Mental health care needs and access among Australian men: A data linkage study
Ten to Men Insights #2 Report: Chapter 2
Overview
Men's mental health remains a significant public health concern and a priority issue for Australia. In 2020-21, 7.8% of Australian men were estimated to have depression or feelings of depression while slightly more (10.6%) had an anxiety-related condition (Australian Bureau of Statistics [ABS], 2022). For the whole population, mental ill-health is estimated to cost the Australian economy up to $70 billion annually, with costs of disability, self-harm, suicide and premature death due to mental ill-health estimated at another $151 billion per year (Productivity Commission, 2020).
While mental ill-health constitutes a substantial cost to the public health system (Doran & Kinchin, 2019), Australian men tend to have lower usage of health care in general compared to women, despite comparable health needs (Burgess et al., 2009; Mansfield, Addis, & Mahalik, 2003).
Understanding patterns of mental health care use among men in Australia is essential for addressing this gap, particularly in the context of ongoing mental health needs. This chapter addresses this issue in six different ways. First, using data collected across the first three waves (2013-21) of Ten to Men: The Australian Longitudinal Study on Male Health (TTM), it outlines Australian men's self-reported experience and trajectories of depressive symptoms, as measured by the Patient Health Questionnaire-9 (PHQ-9). Second, this chapter examines the different types of mental health services and mental health prescriptions accessed by Australian men through linked Medicare Benefits Schedule (MBS) and Pharmaceutical Benefits Scheme (PBS) data. Third, patterns of health care usage over time, and typical monetary costs paid by men for health care, are presented. Fourth, differences in several priority population groups identified in the National Men's Health Strategy 2020-20301 are highlighted. Fifth, factors associated with the non-use of mental health care among men are presented. Finally, the chapter examines patterns of mental health service usage during COVID-19-related restrictions in 2020.
Several features of TTM are leveraged for the analyses in this chapter. The study's longitudinal nature affords examination of how men's experience of depressive symptoms change over time; repeated data collections measuring men's mental health are rare in Australia, and seldom consider other relevant information on health behaviours/attitudes. Linking TTM participants' self-report survey responses with Medicare information is also an important aspect of this chapter. Analyses use the detailed records of health care services and pharmaceuticals that are at least partly funded by the federal government under the MBS or PBS. Information on the use of such services is typically difficult to collect comprehensively, objectively and accurately in retrospective surveys, particularly when using self-report data. The linked data used in this research span nearly nine years over 2012-21, providing information between waves that is otherwise not covered by TTM survey tools. Note these data exclude mental health care services not funded under the MBS or PBS, which may include those provided by private practitioners with no Medicare rebate, publicly-funded mental health services at the state/territory level, and community-based mental health options funded through primary health care networks.2
The COVID-19 pandemic changed health care needs and access for many Australians. In addition to health risks associated with COVID-19 infection, public health responses involving stay-at-home 'lockdown' restrictions also affected Australians' social support and access to professional services, which led to concerns over mental health during this period (Holmes et al., 2020; Hossain et al., 2020). In response to restrictions to health care access, various services - including mental health options - were made available to the general public via telehealth.3 Investigating changes in mental health and the use of health care during and following this period is important for determining uptake of non-traditional service options, and for informing appropriate future responses to public health crises.
1 The National Men's Health Strategy 2020-2030 can be found at: www.health.gov.au/resources/publications/national-mens-health-strategy-2020-2030
2 Further information on the types of services covered under the MBS and PBS is available here: www.servicesaustralia.gov.au/about-medicare?context=60092
3 Telehealth services for mental health had been available before the COVID-19 pandemic for residents in remote areas (i.e. where in-person health care is very difficult to provide).
Key messages
-
Around three in 10 Australian men accessed a mental health service at least partly funded by the Medicare Benefits Schedule (MBS) at some point between 2012 and 2021. Almost one in three were prescribed mental health medications at least partly funded by the Pharmaceutical Benefits Scheme (PBS) during the same period.
-
The most commonly used MBS-funded mental health service was a mental-health-specific general practitioner (GP) consultation; antidepressants were the most commonly prescribed PBS-funded pharmaceutical for mental health. Use of both these forms of mental health care became more common over time among Australian men.
-
The proportion of visits to services that involved no out-of-pocket expenses included 84% of visits to GPs for mental health reasons, 30% of visits to psychiatrists and 50% of visits to psychologists.
-
Men's use of MBS- or PBS-funded mental health care differed by socio-economic factors; usage tended to be higher among men who were older, less educated, unemployed or who identified as Aboriginal and/or Torres Strait Islander. These usage differences were more pronounced in mental health prescriptions compared to mental health services.
-
Conformity to traditional masculine norms was associated with reduced use of mental health care services among those in need (i.e. those with greater depressive symptoms).
-
Rates of mental health service use between March 2020-February 2021, during the COVID-19 pandemic, were similar to pre-COVID levels (January 2018-February 2020); however, 18% of services during COVID-19 were delivered through expanded telehealth measures.
Research objectives
This chapter used data from the first three waves of Ten to Men (TTM) across 2013-21 to:
- investigate the prevalence and changes in self-reported depressive symptoms among Australian men between 2013 and 2021
- identify the frequency of, and financial costs associated with, MBS service use and PBS medication usage for mental health among Australian males
- describe changes in the prevalence of MBS- and PBS-funded mental health care usage and out-of-pocket expenses over 2013-20
- investigate levels of MBS service use and PBS prescription access for mental health among Australian males by demographics of interest and experience of depressive symptoms
- examine the characteristics of men reporting greater depressive symptoms who did not access relevant MBS services or PBS medications
- describe MBS and PBS usage patterns relating to mental health among Australian men following the commencement of the COVID-19 pandemic and implementation of related restrictions nationwide.
Method
This section describes the key measures and data analysis techniques used to address the above objectives. Bandara, Howell, Silbert, and Daraganova (2021) and Swami et al. (2022) provide more information regarding the overall methodology of the TTM study.
Measures
Mental health (depression): PHQ-9
Included at each of the first three waves of TTM data collection, the PHQ-9 (Kroenke, Spitzer, & Williams, 2001) was used to measure self-reported experiences of depressive symptoms among participants in the two weeks preceding the survey. Total scores for the PHQ-9 range from 0 to 27, with higher scores indicating greater levels of depressive symptoms. Scores can be assigned to five categories of depression severity: None or minimal (0-4), mild (5-9), moderate (10-14), moderately severe (15-19), and severe (20-27).
MBS and PBS data linkage
For TTM participants who provided consent (N = 8,887, 64% of the adult sample in 2013/14), their self-report survey responses were linked to Medicare data spanning from 2 March 2012 to 15 February 2021 (Bandara, Howell, & Daraganova, 2021). Medicare data indicate participants' receipt of health care services through the MBS and dispensed (filled) medical prescriptions through the PBS.
With around 90% of the Australian population accessing an MBS service in 2014-15 and the PBS subsidising approximately 75% of prescribed medicines (Australian Institute of Health and Welfare [AIHW], 2016; Mellish et al., 2015), the linked data can be used to achieve a detailed picture of participants' use of services and pharmaceuticals funded under the MBS and PBS between 2012 and 2021.
It is important to note, however, that health care services not funded under the MBS or PBS may include unfilled and private prescriptions, over-the-counter medications and prescriptions filled for public or private hospital in-patients, in addition to services for patients in public hospitals and other publicly funded mental health services at the state/territory level, services provided by private practitioners with no Medicare rebate and community-based health services funded through primary health care networks (AIHW, 2018; Mellish et al., 2015; van Gool, Parkinson, & Kenny, 2015). Therefore, any findings presented in this chapter likely do not fully capture mental health care use by the TTM sample.
The linked Medicare data contain information on treatments for many different types of health conditions. Classification of those relevant to mental health are in line with definitions of mental health services by the AIHW (2022). Mental health services are classified by their MBS item numbers across five categories: psychiatrists, general practitioners (GPs, specifically for mental health reasons), clinical psychologists, psychologists not excluding clinical psychologists,4 and other allied health providers. Mental health prescriptions are identified by their Anatomical Therapeutic Chemical (ATC) codes and may correspond to five categories: antipsychotics (N05A), anxiolytics (N05B), hypnotics and sedatives (N05C), antidepressants (N06A), and psychostimulants (N06B).
