among parents that underage drinking is becoming increasingly normalised, and that parents do not feel they have the power to change this.
Research suggests that parents who feel empowered are more likely to influence their adolescents. Beck et al. (1997) found that parents who accepted the potential for their adolescents to be involved in alcohol misuse and who felt confident about their ability to intervene, were more likely to believe that alcohol misuse was a serious issue, were less likely to report that their adolescent had come home intoxicated, and were also more likely to supervise adolescent parties.
Summary
There is a considerable body of research linking parental monitoring and adolescent alcohol use. Of all the parenting factors investigated, this aspect of parenting was most consistently associated with adolescent alcohol use across both longitudinal and cross-sectional studies. The findings show that adolescents who are poorly monitored begin alcohol consumption at an earlier age, they tend to drink more, and are more likely to develop heavier drinking patterns. A second effect is also seen in that poorly monitored adolescents are more likely to associate with "deviant" peers. Parental monitoring has been studied in relation to all aspects of adolescent alcohol use - initiation, differing levels of use, and risky use or misuse.
A more specific aspect of monitoring, parental awareness of their adolescents' alcohol use, was also reviewed. The findings reveal that parents are likely to be unaware of, or to underestimate, their adolescent's alcohol consumption and are more concerned about illicit drug use than alcohol use. Australian parents may feel pressured to accept alcohol use by adolescents as "normal". For many parents, knowing the "right age" to permit their adolescents to consume alcohol, or indeed if they should permit alcohol consumption at all, was a critical question that they felt ill equipped to answer.
The studies investigating this issue focused on adolescents' current patterns of use, including levels of use. No research was found concerning the age of initiation of use, or risky use or misuse. Parents who feel empowered are more likely to share decisions about adolescent alcohol consumption and are also more likely to intervene in order to reduce consumption.
Parental behaviour management
Behaviour management as depicted in Figure 1 encompasses parents' active efforts to shape the behaviour of their adolescent. This includes the use of incentives, positive reinforcement, setting limits for appropriate behaviour, providing consequences for misbehaviour, and negotiating boundaries and rules for appropriate behaviour (Dishion and McMahon 1998). Less effective behaviour management methods include harsh and punitive discipline, or conversely, lax, inconsistent and over-permissive approaches.
Parents' positive behaviour management practices
Somewhat surprisingly, the relationship between parents' positive behaviour management practices and adolescent alcohol use has been relatively understudied to date. Furthermore, it has been difficult to disentangle the measurement of behavioural management from that of parental monitoring and parental norms for alcohol use. The relationship between behaviour management and adolescent alcohol use is likely to be complex and change over the course of adolescence. However, the large volume of more general research on parenting attests to the importance of parents continuing to reinforce behaviours that are appropriate and providing consequences to deter inappropriate behaviours.
Nevertheless, the program of research from the Seattle Social Development Project, using a sample of 808 adolescents followed from childhood to adulthood (Guo et al. 2001; Kosterman et al. 2000; Oxford et al. 2001), has consistently demonstrated the importance of a range of positive parental practices. Thus, family standards and rules, parental monitoring, and adolescent family attachment were all found to be important in delaying alcohol initiation in early adolescence, even after the influence of deviant peers was taken into account. Furthermore, parental rules, rewards for good behaviour, a strong values system, and well developed negotiation skills when adolescents were aged 10-16 years, predicted lower alcohol abuse and dependence at the age of 21 years.
Harsh parenting/conflict
Research indicates that harsh parenting or discipline and high levels of conflict are connected to adolescent alcohol use, but that the links are often indirect and exerted through their impact on other parenting behaviours such as parental monitoring (Ary et al. 1999a; Ary et al. 1999b; Brody and Ge 2001). Two longitudinal studies by Ary and colleagues (1999a and 1999b), for example, showed that families with high levels of conflict tended to have lower levels of parent-child involvement, leading to lower levels of parental monitoring one year later. At this later time point, poor parental monitoring was a powerful predictor of adolescents' engagement in substance use. Using a 3-wave longitudinal study, Brody and Ge (2001) showed that harsh-conflicted parenting was relatively stable over time, and that youth self-regulation (an aspect of temperament) mediated the pathways between this type of parenting at wave 2 and adolescent alcohol use at wave 3. However, one study (Duncan, Duncan, Biglan and Ary 1998) has revealed direct and indirect connections between parent-child conflict (along with poor parental monitoring) and levels of substance use among 664 adolescents aged 14-17 years, as well as an escalation in the trajectory of substance use over time.
Parental permissiveness towards adolescent alcohol use
International research has found that parental permissiveness towards adolescent alcohol use is related to increased use. The term "parental permissiveness" is used to refer to parents who permit adolescents to drink when they are under the legal age and does not imply a more general lack of discipline across several parenting areas.
Wood et al. (2004) found that where parents were more permissive towards alcohol use (measured as "no permission for adolescents to drink alcohol at home" through to "no limits on adolescent alcohol use at home"), their adolescents were more likely to engage in heavy binge drinking. Parental permissiveness also appeared to influence peer associations, with a significant relationship between peer influence and alcohol use demonstrated when parents were permissive.
Similarly, in their Queensland study of 320 rural adolescents with an average age of 15.8 years, Williams and Hine (2002) measured the role of parental attitudes towards their adolescent's alcohol use in mediating the impact of more global parental permissiveness in the prediction of adolescent alcohol misuse. They found that parental permissiveness and family alcohol use were indirectly related to adolescent misuse, as they were mediated by parental and significant others' level of approval of the adolescent's alcohol use. Thus parental attitudes concerning alcohol use appeared in this research to have a more influential role than more general parental permissiveness.
Parental authority
Adolescents who rebel against parental authority (that is, when parental behaviour management is ineffective or fails) are very likely to use alcohol. In a cross-sectional study of 959 adolescents which measured adolescents' intention to use alcohol, Jackson (2002) found adolescents who denied parental authority were four times more likely to be current drinkers.
This research also showed that adolescents who received authoritarian parenting (high levels of direction, control, and punishment) were six times more likely to deny parental authority than adolescents who were parented in an authoritative style (high warmth and support together with appropriate limit-setting and explanation). Similarly, adolescents who experienced distant parenting (low engagement, low connectedness) were 2.5 times more likely than those who received authoritative parenting to deny parental authority. In this study, authoritarian or distant parenting was associated with greater adolescent rebelliousness, which in turn was related to alcohol use. Somewhat surprisingly, no significant relationship was found between a permissive parental style (high warmth but few demands or restrictions) and adolescent alcohol use.
Somewhat overlapping with the literature on monitoring, the importance of parental knowledge about adolescents' use of free time has been shown in a recent study which measured the use of negotiated unsupervised free time with 692 adolescents (average age of 15.7 years) (Borawski et al. 2003). Negotiated unsupervised time was where adolescents reported being able to stay out past curfew provided they call home first, or being allowed to have a friend at home when parents are not there, providing parents were asked beforehand. This study found that when male adolescents were able to negotiate more unsupervised time they were 1.85 times more likely to drink alcohol, while female adolescents were 1.58 times more likely to drink. While some aspects of parental behaviour measured in this study appear to indicate monitoring attempts (for example, the requirement for adolescents to inform parents of adolescents' activities), another aspect, the agreement to permit unsupervised free time, could indicate permissiveness or low behavioural management and emerged as particularly influential.
Parenting style
Parenting style is a term commonly used to draw together clusters of parenting behaviours that are thought to co-occur. These encompass aspects of parental behaviour management practices, and discussion of this type of parenting has therefore been placed in this section.
Four family-parenting styles are thought to relate to differing child outcomes (Mandara 2003). Cohesive-Authoritative families exhibit cohesion and low conflict in family interactions, and are not over controlling. Conflictive- Authoritarian families have low family cohesion, use authoritarian, harsh discipline, and are controlling. Defensive-Neglectful type families display chaotic family functioning, and have very little control, warmth, or cohesion. Finally, the Permissive type is highly responsive but low in control.
Cohesive-authoritative parenting is purported to be the optimal approach, and this style has been correlated with positive adolescent psychological adjustment across several studies (Baumrind 1991; Mandara 2003; Steinberg, Mounts, Lamborn and Dornbusch 1991). As reported earlier, Jackson (2002) showed that adolescents who were parented in an authoritative style were less likely to deny parental authority than adolescents who were exposed to authoritarian or distant parenting. Denial of parental authority was in turn associated with higher alcohol use.
The Australian Temperament Project has shown that some aspects of an authoritative parenting style interacted with adolescent temperament style to predict substance use (Letcher et al., in press). This recent cross-sectional analysis of the Australian Temperament Project data at an adolescent age of 13-14 years, found that parental warmth was not significantly related to substance use, and only parental monitoring was a direct contributor. Hence, only one aspect of an "authoritative" parenting style appeared influential. Earlier United States research by Baumrind (1991) found that global parenting style was significantly associated with lower use. Thus, when parents were highly demanding as well as highly responsive there was a reduced likelihood that adolescents would exhibit problem substance use behaviours, compared to parents who were more likely to be lax, unsupportive, disorganised or under stress.
Parental supply of alcohol
Adolescents' levels of alcohol use are related to their source of access, and the location in which alcohol is consumed. As well as introducing adolescents to alcohol in the relatively safe home environment, parents may provide adolescents with alcohol to take to social events as a means of controlling the amount consumed. Thus, parents may supply alcohol as a means to guide responsible alcohol use.
The ASSAD data shows that both younger and older adolescents drink significantly less alcohol when they obtain it from their parents than when they obtain it from friends or someone else. As shown in Table 7, when 12-15 year old adolescents obtained alcohol from home they consumed 3.6 drinks per week, compared with 4.9 drinks if alcohol was obtained from a friend. When 12- 15 year old adolescents obtained alcohol from someone else they consumed a relatively high average number of 7.6 drinks per week, or 110 per cent more. Similar effects are seen for the 16-17 year old group, although to a lesser degree. At this age there was little difference in consumption according to whether alcohol was obtained from home or from friends, but consumption levels rose by 56 per cent when alcohol was obtained from someone else.
In terms of the location in which alcohol was consumed, the ASSAD data showed that students drank less when they consumed alcohol at home compared with at their friends' homes or at parties. (White and Hayman in press). Table 7 shows that when 12-15 year old adolescents consumed alcohol at home, the average number of drinks per week was 3.4, compared with 6.4 drinks at a party or 6.3 at a friend's home, representing an approximately 90 per cent increase.
| 12-15 years | 16-17 years | Overall 12-17 years | |
|---|---|---|---|
| Where obtained* | |||
| Parent's home | 3.6 | 6.0 | 4.4 |
| Friend's home | 4.9 | 6.8 | 5.6 |
| Someone else | 7.6 | 9.4 | 8.5 |
| Where consumed* | |||
| Home | 3.4 | 6.3 | 4.3 |
| Party | 6.4 | 8.9 | 7.5 |
| Friend's place | 6.3 | 9.1 | 7.5 |
| * = p < .01 | |||
Source: White and Hayman (in press).
For the 16-17 year olds, a similar increase was evident, with adolescents consuming approximately 40 per cent more when they drank at a friend's home or at a party than when they drank in their own home. While these findings examine levels of use, it remains unknown whether the nature of drinking differs across the various locations. For example, drinking at home may be spread across a number of days and occur at low levels per day, whereas drinking at parties or friends' homes may occur on a smaller number of days and involve binge drinking.
In contrast, another study has shown that children who are allowed to drink alcohol at home when young may consume more alcohol later on. Jackson et al. (1999) used a predictive study design to measure connections between Grade 5 children's perceptions of their parent's socialisation practices concerning alcohol and children's subsequent alcohol use in Grade 7. The odds of the children consuming alcohol in Grade 7 were 2.1 times greater among those who perceived that they were allowed to have a drink of alcohol at home at an earlier age.
This finding demonstrated that parental socialisation that included disapproval of early age drinking was associated with a decreased likelihood that children would have commenced drinking two years later. However, with only one study to support this finding, further examination is required. Nevertheless, it appears that connections between young people's alcohol use at home and their more general propensity to use alcohol may be complex, and influenced by the age of the child, and parents' attitudes towards young people's alcohol use, among other factors.
Summary
Parental behaviour management encompasses positive practices such as the use of incentives, positive reinforcement, setting limits for appropriate behaviour, providing consequences for misbehaviour, and negotiating boundaries and rules for appropriate behaviour, as well as less effective strategies such harsh and punitive discipline, high conflict, lax, inconsistent or over permissive approaches.
While there has been limited investigation of positive parental behaviour management in relation to adolescent alcohol use, the research from the Seattle Social Development Project demonstrates that family standards and rules, rewards for good behaviour, and well developed refusal skills were associated with lower initiation of alcohol use in early adolescence, and lower rates of alcohol abuse and dependence in early adulthood.
Regarding less effective parent management approaches, harsh discipline and high conflict were associated with higher rates of alcohol and substance use, although the majority of research indicated that the effects of these practices were indirect, and exerted through their impact on parental monitoring. Further, the research showed that when parents were openly permissive toward adolescent alcohol use, adolescents consumed more alcohol.
Additionally, adolescents who rebelled against parental authority (that is, when parental management of adolescent behaviour was ineffective or failed) were found to more often consume alcohol. Adolescents who gained unsupervised free time (even with parental knowledge and permission), also tended to more frequently use alcohol.
Most research on the above parenting factors has focused on initiation, levels of use and high risk use.
