Gambling participation and harm among Australian men
Ten to Men Insights #2 Report: Chapter 1
Overview
Gambling is a major public policy issue in Australia, affecting the health and wellbeing of many individuals and families (Australian Institute of Health and Welfare [AIHW], 2021). Gambling-related harms can range from financial, relationship or psychological issues to serious legal or health issues (Murray Boyle, Joshi, & Jenkinson, 2021). Such consequences not only affect the people who gamble but also their families, peers and the wider community (AIHW, 2021). Recent estimates suggest that Australians lose approximately $25 billion on legal forms of gambling every year, representing the largest per capita losses in the world (Queensland Government Statistician's Office, 2021). In Victoria alone in 2014/15, the social costs of gambling, including adverse emotional, psychological, relationship and family wellbeing outcomes, are estimated to be about $7 billion (Browne et al., 2017).
An emerging body of research has examined behavioural and social factors associated with gambling problems. Gambling problems are commonly assessed via the Problem Gambling Severity Index (PGSI) (Ferris & Wynne, 2001). The PGSI provides an indication of 'at-risk' or 'problem' gambling during the previous 12 months; individuals classified as 'at-risk' gamble at a level that can cause adverse consequences. Males, particularly during early adulthood, are more likely to be classified 'at-risk' than other subpopulations, though all demographic groups are exposed to some degree of gambling risk (Browne et al., 2019; Hing, Russel, Vitartas, & Lamont, 2015; Jenkinson, de Lacy-Vawdon, & Carroll, 2018, Jenkinson, Sakata, Khokhar, Tajin, & Jatkar, 2020).
The consumption of alcohol, tobacco and other drugs are among the most common behavioural factors associated with gambling risk. Substance use and symptoms of poor mental health (e.g. depression, anxiety) have been found to be more prevalent among at-risk or problem gambling subpopulations than in the general population. For example, a recent study of Australian university students identified hazardous alcohol use and past-year substance use as significant predictors of problem gambling (Dowling, Aarsman, & Merkouris, 2021). Another study of US adults found problem gambling to be highly correlated with dependence on alcohol, cannabis and tobacco (Barnes, Welte, Tidwell, & Hoffman, 2015). Systematic review findings have also shown that problem gambling rates are generally higher in populations with substance use disorders and other psychiatric diagnoses (Loo, Kraus, & Potenza, 2019).
A number of studies provide evidence to support an increased likelihood of mental health diagnoses and associated behaviours among people gambling at 'at-risk' or 'problem' levels. Men gambling at a risky level are typically at greater risk of these diagnoses and behaviours, which can include depression, obsessive compulsive disorder, alcohol dependence and illicit drug use (Afifi, Nicholson, Martins, & Sareen, 2016; Barnes et al., 2015; Hing, Russell, & Browne, 2017). Similarly, studies on the prevalence of co-morbid psychiatric disorders among gambling treatment-seeking populations have found generally high rates of anxiety disorders, mood disorders and substance use disorders (Dowling et al., 2015; Rodriguez-Monguio, Errea, & Volberg, 2017).
Gambling at a risky level can also impact the financial wellbeing of people who gamble and their family members. Financial harms associated with gambling include reduced funds for essential family expenditures or recreational activities, loss of savings or wealth, debt, circumstances that force people into lowered standards of living, and involvement in illegal activities (Barnard et al., 2014; Mathews & Volberg, 2013).
Despite increasing evidence of co-occurring behaviours and harms among populations of people who gamble, limited research has examined gambling participation and associated harms, including alcohol and other drug use, mental ill-health and experience of financial stress among Australian males at a national level. The Ten to Men (TTM) dataset provides a unique opportunity to address this gap.
Key messages
-
Of Australian men aged 18-63 years, 44% had gambled in the past 12 months in 2020/21.
-
One in four men who gambled (around 739,511 Australian men) were classified as being at risk of, or experiencing, problem gambling in the past year. Almost one-quarter (26%) of these men also experienced financial stress during that time.
-
Most men who gambled spent money on multiple activities, including horse racing (56%), poker machines (54%) and sports betting (46%).
-
Men most frequently gambled on sports betting, horse racing and greyhound racing.
-
Engaging in at-risk or problem gambling was significantly associated with:
- recent financial stress (two times more likely)
- more frequent gambling (1.71 times more likely) and gambling on a higher number of activities (1.32 times more likely)
- drinking alcohol at harmful levels in the past year (1.25 times more likely)
- past-year depression (1.58 times more likely).
Research objectives
This chapter of the Insights #2 report used data from TTM to examine:
- the prevalence, frequency and characteristics of gambling participation among Australian men (aged 18-63) in 2020/21.
- the prevalence of 'at-risk or problem gambling' ('ARPG') among Australian men who gambled in 2020/21.
- associations between ARPG and:
- alcohol, tobacco and illicit drug use (past and current use; 2013/14-2020/21)
- negative mental health experiences (past and current experiences; 2013/14-2020/21)
- financial stress (current; 2020/21)
- socio-demographic, behavioural and mental health predictors of ARPG among Australian men who gambled in the past 12 months in 2020/21.
Method
This section describes the key measures and data analysis techniques used to address the above objectives. Information regarding the overall methodology of the TTM study is detailed elsewhere (e.g. Bandara, Howell, Silbert, & Daraganova, 2021; Swami et al., 2022).
Measures
Gambling
Survey questions regarding gambling participation and experience of at-risk and problem gambling (ARPG) were included for the first time in the Wave 3 (2020/21) survey. Recent (past 12 months) gambling participation was derived from responses regarding frequency of involvement in eight types of gambling activities (see Box 1.2); that is, spending money on gambling at least once on any of the activities was coded as '1', and '0' indicated no gambling participation.
Gambling risk was assessed using the nine-item Problem Gambling Severity Index (PGSI; see Box 1.3); a score of 1 or more was characterised as 'at-risk or problem gambling', and '0' as non-problem gambling (Ferris & Wynne, 2001).
Mental health and wellbeing
At each of the first three data collection waves, past-year ('recent') experience of both depression and anxiety was captured by asking, 'Have you been treated for or had any symptoms of [condition] in the past 12 months?'.
'Current' depression (past two weeks) was assessed at each wave using the Patient Health Questionnaire-9 (PHQ-9; Kroenke, Spitzer, & Williams, 2001). Based on the total PHQ-9 score (0-27), participants were categorised into either 'moderate to severe' or 'no or mild' depression.
Current anxiety was captured only at Wave 3 using the Generalised Anxiety Disorder-7 scale (GAD-7; Spitzer et al., 2006). In consideration of participants' total GAD-7 score (0-21), they were categorised as experiencing either 'moderate to severe' or 'no or mild' anxiety in the past two weeks.
Life satisfaction was assessed at each wave using the Personal Wellbeing Index (PWI; International Wellbeing Group, 2013).
Alcohol and other substance use
Recent (past year) harmful drinking was measured using the Alcohol Use Disorders Identification Test (AUDIT). See Box 1.1 below for details of alcohol and other drug measures used in this report.