In rare cases (n = 103 TTM participants), consent was provided but the individual had no recorded health care through the MBS/PBS; these individuals were counted in the linked data sample as not having accessed mental (or any) healthcare between 2012 and 2021. This is distinguished from even rarer instances (n = 2 TTM participants) where consent was provided but data linkage was unsuccessful. Since the Medicare data were successfully extracted for all but two of 8,889 men who provided consent, there is minimal susceptibility to statistical bias from linkage error (Doidge & Harron, 2019).
Socio-economic, demographic and other factors
This chapter uses several socio-economic, demographic and other factors measured through the TTM survey to give context to the health care needs and usage among Australian men. Their age, educational attainment, employment status, marital/partnered status, area of residence (distinguishing major cities from regional/remote areas) and financial hardships are accounted for. Financial hardships are measured through an index counting whether the individual asked for financial help from friends or family, and how many of the following could not be paid for due to a shortage of money: (a) a prescription, (b) medical care, (c) bills, (d) mortgage/rent.
The Conformity to Masculine Norms Inventory (CMNI) was included in analysis to account for attitudes and adherence to traditional masculine norms, given that greater adherence to traditional masculine norms has been associated with poorer health literacy (Milner, Shields, & King, 2019) and health behaviours (Mahalik, Levi-Minzi, & Walker, 2007). The CMNI comprises 22 items and total scores range from 0-22, with higher scores indicating greater conformity to masculine norms (Mahalik et al., 2003).
Additionally, the chapter uses information about Aboriginal and Torres Strait Islander identity, culturally and linguistically diverse backgrounds (CALD), and whether the individual has a functional difficulty or disability. Functional difficulty or disability was measured through the Washington Group Short Set (WGSS) across six core functional domains: vision, mobility, hearing, cognition, self-care and communication.5
Analysis
Addressing the first research objective, survey data from Waves 1-3 were used to tabulate depressive symptoms and examine transition rates between PHQ-9 categories over time. All remaining research objectives used both survey data and linked Medicare data in conjunction, to show the prevalence and costs of health care items over time and by survey characteristics. The analyses throughout this chapter are unweighted.
Linear regression models were estimated to address the fifth research objective: to identify the factors and characteristics of men associated with non-use of mental health care. Models were disaggregated by PHQ-9 category (No to minimal/mild vs moderate/moderately severe/severe) to highlight cases where men may have needed mental health care but did not receive it. These models included the set of control variables outlined above, and standard errors were clustered at the individual level as most men had repeated observations. Interpreted as a linear probability model, the estimated constant indicates the probability of non-use of mental health care for the reference category, while estimated coefficients modify this probability with all other factors left unchanged.
4 Some MBS items are exclusive to clinical psychologists and are classified as such. Other items are provided by psychologists in general and typically attract a lower fee, which may include clinical psychologists (but not in an exclusive manner). Clinical psychologists may therefore provide services across both categories; these records are not double-counted. Since clinical psychology items typically attract higher MBS fees, there is little financial incentive for clinical psychologists to provide general psychology MBS items.
5 More information on the WGSS can be found at www.washingtongroup-disability.com/question-sets/wg-short-set-on-functioning-wg-ss
Findings
Prevalence and changes in experience of depressive symptoms between 2013 and 2021
Table 2.1 shows the proportions of TTM participants in each PHQ-9 category across the first three waves of data collection in 2013/14, 2015/16 and 2020/21 (Waves 1-3, respectively). Wave 3 data collection was undertaken during the COVID-19 pandemic. These data suggest that, while most (64%) Australian men in the sample had no or minimal depressive symptoms, around 36% experienced mild to severe depressive symptoms.

These proportions remained quite similar over time, which suggests that the distribution of PHQ scores collected at the time of the COVID-19 pandemic was similar to previous years. Analysis of health service usage before and during COVID-19 is presented later in the chapter.
| PHQ-9 category | 2013/14 (Wave 1) % [95% CI] | 2015/16 (Wave 2) % [95% CI] | 2020/21 (Wave 3) % [95% CI] | Overall % [95% CI] |
|---|---|---|---|---|
| No or minimal | 62.9 [61.9, 64.0] | 65.1 [64.0, 66.2] | 65.5 [64.2, 66.8] | 64.3 [63.6, 65.0] |
| Mild | 23.7 [22.7, 24.6] | 23.0 [22.0, 24.6] | 22.3 [21.2, 23.5] | 23.1 [22.5, 23.7] |
| Moderate | 8.3 [7.7, 8.9] | 7.3 [6.7, 7.9] | 7.4 [6.7, 8.1] | 7.7 [7.4, 8.1] |
| Moderately severe | 3.1 [2.8, 3.5] | 3.1 [2.7, 3.5] | 3.2 [2.7, 3.5] | 3.1 [2.9, 3.4] |
| Severe | 1.9 [1.6, 2.2] | 1.6 [1.3, 1.9] | 1.6 [1.3, 2.0] | 1.7 [1.5, 1.9] |
| Observations | 8,680 | 6,974 | 5,011 | 20,665 |
Notes: Data presented here relate only to participants with linked Medicare data from Wave 1. 95% CI = 95% confidence interval; PHQ-9 = Patient Health Questionnaire
Source: TTM data, Waves 1, 2 and 3, adult cohort, unweighted
To help understand how the prevalence of depressive symptoms among men changed over time, Table 2.2 displays the proportions of TTM participants in each category across 2013/14 and 2015/16. Specifically, it shows the proportions of men who moved from one depression category to another over this two-year period. Likewise, Table 2.3 shows the equivalent transition rates between categories over the approximate five-year period between 2015/16 and 2020/21. To assist with interpretation of the transition matrices in Table 2.2 and Table 2.3, cells are colour-coded. Green, yellow and red correspond to improvements, no change and deteriorations in experiences of depression symptoms, respectively, as classified using PHQ categories (see notes below each table).
For most men, reports of low burden of depressive symptoms remained stable over time. Indeed, 83% of men in 2013/14 who were categorised as having no or minimal depression severity remained in this category in 2015/16. Similarly, 81% of men in 2015/16 with no or minimal depression severity remained in this category in 2020/21.
By comparison, fewer than half of men in the mild to severe depressive symptoms categories remained in the same category when surveyed at the following wave (indicated by the yellow diagonal cells in Tables 2.2 and 2.3).
The proportions of men experiencing mild to severe depressive symptoms, who then reported lower levels of symptoms when later surveyed (i.e. an improvement in mental health across waves; indicated by the green cells) are also shown in Table 2.2 and Table 2.3. Between 10% and 42% of men reported improvement in symptoms between Waves 1 and 2 and Waves 2 and 3.
In contrast, a decline in depressive symptoms across waves (indicated by the red cells in both tables) saw percentages that ranged between 0.3% and 14%.
The proportion of men who reported severe depressive symptoms at one wave and subsequently reported severe depressive symptoms in the following survey wave ranged between 32% and 34%.
To compare depressive symptoms over a longer period of time, Table S2.1 in the Supplementary Materials shows changes between 2013/14 and 2020/21. Transition rates to other PHQ-9 categories tend to be slightly higher, in line with the longer time frame, where men may have experienced improvements or deteriorations in depressive symptoms. The overall pattern of transition rates remains similar to Table 2.2 and Table 2.3, however, again indicating that men in the sample were more likely to report reduced depressive symptoms over time (or remain in the lowest symptoms category).
Data across the three survey waves in 2013/14, 2015/16 and 2020/21 indicate that enduring depressive symptoms are rare. Among men who responded at all three waves, under 2% reported moderately severe or severe depressive symptoms every time they were surveyed. This corresponds to a population estimate of around 52,000 Australian men reporting moderately severe or severe symptoms in 2013/14, 2015/16 and 2020/21. In contrast, nearly 50% of men in the sample had reported no to minimal depressive symptoms at every survey, showing that a lower burden of depression tends to persist over time while greater depressive symptoms are less likely to endure over a longer period.
| 2013/14 (W1) | 2015/16 (Wave 2) | ||||
|---|---|---|---|---|---|
| No or minimal | Mild | Moderate | Moderately severe | Severe | |
| No or minimal | 82.9 | 13.7 | 2.3 | 0.9 | 0.3 |
| Mild | 41.9 | 43.8 | 10.8 | 2.6 | 0.8 |
| Moderate | 22.8 | 35.1 | 26.0 | 10.4 | 5.7 |
| Moderately severe | 6.5 | 26.6 | 33.2 | 24.6 | 9.0 |
| Severe | 10.4 | 20.0 | 15.7 | 21.7 | 32.2 |
Notes: Data presented here relate only to participants with linked Medicare data at Waves 1 and 2. A transition matrix containing percentages of men (N = 6,844) in each PHQ-9 category in 2013/14 (rows, N = 4,396, 1,604, 530, 199, 115 respectively across no to minimal, mild, moderate, moderately severe and severe categories) that transitioned to PHQ-9 categories in 2015/16 (columns). Green cells indicate reduced depressive symptoms over time; yellow cells indicate remaining in the same category over time; red cells indicate heightened depressive symptoms over time.