Although research into broad parenting styles is richly descriptive and useful for considering the overall parenting environment, it can be difficult to determine which aspects of particular styles (authoritative, authoritarian, neglectful and permissive) are important for reducing adolescent alcohol use. However, it seemed that an authoritative style of parenting was associated with lower adolescent alcohol use, while authoritarian and distant parenting styles were associated with higher levels of use. It may be more advantageous to break parenting "style" down into those components that might be amenable to change when applying these findings to intervention programs designed to change parenting behaviours.
Australian research has shown that on occasions when parents are aware of their adolescents' alcohol use and they actively engage with their adolescents in the purchase or provision of alcohol, then their adolescents consume less. Furthermore, adolescents tend to consume less alcohol when they drink at home, by comparison with at a friend's home or other social occasion. However, it is as yet unknown whether adolescents' drinking intentions and practices differ according to whether they are at home, or another venue. That is, do adolescent simply drink less at home because they have different drinking intentions? It is possible that consuming alcohol at home is more controlled, but this more moderate consumption may not generalise to consumption at parties or with friends. Additionally, the extent to adolescents' alcohol consumption at home takes place under parental supervision is not known.
One study found that when children were not permitted to drink alcohol at home this appeared to have a subsequent protective effect, reducing the likelihood that they would have commenced alcohol use two years later in early adolescence. Thus, the association between adolescents' alcohol consumption in the home environment and their more general propensity to consume alcohol may be complex, and likely to be affected by factors such as the child's age, and parents' attitudes towards adolescent alcohol use. The research concerning parental supply of alcohol has focused predominantly on levels of use, although one study investigated the initiation of alcohol use in early adolescence.
Relationship quality
Parent-adolescent relationship quality underpins all the aspects of parenting discussed above. Relationship quality is the product of an ongoing interplay between parents and adolescents, and affects, and is also affected by, these other aspects of parenting. For example, without a warm relationship, adolescents are more likely to resist monitoring, while authoritative parenting may contribute to and enhance strong parent-adolescent relationships. Thus, the findings concerning parent-adolescent relationship quality reviewed here will also reflect the contribution of other aspects of parenting, and vice versa. Whether intervention attempts should focus directly on the parent-adolescent relationship, other aspects of parenting, or both, is an important consideration, which is addressed in Section 9.
Parent-adolescent relationship quality forms the core of the Dishion and McMahon (1998) model, attesting to its fundamental importance. While it is often assumed that adolescence is a time of storm and stress, characterised by conflict with parents, research has shown that this level of disruption is not typical. Transformation, rather than storm and stress, is a more apt way of considering how parent and adolescent relationships might change during adolescence. Research has shown that while established patterns of family relations undergo change (Robin and Foster 1989), when adolescents report feeling close to their parents they consistently score higher on measures of psychological development, behavioural competency, self-reliance, and report lower rates of psychological and social problems (Armsden and Greenberg 1987; Steinberg 1990).
Australian Temperament Project findings show that both parents and adolescents report positive parent-adolescent relationships (Sanson, Letcher and Smart 2003). For example, 64 per cent of parents reported that they got on "very well" with their 13-14 year old adolescent and a further 26 per cent got on "well", with similar rates of 53 per cent and 35 per cent reported by adolescents, respectively. Furthermore, at 16-17 years, approximately two-thirds of adolescents and parents reported that they "seldom" or "never" had disagreements (Prior et al. 2000). Steinberg (1990) found that only 5-10 per cent of families experience dramatic deterioration in the quality of relationships during adolescence, and that marked deteriorations in parent-adolescent relationships are highly correlated with prior family problems. These results therefore suggest that if relationships in the family are strong, parents should continue to have an influence on the alcohol consumption patterns of their adolescents.
Adolescent perceptions of parental care have been shown to influence their propensity to drink alcohol. In an Australian study with 493 Australian secondary students, with an average age of 16.2 years, adolescents who misused alcohol were significantly more likely to report lower parental care (Mak and Kinsella 1996). Because this was a cross-sectional study, it is not possible to tease apart the direction of effects - that is, whether perceived lower care preceded alcohol misuse or was a result of it.
International research has shown that good quality parent-adolescent relationships are associated with lower drinking. Bray, Adams, Getz and Baer (2001) used statistical modelling (Hierarchical Linear Modelling) in a longitudinal study with 7540 adolescents over three years, to examine patterns of adolescent substance use alongside parent-adolescent relationships. They found that adolescents with increasing across-time levels of alcohol use more frequently experienced relationship difficulties (detachment, emotional separation, and emotional difficulties), and also reported more family conflict and higher stress. Conversely, adolescents characterised by decreasing across time alcohol consumption had more positive relationships (greater emotional autonomy, less family stress, and less conflict). In this latter situation, parental monitoring became less influential.
Parent-adolescent relationship quality is also associated with adolescent temperament, and both were found to be predictive of adolescent alcohol use. Neighbours and colleagues (2000) tested the importance of parent-adolescent relationship quality, a difficult temperament style, and alcohol use disorders in a cross-sectional study involving 438 adolescents aged 12-18 years (average age 15.8 years). A difficult temperament style was found to predict problematic alcohol use for both males and females, and was also negatively associated with relationship quality.
However, there were specific associations between parent-adolescent relationship quality, gender, and alcohol misuse. For males, relationship quality mediated the effect of temperament on alcohol misuse (a good parent-adolescent relationship reduced the contribution of temperament to alcohol misuse); but for females, relationship quality and temperament separately predicted alcohol use disorder, and high quality relationships did not reduce the effect of temperament on alcohol use. The authors hypothesised that parents may have struggled to engage male adolescents who possessed a difficult temperament style in family activities and to maintain open communication, which may then have limited their capacity to influence their sons' alcohol use and association with deviant peers. However, high quality relationships with parents were not protective against high risk alcohol use for females who possessed a difficult temperament style, and the authors hypothesised that other intra-individual characteristics (for example, maladaptive coping, low self-esteem) may have been involved.
It was shown earlier that good parental monitoring is a key factor related to adolescent alcohol use. A recent Australian study involving parents and adolescents revealed that better quality parent-adolescent relationships were predictive of and appeared to underpin higher parental monitoring (Hayes 2004). This study suggested that good parent-adolescent relationships are a necessary prerequisite for monitoring to occur. The longitudinal work of Barnes and colleagues (2000) has also shown that broad parental support may directly contribute to parental monitoring, which in turn has a direct influence on adolescent alcohol use. Barnes and colleagues contend that children who are reared in supportive environments are likely to have better relationships, and they will therefore receive better monitoring and have lower rates of alcohol misuse.
Several longitudinal studies (Ary et al. 1999b; Barnes et al. 2000; Brody and Ge 2001) also suggest that parent-adolescent relationship quality has an indirect influence on adolescent alcohol use, through its impact on parental monitoring and deviant peer associations.
Summary
The quality of parent-adolescent relationships is a key factor that influences all interactions between parents and adolescents. When parents are able to maintain a quality relationship with their adolescents, they are likely to communicate about alcohol use and experience less conflict surrounding adolescent behaviours. Further, key parenting behaviours such as parental monitoring and behaviour management skills are dependent on the quality of parent-adolescent relationships.
The reviewed research suggests that high quality parent-adolescent relationships are associated with lower levels of adolescent alcohol use, as well as lower rates of problematic use and misuse. Additionally, adolescents exhibiting escalating patterns of alcohol use report greater parent-adolescent relationship difficulties, while those who displayed decreasing patterns of alcohol consumption report more positive relationships. While these studies demonstrate links between relationship quality and levels of alcohol use and high risk patterns of use, there has been little research into connections between relationship quality and the initiation of alcohol use.
Parental norms
The final area of parenting highlighted by the Dishion and McMahon (1998) model is parenting norms, values and goals. These refer to parents' belief systems, attitudes and conceptions concerning adolescent behaviour. Patterns of adolescent alcohol use have been found to vary across Australia and the United States (see Section 3) and, as discussed later in Section 6, there is evidence of stronger anti-alcohol values and attitudes in the United States, which may contribute to differing alcohol use patterns across the two countries. These trends emphasise the potential importance of parental norms and values.
Parental attitudes towards adolescent alcohol use
Data from the Australian Temperament Project show that the great majority of parents (83.5 per cent) of 17-18 year old adolescents reported that their adolescents were allowed to drink alcohol at home. The age that parents reported they first allowed their adolescents to drink alcohol at home is shown in Figure 3. Parents most frequently reported that adolescents had first been permitted to have a glass of alcohol (not just a sip) at home at 16 or 17 years.
The age that parents first allowed their adolescent to take alcohol to parties is shown in Figure 4. The most common age is also 16-17 years; however, a large number of parents (35.8 per cent) continued not to permit their adolescents to take alcohol to parties at the time the survey was completed (child age of 17-18 years), and very few (2.6 per cent) reported that they had allowed their adolescent to take alcohol to social events at 15 years or younger.
Other research shows that parents and adolescents differ on their perceptions of the appropriate age to drink alcohol. In a recent Australian study (Wilks and McPherson 2002) with 290 parents and 196 adolescents, similarly to the Australian Temperament Project, it was reported that parents perceive male and female adolescents should be able to drink alcohol when they are around 18 years of age. Not surprisingly, adolescents reported a lower age, perceiving that they should be allowed to drink alcohol approximately 18 months earlier at the age of 16.5 years.
This study was a replication of a previous administration of this survey completed in 1986, with 771 adolescents and 1482 parents (Hudson, Bell, Hudson, and Houndoulesi 1986). Comparisons show there has been little change over this 12- year period in parental reports of the appropriate age in which adolescents should drink alcohol. However, the perceptions of adolescents appear to have changed. In the earlier 1986 data, adolescents perceived that males should be allowed to drink at 16.8 years, and females at 17.1 years. Although this change in age was not statistically significant, there is some indication in this data that adolescents may be inclined to perceive that they should be allowed to drink alcohol at an earlier age than they had previously.
Figure 3. Age when parents first allowed adolescents to have a glass of alcohol (not just a sip) at home

Source: Reproduced with permission of the Australian Temperament Project (2004)
Figure 4. At what age did you let him/her take alcohol to a party or social event?
Source: Reproduced with permission of the Australian Temperament Project (2004)
Parental approval or disapproval of adolescent alcohol use
Parental disapproval of alcohol use appears to result in lowered drinking patterns. In an Australian study with 650 students from Years 7, 9, and 11 (Smith and Rosenthal 1995), parental disapproval was found to have a significant negative effect on adolescent drinking behaviour. There were also age effects, with parents inclined to be more approving of adolescent alcohol use with the advancing age of the students (Smith and Rosenthal 1995).
The Australian Temperament Project asked parents to report their tolerance of their adolescents' alcohol use, and compared these to adolescents' reports of alcohol consumption. This data showed that adolescents who drank alcohol were significantly more likely to have parents who allowed them to drink at home. The great majority (93.5 per cent) of the adolescents who reported that they drank alcohol at very high levels were allowed to drink at home. Similarly, the great majority of low (84.5 per cent), moderate (89.0 per cent), and high drinkers (93.2 per cent) were also allowed to drink at home. Of note is the difference in parental tolerance amongst the abstainers, with only 58.6 per cent of parents of these adolescents reporting that their adolescent was allowed to drink alcohol at home.
Australian Temperament Project data also revealed that there was a significant relationship between the age at which parents first allowed their adolescents to drink alcohol at home and the amount of alcohol the adolescents consumed at 17-18 years of age. The pattern of alcohol use reported by adolescents was broken down into five categories ranging from "no use" to "very high use". Figure 5 shows that, compared with adolescents from the other four groups, fewer of the group who were abstainers at 17-18 years had been permitted to drink alcohol at home over the period of 12-18 years, and many (44 per cent) were still not permitted to drink at home in late adolescence (17-18 years). Differences between the remaining groups were less marked, although a trend for a higher proportion of those who later drank at very high levels to be permitted to drink at home at 16 years was noticeable.
Figure 5. The age at which parents allowed adolescent to drink at home by patterns of adolescent alcohol use at 17-18 years of age
No use = no alcohol consumption in past month (N = 149, 13.1%). Low use = consumed alcohol on 1-4 days in past month (up to once a week) (N =557, 48.8%). Moderate use = consumed alcohol on 5-8 days in past month (more than weekly, up to twice a week) (N = 256, 22.4%). High use = consumed alcohol on 9-14 days in past month (more than twice a week - that is,more than weekend use) (N = 116, 10.2%). Very high use = consumed alcohol on 15-30 days in past month (that is, every second day or more often) (N = 63, 5.5%).
Source: Reproduced with permission of the Australian Temperament Project (2004)
International research confirms the influence that parental norms have on adolescent alcohol use. Wood et al. (2004) compared the importance of parental and peer norms among a sample of 556 adolescents (mean age of 18.1 years) using a cross-sectional methodology. They found that when parents reported greater disapproval of heavy drinking among adolescents (and also higher parental monitoring), their adolescents were less likely to engage in heavy binge drinking. In a test of the Social Development model, Sale et al. (2003) found that parental attitudes toward substance use had a direct effect on adolescent substance use (cigarette, alcohol and marijuana), and were also related to the attitudes of their teenager's peers. A one-year study conducted using parent and adolescent telephone interviews found that parental communication about alcohol was not related to the initiation of drinking (Ennett et al. 2001) but instead parental approval was related to the escalation of drinking, with parents who showed less disapproval having adolescents who were 1.9 times more likely to also have escalating drinking behaviours.