Box 1.1: Surveying TTM participants about harmful or hazardous drinking, illicit drug use and tobacco smoking
Alcohol consumption
At each data collection wave, harmful or hazardous drinking among TTM participants was measured using the Alcohol Use Disorders Identification Test (AUDIT). The AUDIT is a 10-item questionnaire used to screen for excessive drinking practices (Babor et al., 2001). It is used widely by health workers and researchers in Australia and internationally. Items assess various components or outcomes of alcohol use including:
- hazardous consumption levels (e.g. 'How often do you have six or more drinks on one occasion?')
- alcohol dependence (e.g. 'How often during the last year have you found that you were not able to stop drinking once you had started?')
- experience of related harms (e.g. 'Have you or someone else been injured as a result of your drinking?').
Total AUDIT scores range from 0-40. Scores of 8 or more indicate harmful/hazardous drinking patterns.1
Illicit drug use
TTM participants are asked about their use of different illicit drugs at each data collection wave. In this chapter we only report on past-year ('recent') use of cannabis, meth/amphetamine ('speed' powder, crystal methamphetamine/'ice'), ecstasy and cocaine because these are the four drugs that adult participants were consistently asked about at Waves 1-3.
For comprehensive information about drug use among Australian men using data from the first three waves of TTM data collection, please see chapter 3 of this report.
Smoking status
Adult (18+) participants at each wave were asked if they had ever smoked even part of a cigarette. Those who responded with a 'yes' were further asked, 'Do you currently smoke?' (yes/no). 'Cigarettes' excluded electronic cigarettes, cigars, pipes and cannabis but included filtered, 'light' or 'mild' or roll-your-own cigarettes. In this report chapter, 'smoking' refers to the smoking status at the time of interview for a given wave.
Table S1.1 in the supplementary materials summarises the periods of data collection and the TTM participants surveyed for each of the gambling, substance use and mental health measures included in this report.
Data analysis
TTM participants at Wave 3 were aged 18-63 but the upper age limit for those who gambled was 62; therefore, an age range of 18-62 is used when estimates are presented for only the gambling subpopulation, rather than the entire Wave 3 sample.
For research objectives 1 and 2 (using Wave 3 data), weighted cross-tabulations, Chi-square tests (for categorical variables) and t-tests (for continuous variables) were used to examine prevalence estimates and related covariates. To address research objective 3, weighted prevalence (proportions) of alcohol and other drug use and experiences of depression and anxiety in Waves 1, 2 and 3 were reported for adult TTM participants (≥18 years) who gambled in 2020/21, along with significant differences between men classified as engaging in gambling at 'non-problem' and 'at-risk or problem gambling' (ARPG) levels.
Two sequential multivariable logistic regression models were developed using Wave 3 data to identify correlates of ARPG (research objective 4). To fit the most parsimonious model, the modelling strategy was as follows: Model 1 was used to identify significant socio-demographic characteristics. These were retained in Model 2, which additionally tested for the effect of financial stress, gambling frequency and number of activities gambled on, substance use, and mental health and wellbeing variables. Among the mental health measures, only past-year depression and past-year anxiety were included in Model 2, as the time frames (past-year) matched that of the gambling risk measure (PGSI).
1 Alcohol use among Australian males was previously explored in detail - using data only from Waves 1 and 2 - in the Insights #1 report (Quinn, Swami, Terhaag, & Daraganova, G., 2020).
Findings
Prevalence, frequency and characteristics of gambling participation among Australian men
In 2020/21, 44% of Australian men aged 18-63 reported having gambled in the past 12 months (or an estimated 2,751,934 Australian adult males). The average age of those who had recently gambled was 39 years (SD = 12.7) and around 60% were married or lived with a partner (Table 1.1). One-fifth (21%) of men who gambled were born overseas and approximately 4% identified as Aboriginal and/or Torres Strait Islander. Around three-quarters (73%) resided in major cities.
Among men who had recently gambled, most (71%) had completed a post-secondary school qualification; 42% had attained a certificate or diploma, and 29% a university degree. The majority (88%) were employed and almost one-third (30%) had a combined household income of $150,000 or more per annum. More than half (53%) reported a combined household income of $50,000-$149,000.
Compared to adult Australian males who did not gamble in the past 12 months, men who gambled were significantly more likely to be younger, born in Australia, mainly speak English at home and have a higher household income. They were significantly less likely to have a partner, be married or have a university degree. The two groups did not significantly differ in other socio-demographic characteristics.
| Characteristics | % of men who gambled | 95% CI | % of men who did not gamble | 95% CI |
|---|---|---|---|---|
| Gambled past 12 months (TTM Wave 3 sample) | 44% of men gambled | 56% did not gamble | ||
| Age group (years)** | N = 3,339 | N = 4,306 | ||