Source: TTM data, Waves 1 and 2, adult cohort, unweighted
| 2015/16 (W2) | 2020/21 (Wave 3) | ||||
|---|---|---|---|---|---|
| No or minimal | Mild | Moderate | Moderately severe | Severe | |
| No or minimal | 81.2 | 15.2 | 2.5 | 0.8 | 0.3 |
| Mild | 44.3 | 36.8 | 14.2 | 4.0 | 0.7 |
| Moderate | 16.3 | 40.4 | 25.0 | 12.5 | 5.8 |
| Moderately severe | 13.3 | 26.6 | 25.8 | 21.1 | 13.3 |
| Severe | 10.4 | 20.9 | 10.4 | 23.9 | 34.3 |
Notes: Data presented here relate only to participants with linked Medicare data at Waves 2 and 3. A transition matrix containing percentages of men (N = 4,699) in each PHQ-9 category in 2015/16 (rows, N = 3,138, 1,054, 312,128, 67 respectively across no to minimal, mild, moderate, moderately severe, and severe categories) who transitioned to PHQ-9 categories in 2020/21 (columns). Green cells indicate reduced depressive symptoms; yellow cells indicate remaining in the same category; red cells indicate heightened depressive symptoms.
Source: TTM data, Waves 2 and 3, adult cohort, unweighted
Mental health service use and prescribed mental health medications among Australian males
Overall prevalence and costs of mental health care usage
Table 2.4 summarises MBS and PBS usage by TTM participants over 2012-21. It shows the aggregate number of records, prevalence of users among the TTM sample (i.e. ever accessed between 2012 and 2021) and details of costs by each mental health service and mental health medication category. Since health care services are subsidised at different levels, cost information includes both the proportion of service/prescription records that are fully subsidised, and therefore incur zero out-of-pocket costs, and the median non-zero costs for each category. Patterns over time for usage and cost data are presented in the following subsection. Findings from Table 2.4 indicate that 31% of men in the sample accessed mental health services and 33% accessed mental health prescriptions at some point at least once over the nearly nine-year period.
| Records (n) | Unique Users (n) | Prevalence (%) | Propn. Zero Cost (%) | Item median non-zero Cost ($) | |
|---|---|---|---|---|---|
| Mental health services (MBS) | |||||
| Psychiatrists | 7,974 | 517 | 5.8 | 29.7 | 51.95 |
| General practitioners (mental health-specific) | 11,009 | 2,573 | 29.0 | 83.8 | 33.95 |
| Clinical psychologists | 5,971 | 762 | 8.6 | 39.8 | 55.50 |
| Psychologists including clinical psychologists | 7,909 | 1,111 | 12.5 | 49.9 | 60.20 |
| Other allied health providers | 1,063 | 165 | 1.9 | 67.7 | 45.20 |
| Total: Any mental health service | 33,926 | 2,707 | 30.5 | 54.9 | 54.75 |
| Mental health prescriptions (PBS) | |||||
| N05A Antipsychotics | 12,161 | 335 | 3.8 | 8.9 | 6.30 |
| N05B Anxiolytics | 7,727 | 1,011 | 11.4 | 18.7 | 6.40 |
| N05C Hypnotics and sedatives | 2,786 | 789 | 8.9 | 10.2 | 7.56 |
| N06A Antidepressants | 71,529 | 2,219 | 25.0 | 5.3 | 13.36 |
| N06B Psychostimulants | 2,346 | 105 | 1.2 | 4.3 | 17.10 |
| Total: Any mental health prescription | 96,549 | 2,954 | 33.2 | 6.9 | 12.56 |
Notes: MBS = Medicare Benefits Schedule; PBS = Pharmaceutical Benefits Scheme. For each category of mental health service and prescription, displayed are the number of records in the linked Medicare data between March 2012 and February 2021, the number of unique TTM individuals who accessed these health care items, the proportion of the sample with linked Medicare data who accessed these health care items, the proportion of records that involved zero out-of-pocket costs to the user, and the median value of non-zero out-of-pocket costs. Classifications of mental health services and prescriptions follow AIHW (2022). Some MBS items are exclusive to clinical psychologists; however, clinical psychologists may also provide services listed on the MBS that correspond to psychologists more generally. Clinical psychologists may therefore provide services across both categories; these records are not double counted.
Source: TTM, Wave 1, adult cohort, linked Medicare data from MBS (top) and PBS (bottom); Classifications of mental health services and prescriptions from AIHW (2022)
Mental health service usage and cost from MBS data between 2012 and 2021
Service use
As detailed in Table 2.4, around three in 10 men in the TTM sample (31%) accessed any MBS mental health service at some point between March 2012 and February 2021. Visits to a GP specifically for mental health reasons was the most prevalent mental health service type; 29% of men in the sample - nearly all the men who had accessed any mental health service - had consulted a GP at least once during this nine-year period.
Among specialist services, visits to psychologists and clinical psychologists were also somewhat common (taken up by 13% and 9% of the sample, respectively). By contrast, visits to psychiatrists (6%) and other allied health providers (2%, usually a social worker) were relatively uncommon. Despite the lower prevalence of these specialist services in terms of unique (individual) users, the men who accessed such help tended to do so repeatedly.
For example, psychologist and psychiatrist services constituted 23% and 24% of all mental health service records over the nine-year period, despite being used by comparatively fewer individuals. The high number of records is likely reflective of the nature of mental health service treatment, which can often involve repeated contact and support by the health professional (Bruijniks et al., 2015).
Out-of-pocket expenses
Table 2.4 also shows the proportion of health services provided without out-of-pocket expense to the individual. Notably, a very high rate (84%) of GP mental health visits incurred no fees. Other mental health services were also provided without incurring out-of-pocket expenses at high rates - overall, more than half of all mental health services were supplied at no out-of-pocket cost to the individual. In addition to the use of bulk-billed services,6 many health visits could also have been covered by the Better Access initiative,7 which subsidised up to 10 mental health services per calendar year from most of 2012-19, and was expanded to up to 20 services in 2020 in response to COVID-19.
The median costs in Table 2.4 are a measure of typical expenses in cases when services required any out-of-pocket expenditure. The highest median costs in these cases were visits to psychologists and psychiatrists, which often involved payments over $50. Since men may access these health services repeatedly, typical annual costs are described in the next section.
PBS data: Mental health prescription usage and cost between 2012 and 2021
Linked Medicare data detailing mental health medications offered through the PBS and prescribed to TTM participants are also presented in Table 2.4.. Findings show that nearly one in three men (33%) filled a mental health prescription at some point over the nine-year period. Among these medications, antidepressants were the most commonly prescribed. Antidepressants constituted 74% of all mental health prescription records, and one-quarter (25%) of the TTM sample filled at least one such prescription between 2012 and 2021.
One disproportionately large category of mental health medication were antipsychotics; despite only being used by 4% of the sample, antipsychotic prescriptions constituted 13% of mental health PBS records.
The data provided in Table 2.4 further indicate that mental health prescriptions are often not provided with zero out-of-pocket expense; these medicines are below the $42.50 general patient co-payment (current in 2022), and the cost of PBS prescriptions for all patients is capped by the maximum co-payment amount.8 Instances where pharmaceuticals are provided with zero or reduced expense to the patient may be due to the PBS Safety Net, where medications are provided at reduced cost (free for holders of concession cards) once a household has already spent a threshold amount on PBS medications in a calendar year (in 2022 the PBS Safety Net thresholds were $326.40 for concession card holders and $1,542.10 for general patients). Psychostimulant prescriptions had the highest median cost of $17.10, followed by antidepressant prescriptions with a median cost of $13.36 (both of these pharmaceuticals are below the general co-payment threshold of $42.50; hence the cost is fully borne by the patient).
Changing prevalence and cost in mental health care between 2013-20
To aid in understanding whether usage of mental health care has changed over time, Figure 2.1 displays the proportions of the TTM sample who had accessed any mental health service or been prescribed any mental health medication within each calendar year 2013-20.9 It also presents trends for the five service types and five medications listed in Table 2.4. Individual and contextual factors associated with the use of any mental health service or prescription are explored in the next section of this chapter.
