The use of intimate partner violence among Australian men
Ten to Men Insights #3 Report: Chapter 1
This research explores the use of intimate partner violence among Australian men, including factors that may reduce the likelihood of such behaviours. A public health approach is taken that considers the power of improving men’s health and wellbeing in relation to preventing intimate partner violence.
We acknowledge that the responsibility for intimate partner violence is with the person who uses/engages in the behaviour and not the victim–survivor who experiences it.
On this page:
- Key messages
- Research and policy implications
- What is intimate partner violence?
- Overview
- Methods
- Findings
- Summary
- References
- About the authors
- Acknowledgements
Key messages
-
In our nationwide sample, around 1 in 3 men (35%) reported they had ever used a form of intimate partner violence, as an adult, by 2022; this is up from 24% who had ever reported use by 2013-14. These estimates provide the first longitudinal data on the use of intimate partner violence from a representative sample of Australian men.

-
Emotional-type abuse (32% by 2022) was the most common form of intimate partner violence used, followed by physical violence (9% by 2022) and sexual abuse (2% by 2013–14).
-
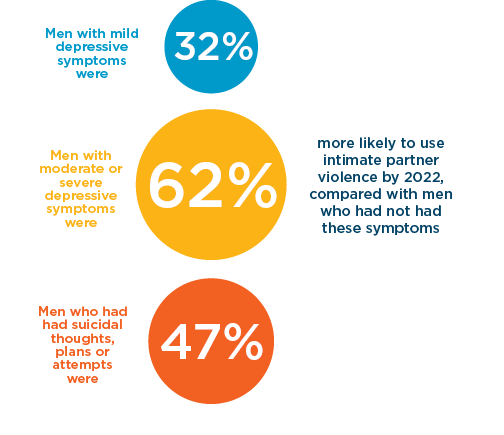
Men with depressive symptoms and those who had reported suicide related experiences by 2013–14 were more likely to have started using intimate partner violence by 2022.
-
By 2022, 25% of men reported ever using and experiencing intimate partner violence, more than twice the proportion who reported using violence but never experiencing it (10%).
-
Social support and paternal affection were protective against intimate partner violence use.
Men with higher levels of social support in 2013–14 were 26% less likely to start using intimate partner violence by 2022 compared to men with lower levels of social support.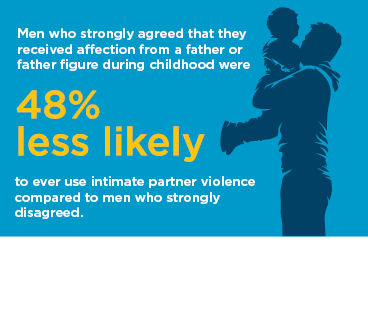
Research and policy implications
Our findings highlight the importance of mental health and social support as well as paternal affection in childhood in men’s use of intimate partner violence. Policy and practice changes that focus on providing integrated mental health support for men, and programs that promote the importance of social support as well as good quality relationships between fathers and their sons could contribute to a reduction in men’s use of intimate partner violence.
What is intimate partner violence?
Definitions of intimate partner violence, and other forms of gender-based violence, can vary substantially between the academic community and both the private and public sectors. Across these settings, intimate partner violence can also be known as ‘domestic violence’, ‘domestic abuse’, ‘domestic violence and abuse’ and ‘dating violence’ (Heyman et al., 2022). In the National Plan to End Violence Against Women and Children 2022–2032 (Department of Social Services [DSS], 2022), these definitional inconsistencies are acknowledged as a whole-of-system issue, and the need to work towards national consistency is emphasised. In this research, we adopt the definition of intimate partner violence set out in the National Plan as:
Any behaviour within an intimate relationship (including current or past marriages, domestic partnerships or dates) that causes physical, sexual or psychological harm ... Intimate partner violence can occur outside of a domestic setting, such as in public, and between 2 people that do not live together. (DSS, 2022, p 37)
In this research, 3 specific forms of violent and abusive behaviour (emotional-type abuse, physical violence and sexual abuse) carried out within the bounds of an intimate relationship are captured. For readability, men’s use of (also known as perpetration of) these violent and/or abusive behaviours will be collectively referred to as ‘use of intimate partner violence’. Men’s experiences of violent and/or abusive treatment within an intimate relationship will be collectively referred to as ‘experience of intimate partner violence’. Further details on the measures of intimate partner violence included in this report are available in the Methods section. Intimate partner violence is a critical health issue in Australia and has recently been described as a national crisis by advocates, members of parliament and support services (Campbell et al., 2024). This form of violence is widespread in our communities, with estimates suggesting that 1 in 4 women and 1 in 14 men are victim-survivors of intimate partner violence (Australian Bureau of Statistics [ABS], 2023). Reducing the rates of intimate partner violence and other forms of family, domestic and sexual violence is a national priority that requires an evidence-informed approach to address the drivers of violence across all areas of society (Our Watch, 2021).