| 18-24 | 17.1 | [14.9, 19.6] | 13.5 | [11.8, 15.5] |
| 25-34 | 21.9 | [19.6, 24.5] | 22.2 | [20.1, 24.4] |
| 35-44 | 24.7 | [22.4, 27.1] | 21.5 | [19.7, 23.5] |
| 45-54 | 21.7 | [19.9, 23.7] | 24.4 | [22.6, 26.3] |
| 55-63 | 14.6 | [13.1, 16.3] | 18.4 | [16.8, 20.1] |
| Aboriginal and/or Torres Strait Islander | N = 3,316 | N = 4,275 | ||
| 3.5 | [2.5, 4.9] | 2.1 | [1.4, 3.2] | |
| Born outside Australia*** | N = 3,316 | N = 4,278 | ||
| 20.6 | [18.3, 23.1] | 28.2 | [25.9, 30.5] | |
| Language other than English* | N = 3,333 | N = 4,281 | ||
| 6.7 | [5.2, 8.7] | 9.6 | [8.1, 11.5] | |
| State of residence | N = 3,221 | N = 4,143 | ||
| New South Wales | 34.4 | [30.5, 38.4] | 29.9 | [26.6, 33.5] |
| Victoria | 25.3 | [22.1, 28.7] | 26.5 | [23.3, 30.0] |
| Queensland | 19.1 | [16.3, 22.3] | 20.0 | [17.3, 22.9] |
| South Australia | 6.4 | [4.6, 8.9] | 7.8 | [5.9, 10.3] |
| Western Australia | 9.3 | [7.6, 11.5] | 10.5 | [8.7, 12.8] |
| Tasmania | 2.2 | [1.3, 3.6] | 2.8 | [1.7, 4.6] |
| Northern Territory | 0.9 | [0.4, 1.9] | 0.5 | [0.2, 1.5] |
| Australian Capital Territory | 2.4 | [1.4, 4.3] | 1.9 | [1.1, 3.3] |
| ASGS region | N = 3,155 | N = 4,038 | ||
| Major city | 73.3 | [71.1, 75.3] | 74.9 | [72.5, 77.0] |
| Inner regional | 18.2 | [16.4, 20.1] | 17.6 | [15.7, 19.7] |
| Outer regional | 8.5 | [7.5, 9.7] | 7.5 | [6.5, 8.7] |
| Relationship status** | N = 3,262 | N = 4,207 | ||
| Single | 21.5 | [19.0, 24.2] | 22.4 | [20.4, 24.7] |
| In relationship/engaged | 15.2 | [13.3, 17.3] | 10.7 | [9.2, 12.4] |
| Live with partner/married | 60.4 | [57.6, 63.2] | 63.6 | [61.1, 66.0] |
| Widowed/divorced/separated | 3.0 | [2.3, 3.8] | 3.2 | [2.5, 4.1] |
| Highest qualification*** | N = 3,210 | N = 4,160 | ||
| <Year 12 | 12.0 | [10.2, 14.0] | 9.5 | [8.1, 11.2] |
| Year 12 or equiv. | 17.4 | [15.3, 19.7] | 16.2 | [14.4, 18.3] |
| Cert/diploma/other | 41.7 | [39, 44.4] | 38.4 | [36.0, 40.8] |
| Bachelor or higher | 28.9 | [26.5, 31.6] | 35.9 | [33.6, 38.3] |
| Employment status | N = 3,226 | N = 4,163 | ||
| Employed | 88.1 | [86.0, 89.9] | 84.9 | [82.9, 86.6] |
| Unemployed and looking for work | 6.3 | [4.9, 8.0] | 7.7 | [6.5, 9.1] |
| Out of labour force | 5.6 | [4.5, 7.1] | 7.4 | [6.2, 8.9] |
| Annual combined household income* | N = 2,999 | N = 3,790 | ||
| $200,000+ | 16.0 | [14.1, 18.1] | 14.4 | [12.8, 16.2] |
| $150,000-$199,999 | 14.3 | [12.5, 16.3] | 14.0 | [12.5, 15.8] |
| $100,000-$149,000 | 27.4 | [25.0, 30.1] | 24.2 | [22.0, 26.4] |
| $50,000-$99,999 | 26.0 | [23.6, 28.6] | 27.4 | [25.2, 29.7] |
| $49,999 or less | 16.2 | [14.1, 18.6] | 20.0 | [17.9, 22.2] |
Notes: N > 2,999; ASGS = Australian Statistical Geography Standard; CI = confidence interval. Significant differences between the gambling and non-gambling groups at three alpha levels are noted by: *p < .05, **p < .01, ***p < .001.
Source: TTM data, Wave 3, adult cohort, weighted
Box 1.2: Participation in, and frequency of, gambling activities measured in the Wave 3 TTM survey
Gambling is an activity where a person places a 'stake' (i.e. money or other items of value) on a chance or mixed chance/skill outcome in the hope of winning a prize (i.e. money or something of monetary value) (Gambling Regulation Act 2003). In this chapter, 'gambling' refers to spending money on land-based products - for example, 'pokies' - or online gambling, not on gambling informally with friends.
At Wave 3 (2020/21) of TTM, participants were asked about how often they spent money on eight different gambling activities in the past year:
Activities
Horse racing, poker machines, sports betting, greyhound racing, casino table games, poker, esports betting, fantasy sports betting.
Frequency of participation
TTM participants were asked to specify how often they had spent money on each activity in the past year: 1) never, 2) once or twice, 3) a few times, 4) once a month, 5) 2-3 times a month, 6) once a week, 7) 2-3 times a week, and 8) 4 or more times a week.
The prevalence and frequency of participation in eight different types of gambling activities (see Box 1.2) among adult Australian males in 2020/21 are shown in Figures 1.1a and 1.1b, respectively. The most common activities that men recently gambled on were horse racing (56%), poker machines (54%) and sports betting (46%) (Figure 1.1a). Most men who gambled (60%) spent money on multiple gambling activities (two activities on average); about one-quarter (23%) spent money on two activities, 15% on three, and 22% on four or more gambling activities.
Regarding gambling frequency, differences were observed when examined by type of activity (Figure 1.1b2 Adult men gambled most frequently on sports and horse and greyhound racing during the past 12 months, and least frequently on pokies, poker and casino table games.
Differences in the average age of men who gambled were observed for different gambling activities. Men who spent money gambling on horse racing (avg. age = 41 years), sports betting and poker machines (avg. age = 39 years, each) tended to be older than men who gambled on esports and fantasy sports (32 and 33 years, respectively).
Figure 1.1: Estimated prevalence (%) of a) participation in gambling activities among adult Australian men (18-623 years) and b) frequency of participation by gambling activity type among men who gambled in the past 12 months, 2020/21
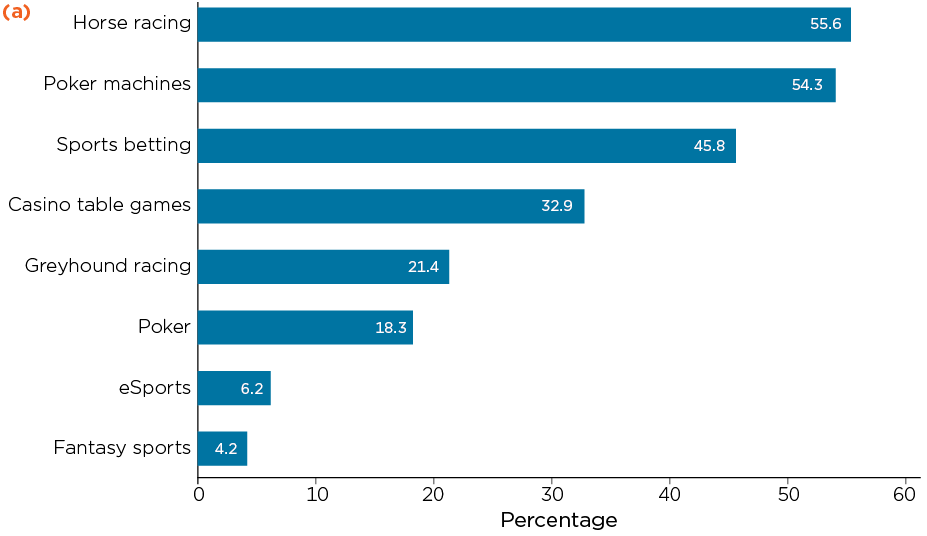
Notes: N = 3,339; Estimated prevalence for an activity does not represent sole participation in that activity.