Figure 2.1: Usage rates by mental health care service and prescription, 2013-20
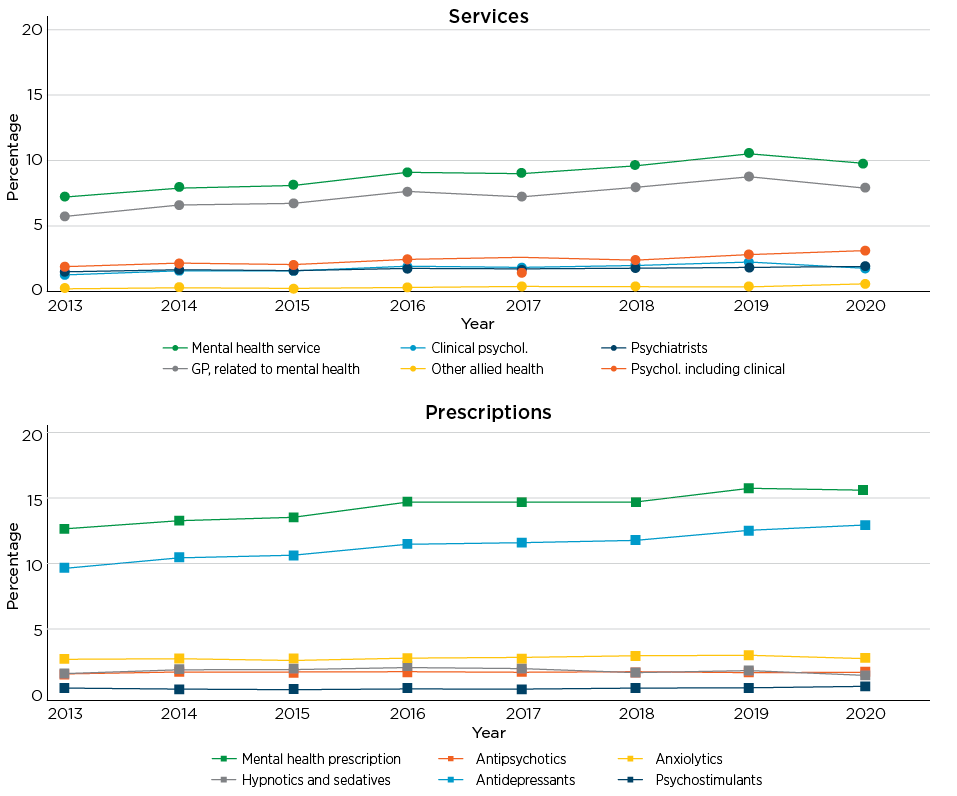
Notes: Displayed are percentages of the TTM sample that accessed a mental health service (top) or mental health prescription (bottom) in each calendar year (N = 8,887 for 2013-17; N = 8,784 for 2018-20 due to withdrawn linkage consent during 2017. These cases of withdrawn consent led to a conservative estimate only in 2017.)
Source: TTM, Wave 1, adult cohort, linked Medicare data from MBS (top) and PBS (bottom)
Figure 2.1 shows that the use of any mental health service by TTM participants increased over the observed period, from 7% of the sample in 2013 to 10% in 2020. Although there were some minor increases in visits to psychologists and psychiatrists, much of the overall increase was driven by visits to GPs for mental health reasons, which increased from 6% to 8% over the same period. Similarly, rates of accessing any mental health prescription increased from 13% to 16% of the sample between 2013 and 2020. This was largely driven by an increase in prevalence of antidepressant prescriptions from 10% to 13%, with other medications remaining stable and less commonly prescribed over the period.
As indicated in Table 2.4, mental health services and medications can involve different rates of repeated usage and out-of-pocket expenses. In Figure 2.2, the average annual out-of-pocket expenses are shown for users of each type of mental health treatment across the eight years.
Figure 2.2: Average annual out-of-pocket costs by mental health care service and prescription, 2013-20
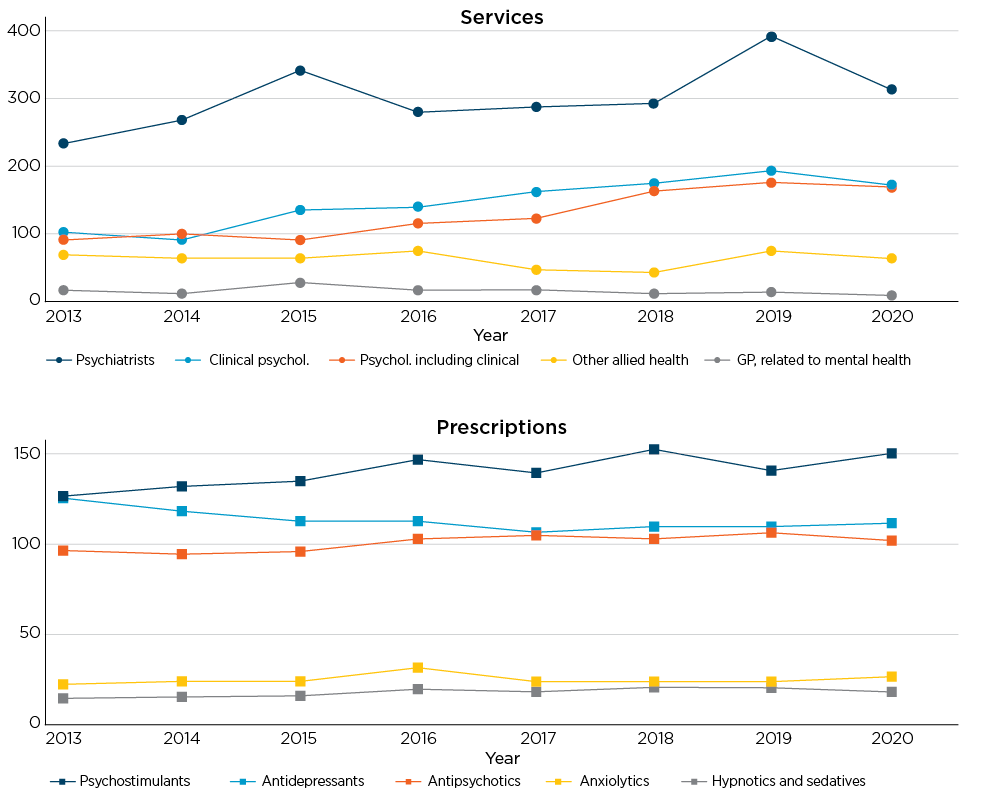
Notes: Displayed are average annual out-of-pocket costs among TTM participants who had used the corresponding mental health service (left) or mental health prescription (right).
Source: TTM, Wave 1, adult cohort, linked Medicare data from MBS (left) and PBS (right)
Among mental health services, visits to GPs for mental health reasons involved very low average annual expenditures, with little marked change over time. Total yearly out-of-pocket expenses among men who consulted their GP regarding mental health remained below $30 during 2013-20. This may again reflect the availability of bulk-billed services or subsidies through the Better Access initiative.
Out-of-pocket expenses for other allied health providers fluctuated over the same period, ranging from between $40 to $80 annually. However, average total annual expenditures rose substantially for men accessing services from psychologists and psychiatrists, increasing 73% from just over $90 in 2013 to $170 in 2020 for general psychologists, 88% from $100 in 2013 to $172 in 2020 for clinical psychologists, and 36% from $230 to over $300 for psychiatrists over the same period. Typical annual costs for men who visited psychiatrists were the highest, remaining over $200 between 2013 and 2020.
Average annual expenses for mental health medications remained steady in most cases. Patient contributions for antipsychotics, anxiolytics and hypnotics and sedatives changed little over time, with average annual expenses for antidepressants (as a major category of mental health prescription medication) decreasing by 12% from $125 in 2013 to $111 in 2020. In comparison, average annual costs for men prescribed psychostimulants increased by 20% from $126 in 2013 to $150 in 2020 (these were the most expensive medicines considered and are above the concessional co-payment threshold).
Factors associated with mental health care
Differences in mental health services and prescriptions
Bivariate associations were examined between mental health care usage and individual and contextual characteristics among adult participants (18-55 years) at Wave 1 of TTM (2013/14). Figure 2.3 shows the annual proportion within each group who accessed mental health services or prescriptions in 2014.
