What is an evidence-informed approach to practice and why is it important?
You are in an archived section of the AIFS website
This is the first short article in a series focusing on the use of evidence in practice. This article discusses the role of research in the context of evidence-informed practice and describes the different types of research typically used.
Service providers and practitioners in the child, family and welfare sector are increasingly being asked to incorporate research evidence into their decisions about service and program design and delivery to facilitate positive outcomes for children and families. They are also encouraged to demonstrate how their use of evidence informs their activities, evaluation and reporting to contribute to intended program outcomes.4,5 This short article describes the role of research within an evidence-informed approach to practice and introduces the different types of research that can be used in decision making.
What is an evidence-informed approach to practice?
An evidence-informed approach to practice can be defined as the integration of research evidence alongside practitioner expertise and the people experiencing the practice (e.g. child and parent using a service or program)3,7 (see Figure 1). Blending knowledge from different sources is an inclusive and useful approach because knowledge is personal, context driven and evolving.6 This type of approach also allows for innovation and adaptation based on factors and context at individual, organisational and service levels, while reducing biases.
Figure 1: Evidence-informed approach to practice
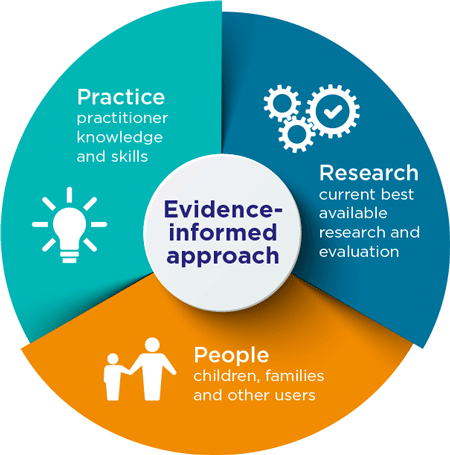
The inclusion of research in evidence-informed decision making is important because it provides credible knowledge that has been created through rigorous methods. This means applying scientific principles of proof, reliability and ethical standards to ensure quality.1,2 Practice evidence is important because it uses practitioner expertise (skills and knowledge) and practical experience in the delivery of solutions.8 When practice evidence is combined with research evidence, it reduces biases. This may include cognitive bias (an inability to be objective that manifests in inaccurate judgement) and confirmation bias (a focus on evidence that fits our beliefs and disregards what does not).2 This approach is further strengthened by incorporating the views of stakeholders and end users. For example, the lived experience of a child and their family accessing a service for a health issue.
Different types of research
The inclusion of research in decision making helps balance professional and service user opinions, so that decisions are less biased. It can help design more effective programs and services, increase accountability and support funding sustainability. There are eight common types of research evidence used in social and health care research. These are listed in Table 1, along with a short description. Each of these types of research can be useful as a source of evidence.
It is helpful to be aware that each type of evidence has strengths and limitations when used in context (see the next short article in this series). To overcome any limitations, using different types of research in a complementary manner or synthesising existing research can be useful.
| Type of research | Description |
|---|---|
| Qualitative research | Involves verbal descriptions of characteristics, cases and settings. Typically uses observation, interviewing or document analysis to examine quality, meaning or context. |
| Surveys | A representative group of people surveyed at one point in time commonly using a survey questionnaire. |
| Case-control studies | Compares a group who has, for example, a health condition with a group of people who do not; and looks back in time to see how characteristics of the two groups differ. |
| Cohort studies | The same group of people surveyed over several points over time, sometimes from childhood to old age. |
| Randomised control trials (RCTs) | One group receives an intervention while another does not receive that intervention or receives a different intervention; groups are formed using a random process, usually with the same chance of being allocated to either group. |
| Quasi-experimental studies | Compares a group who, for example, receives an intervention with a group of people who do not; and explores how characteristics of the groups differ. Differs from RCTs as participants are not randomly assigned to groups. |
| Non-experimental studies | Retrospective studies that do not include an intervention or random assignment of participants into groups. |
| Systematic reviews | Synthesis of results from studies selected systematically based on predetermined criteria and methods reviewed. |
Sources: Blanchet et al. (2018) and Nutley et al. (2013)
Conclusion
An evidence-informed approach blends knowledge from research, practice and people experiencing the practice. Understanding the strengths and limitations of research can facilitate its effective use as part of an evidence-informed approach to practice. It is helpful for practitioners to be familiar with the common types of research evidence to be able to critically assess the appropriateness to their work. The second article in this series describes how to incorporate research into decision making and the practice relevant questions that can guide this process.
Further reading and related resources
- What counts as good evidence?
This report by the Alliance for Useful Evidence explains the use of evidence and the different approaches for identifying evidence in practice. - Evaluation and Expert Panel project resources
These AIFS resources help service providers with research and evaluation initiatives. - Evidence, evidence-based programs and evaluation
This CFCA webinar covered various aspects of research evidence use in practice.
References
1. Baillie, L., Carrick-Sen, D., Marland, A., & Keil, M. F. (2019). Research and evidence-based practice: The nurse’s role. In S. Llahana, C. Follin, C. Yedinak, & A. Grossman (Eds.), Advanced practice in endocrinology nursing. Cham, Switzerland: Springer.
2. Blanchet, K., Allen, C., Breckon, J., Davies, P., Duclos, D., Jansen, J. et al. (2018). Using research evidence in the humanitarian sector: A practice guide. London, UK: Evidence Aid, London School of Hygiene and Tropical Medicine and Nesta (Alliance for Useful Evidence).
3. Boaz, A., Davies, H., Fraser, A., & Nutley, S. (Eds.). (2019). What works now? Evidence-informed policy and practice. Bristol, UK: Policy Press.
4. Department of Social Services (DSS). (2017). Families and Communities Program: Families and Children Guidelines overview. Canberra: DSS. Retrieved from www.dss.gov.au/sites/default/files/documents/12_2017/program_guidelines_overview_-_families_and_children.pdf
5. Department of Social Services. (2020). Families and children services: Discussion paper 2020. Canberra: DSS. Retrieved from engage.dss.gov.au/wp-content/uploads/2020/11/FaC-reform-discussion-paper-for-publication-1.pdf
6. Nutley, S., Powell, A., & Davies, H. (2013). What counts as good evidence? Provocation paper for the alliance for useful evidence. St Andrews, UK: Nesta (Alliance for Useful Evidence).
7. Ontario Centre of Excellence for Child & Youth Mental Health (OCECYMH). (2019). Glossary. Ontario, Canada: Ontario Centre of Excellence for Child & Youth Mental Health. Retrieved from www.kmbtoolkit.ca/glossary-glossaire#undefined
8. Samson, P. L. (2015). Practice wisdom: The art and science of social work. Journal of Social Work Practice, 29(2), 119–131.
© GettyImages/Drazen_
16 March 2021