Source: TTM data, Wave 3, adult cohort, weighted
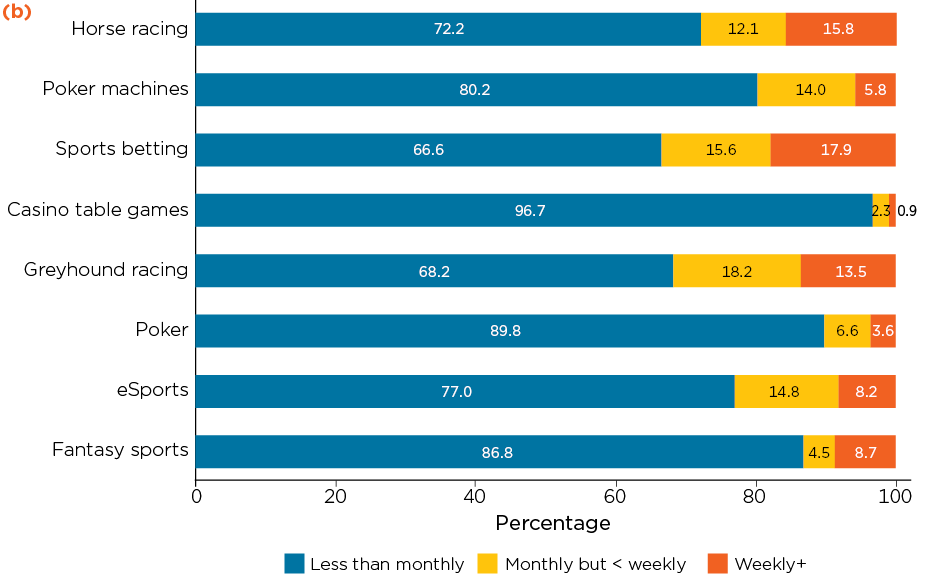
Notes: Horse racing (N = 2,036), poker machines (N = 1,666), sports betting (N = 1,473), casino table games (N = 973), greyhound racing (N = 728), poker (N = 496), esports (N = 129) and fantasy sports (N = 110).
Source: TTM data, Wave 3, adult cohort, weighted.
Box 1.3: Measuring gambling-related harms: the Problem Gambling Severity Index (PGSI)
The PGSI consists of the following nine items (questions) relating to gambling behaviour in the past 12 months, with response options being never (coded as 0), sometimes (1), most of the time (2) and almost always (3):
- How often have you bet more than you could really afford to lose?
- How often have you needed to gamble with larger amounts of money to get the same feeling of excitement?
- How often have you gone back another day to try to win back the money you lost?
- How often have you borrowed money or sold anything to get money to gamble?
- How often have you felt that you might have a problem with gambling?
- How often have people criticised your betting or told you that you had a gambling problem, regardless of whether or not you thought it was true?
- How often have you felt guilty about the way you gamble or what happens when you gamble?
- How often has your gambling caused you any health problems, including stress or anxiety?
- How often has your gambling caused any financial problems for you or your household?
Individual item scores are summed to achieve a total score ranging between 0 and 27. Respondents are grouped into four categories based on their total scores: non-problem gamblers (0), low-risk gamblers (1-2), moderate-risk gamblers (3-7), and problem gamblers (8-27). Respondents who score 1+ may be classified as being at some risk of, or already experiencing, gambling-related problems. As mentioned earlier, we refer to this group as at-risk or problem gamblers (ARPG) throughout this report.
Prevalence of 'at-risk or problem gambling' (ARPG) among Australian men who gamble
Experience of gambling-related problems is commonly assessed via the Problem Gambling Severity Index (PGSI) (Ferris & Wynne, 2001). As detailed in Box 1.3, the PGSI provides a measure of 'problem' or 'at-risk' gambling during the previous 12-month period. TTM participants who had spent money on any of eight gambling activities in the past year (see Box 1.2) were categorised as engaging in either non-problem gambling, low-risk gambling, moderate-risk gambling or problem/high-risk gambling.
In 2020/21, more than one-quarter (27%) of adult Australian males who gambled in the past 12 months, equivalent to around 739,511 men, were classified as being at some risk of experiencing gambling problems/harms (Table 1.2). The estimated prevalence rates for the three risk categories for Australian men who had recently gambled were: low-risk (17%), moderate-risk (7%) and high-risk/problem gambling (3%). Among men who had recently engaged in specific types of gambling activities, 38% of those who engaged in sports betting were categorised as ARPG, as were 33% of those who used pokies and 31% of those who bet on horse races.
| PGSI risk group | n | % of men who gambled | 95% CI |
|---|---|---|---|
| Non-problem gambling | 2,505 | 72.9 | [70.3, 75.4] |
| Low risk | 491 | 16.7 | [14.8, 18.9] |
| Moderate risk | 247 | 7.3 | [5.9, 9.0] |
| High risk or problem gambling | 81 | 3.1 | [2.2, 4.3] |
| ARPG | 819 | 27.1 | [24.6, 29.7] |
Notes: N = 3,324. TTM participants without valid responses to the PGSI items were excluded from analyses (n = 15); ARPG = at-risk or problem gambling; CI = confidence interval; PGSI = Problem Gambling Severity Index
Source: TTM data, Wave 3, adult cohort, weighted
Associations between ARPG and behavioural, health and financial factors
Alcohol, tobacco and illicit drug use
This section examines patterns of alcohol and other drug use across the first three TTM waves (2013/14, 2015/16 and 2020/21) among Australian males classified as ARPG in 2020/21 (Wave 3 of TTM).
Analyses focused on recent (past year) harmful drinking, measured by the AUDIT (see Box 1.1), recent use of four key illicit drugs - cocaine, ecstasy, cannabis and meth/amphetamine, and tobacco smoking status (Box 1.1), for each of the three waves. Estimates in Table 1.3 are for adult Australian males (18 years or over) from each of the three time points of TTM data collection.4
| Substance | 2013/14 | 2015/16 | 2020/21 | |||
|---|---|---|---|---|---|---|
| % of ARPG | % of non-problem | % of ARPG | % of non-problem | % of ARPG | % of non-problem | |
| Any substance (excl. smoking) (ARPG N = 676, Non-problem N = 2,210) | 58.6** | 49.6 | 58.2** | 47.3 | 63.6*** | 48.8 |
| Harmful drinking (ARPG N = 492, Non-problem N = 1,599) | 55.5* | 45.8 | 53.5** | 41.9 | 54.8*** | 40.9 |
| Any illicit drugs (At-risk N = 588, Non-problem N = 1,948) | 30.7* | 23.2 | 35.6** | 25.5 | 38.4*** | 25.8 |
| Cannabis (ARPG N = 583, Non-problem N = 1,957) | 27.6* | 21.3 | 29.3* | 21.6 | 28.1* | 20.3 |
| Cocaine (ARPG N = 657, Non-problem N = 2,153) | 6.4 | 4.7 | 9.3 | 6.9 | 14.8** | 8.8 |
| Ecstasy (ARPG N = 658, Non-problem N = 2,145) | 7.4 | 4.6 | 11.0 | 6.7 | 9.4* a | 5.2 |
| Meth/amphetamine (ARPG N = 506, Non-problem N = 1,777) | 7.6** | 3.1 | 14.8*** | 4.1 | 12.4*** | 3.1 |
| Smoking(ARPG N = 403, Non-problem N = 1,304) | 37.0** | 26.5 | 38.1** | 26.6 | 33.8** | 22.8 |
Notes: ARPG = at-risk or problem gambling; CI = confidence interval. Asterisks (*) denote significant differences between at-risk/problem gambling (ARPG) and non-problem gambling groups in the corresponding wave, *p < .05, **p < .01, ***p < .001. Chi-square tests were used for significance testing. 'Any illicit' was derived from cannabis, cocaine, meth/amphetamine and ecstasy variables, coded '1' if used any of these substances, and '0' if a participant nominated 'no' for one or more of these substances and had missing data for the rest. 'Any substance' was derived from harmful drinking and 'any illicit' variables, coded '1' if used any of these substances, and '0' if a participant nominated 'no' for one or more of these substances and had missing data for the rest. a p = .0463, which rounds to .05.