Figure 2.3: Annual mental health care usage rates by depression category (PHQ-9) and socio-demographic characteristics, 2014
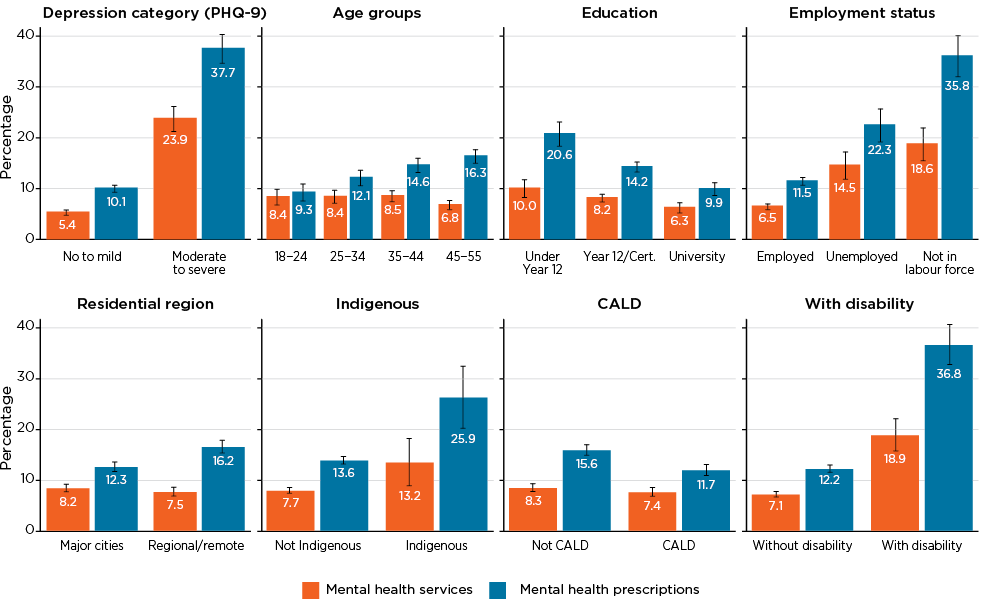
Notes: Figure displays the proportion of TTM adults with linked Medicare information that accessed mental health services or mental health prescriptions in 2014 along with 95% confidence intervals, by categories of PHQ-9, age, education, employment, residential region, Aboriginal and Torres Strait Islander identity, cultural and linguistically diverse (CALD) status, and having a functional difficulty/disability. N = 8,887
Source: TTM, Wave 1, adult cohort, linked Medicare data from MBS and PBS
Figure 2.3 shows that men who reported moderate to severe depressive symptoms were significantly more likely to access mental health services and prescriptions than men reporting no to mild symptoms. Over one in three men (38%) in the consolidated moderate, moderately severe and severe PHQ-9 categories had accessed mental health prescriptions, and over one in five (24%) had used a mental health service. Importantly, however, around three in four men with moderate or greater depressive symptoms did not access a mental health service in 2014, despite the indication that they may have needed it.
Likely reflecting reduced need, a much lower proportion of men with no to mild depressive symptoms accessed mental health services and prescriptions (5% and 10% respectively), showing that mental health needs track strongly with usage of mental health care.
Usage of mental health services tended to be similar across the age profile; on average, 7%-9% of males accessed an MBS-funded mental health service each year, regardless of age. However, usage of medications differed by age, with older men receiving mental health prescriptions at much higher rates than younger men. For example, 16% of 45-57 year olds accessed mental health medications compared to 9% of 18-24 year olds.
Differences in accessing mental health care were evident by socio-economic background - both in aspects that tend to remain constant and those that may be circumstantial or more dynamic. For example, mental health prescriptions were higher among men who had left high school before completing Year 12 compared to those with a university degree (21% vs 10%, respectively).
A very large gap was also observed in relation to labour market outcomes; employed men were less likely to access mental health prescriptions compared to those who were unemployed (12% vs 22%, respectively). Both of these groups were also less likely to access mental health services and prescriptions than men out of the labour force (36%). This trend was reflected in MBS records; an average of around 7% of employed men accessed mental health services on an annual basis, compared to 15% of unemployed men and 19% of men not in the labour force. This suggests that income may not be the primary barrier to accessing mental health care. As non-employed men use these services/prescriptions at higher rates, usage of health care items that are not subsidised may also use a larger proportion of their financial resources.
Rates of mental health service usage were similar for men living in major cities and regional areas (8%). However, more men in regional areas had been prescribed mental health medications (16% vs 12%, respectively) to a statistically significant extent.10 Although regional Australians tend to have poorer access to health professionals and services (Productivity Commission, 2020), this is not evident among this sample of men in 2014.
Differences by cultural background were substantial. Men who identified as Aboriginal and/or Torres Strait Islander were more likely to access mental health care services and prescriptions (at 13% and 26% respectively) than non-Indigenous men (8% and 14%). Similar rates of service usage were observed among culturally and linguistically diverse (CALD) and non-CALD men (7% vs 8%, respectively); however, CALD men tended to access mental health prescriptions at lower rates than their non-CALD counterparts (12% vs 16%).
Men who were classified as experiencing some functional difficulty and/or disability across any WGSS domain had much higher rates of accessing mental health services (19%) and prescriptions (37%) compared to men without difficulty/disability (7% and 12%, respectively).
Factors associated with non-use of mental health care
The model depicted in Figure 2.4 compares men's non-use of mental health care against those who used such services or prescriptions within two years of their interviews in 2013/14 and 2015/16 (Waves 1 and 2 of TTM).11 By orienting the model around non-use, the results highlight groups or factors associated with lower access to mental health services and prescriptions. The models are disaggregated by PHQ-9 categories (no to minimal and mild vs moderate, moderately severe, and severe) so that the results are adjusted for lower/higher depressive symptoms. Crucially, this helps identify socio-economic and other factors (see Table S2.2) associated with lower access of mental health care among men with greater mental health needs. For brevity, the following analysis refers to moderate, moderately severe, and severe depressive symptoms as 'greater depressive symptoms' in contrast to the no to minimal and mild PHQ-9 categories.
Figure 2.4 summarises the estimates from the model (full results are provided in the supplementary material in Table S2.3). For the reference case (18-24 years old, not completed Year 12, employed, without financial hardship, never married, resided in a major city, without functional difficulty/disability, and neither Indigenous nor CALD), the probability of not accessing mental health care within two years of being surveyed among men with no to mild depressive symptoms was 88%, compared to 66% among men reporting greater depressive symptoms. The estimated coefficients can be interpreted as modifiers to these probabilities, holding other factors constant. In Figure 2.4, factors to the left (negative) indicate a greater likelihood of having accessed mental health care during the two years following Wave 1 and 2 interviews, whereas factors to the right (positive) indicate a reduced likelihood of engaging with mental health care.
Figure 2.4: Factors associated with non-usage of mental health care two years following interviews in 2013/14 and 2015/16, by depression (PHQ-9) category (N = 8,887)

Notes: Plot of coefficient estimates (as percentages) and 95% confidence intervals from linear probability models on not accessing mental health care two years following interviews in 2013/14 and 2015/16, disaggregated by PHQ-9 category: No to minimal/Mild (N = 7,518 individuals, 12,683 obs.) and Moderate/Moderately severe/Severe (N = 1,411 individuals, 1,803 obs.). CALD = Culturally and linguistically diverse; CMNI = Conformity to Masculinity Norms Index. The CMNI measures extent of conformity to traditional masculine roles; total scores range from 0-66, with higher scores indicating greater conformity to masculine norms. Standard errors are clustered at the individual level. Significant negative values (i.e. to the left of the vertical line) indicate association with accessing mental health care within two years of interview; significant positive values (i.e. to the right of the vertical line) indicate associations with not accessing mental health care within two years of interview. 'Financial hardships' = index counting whether asked friend/family for financial help, and if couldn't pay for: (a) prescriptions, (b) medical care, (c) bills, (d) mortgage/rent.
In line with the descriptive, cross-sectional evidence in Figure 2.3 from 2014, rates of mental health care access differed by age, particularly among men reporting greater depressive symptoms. Among these men, those who were younger and aged 18-24 years were around 9 percentage points less likely than men aged 25-34 and 45 and over to access any mental health care two years after interview. Differences by education level were not statistically significant but positive point estimates suggest that more educated men with greater depressive symptoms could have a lower tendency to access mental health care.
Compared to employed men, the model results showed that unemployed men - and to a greater extent, men out of the labour force - were more likely to have accessed mental health care. These associations were large for men reporting greater depressive symptoms; unemployed men were 8 percentage points more likely to access mental health care within two years of the survey, and men who were out of the labour force were 21 percentage points more likely to access mental health care during this time. Financial hardships were associated with a 3-4 percentage point increase to the likelihood of accessing mental health care for men irrespective of mental health status.