It appears that for some adolescents, the opinions of their parents toward alcohol use are important mediators of their decision to use alcohol. Beck et al. (2003) found that parental monitoring had the strongest influence on adolescent drinking behaviours, but that the likelihood that adolescents had obtained alcohol without parent knowledge or had consumed alcohol in the past three months decreased when adolescents reported that their father's opinion was important to them (odds ratio .55, and odds ratio .50 respectively).
It is important to also consider that parental norms for alcohol use, like all previously mentioned parenting factors, are not static and are likely to change with adolescent development. Smith and Rosenthal (1995) found a significant inverse relationship between adolescents' age and their perceptions of parental disapproval of drinking. The studies investigating parental norms cited above did not investigate age effects. Recalling the assumptions adopted for this review, that parent-adolescent influence is bi-directional, this would suggest that over time the developmental changes and increasing independence of adolescents would exert some change on parents' attitudes toward alcohol use, although to date the relationship of parental norms and age has not been thoroughly investigated.
Parental concern about adolescent alcohol use
The majority of parents participating in the Australian Temperament Project did not worry about their adolescents' alcohol consumption. Table 8 compares parents' reports of how much they worry about their adolescent's drinking with adolescent reports of alcohol use at age 17-18 years. Overall there was a significant effect found. The majority (88 per cent) of adolescents who reported that they did not drink alcohol at all also had parents who did not worry about alcohol use. Of the adolescents who reported drinking at very high levels, 42 per cent of their parents reported that they did not worry about their adolescent drinking, and 53 per cent reported that they worried "a little". Very few parents reported that they worried "a lot", irrespective of the alcohol use of their adolescents. These trends are consistent with the previously discussed Australian Temperament Project findings that parents tended to be unaware of the extent of risky alcohol consumption undertaken by their adolescents.
| Do you worry about his/her drinking?*** | Pattern of alcohol use in past month reported by 17-18 year old adolescents (%) | ||||
|---|---|---|---|---|---|
| No | Low | Moderate | High | Very high | |
| No | 87.8 | 64.7 | 53.8 | 47.8 | 41.9 |
| A little | 12.1 | 32.6 | 42.5 | 44.2 | 53.2 |
| A lot | 0.0 | 2.7 | 3.6 | 8.0 | 4.8 |
| *** = p < .001 No use = no alcohol consumption in past month (N = 149, 13.1%). Low use = consumed alcohol on 1-4 days in past month (up to once a week) (N = 557, 48.8%). Moderate use = consumed alcohol on 5-8 days in past month (more than weekly, up to twice a week) (N = 256, 22.4%). High use = consumed alcohol on 9-14 days in past month (more than twice a week - that is,more than weekend use) (N = 116, 10.2%). Very high use = consumed alcohol on 15-30 days in past month (that is, every second day or more often) (N = 63, 5.5%). | |||||
Source: Australian Temperament Project (2004).
Summary
Overall, the findings from Australian and international research suggest that parental norms, attitudes, and beliefs with regard to adolescent alcohol use have an important influence on adolescent alcohol consumption. When parents show disapproval, their adolescents are less likely to drink, and conversely, when parents are tolerant or permissive, their adolescents are likely to drink more. Parents tend not to worry very much about their adolescents' use of alcohol, even when adolescents reported high rates of use. This finding was consistent with earlier reviewed research which suggested that parents tended to be unaware of the extent of alcohol consumption undertaken by their adolescent.
Parents and adolescents differ somewhat in their perceptions of the appropriate age at which adolescents should be permitted to consume alcohol, with several studies suggesting that parents believed 17 years was an appropriate age for adolescents to begin consuming alcohol at home. Adolescents tended to believe this should occur earlier at approximately 16 years. These perceptions are somewhat inconsistent with actual trends, which suggest that alcohol initiation commonly begins at an earlier age.
The research concerning the impact of parental norms, attitudes and values has generally focused on their relevance for levels and rates of use, patterns of escalation, and associations with high risk use. Although there is research into parental and adolescent perceptions of the appropriate age at which adolescents should commence alcohol use, studies have not yet tested whether these attitudes align with the actual onset of alcohol use, and these beliefs are clearly inconsistent with population-level trends for most young people to have commenced using alcohol by 14-15 years of age (see Section 3).
Summary of parenting influences on adolescent alcohol use
Up to this point, this review has demonstrated that parenting behaviours can have a direct influence on adolescent alcohol use. The majority of research has shown that parental monitoring is the most proximal parenting behaviour associated with adolescent alcohol use. It has also been demonstrated that several other parenting behaviours are associated with alcohol use, with associations seen when parents express disapproval, set limits, or actively manage their adolescent's alcohol consumption.
This review has also shown that parental norms for adolescent alcohol use can have a significant impact on consumption; however, the research has not been clear on whether parental norms for drinking exacerbate risky drinking behaviours or reduce them. Finally, it was shown that the relationship of parents and adolescents can have a global impact, and is likely not only to influence adolescent alcohol use, but also influence parental behaviour management and monitoring.
3. The terms "deviant peers", "deviant peer affiliations", and "deviant peer associations" have been widely used in the research literature to refer to peers who engage in substance use or antisocial behaviour. These terms do not imply participation in more extreme types of deviant activities. While recognising that the terms are less than ideal, they will continue to be used here, as they are in such widespread use and no better alternatives could be found.
4.The odds ratio for a variable denotes the change in the odds of being in the outcome group (for example, alcohol use) for each change in the level of that variable (for example, parenting factor). An odds ratio of 1 represents no change in risk (odds are the same at any level of the variable). Odds ratios significantly greater than 1 indicate an increased risk at increased levels of the variable, while odds ratios smaller than 1 indicate a decreased risk at higher levels of the variable. Thus, with regard to parental monitoring, the odds ratios suggest that as monitoring increases, rates of alcohol use and abuse decrease.
5. Parental, family, and broader environmental factors
In addition to parenting behaviours, there are other ways in which parents may influence their adolescent's alcohol use. The aspects to be reviewed here range from individual parental characteristics (such as parental alcohol use) to broader contextual and cultural influences. As made clear by ecological models of development (for example, Bronfenbrenner 1992) and more specific approaches such as the Social Developmental Model, it is important to consider the broader social context in which families are embedded, including cultural norms and values, laws concerning adolescent alcohol use, and the applicability of the findings to particular communities and sub-groups.
This review thus now turns to an examination of the research on parental and family characteristics and their relationship with adolescent alcohol use. The following sections examine parental consumption of alcohol, risky parental alcohol use and alcohol dependence, followed by family structure, and family socio-economic background, the role of differing cultural norms and legal systems, and findings regarding Indigenous adolescents.
Parental factors
Regular parental alcohol consumption
Parents' own use of alcohol is related to adolescents' alcohol consumption. An Australian cross-sectional study (Quine and Stephenson 1990), with 2336 primary school children in Grades 5 and 6, found that even young children were significantly more likely than other children to have the intention to drink, or to have drunk a glass of alcohol, if their parents drank at least weekly. They were also more likely than other children to accept a glass of alcohol from a friend if their parents drank at least weekly.
With regard to drinking behaviour, as opposed to intentions, the importance of parents and peers was shown in a sub-sample of these children. From the sample of 2336 children, there were 720 children classified as either occasional or more frequent drinkers. These children were significantly more likely to drink frequently if a close friend also drank, more likely to drink if a sibling drank, and the significance of parental drinking was third in importance (Quine and Stephenson 1990). Thus in this study the intention to drink appeared to be primarily influenced by parental behaviour, but for actual drinking behaviour (as opposed to intentions) parental influence was ranked third, after the influence of peers and siblings.
An analysis within the Australian Temperament Project (Prior et al. 2000) found that while the most significant predictor of substance use at age 15-16 years was antisocial behaviour at 13-14 years; substance use was also associated with maternal smoking and drinking, as well as poorer attachment to parents, and other child characteristics such as thrill-seeking.
Some research suggests that when parents use alcohol frequently, their adolescents have an increased likelihood of being exposed to alcohol-related risk behaviours. In a survey of 658 Victorian students aged 16-17 years, Bonomo et al. (2001) found adolescents who had experienced an alcohol-related injury were 1.8 times more likely than other adolescents to have parents who drank alcohol daily. (There was also a significant relationship with sexual risk-taking behaviour, with adolescents who reported sexual risk-taking behaviours being 3.1 times more likely than other adolescents to report that their parents drank daily).
Further analysis of data from the Australian Temperament Project for the present review also revealed significant associations between maternal and paternal drinking patterns (as reported by the mother), and the level of alcohol use reported by the adolescent. Adolescents who reported that they did not drink were more likely to have parents who reported that they were occasional or non-drinkers, while adolescents who drank at very high levels were more likely to have parents who reported that they were occasional or frequent drinkers. There was also a significant association between parental alcohol use and allowing adolescents to take alcohol to parties, with those parents who were non-drinkers less likely to give permission for their adolescent to take alcohol to parties.
It is possible that frequent parental alcohol use might affect the parenting behaviours that were shown previously in this review to be most proximal to adolescent alcohol use. In international research, an important longitudinal body of work by Dishion et al. (1999) has found that parental substance use does not show unique influence, after controlling for parenting practices or peer influence, and these authors argue that it is parenting skills and behaviour management that have the most direct influence on adolescent behaviour. Using the parenting framework of Dishion and McMahon (1998) to interpret these findings, it could be inferred that a range of parental behaviours might change as a result of frequent parental alcohol use. For example, it may be that parents who drink alcohol daily may be less likely to monitor their adolescents' free time, or to have beliefs supporting young people's early alcohol initiation, or they may have poorer relationships with their adolescents. These are areas that warrant further investigation.
Alternatively, research has suggested that there may be an educative modelling role in responsible parental drinking. For example, Johnson and Johnson (2000) suggest that controlled parental alcohol use may have a buffering effect when used within ritualised family practices. There may also be different associations between the use of alcohol by mothers and fathers. For example, Chassin and colleagues (1993) found that there was a direct relationship between mother's current use and adolescent alcohol use, but not father's current use. To understand these issues it is necessary to identify the impact of specific parental drinking patterns on adolescent drinking, and the influence of parental alcohol use on parenting behaviours in general, and parent-adolescent relationships in particular.
Parental alcohol abuse
With regard to parental alcohol abuse, the research has taken two directions, and has examined either the biological propensity for abuse, or the social and behavioural learning links. Each of these will be reviewed in turn.
Research has demonstrated significant biological links between parental alcohol abuse and the alcohol use of their children. In a summary of the key research on these biological associations, Hawkins et al. (1992) reported that research has demonstrated some genetic differences in alcohol responses in the children of adults who are dependent upon alcohol. Twin studies have shown that male children of such individuals have a greater likelihood of alcohol abuse (discussed in Hawkins et al. 1992). Adoption studies, too, have shown consistent evidence for the genetic transmission of alcohol dependence to male children, with rates of dependence of 18 per cent to 27 per cent among male offspring (Hawkins et al. 1992). However, as Hawkins and colleagues (1992) point out, approximately half the adults hospitalised for alcohol dependence do not have a history of family alcohol abuse, suggesting that biological linkages are not pervasive.
However, parenting behaviours and skills that have been discussed previously may have a greater impact on adolescent alcohol use than biological propensities. The greatest effect of parental alcohol abuse is likely to come from disrupted parent-adolescent relationships. For example, in a matched sample comparing families with at least one biological parent who was dependent on alcohol to a control group with no dependence, the biological effect on adolescent alcohol use was mediated by the child's stress level (Chassin et al. 1993). This study showed that parental alcohol dependence increases the child's stress, and this stress is directly related to negative affect, associations with deviant peers, and increased use of alcohol.
Similarly, the longitudinal modelling of Barnes and Farrell (1992) (using latent growth modelling) revealed that parental alcohol abuse had an indirect effect on adolescent alcohol use, and was mediated through parental support and parental monitoring. They also reported that adolescent orientation to peers had a significant impact. The peer orientation factor measured whether adolescents were more likely to choose the views of their peers, rather than their parents. In this study, when adolescents had a familial history of alcohol abuse plus a high regard for peers, the adolescent was more likely to develop regular drinking patterns.
Other researchers have investigated adolescents' internalised cognitions toward alcohol, and have found that parental consumption is associated with adolescents having positive attitudes towards alcohol, even when the parents abused alcohol. For example, in a sample of 97 adolescents aged 12-18 years, Brown and colleagues (1999) found that adolescents who were exposed to familial alcohol dependence tended to have positive attitudes toward alcohol in general, and positive expectancies for the effects of alcohol on social behaviour, sexual enhancement, relaxation, and tension reduction. Surprisingly, exposure to parental alcohol dependence did not predict negative alcohol expectancies in these adolescents. The findings from this study highlight the importance of learning and modelling processes in the expectancies adolescents develop about alcohol consumption. They also showed that adolescents from alcohol-abusing families did not develop more negative attitudes towards alcohol use.
Summary
The research reviewed reveals that parents' own use of alcohol increases the likelihood that adolescents will also consume alcohol. Australian research has shown that parental alcohol use is also associated with greater alcohol-related risk behaviours in adolescents. Other research suggests that parental alcohol use impacts indirectly, by changing parental management skills. Although limited, some alternative research suggests that controlled parental alcohol use may have a buffering effect when used within ritualised family practices.
Biological links between parental alcohol dependence and adolescent alcohol use have been found. Additionally, other research indicates that parental alcohol dependence has indirect effects on adolescent alcohol use, through the changes it exerts on parenting behaviours and socialisation patterns. Exposure to parental alcohol abuse has been shown to influence adolescent attitudes toward alcohol, and appears to result in positive, rather than negative, attitudes. The studies reviewed have examined adolescent levels of use, risky use and abuse, with connections between parental alcohol use or alcoholism and adolescents' initiation of alcohol use under-studied at present.