Source: TTM data, Waves 1, 2 and 3, adult cohort, weighted; includes adults (aged 18+) at W1 who gambled at W3. Balanced data for each row; i.e. each row only includes data from participants with valid data for both the PGSI and the substance in that particular row for all three waves.
Among Australian men classified as engaging in ARPG, the prevalence of any substance (alcohol and illicit drugs) use increased between 2013/14 and 2020/21 (59% to 64%). More than half of men in the ARPG group (54% to 56%) drank alcohol at a harmful or hazardous level in each of the three time points. The prevalence of illicit drug use among the ARPG group also increased significantly from 31% in 2013/14 to 38% in 2020/21.
More specifically, among men engaging in ARPG, recent use of cocaine increased more than twofold from 6% in 2013/14 to 15% in 2020/21. Between 2013 and 2016, meth/amphetamine use almost doubled (8% to 15%) and ecstasy use increased (7% to 11%) among this group, before recent use of both drugs reduced in 2020/21 (albeit levels remained higher than those recorded in 2013/14). In comparison, harmful drinking and cannabis use remained relatively stable, whereas tobacco smoking decreased slightly (37% to 34%) between 2013/14 and 2020/21; almost similar patterns were observed for the non-problem gambling group in relation to the use of alcohol, cannabis and tobacco (Table 1.3).
Adult males who were classified as ARPG in 2020/21 were significantly more likely to have drunk alcohol at harmful levels, used some illicit substances and to have smoked tobacco in 2013/14, 2015/16 and 2020/21, in comparison with men who gambled at non-problem levels. Across the three time points, rates of any substance use ranged between 58% and 64% for the ARPG group, compared to between 47% and 50% for men classified as engaging in non-problem gambling (Table 1.3). For meth/amphetamine use, the estimated rates for the ARPG and non-problem gambling participants were 8%-15% and 3%-4%, respectively. The only exceptions were cocaine and ecstasy use at Waves 1 and 2 where there was no difference in use between ARPG and non-problem groups.
Mental health and wellbeing
This section investigates the prevalence of depression and anxiety and levels of life satisfaction (personal wellbeing) across 2013/14-2020/21 among Australian men who had recently gambled in 2020/21 and were classified as either ARPG or in the non-problem gambling group. Experience of both depression and anxiety were assessed for two time periods; past-year ('recent') and past two weeks ('current').
Across all three time points, a significantly higher proportion of men engaging in ARPG were estimated to have experienced recent (past 12 months) and current (past two weeks) depression and anxiety than men in the non-problem gambling group, with the only exception observed for recent anxiety in 2020/21 (Table 1.4). For example, in 2020/21, 16% of ARPG men experienced recent depression (vs 9% of non-problem), 21% experienced moderate to severe current depression (vs 12% of non-problem), and 13% reported moderate to severe current anxiety in the past two weeks (vs 8% of non-problem) (Table 1.4).
| Condition | 2013/14 | 2015/16 | 2020/21 | |||
|---|---|---|---|---|---|---|
| Among ARPG % | Among non-problem gamblers % | Among ARPG % | Among non-problem gamblers % | Among ARPG % | Among non-problem gamblers % | |
| Past-year depression (At-risk N = 712, Non-problem N = 2,250) | 15.7*** | 9.3 | 19.8*** | 10.5 | 16.1*** | 8.9 |
| Moderate to severe depression (PHQ-9) (At-risk N = 715, Non-problem N = 2,223) | 16.1*** | 8.8 | 16.6** | 10.1 | 20.6*** | 11.5 |
| Past-year anxiety (At-risk N = 714, Non-problem N = 2,243) | 10.4** | 5.8 | 11.8** | 6.3 | 8.1 | 7.2 |
| Moderate to severe anxiety (GAD-7) a (At-risk N = 805, Non-problem N = 2,479) | - | - | - | - | 12.8** | 7.6 |
Notes: a Not assessed at Waves 1 and 2 of TTM; ARPG = at-risk or problem gambling; CI = confidence interval. Asterisks (*) denote significant differences between at-risk/problem and non-problem gambling groups, *p < .05, **p < .01, ***p < .001. Chi-square tests were used for significance testing.
Source: TTM data, Waves 1, 2 and 3, adult cohort; men who had recently gambled at W3, weighted. Balanced data for each row, i.e. cases who had gambled at W3 and had valid data for all three waves
Although significantly more men who were classified as engaging in ARPG experienced depression and anxiety compared to the non-problem group at each time point, the prevalence within an individual group remained relatively stable across the three time points between 2013 to 2021. For example, prevalences of past-year depression were 16%, 20% and 16% among the ARPG group, and 9%, 11% and 9% among the non-problem gambling group in 2013/14, 2015/16 and 2020/21 respectively.
Average levels of life satisfaction, measured using the PWI, are reported for adult men based on their at-risk or problem gambling status at 2020/21 in Table 1.5. For all time points, men classified as ARPG reported significantly lower life satisfaction (i.e. lower average PWI scores) compared to the non-problem gambling group; a score of 67 versus 72 in 2013/14, 66 versus 70 in 2015/16, and 65 versus 72 in 2020/21.
| Time point | Mean PWI score [95% CI] | |||
|---|---|---|---|---|
| ARPG gamblers (N = 646) | Non-problem gamblers (N = 2,104) | |||
| 2013/14 | 67.0*** | [65.1, 69.0] | 72.4 | [71.4, 73.2] |
| 2015/16 | 65.8*** | [63.8, 67.7] | 70.3 | [69.4, 71.3] |
| 2020/21 | 65.3*** | [63.2, 67.5] | 72.2 | [71.2, 73.2] |
Notes: ARPG = at-risk or problem gambling; CI = confidence interval. Asterisks (*) denote significant differences between at-risk and non-problem gambling groups, *p < .05, **p < .01, ***p < .001. Independent sample t-tests were used for significance testing.
Source: TTM data, Waves 1, 2 and 3; adults (aged 18+) at W3, weighted. Balanced data for each row, i.e. cases who had gambled at Wave 3 and had valid PWI data for all three waves. PWI asked of adults only.
Experience of financial stress
At Wave 3, TTM participants were asked whether they had experienced different forms of financial stress (multiple-choice items listed in Box 1.4) due to a shortage of money in the past 12 months. Findings are presented in Table 1.6. Similar proportions of men who had recently gambled (18%) and had not recently gambled (19%) reported having experienced at least one type of financial stress in the past 12 months; the two groups did not differ significantly on prevalence of any individual financial stress items (Table 1.6).