Compared to men who had never married, those who were married or living in de facto partnerships were neither significantly more nor less likely to access mental health care. However, men who had divorced, separated or become widowers were more likely to have accessed mental health care within two years after being surveyed, although this was only statistically significant for men who reported no to mild depressive symptoms.
Men who lived in regional areas were neither statistically more nor less likely to access mental health care when compared to those who resided in major cities. The bivariate differences by area of residence displayed in Figure 2.3 may therefore reflect other demographic, socio-economic or individual differences between men from major cities and regional areas that are captured by the model rather than an inherent regional effect.
One factor found to be associated with non-usage of mental health care was conformity to masculinity norms, captured through the Conformity to Masculinity Norms Index (CMNI) score (higher scores indicate greater conformity to masculine norms). An increase in CMNI score by one standard deviation among men reporting greater depressive symptoms was associated with a 3.4 percentage point increase in the probability of not accessing mental health care within the following two years. A smaller but also statistically significant association of 1.2 percentage points was also estimated for men reporting no to mild depressive symptoms.
Men with self-reported disability were more likely to access mental health care within two years of each survey wave. This association was larger among men reporting greater depressive symptoms (12 percentage points) than men reporting no to mild symptoms (10 percentage points).
Estimates for Aboriginal and/or Torres Strait Islander identity suggests that Indigenous men were more likely to access mental health care than men who did not identify as Aboriginal and/or Torres Strait Islander. The point estimates were larger among men reporting greater depressive symptoms than men with no to mild symptoms (12 vs 6 percentage points, respectively).
Men from CALD backgrounds in the sample with no to mild depression were three percentage points less likely to access mental health care than non-CALD men. A similar coefficient was estimated for CALD men reporting greater depressive symptoms; however, this was not statistically significant.
Mental health care following the COVID-19 pandemic
As described at the start of this chapter, the TTM sample reported similar rates of depressive symptoms around mid-to-late 2020 (during Wave 3 of the data collection) when compared to earlier survey waves. This yields suggestive (but inconclusive) evidence that mental health needs in the first year following the COVID-19 pandemic were similar to mental health needs in 2013/14 and 2015/16.
However, the linked Medicare data for the TTM survey do show nuanced changes in health care following the COVID-19 pandemic. Figure 2.5 displays the monthly counts of mental health services (labelled along the left vertical axis) benchmarked against 'typical' GP consultations12 (i.e. consultations not designated as mental-health-specific; labelled along the right vertical axis) between January 2018 and January 2021. Fitted dashed lines delineate the trends in health care usage before the pandemic between January 2018 and January 2020, and during the first year of the pandemic between January 2020 and January 2021.
To aid interpretation, typical GP consultations are presented in Figure 2.5 as a comparison category. Typical GP consultations constitute the most common category of health care service in the linked MBS data, thus serving as a broad indicator of men's health care access and usage. Even when including COVID telehealth options, the number of typical GP consultations declined in April 2020 (soon after border closures and widespread lockdown restrictions were introduced in both Victoria and New South Wales in March) and remained at lower levels until the end of the observation period in early 2021.
Figure 2.5: Counts of mental health service utilisation and common GP consultations, January 2018-January 2021
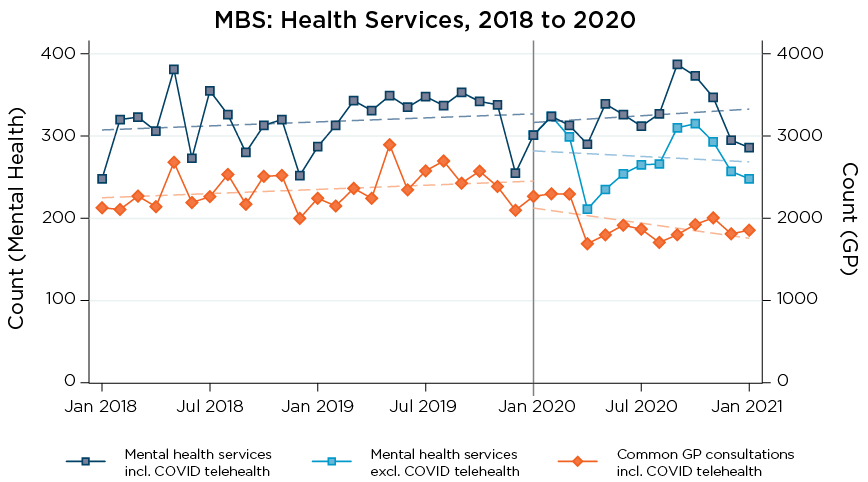
Notes: Displayed are counts of health care services in each calendar month between January 2018 and January 2021. The left vertical axis displays scale/labels for mental health services as listed under Table 2.4; the right vertical axis displays scale/labels for typical GP consultations (not specifically for mental health). Dotted lines are fitted through data points before/after January 2020, displaying trends before/during the COVID-19 pandemic respectively. N = 8,784 individuals.
Source: TTM, adult cohort, linked Medicare data from MBS
Rates of mental health service access, when including those delivered via telehealth, remained at levels similar to those recorded prior to the COVID-19 pandemic and its associated restrictions to in-person health care, as indicated by the fitted lines around January 2020. This suggests a substantial uptake of telehealth services among the TTM sample; however, delivering MBS mental health services via telehealth did not appear to result in lower service utilisation rates.
The linked MBS data also indicate that men who accessed mental health services during the COVID-19 pandemic had different histories of mental health care utilisation. Following March 30 2020, when stay-at-home restrictions were widely imposed with limited reasons to leave home, 9% of the sample (n = 748) used a MBS-funded mental health service at least once. Most of these men (78%) had previously accessed mental health care between March 2012 and March 2020. However, just over one in five (22%) men who used mental health services after the pandemic and associated restrictions commenced (i.e. after March 30, 2020) had not accessed MBS-funded mental health services since 2012; that is, they accessed such mental health care for the first time in at least nine years.
6 'Bulk billing' is when the Medicare benefit defined in the MBS is accepted by the health service provider as the full payment, such that no additional cost needs to be paid by the patient/client for a given service. Further information can be found at www.servicesaustralia.gov.au/bulk-billing?context=60092
7 The Better Access Initiative provided for up to 10 individual mental health services in a calendar year. More information can be found at www.health.gov.au/initiatives-and-programs/better-access-initiative
8 Comprehensive information on PBS fees, patient contributions and Safety Net thresholds is available at: www.pbs.gov.au/info/healthpro/explanatory-notes/front/fee
9 Since linked Medicare data do not fully cover 2012 and 2021, these were omitted from Figure 2.1. A small number of individuals also withdrew consent for data linkage during 2017, which resulted in a conservative estimate for that year.
10 Males living in remote and very remote areas of Australia were not recruited in Wave 1 of TTM; therefore, no comparisons can be made with residents of these areas. At Waves 2 and 3, the number of men who resided in remote areas was very low (n = 23 in Wave 2, n = 9 in Wave 3); to facilitate statistical analysis residents of regional/remote areas were grouped together.
11 This corresponds to mental health care records between 2013 and 2016 for Wave 1 and 2015 and 2018 for Wave 2 of TTM. Since linked Medicare data were only available up until February 2021, at the time of writing it was not possible to analyse (non-)use of health care for two years following Wave 3 of TTM.
12 Typical GP consultations are defined as MBS items 3, 23, 36 and 44, which are in-person consultations of varying time lengths, as well as items 91790, 91800, 91801 and 91802, which are corresponding telehealth counterparts. Typical GP consultations are much more common than mental health services; a separate scale is used in Figure 2.5 to facilitate comparisons.
Summary
This chapter examined MBS and PBS health care usage among men in the context of their reported depressive symptoms and in consideration of need, and their socio-economic status and demographic characteristics. It analysed Medicare data between March 2012 and February 2021, linked to self-report responses from the TTM survey.
Accessing mental health care
Men's reported depressive symptoms appeared to remain stable in aggregate when measured in 2013/14, 2015/16, and 2020/21. From the PHQ-9 scale of depressive symptoms, most (64%) men reported no to minimal depressive symptoms. Over 80% of men in this category would continue to report no to minimal symptoms when later surveyed, indicating a stability of relatively good mental health. For men who reported greater depressive symptoms, transitions to improved symptoms tended to be more likely (ranging from 10%-42%) than deteriorated symptoms (between 0.3%-13.7%). Between 32%-34% of men who reported severe depressive symptoms did so again in the following survey, suggesting that severe depression has a higher tendency to persist over time in comparison to milder depression.