Overview
Men’s use of intimate partner violence
Use of violence and/or abuse in intimate relationships is higher among men than women (Flood et al., 2022). A focus area of the National Plan to End Violence Against Women and Children 2022–2032 (National Plan) is working with men and boys to prevent violence against women and girls (DSS, 2022). Most of the current evidence base of men’s use of intimate partner violence in Australia is drawn from administrative datasets in the criminal justice system or from specific subpopulations of men (Flood et al., 2022). These data sources cannot be used to comprehensively understand the scope of intimate partner violence in Australia or to examine factors that may contribute to the use of intimate partner violence among men at a population level (Payne & Morgan, 2024).
Evidence-based findings, particularly those at a population level, have a key role in supporting the ongoing efforts to reduce the use of intimate partner violence in Australia (DSS, 2022). Understanding the factors associated with the use of intimate partner violence is crucial for developing effective prevention and intervention strategies (Campbell et al., 2024). The aim of this chapter is to better understand the magnitude of intimate partner violence use by Australian men over time and gain further knowledge of the factors that may reduce the likelihood of men using intimate partner violence.
Aligned with the National Plan, in this research we apply a socio-ecological perspective to men’s use of intimate partner violence. Adopting this lens means we consider factors associated with the use of intimate partner violence at various levels of analysis, including the ‘individual and relationship’ level, such as individual attitudes, health and close relationships; the ‘organisation and community’ level, including the settings where people live, work and play; and the overarching ‘societal level’ that includes broad factors that create a climate where violence can occur (DSS, 2023). There is an additional level, which the Ten to Men study does not have relevant data on and is therefore not considered in this research, called the ‘systems and institutional’ level. This domain captures the systems, institutions and policies that protect Australians.
There are many known factors, across each of these levels, associated with men’s use of intimate partner violence (Hardesty & Ogolsky, 2020; Meyer et al., 2024). In this research, we specifically focus on selected health, relational and personal historical factors, of which there is limited evidence in the Australian context. These factors include mental health, wellbeing, social support and the paternal affection received during childhood. Where relevant, our analyses account for the potential influence of individual, community and societal factors that are associated with intimate partner violence use, such as alcohol and drug use, masculine norms and area-level socio-economic status (see supplementary materials for more detail). These factors, while important, are beyond the scope of the current study and are therefore not part of our research objective.
Mental health
Mental ill-health is high among Australia men, with estimates suggesting that up to 25% of men will be diagnosed with a mental health disorder in their lifetime (Terhaag et al., 2020). Recent statistics show that death by suicide continues to be substantially higher among Australian men than women, with 75% of those who died by suicide in 2023 identified as male (ABS, 2023). Within the context of intimate partner violence, these figures are concerning, as international evidence shows that men who use intimate partner violence are more likely to have mental health conditions, including depression and anxiety (Oram et al., 2014; Spencer et al., 2019; Spencer et al., 2024; Yu et al., 2019). Some studies have also demonstrated a link between suicidal behaviour and the use of intimate partner violence among men in the family court system (Conner, Cerulli, & Caine, 2002; Dalve et al., 2024; Wolford-Clevenger et al., 2017).
There is little Australian evidence on the link between mental health and the use of intimate partner violence (Hulme, Morgan, & Boxall, 2019). Of the scant Australian evidence available, one study found that those in contact with police for using intimate partner violence were 11 times more likely than the general population to have a prior mental health-related presentation to a hospital emergency department (Papalia et al., 2024). In this chapter, we consider how depressive symptoms, an anxiety diagnosis and suicidal behaviours are associated with the later use of intimate partner violence.