However, men classified as ARPG differed significantly to the non-problem gambling population on five of the six financial stress measures (see asterisks (*) in Table 1.6). For example, a significantly higher proportion of ARPG gamblers (26%) experienced financial stress, compared to participants classified as in the non-problem gambling group (15%). Almost one in five (18%) men who were classified as gambling at a risky or problematic level requested financial help from friends or family, 8% could not get medical care, 7% could not pay mortgage/rent on time, and 6% could not fill/collect prescription due to a shortage of money in the past 12 months (Table 1.6).
Box 1.4: Financial stress caused by a shortage of money in the past 12 months, 2020/21
At Wave 3, TTM participants were asked, 'Over the past 12 months did any of the following happen to you because of a shortage of money?' ('Yes' or 'No')?
- Could not fill or collect a prescription medicine
- Could not get a medical test, treatment or follow-up that was recommended by a doctor
- Could not go to the doctor when you needed to
- Could not afford to heat your home
- Could not pay electricity, gas or telephone bills on time
- Could not pay the mortgage or rent on time
- Asked for financial help from friends or family
A binary variable indicating recent experience of 'Any financial stress' (yes/no) was derived from the above items; those who selected 'yes' for at least one of these items received a 1 ('yes'); '0' otherwise.
| Financial stress | By gambling status | By ARPG status | ||
|---|---|---|---|---|
| % of men who gambled [95% CI] | % of men who didn't gamble [95% CI] | % of ARPG men [95% CI] | % of non-problem gambling men [95% CI] | |
| Any financial stress | 17.8 [15.7, 20.1] | 18.5 [16.7, 20.4] | 25.8*** [21.2,31.0] | 15.0 [12.7, 17.6] |
| Asked for financial help | 10.2 [8.6, 12.1] | 9.7 [8.4, 11.1] | 17.6*** [13.8,22.2] | 7.5 [5.9, 10.0] |
| Could not pay bills on time | 7.1 [5.8, 8.6] | 7.1 [6.1, 8.3] | 8.5 [6.0,12.0] | 6.6 [5.2, 8.3] |
| Could not get medical care | 5.1 [4.0,6.5] | 5.8 [4.7, 7.2] | 8.2** [5.6,11.8] | 4.0 [2.9, 5.4] |
| Could not pay mortgage/rent on time | 4.8 [3.6,6.2] | 4.0 [3.2, 4.9] | 7.4* [4.9,11.1] | 3.8 [2.7, 5.5] |
| Could not fill/collect prescription | 3.8 [2.8,5.1] | 4.2 [3,3. 5.4] | 6.4** [4.1,10.0] | 2.8 [1.9, 4.2] |
Notes: ARPG = at-risk or problem gambling; N varies between columns due to varying degrees of missingness. N is between 3,225 and 3,235 for men who gambled, 4,164 and 4,180 for men who didn't gamble, 785 and 790 for ARRG men, and 2,428 and 2,431 for non-problem gambling men. The item 'could not afford to heat your home' was not reported due to low prevalence among people who gamble (n = 29); CI = confidence interval; *p < .05, **p < .01, ***p < .001. Chi-square tests were used for significance testing.
Source: TTM data, Wave 3, adult cohort, weighted
Multivariable analysis: Factors independently associated with at-risk or problem gambling (ARPG)
A multivariable logistic regression model (Model 1; supplementary materials Table S1.4) was developed to identify significant socio-demographic correlates of ARPG in 2020/21 (‘yes’ or ‘no’). Protective factors for at‑risk or problem gambling included having a partner, being employed, having a university degree (reference = less than year 12) and earning a combined household income of $200,000 or more (reference = less than $50,000). The odds of ARPG were 59% higher (aOR = 1.59) among men aged 18–24 and 51% higher (aOR = 1.51) among men aged 25–34, compared to those aged 55 years or over.
Socio-demographic factors that were not significantly correlated with ARGP included Aboriginal and Torres Strait Islander identity, country of birth (Australia vs elsewhere), CALD status and residential location (major cities vs inner and outer regional areas) (supplementary materials Table S1.4).
Significant socio-demographic correlates of ARPG in Model 1 were then entered into a second logistic regression model (Model 2) with gambling behaviour (gambling frequency and number of activities), substance use (past-year harmful drinking and illicit drug use), mental ill-health (past-year depression and anxiety), and past-year experience of financial stress.
In Model 2 (Table 1.7), having experienced any financial stress had the highest positive association with gambling at a risky/problematic level in the past 12 months; men who had recently experienced financial stress had around double the odds of engaging in ARPG (aOR = 1.97, 95% CI [1.50-2.58]). In addition, more frequent gambling (aOR = 1.72, 95% CI [1.61-1.82]), gambling on a higher number of activities (aOR = 1.32, 95% CI [1.23-1.42]), past-year harmful drinking (aOR = 1.25, 95% CI [1.01-1.54]), and past-year depression (aor = 1.58, 95% CI [1.09-2.31]) remained correlated with risky/problematic gambling in the past year (Table 1.7). Having a partner remained protective for ARPG in this analysis (aOR = 0.64, 95% CI [0.49-0.84]).
| Characteristics | aOR | SE | 95% CI |
|---|---|---|---|
| Age (ref. = 55-63) | |||
| 18-24 | 1.20 | 0.26 | [0.78, 1.84] |
| 25-34 | 1.40 | 0.26 | [0.98, 2.03] |
| 35-44 | 1.22 | 0.20 | [0.88, 1.69] |
| 45-54 | 1.19 | 0.18 | [0.88, 1.61] |
| Partnered (ref. = no) | 0.64** | 0.09 | [0.49, 0.84] |
| Highest qualification (ref. = less than year 12) | |||
| Year 12 or equivalent | 1.36 | 0.28 | [0.90, 2.05] |
| Cert./diploma/other | 0.96 | 0.17 | [0.68, 1.36] |
| Bachelor or higher | 1.21 | 0.23 | [0.83, 1.77] |
| Employed (ref. = no) | 0.78 | 0.15 | [0.54, 1.13] |
| Annual combined household income (ref. = less than $50,000) | |||
| $200,000 or more | 0.65* | 0.14 | [0.43, 0.99] |
| $150,000-$199,999 | 1.00 | 0.21 | [0.67, 1.53] |
| $100,000-$149,1000 | 0.80 | 0.15 | [0.56, 1.16] |
| $50,000-$99,999 | 0.80 | 0.14 | [0.56, 1.14] |
| Harmful drinking (ref. = no) | 1.25* | 0.13 | [1.01, 1.54] |
| Illicit drugs (ref. = no) | 1.12 | 0.14 | [0.87, 1.43] |
| Currently smoking (ref. = no) | 1.14 | 0.16 | [0.86, 1.50] |
| Past 12-month depression (ref. = no) | 1.58* | 0.30 | [1.09, 2.31] |
| Past 12-month anxiety (ref. = no) | 0.91 | 0.20 | [0.59, 1.40] |
| Financial stress (ref. = no) | 1.97*** | 0.27 | [1.50, 2.58] |
| Number of gambling activities | 1.32*** | 0.05 | [1.23, 1.42] |
| Overall gambling frequency | 1.72*** | 0.05 | [1.61, 1.82] |
| Constant | 0.04*** | 0.01 | [0.03, 0.08] |
Notes: N = 2,864; aOR = adjusted odds ratio; CI = confidence interval; *p < .05, **p < .01, ***p < .001. Model tested for multicollinearity with mean Variance Inflation Factor (VIF) of 1.77 and maximum 3.11, indicating a low correlation among predictors.