Analyses showed that rates of both mental health service use and prescribing of mental health medications increased over the study period. Specifically, usage of mental health services increased from 7.2% of the sample in 2013 to 9.8% in 2020; mental health prescriptions likewise increased from 12.6% to 15.6% of the sample. Combined with evidence that indicated depressive symptoms remained similar across this period, the increased prevalence of mental health services and prescriptions suggests that access and norms around treating mental health may have improved between 2013 and 2021.
Predominant among men's access of mental health services were visits to GPs for mental health reasons. Between 2012 to 2021, 29% of men in the sample - nearly all the men who had accessed any mental health service - had consulted a GP about mental health at some point. This high rate relative to other service types is likely due to the role of general practice in the Australian health care system, as GPs are often the first port of call among Australian males with respect to health care needs (Swami, Terhaag, Quinn, & Daraganova, 2020) and can provide subsequent referrals to specialist services alongside the preparation of a mental health treatment plan for the individual.13 Annual out-of-pocket costs for men who consult with GPs for mental health consistently averaged below $30 across 2013-2020. This may reflect high rates of bulk-billing, subsidised services through the Better Access program, or the primary care role of GPs as men with lower mental health needs may not require repeated GP consultations nor specialist referrals.
Antidepressants appear to play a substantial role in the treatment of men's mental health. They were the largest category of mental health medication prescribed to participants between 2012 and 2021, constituting 74% of all prescription records. One-quarter of men in the sample filled an antidepressant prescription at some point over the nine-year period. Average annual out-of-pocket costs for antidepressants decreased by 11.5% from $125 in 2013 to $111 in 2020.
In comparison, health care services from specialists such as psychologists and psychiatrists became more expensive for the 4%-6% of participants who accessed these services in a given year between 2013 and 2020.
Mental health care usage by characteristics
Evidence from the multivariate model in this chapter indicated that rates of mental health care usage differed by socio-economic, health and demographic characteristics. In line with past research (Martin et al., 2021), men who reported greater depressive symptoms were more likely to access mental health care. Despite this, a large proportion of the sample with greater depressive symptoms did not subsequently access a relevant mental health service or prescription, suggesting that unmet need exists among Australian men experiencing mental health issues.
The results from the model also highlighted age, employment, disability and cultural background as factors associated with not using mental health care. Irrespective of reported depressive symptoms, employed men were less likely than unemployed men - who were again less likely than men out of the labour force - to access mental health care during the two years following interview at Waves 1 and 2. This is indicative of structural barriers to accessing mental health care, possibly as employed men have fewer opportunities to access mental health services. The links between mental health and labour market outcomes are complex (Olesen, Butterworth, Leach, Kelaher, & Pirkis, 2013); past research has shown that poor mental health can adversely affect labour market outcomes (Frijters, Johnston, & Shields, 2014; Olesen et al., 2013). Amid this literature, the results from this chapter show that, even among men with similar (greater) needs for mental health care, employed men are less likely to access publicly funded mental health care options than non-employed men.
Among those reporting greater depressive symptoms, younger men aged 18-24 years were 6-10 percentage points less likely than older men to access any mental health care two years after interview. This may reflect the young adulthood stage of the life course and a developing familiarity with professional help and mental health care from adolescence (Butterworth et al., 2021).
Those in the TTM sample with higher conformity to masculine norms were less likely to access health care than men with lower conformity to masculine norms, in line with research showing these men also had lower health literacy (Milner et al., 2019). Men who were classified as experiencing functional difficulty and/or disability were between 10-12 percentage points more likely to access mental health care. Men reporting greater depressive symptoms with greater conformity to masculine norms or who were from CALD backgrounds were 6 percentage points less likely to access mental health care within two years.
Levels of mental health service use did not seem to change for men during the COVID period between January 2020 and January 2021. Through this first year of the pandemic, mental health service usage appeared to be at levels similar to 2018 and 2019, suggesting that mental health care was sustained in the context of stay-at-home lockdown restrictions. However, the mode of these health services changed for some men; the number of in-person mental health services dropped beginning from March 2020 as more men used telehealth services, which had been made more broadly available following the introduction of COVID-19 into Australia. MBS data also showed an uptake in mental health care during the first year of COVID-19 by men who had not been in contact with such services for nearly a decade (or never); just over one in five (22%) men using mental health services after 30 March 2020 had not accessed mental health services at least since 2012. Thus, while levels of mental health service usage remained mostly steady through the onset of the COVID-19 pandemic, early evidence from the TTM survey and linked data suggest that many men were accessing Commonwealth-funded help for the first time.
Informing policy
Overall, the findings presented in this chapter could help inform future policies. Evidence from the statistical modelling indicates that younger age, employment and a CALD background were all associated with non-access of mental health care funded under the MBS and PBS, even after reporting greater depressive symptoms. In consideration of previous literature, these findings may reflect low levels of health literacy, limited service availability and accessibility, experience of stigma and unfamiliarity with the health care system (Chatmon, 2020; Gulliver, Griffiths, & Christensen, 2010; Lynch, Long, & Moorhead, 2018; Roche et al., 2016). For example, a systematic review of the impact of mental-health-related stigma on help seeking found that young people, men and ethnic minorities were all disproportionally deterred from help seeking for mental health problems by associated stigma (Clement et al., 2015). Targeted initiatives could aim to combat such barriers and lead to increased engagement with relevant services among these groups.
Being employed was also associated with non-utilisation of MBS and PBS services for mental health among TTM participants. Research has pointed to significantly higher levels of depression among workers specifically in male-dominated industries, highlighting a need to address the mental health of such workforces (Roche et al., 2016). Addressing structural barriers to mental health care for employed men may be beneficial for this group; the workplace could provide opportune settings to develop and deliver appropriate interventions for working males.
Future research opportunities
Men's use of services for their health needs, including for mental health, remains a public health priority. The findings presented in this chapter relate primarily to the use of mental health services and pharmaceuticals funded under the MBS and PBS; it is likely that some participants may have accessed mental health care through primary health network-commissioned mental health and suicide prevention services, in addition to publicly funded state/territory mental health services. Therefore, the estimates provided here regarding use of mental health services are more detailed than has previously been available but also somewhat conservative given the scope of the linkage. Future research could aim to explore patterns of non-MBS and PBS service access relating to mental ill-health among Australian males over time and how barriers and enablers differ between service types.
Future research using subsequent releases of TTM data can bring more insight into men's mental and other health needs and service use throughout the rest of the COVID-19 pandemic, and after. This may help evaluate the broader and longer-term implications of COVID-19, including lasting impacts of lockdown restrictions, and whether men continue to engage health professionals via telehealth. The available data could also be used to examine how men in priority groups (e.g. those residing in regional areas, Aboriginal and/or Torres Strait Islander men, those living with disability) have engaged with the health care system following COVID-19.
Research opportunities using Medicare data linked to the TTM survey are plentiful, extending well past the focus on mental health in this chapter. Investigations into primary care access, many categories of specialist services and prescription medication usage relating to different health conditions (including some measured in the TTM survey) may be feasible with the data from the MBS and PBS. Extensions to this chapter considering the timing between GP consultation and any subsequent specialist service or medication may also yield new findings on Australian men's health behaviours and outcomes. Further investigations relating to mental health may explore levels of MBS service use and PBS prescription access for mental health among Australian males by experience of self-injury and suicidality.
The analyses in this chapter examined and identified significant patterns in Australian men's access of mental health care, both over time and by key characteristics. While the analyses did not identify causal factors, the significant differences in men's health care access could motivate further research to explain why these patterns and differences arise. Additionally, since mental health is complex and needs can differ between individuals, this chapter does not evaluate whether certain health care outcomes are (in)adequate. Future work using the TTM survey and linked Medicare data may consider the causal pathways behind mental health/health care, and the extent to which health care adequately meets the needs of Australian men.
13 Mental health treatment plans are often arranged by GPs and a part of the Better Access initiative; more details are found at www.health.gov.au/initiatives-and-programs/better-access-initiative.