Wellbeing and social support
As with mental health, there is little evidence on the link between men’s wellbeing and the use of intimate partner violence. Wellbeing is interconnected with mental health and represents an overall holistic state of wellness, including satisfaction with life, social fulfillment and general health (Kansky & Diener, 2022). Wellbeing factors, such as receiving adequate social support, can be protective and are associated with a decreased risk of intimate partner violence use (Capaldi et al., 2012; Spencer et al., 2022). However, there is still a gap in knowledge about links between other facets of wellbeing and use of intimate partner violence.
It is important to consider the role of wellbeing factors in men’s use of intimate partner violence alongside mental health to attain a holistic understanding of the underlying factors that may drive intimate partner violence use. In this research, we consider how social support and life satisfaction are associated with the later use of intimate partner violence.
Paternal affection
Family factors have a significant role in the use of intimate partner violence. Exposure to intimate partner or family violence during childhood is a well-known risk factor for the later use of intimate partner violence (Akcabozan Kayabol, 2023; Clare et al., 2021). Other familial factors, such as the parent–child relationship, can be protective against intimate partner violence, with evidence showing that individuals with good quality parent–child relationship are less likely to use intimate partner violence (Kaufman-Parks et al., 2018). Previous research in this area has focused on the influence on maternal affection on later intimate partner violence (Chiesa et al., 2018). Less is known about the specific role of the father–son relationship and whether a quality relationship with one’s father or father figure during childhood is a protective factor.
Fathers and father figures are central to providing children with a secure form of attachment and are typically the first male role models for young boys on how to express love and affection (Floyd et al., 2021). Establishing a secure attachment with caregivers during childhood is associated with better interpersonal functioning, emotional regulation and conflict resolution skills during adulthood (Brennan & Shaver, 1995; Chauhan et al., 2014; Thompson et al., 2022). We suggest that paternal affection may play a protective role in men’s use of intimate partner violence, and we test this hypothesis in this research.
Research in context
Evidence before this research
- The existing evidence base on intimate partner violence use by Australian men heavily relies on administrative data from the criminal justice system or studies on specific subpopulations.
- Limited understanding of the link between use of intimate partner violence and mental health, social support and paternal affection, in samples of Australian men.
Added value of this research
- This study provides the first longitudinal data on the use of intimate partner violence from a representative sample of Australian men.
- This study also provides unique insights on factors that are associated with the likelihood of Australian men starting to use intimate partner violence.
- This is the first Australian study to explore affection in the father-son relationship during childhood and men’s later use of intimate partner violence.
Research objectives
Unique to Ten to Men is longitudinal, self-reported data on the use of intimate partner violence that can be mapped against individual, societal or cultural level factors. This study uses data from Wave 1 (2013–14) and Wave 4 (2022) of Ten to Men to detail the use of intimate partner violence by men in Australia who were aged 18–57 at Wave 1 (2013–14) and to investigate the factors that impact the likelihood of starting to use intimate partner violence. To this end, the following research questions are addressed:
- How have rates of use of intimate partner violence changed among Australian adult men over time?
- What was the cumulative prevalence of use of intimate partner violence by 2013–14 and by 2022?
- For men who have ever used intimate partner violence, have they also ever experienced intimate partner violence?
- Does the prevalence differ for different types of intimate partner violence?
- Does the use of intimate partner violence differ between men in different age cohorts and priority population groups?
- How is mental health and wellbeing associated with new incidences of intimate partner violence use? Specifically, do any of the following experienced in 2013–14 predict the likelihood of the later first use of
intimate partner violence (men who reported use by 2022 but not 2013–14):- depressive symptoms
- anxiety diagnosis
- suicidal thoughts, plans or attempts
- life satisfaction
- social support.
- Is a quality relationship with a father figure during childhood protective against the use of intimate partner violence in adulthood? Specifically, does receiving affection from a father or father figure in childhood predict the likelihood of the later use of intimate partner violence?
Methods
This section describes the key measures and data analysis techniques used to address the research objectives. The overall methodology of the Ten to Men study is detailed elsewhere (see Bandara et al., 2021; Swami et al., 2022).
Measures
Intimate partner violence
Ten to Men respondents were surveyed about their use of, and experience of, forms of intimate partner violence in 2013–14 (Wave 1) and 2022 (Wave 4). In 2013–14, 3 types of intimate partner violence were measured, one indicator each for emotional-type abuse, physical violence and sexual abuse. In the 2022 survey, sexual abuse was not measured, given concerns about possible mandatory reporting obligations at the time. The questions used in Ten to Men were adapted from the COHSAR (Comparing Heterosexual and Same Sex Abuse in Relationships; Donovan et al., 2005) measure. At the time of developing the Wave 1 survey, for 2013–14, the COHSAR was one of the few measures of intimate partner violence that had been validated among a sample of men (Donovan et al., 2005).