Source: TTM data, Wave 3, adult cohort, unweighted
2 Derived from original frequency variables (Box 1.2).
3 TTM participants at Wave 3 were aged 18-63 but the upper age limit for those who gambled was 62. Therefore, an age range of 18-62 is used when estimates are presented for only the gambling subpopulation, rather than the entire Wave 3 sample.
4 Confidence intervals for the estimates reported in Table 1.3 can be found in Supplementary Materials Table S1.2.
Summary
This is the first national study of Australian men to examine gambling behaviour and associated harms. Using data from Wave 3 of TTM, this report chapter examined the prevalence and frequency of gambling participation, the socio-demographic characteristics of men who gamble, risks of experiencing gambling problems, and financial stress experienced by adult men in Australia in 2020/21. It also compared the prevalence of alcohol and other drug use and mental ill-health experienced by men classified as ARPG and those gambling at non-problem levels in 2020/21, for the period 2013/14-2020/21.
Findings suggest that, in 2020/21, an estimated 2,751,934 adult Australian males aged 18-62 had gambled in the past 12 months, most commonly on horse racing, poker machines and sports betting. In 2020/21, 27% of men who gambled were classified as being at-risk of problem gambling in the past year, of which almost one-quarter (26%) also experienced some form of financial stress during that time. Significant predictors of ARPG in the past year included not having a partner, more frequent gambling and gambling on a higher number of activities, drinking alcohol at harmful levels, experience of depression and financial stress.
The findings of this research support the existing literature on the co-occurrence of gambling and other risky behaviours (Barnes et al., 2015; Loo et al., 2019). For example, Díaz and Pérez (2021) observed that people who drank alcohol and/or smoked tobacco were more likely to gamble and to spend greater amounts of money on gambling activities. In another recent study of Swedish adults who gambled, participants classified as engaging in problem gambling were significantly more likely to 'smoke or take snuff daily' and to have used an illegal or prescribed drug for non-medical purposes in the past year (Ford & Hakansson, 2020).
The literature also suggests two-way associations between exposure to alcohol and other drug consumption and mental ill-health during childhood or adolescence and gambling problems in later years. In a multi-wave Australian cohort study, binge drinking and tobacco use in young adulthood were found to predict adult gambling (Merkouris et al., 2021). Similarly, a 2017 systemic review and meta-analysis of longitudinal studies examined early risk and protective factors for problem gambling in adulthood and found that problem gambling was associated with alcohol use frequency, tobacco and illicit drug use and depressive symptoms encountered in childhood though to young adulthood (Dowling et al., 2017). Related research found that 'at-risk' or 'problem' gambling in early adulthood predicted poor mental health and the onset of substance use disorders in later years (Afifi et al., 2016).
Our findings of an association between at-risk or problem gambling and financial stress are also supported by the relevant literature. For example, in an observational study of financial records of 6.5 million individuals spanning over seven years, Muggleton and colleagues (2021) found that gambling was not only related to higher financial distress but also predicted future unemployment and decay of quality of life.
It is worth noting that TTM Wave 3 data collection (July 2020-January 2021) partially coincided with COVID-19 pandemic restrictions in Australia when some land-based (e.g. 'pokies') gambling venues were closed and major sporting/racing events were postponed or cancelled. Our findings of past-year prevalence for horse racing (56%) and sports betting (46%) among adult men in 2020/21 were comparable to what was found for the pre-pandemic period (57% and 46%, respectively) in another Australian study conducted during June-July 2020 of adults who gambled in the past year (Jenkinson et al., 2020). However, the prevalence of gambling on poker machines in the current study (54%) is higher than that observed in the other Australian study (35%). This difference could be explained by the different sampling strategies or time frames examined in the two studies.
Findings from the current study of Australian men support a range of policy and practical initiatives, including the need to develop and implement holistic prevention and treatment frameworks to address co-occurring gambling, drinking and mental ill-health, rather than treating these behaviours and outcomes in isolation. Other strategies recommended to help minimise gambling-related health, social and economic harms to affected individuals and communities include measures such as limiting the availability of gambling marketing and promotions (especially related to sports and race betting), reducing the number of poker machines in venues and restricting operating hours, implementing online and land-based gambling pre-commitment systems and effective self-exclusion programs, and developing a National Gambling Strategy (similar to Australia's National Alcohol Strategy) (e.g. Jenkinson et al., 2020).
The gambling module in the Wave 3 TTM Survey provided a unique opportunity to examine gambling participation and related harm among Australian men. The findings presented in this report will help to inform future research and policy development, and future waves of TTM will provide opportunities to explore changes in gambling behaviours and related harm over time.
References
- Gambling Regulation Act 2003 (Vic.) Retrieved from www.legislation.vic.gov.au
- Afifi, T. O., Nicholson, R., Martins, S. S., & Sareen, J. (2016). A longitudinal study of the temporal relation between problem gambling and mental and substance use disorders among young adults. The Canadian Journal of Psychiatry, 61(2), 102-111.
- Australian Institute of Health and Welfare (AIHW). (2021). Gambling in Australia. Australia's welfare 2021 Research Snapshot. Prepared by the Australian Gambling Research Centre, Australian Institute of Family Studies.
- Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., & Monteiro, M. G. (2001). The Alcohol Use Disorders Identification Test (AUDIT): Guidelines for use in primary care. Department of Mental Health and Substance Dependence, World Health Organization. Retrieved from www.who.int/substance_abuse/publications/audit/en/
- Bandara, D., Howell, L., Silbert, M., & Daraganova, G. (2021). Ten to Men: The Australian Longitudinal Study on Male Health - Data User Guide, Version 4.0, September 2021. Melbourne: Australian Institute of Family Studies. Retrieved from tentomen.org.au/data-access-and-usage/data-documentation/data-user-guide
- Barnard, M., Kerr, J., Kinsella, R., Orford, J., Reith, G., & Wardle, H. (2014) Exploring the relationship between gambling, debt and financial management in Britain. International Gambling Studies, 14(1), 82-95, doi:10.1080/14459795.2013.842606
- Barnes, G. M., Welte, J. W., Tidwell, M. C., & Hoffman, J. H. (2015). Gambling and substance use: Co-occurrence among adults in a recent general population study in the United States. International Gambling Studies, 15(1), 55-71.