Broader family factors
Family structure
The association between family composition and adolescent alcohol use has not been widely investigated. One very large well-designed European study was located that investigated this issue amongst 34,001 adolescents aged 15-16 years (Bjarnason et al. 2002). This cross-cultural study over 11 European countries used random sampling to select schools and classes, and all students present on the day completed the questionnaire (86-92 per cent response rate). A significant positive effect was found for adolescents who lived with both biological parents (intact families). These adolescents had reduced frequency of heavy drinking, when compared with single mother, single father, or blended families. Interestingly, the positive effect of belonging to an intact family was stronger in the societies where adolescent culture favoured heavy drinking.
In the New Zealand Christchurch cohort, early family breakdown was associated with heavier alcohol use at age 14 and this effect was maintained after adjusting for age 8 conduct problems and earlier age of first alcohol use (Fergusson et al. 1995). Although no Australian studies on family composition were found, previous longitudinal research has linked family breakdown as an independent risk factor for the development of youth substance use (Coffey, Lynskey, Wolfe et al. 2000).
Family socio-economic background
While family socio-economic status has been consistently associated with antisocial behaviour, the relationship between socio-economic status and adolescent drinking is equivocal. Class or socio-economic status does not generally appear a strong predictor of youth drug use in Australian follow-up research (Coffey et al. 2000; Williams, Sanson, Toumbourou and Smart 2000).
There are scattered United States findings suggesting that parental occupation and parental prestige are positively related to adolescent drinking (discussed in Hawkins et al. 1992), indicating that alcohol use is higher among adolescents whose parents are of higher socio-economic status. In relation to the impact of low family socio-economic status on adolescent alcohol use, Hawkins et al. (1992) argue that adolescent alcohol use increases only when poverty is extreme, but notes that at this extreme level most adolescent risk factors and problem behaviours also increase.
Community influences on parenting
In disadvantaged communities the impacts of poverty, neighbourhood safety, and social supports on parenting are important factors. Disadvantage in communities has been associated with poorer relationships between parents and their children (FACS Parenting Information Project review 2004). While the effect of poverty alone is not clear, poor families experience greater stress through inadequate housing, economic insecurity, and job loss (FACS Parenting Information Project review 2004). The Parenting Information Project reports that neighbourhood effects are only small to moderate when family factors are controlled for; however, it is not clear how parenting might change to counter the effects of dangerous neighbourhoods. According to a review by Garbarino and Kostelny (1993), parents living in dangerous neighbourhoods respond by being more restrictive with their children. For the purposes of this review, this could mean that parenting norms concerning adolescent alcohol use might be tightened as a response to social disadvantage within communities, but this remains unknown as yet.
Summary
Several broader family characteristics have been shown to be related to adolescent alcohol use. Adolescents from intact families were found to engage less often in heavy alcohol use, while adolescents from sole-parent families were more often involved in heavy drinking. While there are scattered United States findings suggesting connections between higher family socio-economic background and greater adolescent alcohol use, these trends were not evident in the Australian studies reviewed. Relationships between socio-economic status, community disadvantage, and adolescent alcohol use have not been clearly demonstrated as yet.
Broader cultural influences and norms
The theoretical frameworks provided by the Parenting Model and the ecological emphasis of the Social Development Model highlight the fact that parental and adolescent behaviour are influenced at many levels and in many arenas. Therefore a multi-component approach is required to change adolescent drinking behaviour (Catalano, Kosterman, Hawkins, Newcomb and Abbott 1996). That is, there would need to be not only parenting interventions, but also changes within schools, peers, communities, social norms, and laws.
Prevailing cultural norms regarding adolescent alcohol use are thought to exert a powerful influence. Bjarnason and colleagues (2002) found that in countries where there was a tolerant or permissive attitude towards youth alcohol use, rates of heavy alcohol use among young people were higher than in countries where the social climate towards youth alcohol use was less favourable. Distinct differences between Australia and the United States were found in the relationship between norms concerning adolescent substance use and patterns of use, as shown by Beyers Toumbourou, Catalano, Arthur and Hawkins (2004). These authors present findings from three large, representative student samples recruited in Victoria, Australia and in the American states of Maine and Oregon. In each study, a variant of the Communities That Care youth survey was used (Arthur, Hawkins, Pollard, Catalano and Baglioni 2002).
While there were many similarities across the two countries, the factors which were more powerfully associated with risk for substance use among Australian youth reflected more tolerant attitudes and norms, while the risk factors identified for youth in the United States were more reflective of social alienation, measured by individual factors such as rebelliousness, academic failure and low social skills.
Findings were interpreted according to the policy differences in the two countries (Beyers et al. 2004), with Australian harm minimisation policies associated with greater acceptance of experimentation with drug use and American abstinence policies associated with punishment of use. The authors note that although these comparisons are important, methodological differences may limit their validity, including the fact that the studies were cross-sectional and the samples were not prospectively matched. It is likely that other factors also contributed to these across-country differences - for example, norms concerning adolescent alcohol use and different socialisation practices surrounding alcohol.
Summary
Prevailing cultural norms regarding adolescent alcohol use appear to exert a powerful influence. In countries where there is a tolerant or permissive attitude towards youth alcohol use, youth patterns of risky use tend to be higher than in countries where the climate is less favourable towards youth alcohol use.
Young Australians perceive there to be considerable acceptance among parents and the broader community of youth alcohol use, and there appears to be powerful normative pressure toward youth alcohol use.
Laws regarding adolescent alcohol use
Hawkins and colleagues (1992) have proposed that laws affect social norms, and that alcohol use is a function of these social norms. Laws also impact on availability, and when availability increases, so does the prevalence of adolescent drinking (Hawkins et al. 1992). Studies examining the relationship between minimum legal drinking age and adolescent drinking have shown that lower legal age limits are associated with increases in adolescent drinking and adolescent traffic accidents (Hawkins et al. 1992). The previously discussed large cross-cultural study (Bjarnason et al. 2002) across 11 European countries with 34,001 students found that the adolescent drinking culture had a significant overall direct effect on heavy drinking across these countries.
There is strong evidence from both the United Sates (Wagenaar and Toomey 2002), and Canada and some other countries (Shults, Elder, Sleet et al. 2001) that increasing the legal age for youth purchase and use of alcohol can reduce youth alcohol use and related harm. This evidence comes from research studies that have monitored trends in state data concerning alcohol consumption, and alcohol-related mortality and morbidity before and after modifications to state minimum drinking age laws.
The evidence supports the view that increasing the legal age for alcohol purchase and use is associated with reductions in levels of adolescent alcohol consumption and related harm. One flow-on effect of changing the laws concerning access to alcohol among adolescents and young adults is that parents seem to adopt less favourable attitudes to youth alcohol use (Yu and Shacket 1998). There is also evidence from one community trial demonstrating that action to enforce minimum alcohol purchase age laws can reduce associated harms (Grube 1997). It is possible that an increased focus on the enforcement of under-age drinking laws in Australia might influence prevailing attitudes regarding youth alcohol use as well as supporting and reinforcing parental efforts to delay the age of adolescent alcohol initiation and to guide subsequent moderate, responsible patterns of use.
Summary
Laws concerning adolescent alcohol use can exert considerable influence on adolescent consumption and parental attitudes toward adolescent alcohol use. Studies conducted in the United States examining the relationship between minimum legal drinking age and adolescent drinking have shown that lower legal age limits are associated with increases in adolescent drinking and adolescent traffic accidents. Conversely, increasing the legal age for youth purchase and use of alcohol has been associated with reductions in youth alcohol use and related harm. One effect of changing the laws concerning adolescent access to alcohol is that parents seem to adopt less favourable attitudes to youth alcohol use. As yet, the applicability of these findings to the Australian context is unknown.
Indigenous adolescents
One goal of the present project was to review relevant Australian research with Indigenous adolescents. There is little information regarding patterns of drug use among young Indigenous people. Dunne, Yeo, Keane and Elkins (2000) report findings from a primary school student survey completed with a small convenience sample of schools in Brisbane and the Torres Strait Islands. They found no significant association between Indigenous/non-Indigenous background and risk of smoking tobacco or marijuana, while Indigenous children were less likely than non-Indigenous children to report experience with alcohol. Their conclusion was that that the excessive uptake of drug use among Indigenous Australian young people occurs in the early stages of secondary school, arguing for preventive education in primary schools. The Indigenous and non-Indigenous children living in Brisbane had slightly higher smoking rates than those in the Torres Strait Islands. Conclusions from this study should be accepted very cautiously as the small, non-representative sample may not have reflected broader trends.
Gray and colleagues were invited by the local Indigenous community to complete a study in the Albany region of Western Australia. All 110 Indigenous Australians aged 8-17 years living in the region were identified. and 105 surveyed. There were high rates of solvent use and poly drug use, rising sharply from age 15. The overall frequency of alcohol consumption was lower in this survey by comparison with younger Western Australian secondary school students (Gray, Morfitt, Williams, Ryan and Coyne 1996). Findings from the above study were in line with those reported earlier for Dunne and colleagues (2000) in demonstrating that excessive substance use for young Indigenous people around Albany emerged most strongly in the early high school years.
In their consultations in Victoria, Rowland and Toumbourou (2004) reported that the family was considered within the Indigenous community to play an important role in Indigenous youth alcohol and drug use. In this review, interventions to assist Indigenous families through the early years and also with the parenting of adolescents were both indicated. The report noted the recent development in Victoria of a Koori ABCD Parenting Program seeking to assist Indigenous families with culturally specific parenting practices.
Using the NDSHS 1994 Indigenous supplement data, Hennessy and Williams (2001) reported that proportionately fewer Indigenous young people consume alcohol than non-Indigenous people; however, the Indigenous young people who drink do so at more risky levels. This finding was replicated in the recent NDSHS survey, which revealed that more than one-quarter of Indigenous young people aged 18-24 years drank at levels that are considered to be high risk over the long term, compared with 14 per cent of other Australian young people (AIHW 2003a).
A New South Wales survey has compared alcohol use amongst Aboriginal and Torres Strait Islanders (ATSI) school students and non-Aboriginal students (Forero, Bauman, Chen, and Flaherty 1999). This study reported on data collected across several administrations of a large-scale survey, and included data collected in 1996 from 346 ATSI students (from a total sample of 10,026 students), and also on pooled data collected in 1992 and 1989 from 224 ATSI students (from a total sample of 7,614 students). Prevalence comparisons revealed that ATSI students were not significantly more likely to drink alcohol on a weekly basis than other students, but they were 2.1 times more likely to drink at risky levels (Forero et al. 1999).
The Forero et al. (1999) study measured relatively few parenting-related variables, but some differences were shown between the Indigenous and non- Indigenous students. Comparisons revealed that Indigenous students were 1.6 times more likely than non-Indigenous students to be unmonitored in the evening and had higher amounts of spending money each week. They were also 2.0 times more likely not to be living with both parents (Forero et al. 1999).
In the Albany study reported above (Gray et al. 1996), 60 per cent of the parents identified alcohol use as a major problem, and the parents also thought there was a need for more education and support. This study also reported that 89 per cent of the parents wanted more information about alcohol for their children, and 76 per cent wanted more information for themselves (Gray et al. 1996). Clearly, the issue of parenting influences of adolescent alcohol use in the Indigenous context is under-researched at present. It is likely that the recently completed study of Indigenous children and families - the Western Australian Aboriginal Child Health Survey (Zubrick, Lawrence, Silburn, Blair, Milburn, Wilkes et al. 2004) - will provide relevant data in its forthcoming reports. One major aim of the study was to report on the levels of problem behaviours, including alcohol use, among child and adolescent participants, and the family and environmental influences on these behaviours.
While there is lack of information at present, it is probable that many aspects of the parenting behaviours and parental characteristics discussed in this review will generalise to Indigenous adolescents and families. To the extent that aspects of parenting and their effects on child and adolescent development are universal, the broader findings and conclusions described here may be applicable to Indigenous parents, and prove of benefit to them.
Summary
The studies reviewed suggest that the pattern of Indigenous adolescent alcohol consumption differs from that of non- Indigenous adolescents. Those Indigenous adolescents who drink appear to consume alcohol at more risky levels. Unfortunately, these conclusions are based on few studies, and further investigation is needed. No specific research was located concerning the influence of parenting on alcohol use among Indigenous adolescents.
6. Parent and peer influences compared
It is often proposed that in adolescence, there is a shift away from parental influence, with peers taking on greater importance. While this shift has been demonstrated in research, it is erroneous to assume that parents have no or little influence on their adolescents. Rather, research has shown that both parents and peers have an influence on the developing adolescent.
The influence of parents and peers
We have seen that for typically developing adolescents, the relationship with parents is likely to remain strong. Evidence suggests that well-adjusted adolescents tend to have high-quality relationships with their peers (Armsden and Greenberg 1987). Research on decision-making has shown that whether parents or peers are more important depends on the quality of the parent-adolescent relationship (Noller 1994; Wilks 1986).
Generally, parents are considered more vital in decisions concerning vocation or money, and peers are considered more important in decisions about clothes, social activities, and entertainment. According to Noller (1994), when everyday problems arise, adolescents prefer to discuss these with their close friends, rather than parents. While a complete review of the research on peer influence on adolescent alcohol use is beyond the scope of this review, a summary of key studies follows.