To understand the use of intimate partner violence, respondents were presented with a series of questions following the prompt, ‘As an adult, how have you behaved towards a past or present partner?’, and asked to respond either ‘yes’ or ‘no’. Respondents were also able to skip answering these questions. The questions included:
- Have you ever behaved in a manner that has made a partner feel frightened or anxious? (emotional-type abuse)1
- Have you ever hit, slapped, kicked or otherwise physically hurt a partner when you were angry? (physical violence)
- Have you ever forced a partner to have sex or made them engage in any sexual activity they did not want? (sexual abuse)2
Similarly, to measure men’s experience of intimate partner violence, respondents were presented with a series of questions following the prompt, ‘As an adult, have you ever experienced any of the following?’, and asked to respond either ‘yes’ or ‘no’. Respondents were also able to skip answering these questions. The questions included:
- Have you ever felt frightened or anxious because of the behaviour of a partner? (emotional-type abuse).
- Have you ever been hit, slapped, kicked or otherwise physically hurt by a partner when they were angry? (physical violence).
- Has a partner ever forced you to have sex or made you engage in any sexual activity you did not want? (sexual abuse).
As men’s histories with these types of violence and/or abuse were captured as whether they had ‘ever’ used or experienced each type, our data provide an estimate of intimate partner violence among men by 2013–14 and by 2022. Men were categorised as ever having used or experienced forms of intimate partner violence by 2013–14 if they had responded ‘yes’ to any of the types of intimate partner violence. Similarly, men were coded as ever having used or experienced forms of intimate partner violence by 2022 if they had responded ‘yes’ to any of the types of violence at either the 2013–14 survey or the 2022 survey. Men were considered a ‘new incidence’ of either intimate partner violence use or experience if they responded ‘no’ to all types of intimate partner violence in 2013–14 but ‘yes’ to any type of intimate partner violence by 2022.
Mental health and wellbeing
Depressive symptoms
Depressive symptoms, in 2013–14, were measured using the Patient Health Questionnaire (PHQ)-9. The PHQ-9 assesses the experience and severity of depressive symptoms over the past 2 weeks (Kroenke et al., 2001). For each respondent, a total PHQ-9 score was calculated by summing individuals’ responses to 9 questions, resulting in a total score ranging from 0 to 21. Depressive symptoms were categorised as ‘1 = No or minimal depression’ (score between 0 and 4), ‘2 = Mild depression’ (score between 5 and 9) and ‘3 = Moderate or severe depression’ (score of 10 or greater).
Anxiety diagnosis
Whether men had ever received an anxiety diagnosis by 2013–14 was measured with the question, ‘Has a doctor or other health professional ever told you that you had this condition? Anxiety disorders.’ Responses were coded as ‘0 = Never diagnosed with an anxiety disorder’ and ‘1 = Ever diagnosed with an anxiety disorder’.
Suicidal behaviours
In 2013–14, men were asked to respond either ‘yes’ or ‘no’ to the following questions around their experience with suicidal thoughts, plans and attempt.
- Have you seriously thought about killing yourself ever in your life? (thoughts)
- Have you ever made a plan about how you would kill yourself ever in your life? (plans)
- Have you ever tried to kill yourself ever in your life? (attempt)
These questions were coded as indicators of whether men had reported any suicidal behaviour by 2013–14, with ‘0 = No’ and ‘1 = Yes’.
Life satisfaction
Life satisfaction was measured with the Personal Wellbeing Index (International Wellbeing Group, 2013), a measure of how satisfied individuals are with their quality of life made up of 7 questions measuring their standard of living, health, achievements, relationships, safety, community connection and future security. Respondents were asked to provide a response to each question on a scale of ‘0 = No satisfaction at all’ to ’10 = Completely satisfied’. For each respondent, a total life satisfaction score out of 100 was derived by summing each item, with higher scores indicating greater satisfaction with life (see Ten to Men ‘Guide to items and scales’ for more information). These scores were then split into quantiles to get 3 categories of life satisfaction, coded as ‘0 = Low satisfaction’, ‘1 = Moderate satisfaction’ and ‘2 = High satisfaction’.