- doi.org/10.1080/14459795.2014.990396
- Browne, M., Greer, N., Armstrong, T., Doran, C., Kinchin, I., Langham, E. et al. (2017). The social cost of gambling to Victoria. Melbourne: Victorian Responsible Gambling Foundation.
- Browne, M., Hing, N., Rockloff, M., Russell, A. M. T., Greer, N., Nicoll, F. et al. (2019). A multivariate evaluation of 25 proximal and distal risk-factors for gambling-related harm. Journal of Clinical Medicine, 8(4). doi:10.3390/jcm8040509
- Díaz, A., & Pérez, L. (2021). Gambling and substance use: A cross-consumption analysis of tobacco smoking, alcohol drinking and gambling. Substance Abuse, 1-6. doi:10.1080/08897077.2021.1903657
- Dowling, N. A., Aarsman, S. R., & Merkouris, S. S. (2021). Risk, compensatory, and protective factors in problem gambling: The role of positive mental health characteristics. Addictive Behaviors, 112, 106604-106604. doi:10.1016/j.addbeh.2020.106604
- Dowling, N. A., Cowlishaw, S., Jackson, A. C., Merkouris, S. S., Francis, K. L., & Christensen, D. R. (2015). Prevalence of psychiatric co-morbidity in treatment-seeking problem gamblers: A systematic review and meta-analysis. Australian & New Zealand Journal of Psychiatry, 49(6), 519-539. doi:10.1177/0004867415575774
- Dowling, N. A., Merkouris, S. S., Greenwood, C. J., Oldenhof, E., Toumbourou, J. W., & Youssef, G. J. (2017). Early risk and protective factors for problem gambling: A systematic review and meta-analysis of longitudinal studies. Clinical Psychology Review, 51, 109-124. doi:10.1016/j.cpr.2016.10.008
- Ferris, J., & Wynne, H. (2001). The Canadian Problem Gambling Index: Final Report. Canadian Centre on Substance Abuse.
- Ford, M., & Hakansson, A. (2020). Problem gambling, associations with comorbid health conditions, substance use, and behavioural addictions: Opportunities for pathways to treatment. PLoS ONE, 15(1). doi:10.1371/journal.pone.0227644
- Hing, N., Russell, A. M., & Browne, M. (2017). Risk factors for gambling problems on online electronic gaming machines, race betting and sports betting. Fronters in Psychology, 8(779). doi: 10.3389/fpsyg.2017.00779
- Hing, N., Russell, A. M. T., Vitartas, P., & Lamont, M. (2015). Demographic, behavioural and normative risk factors for gambling problems amongst sports bettors. Journal of Gambling Studies, 32(2), 625-641. doi: 10.1007/s10899-015-9571-9
- International Wellbeing Group (2013). Personal Wellbeing Index: 5th Edition. Melbourne: Australian Centre on Quality of Life, Deakin University.
- Jenkinson, R., Sakata, K., Khokhar, T., Tajin, R., & Jatkar, U. (2020). Gambling in Australia during COVID19. Australian Gambling Research Centre, Australian Institute of Family Studies. Retrieved from aifs.gov.au/agrc/sites/default/files/publication-documents/2009_gambling_in_australia_during_covid-19.pdf
- Jenkinson, R., de Lacy-Vawdon, C., & Carroll, M. (2018). Weighing Up the Odds: Young men, sports and betting. Melbourne, Australia: Victorian Responsible Gambling Foundation. Retrieved from responsiblegambling.vic.gov.au/resources/publications/weighing-up-the-odds-young-men-sports-and-betting-394/
- Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001) The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606-613.
- Loo, J., Kraus, S. W., & Potenza, M. N. (2019). A systematic review of gambling-related findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Journal of Behavioral Addictions, 8(4), 625-648.
- doi.org/10.1556/2006.8.2019.64
- Mathews, M. & Volberg, R. (2013). Impact of problem gambling on financial, emotional and social well-being of Singaporean families, International Gambling Studies, 13(1), 127-140. doi: 10.1080/14459795.2012.731422
- Merkouris, S. S., Greenwood, C. J., Youssef, G. J., Letcher, P., Vassallo, S., Dowling, N. A. et al. (2021). Adult gambling problems and histories of mental health and substance use: Findings from a prospective multi-wave Australian cohort study. Journal of Clinical Medicine, 10(7), 1406. doi:10.3390/jcm10071406
- Muggleton, N., Parpart, P., Newall, P., Leake, D., Gathergood, J., & Stewart, N. (2021). The association between gambling and financial, social and health outcomes in big financial data. Nature Human Behaviour, 5, 319-326. doi.org/10.1038/s41562-020-01045-w
- Murray Boyle, C., Joshi, A., & Jenkinson, R. (2021). Understanding gambling harm and ways to identify those at risk. Melbourne: Child Family Community Australia, Australian Institute of Family Studies.
- Queensland Government Statistician's Office, Queensland Treasury. (2021). Australian gambling statistics, 36th edition, 1993-94 to 2018-19. Brisbane: Queensland Treasury.
- Quinn, B., Swami, N., Terhaag, S., & Daraganova, G. (2020). Alcohol use among Australian Males. In G. Daraganova & B. Quinn (Eds.), Insights #1: Findings from Ten to Men - The Australian Longitudinal Study on Male Health 2013-16. Melbourne: Australian Institute of Family Studies.
- Rodriguez-Monguio, R., Errea, M., & Volberg, R. (2017). Comorbid pathological gambling, mental health, and substance use disorders: Health-care services provision by clinician specialty. Journal of Behavioral Addictions, 6(3), 406-415.
- Spitzer, R. L., Kroenke, K., Williams, J. B., & Lowe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of Internal Medicine, 166(10), 1092-1097.
- Swami, N., Prattley, J., Bandara, D., Howell, L., Silbert, M., Renda., J. et al. (2022). Ten to Men: The Australian Longitudinal Study on Male Health: Waves 1-3. The Australian Economic Review, 55(1), 155-165.
The authors of this Insights #2 report chapter are extremely grateful to the many individuals and organisations who contributed to its development, and who continue to support and assist in all aspects of the Ten to Men study. The Department of Health and Aged Care commissioned and continues to fund Ten to Men. The study’s Scientific Advisory and Community Reference Groups provide indispensable guidance and expert input. The University of Melbourne coordinated Waves 1 and 2 of Ten to Men, and Roy Morgan collected the data at both these time points. The Social Research Centre collected Wave 3 data. A multitude of AIFS staff members collectively work towards the goal of producing high-quality publications of Ten to Men findings. We would also especially like to thank every Ten to Men participant who has devoted their time and energy to completing study surveys at each data collection wave
Featured image: © GettyImages/humonia
Tajin, R., Quinn, B., Wong, C., O’Donnell, K., Rowland, B., Prattley, J., & Jenkinson, R. (2022). Gambling participation and harm among Australian men. In B. Quinn, B. Rowland, & S. Martin (Eds.), Insights #2 report: Findings from Ten to Men – The Australian Longitudinal Study on Male Health 2013-21. Melbourne: Australian Institute of Family Studies.
4 November 2022