The role of peers in adolescent alcohol initiation is generally accepted as crucial. In Australia, the high prevalence of alcohol use among peers of adolescent drinkers has been demonstrated by the NDSHS survey (AIHW 2002); with three quarters of male (73 per cent) and female (78 per cent) recent drinkers reporting that all or most of their friends consume alcohol. This was compared to the abstainers or ex-drinkers where only 21 per cent of males and 30 per cent of females reported that their friends drink alcohol (AIHW 2002).
This review has adopted a bi-directional framework in which to consider parent-adolescent relationships. The research also shows that this bi-directionality is an important element in adolescent-peer relationships. This bidirectional peer selection/peer socialisation process has been demonstrated in a longitudinal study using latent growth modelling (Curran, Stice and Chassin 1997). In this study, an individual's earlier levels of alcohol use were predictive of later changes in their peers' use; conversely levels of peer use at time one were also predictive of later changes in the adolescent's use. This suggests that once adolescents commence drinking they may seek out peers who also drink alcohol. Bamberg and colleagues (2001) propose that parents influence this selection of peers because adolescents who have parents who frequently smoke or drink alcohol are more likely to choose to associate with peers who display these behaviours too.
Recent research has begun to look at the similarities amongst peers, specifically close friends, rather than the wider peer group. In a longitudinal study of 1028 students from Grades 6 to 10, only the alcohol use of a close friend predicted the initiation of alcohol use, and the alcohol use of the wider peer group was not significant (Urberg, Degirmencioglu, and Pilgrim 1997). However, both close friends and peer groups predicted drinking to intoxication (Urberg et al. 1997). Of interest is that once initiation has occurred, there appears to be a change in the peer context, in that those who have tried alcohol are more likely to know fellow drinkers. Thus it appears that peer selection and influence are complementary processes.
The importance of peers and parents was compared in a three-year longitudinal sample of adolescents, who were aged 13-16 years at time one. Reifman et al. (1998) measured progression to heavy drinking and found that friend's drinking was the most significant predictor (odds ratio 1.62), and parental monitoring was the only other significant predictor (OR 0.71). In this study maternal disapproval, rule setting, and parents' drinking were not significant.
Similar findings were reported by Rai et al. (2003) in a comparison of peer and parental influence using data from six studies conducted across ten years. Rai and colleagues found the odds ratios for alcohol use among adolescents whose peers were involved in risk behaviours ranged from 1.37 to 1.92 over the six samples, with an overall average of 1.62. The odds ratios for parental monitoring were 0.35 to 0.69 (indicating that increased monitoring was associated with less alcohol use), with an overall averaged odds ratio of 0.65 (the odds ratios obtained for these parent and peer influences cannot be directly compared, as odds ratios smaller than 1 have a possible range of 0 to 1, and are therefore measured on a different scale to odds ratios greater than 1, which can range from 1 to infinity). It should be noted that since parents often influence adolescents' choice of peers, these studies to a certain extent underplay the extent of parental influence.
Summary
These key studies have shown that the effect of peers mediates the influence of parenting factors on adolescents' alcohol use. Peer effects become particularly powerful when parent-adolescent relationships are of poorer quality. The influence of peers is thought to occur through peer modelling, peer pressure, or association with alcohol using peers. However, direct connections between parental monitoring and adolescent alcohol use remained after peer influences were taken into account. The interaction of peers and parents is a complex issue that cannot be easily separated, and thus future research or interventions must consider the interaction of each.
The mediational model
Further evidence of the inter-connected influence of family and peers is shown in the seminal work of Dishion and colleagues, using multiple types of respondents (e.g. adolescents, parents), and multi-method measures (for example, observations and questionnaires). Dishion and colleagues (1999) measured the initiation of alcohol use and found that family, peer, and child characteristics were all connected to initiation of use. Socio-economic status and parental substance use were also significant contextual predictors of the onset of adolescent alcohol use. Statistical modelling showed that the effect of socioeconomic status was mediated through family management (parenting behaviours such as monitoring and limit setting), and in turn family management was mediated through deviant peer associations. Furthermore, after including child characteristics at age 9-10 years, only the boys' antisocial behaviour at this younger age predicted early onset of alcohol use. The authors argued that their research demonstrated the ecological framework of adolescent development, and that more proximal predictors mediated the effects of less proximal predictors.
Other longitudinal work using the Social Development model as a structure for understanding the importance of family, school, social, and community factors supports an ecological view of adolescent development. Guo et al. (2001) measured the alcohol use of 755 adolescents who were followed from age 10-21 years. Using odd ratios adjusted for internalising and externalising behaviours at age ten years, these researchers found that the most significant predictors of alcohol abuse originating from age 10 were associations with deviant peers (OR 1.5), time with antisocial friends (OR 1.3), and alcohol use amongst best friends (OR 1.3). Furthermore, high monitoring as well as clearly defined rules at ten years of age predicted lower alcohol abuse and dependence at 21 years. The size of the odds ratios increased across time and with closeness to the outcome at 21 years, with more powerful associations found for measures taken at age 14 and 16 years.
Summary
Mediational models have shown that there are bi-directional influences between adolescents and others. Adolescents are influenced by parents, peers, the community and society; but conversely, their behaviour has a reciprocal influence on their families and peers too. The research on parenting factors does not always account for this bi-directionality, or for the existence of multiple spheres of influence.
7. Gaps and deficiencies in the research
A number of gaps and deficiencies in the research base were evident. These included the issues addressed, methodological weaknesses, and inconsistencies in findings. The most notable gaps and deficiencies are now briefly described.
Incomplete research coverage
One aim of this review was to explore whether specific parenting factors might be associated with different types and patterns of adolescent alcohol use, for example moderate compared with risky use. Overall, no such trends were found. However, it is difficult to draw definite conclusions because research is lacking on many of the aspects of parenting reviewed and their association with differing types of adolescent alcohol use.
Table 9 provides a summary of the studies reviewed for this report that have addressed parenting influences on adolescent alcohol use. A tick (3) indicates that this aspect of parenting and this type of adolescent alcohol use have been investigated, while a gap means that these connections do not seem to have been investigated as yet, although it should be recalled that this was a targeted, rather than a comprehensive, review. However, this categorisation was made difficult by the considerable variation in definitions of adolescent alcohol use employed across the studies, with there being no single, agreed-upon definitions of different types of use. Thus, the classifications in Table 9 are approximate.
| Initiation | Use | Levels of use | Escalating pattern | Decreasing pattern | Risky use | Misuse | |
|---|---|---|---|---|---|---|---|
| Aspect of parenting | |||||||
| Parental monitoring | 3 | 3 | 3 | 3 | 3 | 3 | |
| Parental awareness of adolescent alcohol use | 3 | 3 | |||||
| Parental behaviour management | 3 | 3 | 3 | ||||
| Parental permissiveness | 3 | ||||||
| Parental authority | 3 | ||||||
| Parenting style | 3 | ||||||
| Parental supply of alcohol | 3 | 3 | 3 | ||||
| Relationship quality | 3 | 3 | 3 | 3 | 3 | ||
| Parental attitudes towards adolescent alcohol use | 3 | 3 | |||||
| Parental approval/ disapproval | 3 | 3 | 3 | 3 | 3 | ||
| Parental concern about adolescent alcohol use | 3 | ||||||
| Parental/family aspect | |||||||
| Parental alcohol consumption | 3 | 3 | 3 | ||||
| Parental alcohol dependence | 3 | 3 | |||||
| Family structure | 3 | ||||||
| Family socio-economic background | 3 | ||||||
| 3 = these associations have been investigated | |||||||
As Table 9 shows, the parenting characteristics that have received most attention in relation to adolescent alcohol use are parental monitoring, relationship quality, and parental approval/ disapproval, while the areas of alcohol use that have been most studied are use, levels of use and risky use. Clearly, there are many gaps, with research investigating parenting influences on the initiation of alcohol use particularly lacking. Thus, the Australian and international database pertaining to parenting influences on adolescent alcohol use is not comprehensive, limiting the conclusions that can be drawn concerning the influence and contribution of parenting and parental/family factors to adolescent alcohol use.
The lack of Australian data
There is a critical lack of Australian data on this issue, and a clear need for more Australian research to be conducted. Very few large, rigorous, cross-sectional or longitudinal Australian studies were located and, as well, the number of smaller scale or clinical studies with pertinent data was quite small. After an extensive search, only 34 relevant Australian studies could be located. Thus, the international research, particularly United States research, was relied upon to a large extent. Yet there are important differences which may dilute the transferability of the international research to the Australian context. Two major considerations apply: how similar are parenting influences across Australia and the United States; and the effects of differing cultural norms and attitudes concerning adolescent alcohol use.
With regard to the mechanisms of parenting influence, there appears to be a high degree of similarity between Anglo-Australian and Anglo-American parenting. The general body of knowledge on parenting has shown there are similar associations between parent-adolescent relationships and parental behaviour management practices across the two countries. The findings of Beyers et al. (2004), who compared three large student samples from the state of Victoria in Australia and the American states of Maine and Oregon, are relevant. The Victorian component of this survey (known as the Health and Wellbeing Survey, HWBS) measured 25 risk factors and ten protective factors that had been identified in the United States and other longitudinal research as predictors of youth outcomes such as alcohol and drug use, antisocial behaviour and mental health. Preliminary analyses revealed that the items which made up each of the risk and protective factors were similar across the Australian and United States samples, suggesting that the variables and constructs were transferable across the two settings (Beyers et al. (2004).
Further evidence of fundamental similarities in parenting practices across cultures can be seen with the successful dissemination of Australian parenting programs into the United States, Europe and the United Kingdom (for example, the Triple P parenting program). Based on the above observations, it seems reasonable to assume that parenting research conducted in similar countries will produce comparable findings when considering relationship aspects and parenting behaviours in the Australian context.
Australian and American parenting appears to differ primarily on social and cultural norms, rather than parent-adolescent relationships, or parenting practices. The research of Beyers et al. (2004) indicated that there are more tolerant attitudes and norms towards adolescent alcohol use in the Australian context, with Australian parents and the broader Australian society appearing to be more accepting of youth alcohol use. Hence, the key differences are social and cultural, and it appears that young Australians perceive parents and the broader community to be more tolerant towards youth alcohol use, and there is more social pressure on young people to consume alcohol. These culturally influenced, alcohol-specific attitudes are part of a broader constellation of values and norms which differ across countries and may impact on usage patterns.
Much of the research reviewed for this report was based on samples from the mainstream of society. Yet Australia, in particular, is a multicultural country. A lack of research on Indigenous youth was especially evident. While the findings thus far suggest that Indigenous youth use alcohol less frequently than other Australian adolescents, those who consume alcohol tend to do so at riskier levels, and alcohol-related problems are reported to be more prevalent among Indigenous communities (Loxley, Toumbourou, Stockwell, Haines, Scott, Godfrey et al. 2004). It would appear crucial for this issue to be given more detailed attention.
There has also been little research on differing cultural sub-groups, whose religious and social attitudes and behaviours may vary substantially from those of mainstream society, with unknown effects on the alcohol use or associated harms among adolescents from these sub-groups. Conversely, studies involving communities or religious and cultural sub-groups in which adolescent alcohol use is less prevalent or non-existent (as demonstrated by the New South Wales study conducted by Chen, Bauman, Rissel, Tang, Forero and Flaherty 1999) could provide valuable information such as: How do these adolescents respond to or ignore broader societal pressures to consume alcohol? How do their parents successfully transmit attitudes and values concerning adolescent alcohol use? One likely difference is that the peer groups of such adolescents may include a substantial number of individuals from the same community or cultural group, and thus peer influences and values may be consistent with parental values. However, this remains to be established. All in all, there is an urgent need for more Australian research to be undertaken on these complex issues.
Reliance on adolescent report
The summaries provided in Tables 4 and 5 make it clear that most research has relied on adolescent respondents, with few studies gathering information from parents or other informants. At least two limitations result from this trend. First, employing the same reporter to inform on predictors (in this case, parenting) and outcomes (alcohol use) may produce inflated estimates of associations due to shared method variance, or "eye of the beholder" effects. Second, as noted earlier, adolescents tend to have more negative views of parent-child interactions and relationships. This trend may be exacerbated among problematic adolescents who may not accurately portray parental behaviour or relationships with parents.
Thus, the findings regarding parenting influences on adolescent alcohol use, which are to a large extent based on adolescents' views, need to be corroborated by parental or other data. Ideally, the reports of adolescents and parents, and potentially other informants, should be obtained.
Inconsistent findings
On almost all aspects reviewed, very consistent findings emerged from the various studies. However, some inconsistency was evident in the area of parental supply of alcohol. Thus, one study found that adolescents consumed less alcohol if they had obtained their alcohol from parents, both at home, and at parties or other social venues. Another study showed that abstinence was much higher among adolescents whose parents who did not permit them to drink at home, or provide them with alcohol to take to parties or social events, and that the later such permission was delayed, the less likely adolescents were to consume alcohol.
Similarly, parental disapproval of adolescent alcohol use was found to be associated with lower use, while permissiveness towards alcohol use was related to higher levels of use. As parental supply of alcohol use is a common practice, particularly for older adolescents who are nearing the legal age for independent access, the effectiveness of this parental strategy needs to be clarified.