Social support
Social support was measured using the emotional/informational support subscale of the Medical Outcomes Study (MOS) Social Support Survey (Sherbourne & Stewart, 1991). Respondents were presented with a series of 8 statements and asked to select on a scale of ‘1 = None of the time’ to ‘5 = All of the time’ how often each kind of support is available to them if they need it. Example statements include ‘Someone you can count on to listen to you when you need to talk’ and ‘Someone to give you information to help you understand a situation.’ The average of the scores for each item was calculated and then transformed into a score out of 100. Social support was then categorised into quantiles and coded in 3 categories ‘1 = Low social support’, ‘2 = Middle social support’ and ‘3 = High social support’.
Paternal affection
Paternal affection was measured using the Paternal Affection Scale (Brim et al., 1996) and only asked of respondents at Wave 2 of the Ten to Men study. Using response options varying from ‘1 = Strongly disagree’ to ‘5 = Strongly agree’, men were asked to respond to their agreement with a series of 6 statements about their father or father figure during childhood. Example statements include ‘He understood my problems or worries’ and ‘He gave me the love and affection I needed’. Responses to the 6 items were summed and an average score on the scale was then calculated for each respondent. These scores were then further coded into 5 distinct categories of those that, on average, strongly disagreed (score of 1–1.99; coded as 1), disagreed (score of 2–2.99; coded as 2), neither agreed nor disagreed (score of 3–3.99; coded as 3), agreed (score of 4–4.99; coded as 4) and strongly agreed (score of 5; coded as 5).
Demographic and other factors
This chapter uses several demographic and other factors to give further context to how the use of intimate partner violence differs between different groups of men. Additionally, some of these factors were included as covariates in the analyses for research questions 2 and 3. These factors include age, cultural and linguistic diversity, disability, area-level disadvantage, geographic region, sexual identity, marital status, alcohol use, drug use, masculine norms and financial stress. Please see the supplementary materials for additional information on how these factors were measured and coded.
Data analysis
Research question 1
The weighted proportions of men who had ever used intimate partner violence by 2013–14 and by 2022 were estimated. The weighted proportion of men who reported using intimate partner violence by 2022, but not by 2013–14, was also estimated, and a direct age-standardised incidence rate was calculated (as per the Australian Institute of Health and Welfare [AIHW], 2011). Additional weighted proportions were estimated to get the proportion of men who reported ever using intimate partner violence without having ever experienced intimate partner violence and the proportion of men who had both used and experienced intimate partner violence.
To test for potential group differences in the use of intimate partner violence by age and priority population groups set out in the National Men’s Health Strategy 2020–2030 (NHMS), the weighted proportions of men who ever used intimate partner violence, across those groups, by 2013–14 and by 2022 were estimated. Age differences were considered by categorising men into 1 of 4 cohorts depending on their age in 2013–14. The cohorts include young adult men (aged 18–24 years in 2013–14 and 27–33 years in 2022), early adult men (aged 25–34 years in 2013–14 and 34–43 years in 2022), middle adult men (aged 35–44 years in 2013–14 and 44–53 years in 2022) and later adult men (aged 45–57 years in 2013–14 and 54–66 years in 2022). The priority groups were defined using the 2013–14 data and include men from culturally and/or linguistically diverse backgrounds, men living in regional areas, men with disability, men living in socio-economically disadvantaged areas and those who do not identify as heterosexual. Although Aboriginal and/or Torres Strait Islander men are identified as a priority population group in the NMHS, we did not examine differences in the use of intimate partner violence among these men in our data due to small sample sizes.
Research question 2
A Poisson regression analysis was conducted to examine the relationship between ever using intimate partner violence by 2022 for the men who had not reported using this behaviour by 2013–14 and several mental health and wellbeing predictor variables measured in 2013–14 including depressive symptoms; ever receiving an anxiety diagnosis; ever experiencing suicidal thoughts, having a suicide plan or attempting suicide; life satisfaction and social support. First, a series of univariable models were tested for each predictor variable and the outcome measure to determine the unadjusted relationship of each. Next a multivariable model was tested with all predictor variables included in the one model with a collection of covariates to account for the association of other relevant health, economic and psychological factors. The covariates included age, region, area-level disadvantage, marital status, sexual identity, masculine norms, drug use, alcohol use and financial stress. Multicollinearity (correlations between the predictors) was assessed through comparison of estimates from univariable, minimally adjusted and fully adjusted models, cross-tabulations and estimation of variance inflation factors. Refer to the supplementary materials for further information on the analytical model tested (Table S1) and the rationale for other variables included in the model.