References
- Australian Bureau of Statistics (ABS). (2022). Health conditions prevalence. Canberra: ABS. Retrieved from www.abs.gov.au/statistics/health/health-conditions-and-risks/health-conditions-prevalence/latest-release#data-download
- Australian Institute of Health and Welfare (AIHW). (2016). Australia's health 2016. Canberra: AIHW. Retrieved from www.aihw.gov.au/reports/australias-health/australias-health-2016
- Australian Institute of Health and Welfare. (2018). Using PBS and MBS data to report on the treatment and management of chronic respiratory conditions 2016-17. Canberra: AIHW. Retrieved from www.aihw.gov.au/reports/chronic-respiratory-conditions/pbs-mbs-data-report-treatment-management-crc-16-17
- Australian Institute of Health and Welfare. (2022). Mental health services in Australia. Canberra: AIHW. Retrieved from www.aihw.gov.au/reports/mental-health-services/mental-health-services-in-australia
- Bandara, D., Howell, L., & Daraganova, G. (2021). Ten to Men: The Australian Longitudinal Study on Male Health - Data Dictionary, Data Release 3.0, September 2021. Melbourne: Australian Institute of Family Studies. Retrieved from tentomen.org.au/data-access-and-usage/data-documentation/data-dictionary/download
- Bandara, D., Howell, L., Silbert, M., & Daraganova, G. (2021). Ten to Men: The Australian Longitudinal Study on Male Health - Data User Guide, Version 4.0, September 2021. Melbourne: Australian Institute of Family Studies. Retrieved from tentomen.org.au/data-access-and-usage/data-documentation/data-user-guide
- Bruijniks, S. J. E., Bosmans, J., Peeters, F. P. M. L., Hollon, S. D., van Oppen, P., van den Boogaard, M. et al. (2015). Frequency and change mechanisms of psychotherapy among depressed patients: study protocol for a multicenter randomized trial comparing twice-weekly versus once-weekly sessions of CBT and IPT. BMC Psychiatry, 15, 137-137. doi:10.1186/s12888-015-0532-8
- Burgess, P. M., Pirkis, J. E., Slade, T. N., Johnston, A. K., Meadows, G. N., & Gunn, J. M. (2009). Service use for mental health problems: Findings from the 2007 National Survey of Mental Health and Wellbeing. Australian & New Zealand Journal of Psychiatry, 43(7), 615-623. doi:10.1080/00048670902970858
- Butterworth, P., de New, S. C., Schilling, C., Saxby, K., Petrie, D., & Wong, C. (2021). Dynamics of mental health and healthcare use among children and young adults. Australian Economic Review, 54(1), 130-142. doi.org/10.1111/1467-8462.12413
- Chatmon, B. N. (2020). Males and mental health stigma. American Journal of Men's Health, 14(4), 1557988320949322. doi:10.1177/1557988320949322
- Clement, S., Schauman, O., Graham, T., Maggioni, F., Evans-Lacko, S., Bezborodovs, N. et al. (2015). What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychological Medicine, 45(1), 11-27. doi:10.1017/S0033291714000129
- Doidge, J. C., & Harron, K. L. (2019). Reflections on modern methods: Linkage error bias. International Journal of Epidemiology, 48(6), 2050-2060. doi:10.1093/ije/dyz203
- Doran, C. M., & Kinchin, I. (2019). A review of the economic impact of mental illness. Australian Health Review, 43(1), 43-48. doi:10.1071/ah16115
- Frijters, P., Johnston, D. W., & Shields, M. A. (2014). The effect of mental health on employment: Evidence from Australian panel data. Health Economics, 23(9), 1058-1071. doi.org/10.1002/hec.3083
- Gulliver, A., Griffiths, K. M., & Christensen, H. (2010). Perceived barriers and facilitators to mental health help seeking in young people: A systematic review. BMC Psychiatry, 10, 113. doi:10.1186/1471-244X-10-113
- Holmes, E. A., O'Connor, R. C., Perry, V. H., Tracey, I., Wessely, S., Arseneault, L. et al. (2020). Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. The Lancet Psychiatry, 7(6), 547-560. doi.org/10.1016/S2215-0366(20)30168-1
- Hossain, M. M., Tasnim, S., Sultana, A., Faizah, F., Mazumder, H., Zou, L. et al. (2020). Epidemiology of mental health problems in COVID-19: a review. F1000Research, 9, 636-636. doi:10.12688/f1000research.24457.1
- Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606-613. Retrieved from www.ncbi.nlm.nih.gov/pmc/articles/PMC1495268/pdf/jgi_01114.pdf
- Lynch, L., Long, M., & Moorhead, A. (2018). Young men, help-seeking, and mental health services: Exploring barriers and solutions. American Journal of Men's Health, 12(1), 138-149. doi:10.1177/1557988315619469
- Mahalik, J. R., Levi-Minzi, M., & Walker, G. (2007). Masculinity and health behaviors in Australian men. Psychology of Men & Masculinity, 8(4), 240-249. doi:10.1037/1524-9220.8.4.240
- Mansfield, A. K., Addis, M. E., & Mahalik, J. R. (2003). 'Why won't he go to the doctor?': The psychology of men's help seeking. International Journal of Men's Health, 2, 93-110.
- Martin, S., Zajac, I., Vincent, A., Adams, R. J., Appleton, S., & Wittert, G. A. (2021). Effect of depression on health service utilisation in men: A prospective cohort study of Australian men aged 35 to 80 years. BMJ Open, 11(3), e044893. doi:10.1136/bmjopen-2020-044893
- Mellish, L., Karanges, E. A., Litchfield, M. J., Schaffer, A. L., Blanch, B., Daniels, B. J. et al. (2015). The Australian Pharmaceutical Benefits Scheme data collection: A practical guide for researchers. BMC Research Notes, 8(1), 634. doi:10.1186/s13104-015-1616-8
- Milner, A., Shields, M., & King, T. (2019). The influence of masculine norms and mental health on health literacy among men: Evidence from the Ten to Men study. American Journal of Men's Health, 13(5), 1557988319873532. doi:10.1177/1557988319873532
- Olesen, S. C., Butterworth, P., Leach, L. S., Kelaher, M., & Pirkis, J. (2013). Mental health affects future employment as job loss affects mental health: Findings from a longitudinal population study. BMC Psychiatry, 13(1), 144. doi:10.1186/1471-244X-13-144
- Productivity Commission. (2020). Mental Health. Report no. 95. Canberra: Productivity Commission. Retrieved from www.pc.gov.au/inquiries/completed/mental-health/report/mental-health-volume1.pdf
- Roche, A. M., Pidd, K., Fischer, J. A., Lee, N., Scarfe, A., & Kostadinov, V. (2016). Men, work, and mental health: A systematic review of depression in male-dominated industries and occupations. Safety and Health at Work, 7(4), 268-283. doi:10.1016/j.shaw.2016.04.005
- Swami, N., Prattley, J., Bandara, D., Howell, L., Silbert, M., Renda., J. et al. (2022). Ten to Men: The Australian Longitudinal Study on Male Health: Waves 1-3. The Australian Economic Review, 55(1), 155-165.
- Swami, N., Terhaag, S., Quinn, B., & Daraganova, G. (2020). Health literacy and health service use among Australian men. Insights #1: Findings from Ten to Men - The Australian Longitudinal Study on Male Health 2013-16. Melbourne: Australian Institute of Family Studies. Retrieved from tentomen.org.au/research-findings/insights-report/health
- van Gool, K., Parkinson, B., & Kenny, P. (2015). Medicare Australia data for research: An introduction. Cancer Research Economics Support Team. Retrieved from www.uts.edu.au/sites/default/files/2019-04/crest-factsheet-medicare-australia.pdf
The authors of this Insights #2 report chapter are extremely grateful to the many individuals and organisations who contributed to its development, and who continue to support and assist in all aspects of the Ten to Men study. The Department of Health and Aged Care commissioned and continues to fund Ten to Men. The study’s Scientific Advisory and Community Reference Groups provide indispensable guidance and expert input. The University of Melbourne coordinated Waves 1 and 2 of Ten to Men, and Roy Morgan collected the data at both these time points. The Social Research Centre collected Wave 3 data. A multitude of AIFS staff members collectively work towards the goal of producing high-quality publications of Ten to Men findings. We would also especially like to thank every Ten to Men participant who has devoted their time and energy to completing study surveys at each data collection wave
© GettyImages/ClarkandCompany
Wong, C., O’Donnell, K., Prattley, J., Jenkinson, R., Tajin, R., & Rowland, B. (2022). Mental health care needs and access among Australian men: A data linkage study. In B. Quinn, B. Rowland, & S. Martin (Eds.), Insights #2 report: Findings from Ten to Men – The Australian Longitudinal Study on Male Health 2013-21. Melbourne: Australian Institute of Family Studies.
3 November 2022