Gender differences
In general, the research revealed few gender differences. However, many studies did not directly investigate gender differences, and this appears to be an understudied area. Other Australian research with younger children shows that parenting behaviours and parental characteristics can have differing impacts on girls and boys (Prior et al. 1993; Prior et al. 1999). Hence the parenting influences reported here cannot be assumed to apply equally to male and female adolescents. Similarly, rates of adolescent problems which commonly co-occur with substance use, such as antisocial behaviour and depression, differ markedly across the sexes, perhaps suggesting the pathways to adolescent alcohol use may vary somewhat for male and female adolescents, as was found by Smart et al. (2001) in relation to multi-substance use.
Summary
The research base currently has a number of gaps and deficiencies. First, the research coverage is incomplete, with many areas of parenting and types of adolescent alcohol use understudied at present.
Second, there is scant Australian data on this issue, and international research was relied upon to a large extent. While research into parenting conducted in other countries reveals findings similar to Australian research when considering parent-adolescent relationships and parenting behaviours, there are key social and cultural differences that may influence parenting in the differing contexts.
Third, much of the research has involved adolescent respondents only, and the findings regarding parenting behaviour and parent-adolescent relationships need to be confirmed by parental or other informants' data. Fourth, while there was considerable consistency in the findings, on one important area - parental supply of alcohol - inconsistent findings were found.
Finally, the possibility of gender differences has often been overlooked.
8. Prevention/early intervention programs
This review has demonstrated that there is a large body of research showing significant associations between parenting behaviours and adolescent alcohol initiation or continued use. There is also a large body of research showing the influence of peers. However, while these studies were seeking to identify direct connections and the majority were longitudinal, it remains difficult to establish the causal role of parenting in adolescent alcohol use.
Experimental demonstrations are one way of demonstrating causality by examining under controlled conditions what would happen if one aspect of parenting were changed. For example, if parents improved their monitoring, would adolescent alcohol use change? Or, if parents were encouraged to develop family norms that disapproved of under-age alcohol use, would this change adolescent behaviour? The outcomes from psychosocial interventions that have used experimental methodology, including treatment and control groups and randomised allocations of participants to groups (randomised control trials), are therefore most valuable in expanding our understanding of how to effect change in adolescent alcohol use.
There is a large body of experimental research demonstrating that parenting interventions, particularly with younger children, can reduce problem behaviours (Sanders, Gooley and Nicholson 2000; Serketich and Dumas 1996; Woolfenden, Williams and Peat 2002). To the authors' knowledge, there are only a handful of studies that have used randomised control trials methodology to examine directly the impact that interventions targeting parenting might have on adolescent alcohol use.
Review of six intervention programs
In the review of parent-adolescent intervention programs that follows, programs were selected for inclusion in two ways. First, programs were included if they had been reported in the scientific literature as being evidence-based programs - that is, they used randomised designs, had independent evaluations, and had achieved positive outcomes after a substantial follow-up period. Second, a number of promising programs are also described. These programs were considered promising because the initial research has shown they have improved parent-adolescent relationships and generally have achieved reductions in adolescent substance use; however, these promising programs await more rigorous long-term scientific evaluations.
A review of primary prevention programs for alcohol misuse among adolescents was recently conducted by the Cochrane consortium (Foxcroft, Ireland, Lister- Sharp, Lowe and Breen 2004). This worldwide review evaluated 56 studies where an educational or psychosocial prevention program specific to adolescent alcohol use was undertaken. This review investigated the longer-term effectiveness of interventions and required follow-up to be maintained beyond three years. The results showed that 20 of the 56 studies reviewed had evidence of ineffectiveness and the reviewers could make no firm conclusions about the effectiveness of these programs overall. Furthermore, six of the intervention studies reviewed had a negative effect and increased alcohol consumption among adolescents.
Only three studies showed effective long-term benefits in alcohol reduction. They were: the Strengthening Families Program (SFP; Spoth, Redmond and Shin 1998) which is a family-based intervention; the Life Skills Training Program which is an intervention program for use within schools (Botvin, Baker and Dusenbury 1995); and a cultural program with Native Americans (Schinke, Tepavac and Cole 2000). Only the Strengthening Families Program is relevant to this review of parenting influences, and an overview of this and other promising programs follows.
The Strengthening Families Program
The Strengthening Families Program (SFP) is an American-based family program developed for widespread application (with a universal focus), that aims to prevent the initiation of alcohol use in adolescents. SFP is based on a psychosocial model and targets the enhancement of family protective factors and resiliency and the reduction of risk factors (Kumpfer, Alvarado and Whiteside 2003).
The program comprises seven once-a-week sessions. During the first hour of the sessions, parents and pre-adolescent children participate in separate skill building sessions. In the second hour, parents and children jointly participate in family sessions, which include practicing the skills learned in the separate sessions. The parent component includes child development norms, discipline, managing emotions, and effective communication. The child sessions parallel the parent sessions, but also include peer resistance, personal issues, and social interactions (Spoth et al. 1998).
In a test of the program, 446 families from a rural area of the United States were randomly allocated into treatment and control groups. The children were in Grade 6 at the time of the intervention. After one year, comparisons of the control and treatment groups showed that significantly fewer of the treatment group had initiated the use of alcohol, with a medium effect size (.26) found. At two years post-treatment, the treatment effect was still evident and a large effect size of .39 was shown (Spoth, Redmond and Lepper 1999). Results of the SFP show that the likelihood of substance initiation was lower for the treatment group two years following the intervention, at a time where the adolescents were entering the peak age for alcohol initiation (Spoth, Lopez Reyes et al. 1999).
In the Cochrane review, Foxcroft et al. (2004) concluded that the SFP showed the greatest promise of the intervention/prevention studies. To examine the effects of the program an "intention to treat" analysis (a strategy for analysing data in which all participants are included in the group to which they were assigned, whether or not they completed the intervention given to the group)5 was used. This review found that for every nine individuals who receive the SFP, there would be one fewer person reporting that they have ever used alcohol, used alcohol without permission, or ever been drunk, four years later.
This study provides evidence on the importance of delaying the onset of alcohol use. Of note is that the largest effect was found at the two-year follow-up, rather than at one year, and this provides further evidence on the importance of including long-term outcome measures in such studies.
The Preparing for the Drug Free Years program
The Preparing for the Drug Free Years (PDFY) program is a American-based skills training program designed to teach parents and children skills that reduce a child's risk for drug and alcohol use (Kosterman, Spoth, Haggerty and Zhu 1997). The PDFY is guided by the Social Development Model. The program includes four two-hour parent sessions, and one individual child session. The parent sessions include instruction and skills training on identifying risk factors, parent-child bonding, developing guidelines and clear expectations related to substance use, monitoring compliance, delivering appropriate consequences, managing anger and conflict, and enhancing positive child involvement in day-to-day tasks. The pre-adolescent child attends for one session and participates in peer resistance skills training. Programs are standardised using videotapes demonstrating parent-child interactions.
In a pre-test, post-test randomised control trial study, the PDFY program was shown to produce changes in parenting behaviours. Using videotaped interactions to measure change, the program increased proactive communication between parents and children. Regardless of whether the interaction task concerned general family life or problem-solving, mothers in the intervention group displayed more positive communication patterns than control group mothers. Fathers in the intervention group exhibited more positive interactions in the problem solving task. The PDFY program also reduced mothers' negative interactions, but had no significant effect on fathers' negative interactions (Kosterman et al. 1997). Although promising, this study did not report the effects of the intervention on adolescent alcohol use.
In a separate study, Spoth, Redmond, Hockaday and Yoo (1996) demonstrated that exposure to the PDFY program reduced adolescent favourable attitudes towards alcohol use. All families with a Grade 6 or 7 student in six selected school districts in Iowa were invited to participate. Of 387 families confirmed as having a sixth or seventh grader, 220 agreed to participate in the project and were randomly assigned to the intervention condition or to a control condition following the completion of pre-test measures. By increasing protective factors, the program made a small significant contribution to increasing adolescents' affectional bonds with parents and had an indirect effect on adolescents' favourable attitudes towards alcohol abstinence.
Promising results for the PDFY program have also been shown in a randomised control trial longitudinal study with 429 rural adolescents (Mason, Kosterman, Hawkins, Haggerty and Spoth 2003). The intervention was delivered with adolescents with a mean age of 11.35 years. Follow-up results at 3.5 years postintervention showed that, compared with the control group, the PDFY adolescents had a lower rate of poly-substance use (tobacco, alcohol, marijuana, inhalants and other illicit drugs). In addition, the PDFY treatment group had lower rates of delinquency, and the authors contend that this is an extension of the positive effects of the program.
The two programs compared
A comparative study of the Strengthening Families Program and the Preparing for the Drug Free Years program was conducted using randomised control designs with equivalence across the three groups (SFP, PDFY, and control). Using pre-intervention and post-intervention comparisons of targeted parenting behaviours, the two programs were found to be comparable with an intervention effect size for the SFP of .51, and intervention effect size for the PDFY of .45. Thus both programs appear to provide initial support for intervening in parenting behaviours, and both appear to have set in motion a measurable change in parenting. However, the program effect on the child's behaviour have not been reported in these comparisons (Spoth et al. 1998).
Project Northland
One United States intervention study using randomised treatment and control groups has also shown the importance of parental norms for alcohol use (Sieving, Maruyama, Williams and Perry 2000). In this longitudinal intervention entitled Project Northland, the influence of parental norms on the control and treatment groups were compared. The study found that when parental norms were tolerant of drinking, there was a significant association with the initiation of alcohol use among adolescents, and that parental norms had a significant long-term influence in both the control and treatment groups. Project Northland entails a multi-level community intervention including a school drug education curriculum, parent education and community activities to reduce youth access to alcohol.
This study also reported a positive intervention effect, with adolescents in the treatment group consuming less alcohol over time. More specifically, fewer adolescents in the treatment group reported using alcohol, they experienced significantly less peer influence to use alcohol, they had greater self-efficacy to refuse alcohol, and they reported more communication with parents about the consequences of drinking.
The Parenting Adolescents a Creative Experience program
The Australian Parenting Adolescents a Creative Experience (PACE) program targeted parents of early adolescents (Toumbourou and Gregg 2002). Designed as a universal intervention and using a facilitated groups approach, the program addressed adolescent communication, conflict resolution and adolescent development. Evaluation investigated the impact of seven-week PACE groups on a national sample of 3000 parents and Year 8 adolescents sampled from 14 schools targeted for intervention and 14 matched control schools. Evaluation included pre- and post- intervention surveys separated by three months for 577 families (parents and adolescents), representing a 60 per cent response rate from those who participated. At the 12-week follow-up, parents and adolescents reported a reduction in family conflict. Adolescents reported increased maternal care, less delinquency, and less poly-drug use (the odds of transition to poly drug use were halved).
Although only around 10 per cent of parents were successfully recruited into PACE groups, pre- and post-intervention findings demonstrated that benefits extended more broadly in the schools where the program was offered. Analysis suggested that the intervention effects might have extended to youth with a high number of risk factors for drug use problems. The evaluation demonstrated that the parents recruited into the intervention were more frequently sole parents and their children reported higher rates of family conflict and poly-drug use. At the post-test, family conflict and youth poly-drug use had reduced markedly in these families.
Evaluation suggested that the drug use of respondents was influenced by their best friend's drug use. Improvements in troubled family relationships appeared to impact on a wider group of families not directly participating in the PACE groups through changes in peer-friendship networks and through the programs efforts to encourage parents to assist other parents in their school community (Toumbourou and Gregg 2002). The fact that the intervention and control groups were not randomly assigned and the lack of long-term follow-up suggest the need for caution in interpreting these promising early results.
The Australian Teen Triple P program
A newly developed Australian program is the Teen Triple P program for parents of young adolescents. This program is an upward extension of the Triple P - Positive Parenting program for parents of younger children and is based on a behavioural family intervention model. Teen Triple P was developed for parents of older children to target risk factors associated with parenting practices, specifically harsh discipline, coercive discipline styles, parent-adolescent conflict, and communication difficulties (Ralph and Sanders, in press). The program can be delivered universally for parents of all teenagers, and is generally targeted at the transition to secondary school, which can be a time of substantial change in developmental pathways (Smart et al. 2003; Vassallo et al. 2002). It can also be delivered as an early intervention program for adolescents exhibiting a range of behavioural problems.
Preliminary evaluations have been completed with initial trials showing that the program achieved reductions in parent-adolescent conflict and improvement in parenting factors (Ralph and Sanders 2003). Evaluations of the program's self-directed format, where parents work in the home and receive telephone support, have shown significant improvements in adolescent behaviour (Stallman, Ralph and Sanders 2004). Evaluations with longer-term follow-up data are currently underway, along with plans to measure adolescent alcohol use in future studies.
The ABCD Parenting Young Adolescents Program
The ABCD Parenting Young Adolescents Program is a promising Australian prevention program aimed at parents of children in late primary school and early secondary school. The program is based on child development and social learning theory, as well as drawing upon recent interventions in marital therapy and parenting interventions for conduct disordered children. Conducted in group sessions over four weeks, the program covers areas such as adolescent development, parenting skill development, and caring for oneself as a parent. Program materials have been developed in five community languages and an online website providing a range of information resources for practitioners and parents has recently been developed.
An external evaluation revealed a high level of overall participant satisfaction with the program. As yet behavioural changes in adolescents have not been evaluated, and the program awaits controlled evaluation (W. Cann, Victorian Parenting Centre, personal communication, 27 July 2004).