Research question 3
A Poisson regression analysis was conducted to examine the relationship between ever using intimate partner violence by 2022 and perceptions of affection from a father or father figure during childhood. First, a univariable model was tested to examine the base association between the use of intimate partner violence and paternal affection. Next a multivariable model was tested that included the covariates of age, sexual identity and masculine norms. Refer to the supplementary materials for further information on the analytical model tested (Table S2) and the rationale for other variables included in the model.
Findings
Intimate partner violence use among Australian men by 2013–14 and 2022
In our nationwide data, by 2013–14 almost 1 in 4 men (24%) reported having ever used intimate partner violence (Table 1.1). By 2022, the proportion for this cohort of men was just over 1 in 3 (35%); that is, an additional 11% of men reported having ever used intimate partner violence between 2013–14 and 2022. At a population level, this equates to an additional 118,476 Australian men (aged 18–57 years in 2013–14), starting to use intimate partner violence each year, on average, or around an additional 1.8% of men per year. This is an estimated incidence rate of 17 men per 1,000 person-years. (Note: a person-year is a type of measurement that accounts both for the number of people in the study and the duration each person has been followed. For example, a study that follows 1,000 people for 1 year, would provide 1,000 person-years.) See Table S5 in supplementary materials for further information.
In our sample, more than twice as many men reported having both ever used and experienced intimate partner violence as reported only ever having used intimate partner violence. By 2013–14, 18% of men reported both using and experiencing intimate partner violence compared to 8% of men who reported only using intimate partner violence. These proportions were higher by 2022, with 25% of men reporting both using and experiencing intimate partner violence and 10% of men reporting its use only. These results indicate that both using and experiencing forms of intimate partner violence is more common than only using it.
Table 1.1: The weighted proportions of ‘ever’ having used intimate partner violence (IPV) among Australian men by 2013–14 and by 2022
By 2013–14 | By 2022 | |||
|---|---|---|---|---|
% | 95% CI | % | 95% CI | |
| Overall use of IPV | 24.1 | 22.5, 25.9 | 35.4 | 33.5, 37.4 |
| New incidence use of IPV | - | - | 11.3 | 10.1, 12.6 |
| Ever used IPV only | 8.3a | 7.4, 9.5 | 10.1b | 8.9, 11.3 |
| Ever used and experienced IPV | 17.5a | 16.4, 19.2 | 25.0b | 23.5, 26.93 |
Notes: Sample consists of men who responded to the intimate partner violence questions at both Wave 1 (2013–14) and Wave 4 (2022).
aThe number of respondents for the 2013–14 data is N = 4,176.
bThe number of respondents for the 2022 data is N = 4,329. More men had a valid response to the intimate partner violence questions in 2022 due to missing data at the Wave 1 variable.
Source: TTM, population weighted, Waves 1 and 4
Use of different types of intimate partner violence
In our data, 3 types of intimate partner violence were measured: emotional-type abuse, physical violence and sexual abuse.3 Emotional-type abuse was the most common form of intimate partner violence used by Australian men, followed by physical violence and sexual abuse (Figure 1.1). By 2013–14, just over 1 in 5 men (21%) reported having ever made an intimate partner ‘feel frightened or anxious’. There were 6% of men who reported that they had ever ‘hit, slapped, kicked or otherwise physically hurt’ an intimate partner when they were angry and 2% of men who reported ever forcing an intimate partner to ‘have sex or engage in any sexual activity they did not want’.
About 1.5 times the proportion of men who reported using emotional-type abuse or physical violence in 2013–14 reported their use in 2022. By 2022, 32% of men reported ever having made an intimate partner ‘feel frightened or anxious’, up 11 percentage points from 2013–14. For physical violence, by 2022, 9% of men reported that they had ever ‘hit, slapped, kicked or otherwise physically hurt’ an intimate partner when they were angry, up 3 percentage points from 2013–14. Sexual violence was only measured in the 2013–14 survey and therefore a comparison with 2022 cannot be made.