Engaging parents
Engaging parents in intervention and prevention programs has been a stumbling block, and yet the issue is critical for the effectiveness of such programs. These difficulties have been demonstrated in Australia (Ralph and Sanders, in press; Ralph, Toumbourou et al. 2003; Toumbourou and Gregg 2002), and also in overseas research (Spoth, Redmond et al. 1999; Spoth et al. 1998). Following low participation rates in the Teen Triple P programs, Ralph and Sanders (in press) have argued that greater ownership of programs by participating schools may be essential to their successful delivery. In the PDFY studies mentioned earlier, of the pre-tested families, 44 per cent (N=116) declined to participate; although the attrition rates among families who did agree to be involved were satisfactory, with 94 per cent participating in three or more sessions, and 61 per cent attending all five sessions (Spoth, Redmond et al. 1999).
Similar problems were shown in the SFP recruitment. Only 49 per cent of the 238 families who completed the pre-test participated in the intervention (Spoth et al. 1998). Those dropping out of these programs are likely to be more stressed, or less motivated, suggesting that the impact of such programs may be only moderately generalisable to parents experiencing substantial adversities.
To test whether stressful life conditions might influence the outcomes of the PDFY program, Rueter et al. (1999) measured parenting skills and family stresses at the pre-program stage among a sample of 209 randomly assigned treatment and control group families. Differences noted between mothers and fathers were related to differing program outcomes. Thus, mothers who reported marital difficulties during pre-test showed greater improvement in post-test communication skills than mothers not reporting such difficulties, whereas pre-existing marital difficulties did not affect the program outcomes for fathers. It was also found that mothers who had poor parent-child communication skills at pre-test showed more improvement than mothers who had shown initially higher skill levels. This effect was not seen in fathers, with those fathers who showed initially high parent-child communication levels showing the greatest program effect. In a further test, the influence of financial concerns on program outcomes was also measured in this study (Rueter et al. 1999). Mothers' program outcomes were not directly affected by financial concerns, but fathers' outcomes were directly impacted on by financial concerns.
In summary, Rueter et al. (1999) found that mothers who had marital difficulties and poorer parenting skills showed the greatest program effectiveness. When fathers had financial concerns the intervention program was less effective for them. These results show that for mothers and fathers, social and psychological factors are likely to impact on the outcomes achieved in intervention programs, but these factors may affect mothers and fathers in different ways. The results also point to the importance of understanding family psychosocial factors and how they might influence program participation or outcomes.
Summary
Using randomised controlled trials as the "gold standard" for intervention programs, this review has shown that a small number of international interventions, which targeted changing parenting behaviours and parental education, have shown long-term reductions in adolescent alcohol use. There is a paucity of this type of quality research in Australia, and further studies undertaking best practice evaluations of intervention initiatives are needed.
Several promising Australian interventions are currently underway, including PACE, Teen Triple P, and ABCD.
In Australia, engaging parents in early intervention or prevention programs can be problematic. Integration of such programs within the school curriculum is viewed as a potential strategy to increase parental involvement in these programs.
9. Integrative synthesis of parenting influences
This review has shown that the aspects of parenting which influence adolescent alcohol use can be separated into two categories. The first comprises parenting behaviours and skills, specifically parental monitoring, parental behaviour management practices, parent-adolescent relationship quality, and parental norms and attitudes. The second sphere of influence comes from the parents' individual characteristics, family characteristics, and broader environmental and cultural influences.
Conceptual model of the role of parents
To summarise the research that has been reviewed, and to provide an overall picture of the role of parents in adolescent alcohol use, a conceptual model has been developed. This model is shown below in Figure 6. This model depicts the main parenting factors and their proximity to adolescent alcohol use as identified in the literature review. It is important to note that this model is conceptual, but does not represent causal (cause and effect) or statistical relationships which will need to be established by future research. To interpret the model, it is necessary to begin with the parenting factors which have the most direct influence on adolescents, and these are depicted closer to the ellipse which represents adolescent alcohol use.
Figure 6. Conceptual model of parenting influences on adolescents' alcohol use
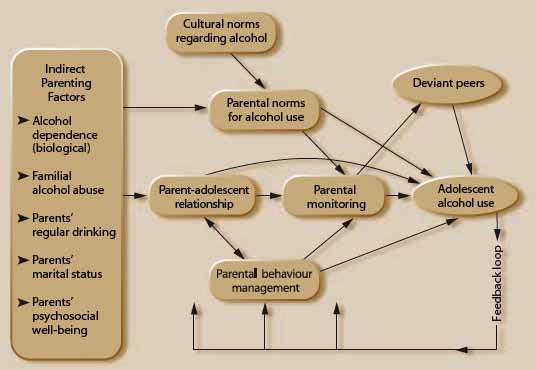
Parental monitoring
The majority of the studies suggested that parental monitoring was the parenting factor with the most direct influence on adolescent alcohol use. Therefore, one strategy for reducing adolescent alcohol use might be to ensure that parents monitor their adolescent more closely. Unfortunately, at this stage, the research has not firmly established which types of interventions are best to increase monitoring. Enhanced monitoring is not likely to occur by simply advising parents to ask more questions about their adolescent's free time, and indeed this increased interrogation is more likely to hinder their monitoring (Hayes 2004). To date, only one experimental trial has been published where improved monitoring has been demonstrated through an intervention (Dishion et al. 2003).
It is sometimes perceived that parental monitoring occurs when parents question their adolescent about free time, and therefore the general advice to parents is often to ask more questions. However, parental monitoring is not merely a matter of parents questioning an adolescent; in fact, repeated questioning can have adverse effects on the parent-adolescent relationship.
Good monitoring occurs at several levels. First, parents begin monitoring before their adolescent goes out, by establishing rules for appropriate behaviours, setting curfews, being interested, and discussing the forthcoming activity. Parents also monitor when their adolescent comes home from free time, and they do this by asking questions (not interrogating), listening to the adolescent, and observing their behaviour. More importantly, parental monitoring is an episodic process - that is, each monitoring episode influences the next occasion of adolescent free time. If an adolescent transgresses on one occasion, parents who monitor well are likely to adapt their monitoring on the next occasion when the adolescent seeks free time. Finally, parental monitoring is not static across adolescence, and marked differences in the levels of parental monitoring have been shown.
Peer influences
Although the influence of peers on adolescent alcohol use was not a major focus of this review, it has been included in the model because, as shown in Section 6, peer influence can be a primary risk factor. In the model, peer alcohol use is depicted in close proximity to adolescent use. There are many studies that have shown that peers have a more important direct influence than parents on ongoing alcohol use. However, other research has taken a wider perspective and suggests that parents influence the selection of peers at the outset. The model indicates the bi-directional nature of parental monitoring, peer influence, and adolescent alcohol use. Each of these three factors continually exert bi-directional influences.
Parental attitudes and values
The conceptual model next draws attention to parental norms for adolescent alcohol use. The research revealed that parents' beliefs about adolescent drinking have an important influence on adolescent use. When parents disapprove of adolescent drinking, adolescents are likely to consume less, and are less likely to engage in binge drinking. Conversely, when parents tolerate or approve of adolescent drinking, young people are more likely to drink and also to binge drink. Additionally, the influence of parental norms and attitudes may not only be direct, but exerted through the influence parents have on the differing social environments in which their adolescents participate. Parental norms and attitudes may be reinforced by other socialising agents, such as teachers, religious leaders, and sports or club leaders. In general the social norms in Australia appear to regard adolescent drinking as "normal" behaviour, and parents report that they feel under pressure to allow their adolescents to use alcohol (Taylor and Carroll 2001). It is also necessary to examine parental norms across several levels, including those which relate to their own adolescents, as well as broader norms regarding peer behaviour, local community, and wider societal norms.
The research on parent and peer influences has shown that adolescents continue to be guided by their parents' goals and values. Within individual parent-adolescent relationships, the longer parents are able to delay the onset of adolescent drinking, the less likely it is that adolescents will drink at high or risky levels. A key role for educators may therefore be to support parents to delay the onset of adolescent alcohol use. Without support parents may not feel confident that they are making the right decision in delaying their adolescents' alcohol use, and may be pressured into acquiescence. Providing education and developing societal norms that discourage adolescents' initiation into alcohol use may be a necessary first step. Some researchers have argued that a change in adolescent drinking patterns requires change at a societal level, rather than just within individual families (Hawkins et al. 1992; Yu 2003). Furthermore, research has suggested that when societal shifts have changed the legal age for alcohol use from 18-21 years, the commonly observed lowering in the incidence of alcohol use among adolescents may reflect an increase in unfavourable attitudes to youth alcohol use on the part of their parents (Yu and Shacket 1998).
Parental behaviour management
Parental behaviour management, as depicted in the conceptual model, covers the skills parents use to shape their adolescents' behaviour. For example, effective parenting involves the discussion of appropriate behaviours and establishment of clear boundaries for acceptable behaviours. Parents also provide logical consequences for misbehaviour; with adolescents this is most likely to be withdrawing material and domestic support services, grounding them or removing privileges. The research, although not extensive, shows that adolescents who denied parental authority were more likely to use alcohol. Furthermore, adolescents who were able to negotiate unsupervised free time were more likely to drink.
The ASSAD data revealed that on occasions when parents actively engaged with their adolescent with regard to alcohol use, and allowed their adolescent to drink in the home, they consumed less than when they drank at friends' homes or elsewhere. From these studies it could be assumed that if parents allow drinking in the home, adolescents might learn responsible use of alcohol. However, this is an assumption that has not been tested. It may be that adolescents drink less when they drink at home because their parents are present (although this has not been clarified as yet), but there is little evidence concerning whether moderation in the home setting translates to moderation in the peer drinking context.
One of the more sophisticated attempts to evaluate a harm minimisation approach to youth drinking has been conducted through the Australian National Drug Research Institute. In this study schools were assigned using a randomised control framework to a drug education program based on harm minimisation. Students exposed to this program demonstrated lower rates of alcohol-related harm over time compared with those in the control condition. Although not solely emphasising this approach, this study demonstrated an advantage for children who delayed the initiation of alcohol use, as well as for children who were supervised when consuming alcohol. One interpretation of the effectiveness of this study might be that an open approach to communication regarding alcohol can help some children to reach a non-use decision (McBride, Midford, Farringdon and Phillips 2000).
The parent-adolescent relationship
A key factor in the conceptual model is the relationship between parent and adolescent. The majority of the research on alcohol use has shown that relationship quality has both a direct and indirect effect on adolescent alcohol use. High quality parental monitoring and behaviour management, plus sharing of values and norms are fundamentally dependent on the existence of a high quality parent-adolescent relationship.
There is a large body of research to show that adolescents who have good relationships with their parents have improved outcomes in many areas, including reduced substance use, better academic achievement, more self-reliance, and lower rates of social and psychological problems (Armsden and Greenberg 1987). In any intervention work with adolescents and parents, it is recommended that the parent-adolescent relationship is the key starting point. Where the parent-adolescent relationship is damaged it is unlikely that an adolescent will respond in interventions that aim to achieve more monitoring, or following of rules, norms and values of the family.
The feedback loops included in the model are essential to understanding how alcohol use influences parents. The research has shown that when an adolescent has begun to use alcohol, this independent adult-like behaviour is likely to set in motion changes in the parental monitoring behaviours, and parental norms for adolescent alcohol use. In some cases, where conflict is high, adolescent alcohol use may have an impact on the parent-adolescent relationship, particularly if parents fear they no longer have an influence on their adolescent.
Parental characteristics
Finally, the model demonstrates that parents' individual characteristics can also influence adolescent alcohol use, but the effect is far more distant. First, parents' regular alcohol use is associated with higher use in adolescents. Second, the research has shown that parental alcoholism and alcohol abuse is related to increased drinking. While these effects may be due to parental modelling of alcohol use, some researchers have proposed that these individual parental factors influence adolescent alcohol use because they change parenting behaviours. That is, parents who are abusing alcohol may be unable to establish a strong relationship with their adolescents, they may have norms that encourage drinking at an early age, and they may be too preoccupied to monitor their adolescents' independent behaviour. The present review supports this argument, and therefore the conceptual model shows that these parenting factors exert their influence by changing the daily parent-adolescent interactions.
10. Conclusions
The evidence summarised in this review demonstrates that there is now a reasonable understanding of the processes by which parents influence adolescent alcohol use. In addition, there is also intervention evidence suggesting this evidence can be translated into effective programs. With regard to education and interventions with families, the research has demonstrated that relationship quality and good monitoring and behaviour management skills are strongly associated, and together they form the essential components needed in interventions to reduce adolescent alcohol use. It is argued that each of these factors must be included in intervention work at both the universal and targeted levels.
The review of more intensive interventions revealed that some intervention programs have had positive outcomes and reduced alcohol use amongst adolescents. Analysis of the content of these programs shows that they primarily work on building a good quality parent-adolescent relationship. Following this, these programs work with parents to provide them with education and support so that they can establish family norms that discourage the use of alcohol at a young age.
It is important to note that for many alcohol abusing young people, excessive or high risk alcohol use is not the only difficulty experienced. Many exhibit multiple problems, such as antisocial behaviour, risk taking (such as risky driving, gambling), depression or anxiety. Thus, recent Australian research found that while substance use was one of the most powerful risk factors for antisocial behaviour (Vassallo et al. 2002), antisocial behaviour was also a strong risk factor for substance use (Williams, Sanson et al. 2000). Some suggest that adolescent substance use is but one element of a broader syndrome of problem behaviour (Jessor and Jessor 1977). If this is the case, interventions that are targeted at other types of problem behaviours are likely to impact on adolescent alcohol use as well. Thus, it would seem that broad based, holistic interventions may be required, which have the potential to ameliorate a number of adolescent problem behaviours. The implementation of such programs may be facilitated by a cross-sectoral approach and the consolidation of efforts may prove to be relatively cost effective.
The consumption of alcohol in Australia is widely accepted, and parents are unsure of the correct approach to take with their adolescents. Research conducted with parents for the development of the National Alcohol Campaign concluded that "while parents perceived themselves as key role models for their adolescents, they see themselves as increasingly alienated, isolated and powerless in this role" (Shanahan and Hewitt 1999: 29). Parents are faced with the dilemma, on the one hand, of introducing their children to alcohol in an effort to encourage moderation, or alternatively, going against the normative tide and attempting to encourage their adolescents not to use alcohol until they reach the legal age.
Six conclusions for policies and practice
The final task of this review is to present conclusions for policies and practice which might assist parents more effectively to guide adolescents towards responsible alcohol use, based on the evidence emerging from this review.
Conclusion 1
Parents should be provided with information concerning the advantages of delaying the age at which young people begin using alcohol.
Based on the available research, there appear to be clear advantages in delaying the age at which young people begin using alcohol. Among these are the reduced likelihood of high risk alcohol use and abuse in adulthood, averting the adverse impacts of alcohol on the developing adolescent body and brain (Scott and Grice 1997), and avoiding the immediate risks to health and wellbeing conveyed by "normal" patterns of adolescent alcohol use (which are often at risky or high risk levels). It is unclear whether parents are aware of this evidence. Publicising this information within a social marketing framework could be a useful way of disseminating such information. This could be augmented by further research investigating under what contexts parents are able to minimise the harmfulness of youth alcohol use.
It is not possible to recommend a particular age at which adolescent alcohol use could commence, due to the great variability in young people's development and the circumstances in which they are growing up. For example, the developing bodies and brains of late maturing adolescents may potentially be exposed to greater alcohol-related harms than those of early maturing adolescents if late maturing adolescents participate in binge drinking from early adolescence onwards. However, it is clear that early adolescent alcohol use in unsupervised peer group situations is to be discouraged.
Thus there appear to be three key messages for parents:
- There is a high risk of long-term harmful consequences if adolescent alcohol use commences early. Compelling evidence now exists that early onset is related to more risky patterns of use in the long-term, while delaying the onset of alcohol use is associated with more moderate and less risky patterns of use in adulthood.
- The child's stage of development, and the degree to which he or she is still going through the developmental changes that occur in adolescence, should be considered. Information that the developing adolescent body copes less well with alcohol than the adult body and that physiological harms can occur should be made available to parents and adolescents.
- Alcohol use should be seen as part of the wider adolescent context, and merely delaying its onset may not be effective on its own. Alternative activities and opportunities, particularly in the peer context, may need to be negotiated and provided. There is also scope for the introduction of youth development programs, local community programs, Big Brother, Big Sister intergenerational programs and similar initiatives to promote healthy youth development.
Conclusion 2
Parents should be provided with educative guidelines on the influence of parental attitudes and norms on adolescent alcohol use, as well as guidance in managing the social pressure they feel to allow their adolescents to consume alcohol.
Parents report feeling adverse social pressure and not having the confidence to assist children and adolescents to wait until they reach the legal age before initiating alcohol use. However, the research evidence suggests that parental attitudes and norms can play a considerable role. For example, when parents showed disapproval of alcohol use, their adolescents were less likely to use alcohol; conversely, when parents were tolerant or permissive, their adolescents were more likely to consume alcohol. Other research showed that parents who felt empowered were more likely to share decisions about adolescent alcohol consumption and were also more likely to be able to intervene effectively in reducing consumption. Empowerment can arise from increased knowledge.
Thus, parents should be made aware of the research indicating that their views and opinions about adolescent alcohol use can exert an influence. They might also benefit from more information about the extent of risky alcohol consumption among Australian adolescents, and, in order to provide effective guidance for their adolescents, information about safe versus risky levels of alcohol use. Additionally, knowledge that many Australian parents believe that late adolescence is the appropriate age at which adolescents should be introduced to alcohol might assist parents to resist pressure to permit their adolescent to commence use at an earlier age.
Conclusion 3
Once adolescents have commenced alcohol use, parents should be provided with educative guidelines and support to help them to guide their adolescents in responsible alcohol use.
Once adolescents have started drinking, enhanced parental monitoring appears to be a key factor in minimising risky alcohol use. However, this first requires attention to the parent-adolescent relationship, and simply advising parents to ask more questions may have a detrimental effect in some families. Similarly, educating parents to increase behaviour management (for example, by establishing firm rules) without attending to relationship issues or levels of conflict may also be problematic. It seems more promising for educational initiatives to promote quality interactions and good relationships between parents and adolescents first. Once this is in place, parents can then be supported in developing clear and consistent rules regarding alcohol use, setting age appropriate limits, and maintaining open communication. It is important to acknowledge that this will require personal agency and cooperation from both parents and adolescents.
Given there is strong evidence for delaying youth alcohol use, it does not appear ethical to conduct a research program where parents are encouraged to provide alcohol to young people. In light of the mixed evidence on whether parental provision of alcohol is an effective method for encouraging moderate and responsible use, further "in situ" research is needed to clarify this issue. It may also be possible to conduct research to examine the effectiveness of parental influences in encouraging more moderate alcohol use among adolescents who have been brought to official attention for alcohol related crime, or for parents of youth of legal drinking age.
Conclusion 4
Parent education and family intervention programs should be supported in Australia to assist parents to gain skills for encouraging their adolescents to delay initiation to alcohol use and to adopt less risky patterns of use. Intervention and prevention programs should receive best practice evaluations.
Interventions that have shown promise in the North American context should be adapted, implemented and evaluated in Australia. Existing Australian interventions should also be evaluated for their potential to encourage a delayed age of first alcohol use and more moderate patterns of use. A key starting point appears to be the parent-child relationship. Once good quality parent-child relationships are in place, parents should be supported to develop more effective parental behavioural management practices, and better quality monitoring. Prior to encouraging a wider dissemination of programs, evaluation funding should be provided to enable "gold standard" evaluations including randomised control designs and long-term follow-up, and priority should be given to funding evidence-based programs. Given the finding that many interventions appear to be ineffective, or in some cases harmful, it is important for resources to be given to evaluation research, and for funding to be withdrawn from programs of demonstrated ineffectiveness or harm.
Conclusion 5
Given that broader social norms exert a considerable influence on adolescent alcohol use, strategies to reduce favourable social and cultural attitudes towards under-age alcohol consumption will be needed to support parental efforts.
An extensive educative effort, aimed at changing favourable societal attitudes towards adolescent alcohol use, appears necessary to assist parental efforts to delay adolescents' initiation of alcohol use and to guide responsible subsequent use. Health-related public awareness campaigns have a good track record in Australia, although they have also often been backed by legal penalties. Thus, the incidence of drink driving has been greatly reduced, restrictions regarding cigarette use have been embraced, and Australians have heeded the messages about the dangers of sun exposure. Similar community-level efforts may be needed to modify widespread tolerant attitudes towards adolescent alcohol use. In addition, it will be necessary to target adolescent attitudes regarding alcohol, as research shows that a number of adolescents drink specifically to get drunk at present.
Conclusion 6
More Australian research is needed to promote understanding of the developmental processes and pathways to adolescent alcohol use. In particular, research on the development of adolescent alcohol use in Indigenous communities is seriously lacking.
At present, there is a critical lack of Australian data on the pathways to differing patterns of alcohol use, and the role that parents play. There is considerable Australian research on the epidemiology of adolescent alcohol use, but a lack of Australian research into developmental processes, especially as they relate to parents. Thus, the international research, particularly that of the United States, is relied upon to a large extent. Yet there are important differences, particularly relating to cultural norms and attitudes, which may dilute the transferability of the international research to the Australian context. There is also a critical lack of Australian research evaluating promising intervention initiatives. All in all, there is an urgent need for more Australian research on these issues.
In particular, there is almost no research involving Indigenous adolescents and parents. While it is known that fewer Indigenous adolescents consume alcohol, it is also apparent that when they do so, they tend to consume at riskier levels, suggesting that particular efforts may be required to change the developmental pathways of these young people. Useful information could also be gained from the study of particular community, cultural and religious groups in which adolescents adhere to norms against adolescent alcohol use. What can be learnt from these adolescents, and how do these parents transmit their values? While there has been research into the reasons underlying adolescents' use of alcohol, the impact of parenting behaviours on adolescent motivations to drink, and the influence that parents might have on these motivations, are not well understood. Thus, a range of issues remain poorly understood and a greater investment in research in this area would appear to be crucial.
Appendices
Appendix 1
List of databases searched
- AEI (Australian Education Index)
- AFSA (Australian Family and Society Abstracts)
- Alcohol and Alcohol problems Science Database - ETOH
- APAIS (Australian Public Affairs Information Service)
- Article First (OCLC Article First)
- Australian Criminology Database
- Caredata
- Cochrane Library
- Campbell Collaboration
- ERIC (Educational Resources Information)
- Family & Society Studies Worldwide - CD Rom and Web
- Ingenta
- MDX Health Digest (MDXHealth) - OCLC
- Medline / PubMed
- PAIS (Public Affairs Information Service)
- ProceedingsFirst (OCLC)
- ProQuest
- PsycARTICLES
- PsychInfo
- ScienceDirect
- Sociological Abstracts
- SocSciSearch
- Wilson Social Science Abstracts
Appendix 2
Personal communication with organisations or their representatives
- Australian Drug Foundation
- Australian Institute of Criminology
- Australian National University
- Brotherhood of St Laurence
- Department of Health and Ageing
- Edith Cowan University
- LaTrobe University
- National Drug and Alcohol Research Centre
- National Drug Research Institute
- South Australian Aboriginal Drug and Alcohol Council
- The Cancer Council of Victoria
- University of Queensland
- Victorian Parenting Centre
- Victorian Premier's Drug Prevention Council
- Women's and Children's Hospital Adelaide
Appendix 3
Internet sites searched
Australian sites
- Australian Clearinghouse for Youth Studies
- Australian Drug Foundation
- National Drug and Alcohol Research Centre (NDARC)
- Indigenous Australian Alcohol and Other Drug Database
- National Drug Research Institute
- Australian Institute of Health and Welfare
- Auseinet
- Queensland Alcohol and Drug Foundation
- Crime Prevention Victoria Knowledge Bank - Drug and Alcohol
- Australian Drug Information Network (ADIN)
- National Drug Strategy (NDS)
- Turning Point Alcohol and Drug Centre
- Institute of Alcohol Studies (IAS)
International sites
- National Clearinghouse for Alcohol and Drug Information (USA)
- Alcohol Advisory Council of New Zealand (NZ)
- National Institute on Drug Abuse (USA)
- National Institute on Drug Abuse (NIDA) (USA)
- Virtual Clearinghouse on Alcohol, Tobacco and Other Drugs (VCATOD) (International)
- DrugScope (UK)
Dr Louise Hayes is currently leading a project for the Ballarat Health Service which is examining the effectiveness of community-wide early intervention programs for children with emerging disruptive behaviour disorders. Prior to this, she was a Research Fellow at the Australian Institute of Family Studies and the Victorian Parenting Centre. Louise's research interests include parenting, adolescent and child development; with a special interest in working with families who are experiencing child behaviour problems or parenting difficulties. Her specialty research area is parental monitoring of adolescent free time activity.
Mrs Diana Smart is a Research Fellow at the Australian Institute of Family Studies, and has been the Project Manager for the Australian Temperament Project since 1988. Her research interests are adolescent and youth development, transitions to young adulthood, developmental pathways and transition points, and the fostering of social competence and social responsibility. Prior to joining the Australian Temperament Project, Diana was a researcher with the Victorian Education Department's Curriculum and Research Branch and the Royal Melbourne Institute of Technology's Education Unit, and she lectured in Psychology at Rusden Teachers College.
Associate Professor John W. Toumbourou is a senior researcher at the Centre for Adolescent Health, Royal Children's Hospital, and a member of the Department of Paediatrics at the University of Melbourne. He is a founding member and the current Chair of the College of Health Psychologists within the Australian Psychological Society. John is a principal investigator on a number of studies investigating healthy youth development, including the Australian Temperament Project and the International Youth Development Study (a collaborative longitudinal study with the University of Washington), and has been involved in the development of a number of youth health promotion programs.
Associate Professor Ann Sanson is an Associate Professor in the Department of Psychology at the University of Melbourne, where her teaching and research have been in the areas of developmental psychology, developmental psychopathology and conflict resolution. She was formerly Acting Director of the Australian Institute of Family Studies, and is the project director for Growing Up in Australia (the Longitudinal Study of Australian Children) and a leading investigator of the Australian Temperament Project. Ann is a fellow of the Australian Psychological Society, and has had leadership roles within the society including terms as Vice-President and Director of Social Issues.
The authors would like to thank Dr Catherine Spooner of the National Drug and Research Centre at the University of New South Wales, and Associate Professor Alan Ralph of the Parenting and Family Support Centre at the University of Queensland, for their very helpful comments on an earlier draft of this Report. Any misinterpretations or errors contained in the report are the responsibility of the authors.
Hayes, L., Smart, D., Toumbourou, J. W., & Sanson, A. (2004). Parenting influences on adolescent alcohol use (Research Report No. 10). Melbourne: Australian Institute of Family Studies.
0 642 39517 9
15 December 2004