Figure 1.1: Proportion of Australian men who reported using different types of intimate partner violence by 2013–14 and by 2022
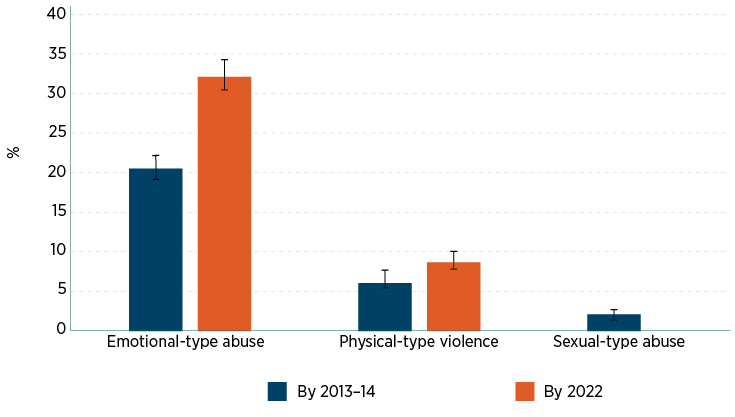
Notes: Sample consists of men who responded to the intimate partner violence questions at both Wave 1 (2013–14) and Wave 4 (2022). Emotional-type abuse, N = 4,941. Physical violence, N = 5,179. Sexual abuse was only measured at Wave 1 (2013–14), N = 13,409.
Source: TTM, population weighted, Waves 1 and 4
Use of intimate partner violence by age
By 2013–14, there were differences by age in the prevalence of intimate partner violence use, with young adult men (those aged 18–24 years) reporting the lowest use of intimate partner violence (13%), compared to other age groups (22%–25%; see Figure 1.2). This is likely due, in part, to this group having had less time to engage in intimate relationships compared to other age groups. By 2022, there were no notable differences in the prevalence of intimate partner violence use between the age cohorts (as determined by the overlap in the 95% confidence intervals between each cohort). This suggests that rates of ever having used intimate partner violence do not meaningfully differ among the adult men in our sample who have been in an intimate relationship.
For each age cohort the use of intimate partner violence notably increased over time (see Figure 1.2). By 2022, use among the youngest cohort, now aged 27–33 years, increased by 17 percentage points. Similarly, among the next age cohort, now aged 34–43 years, use of intimate partner violence by 2022 increased by 15 percentage points. The increase among the middle adult cohort, now aged 44–53 years, was 12 percentage points. The later adult cohort, men now aged 54–63 years, showed the smallest increase of 7 percentage points by 2022. In summary, the use of intimate partner violence notably increased among all age cohorts between 2013–14 and 2022, and although the increase among the older men wasn’t as high as with the other age cohorts, there was still a significant change between the two time points.
Figure 1.2: Proportion of Australian men who report using intimate partner violence by 2013–14 and 2022 for different age cohorts (age at 2013–14)
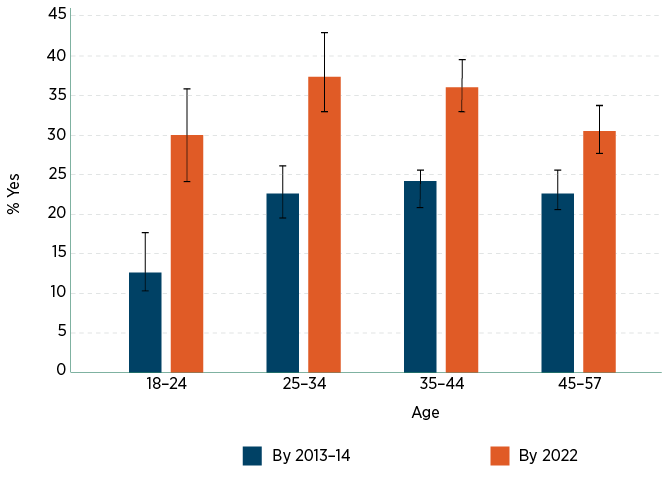
Notes: Sample consists of men who responded to the intimate partner violence questions at both Wave 1 (2013–14), N = 4,947 and Wave 4 (2022), N = 4,603. Young adult men = 18–24 years in 2013–14 and 27–33 years in 2022. Early adult men = 25–34 years in 2013–14 and 34–43 years in 2022. Middle adult men = 35–44 years in 2013–14 and 44–53 years in 2022. Later adult men = 45–57 years in 2013–14 and 54–66 years in 2022. See Table S6 in the supplementary materials for unweighted estimates and number of observations.
Source: TTM, population weighted, Waves 1 and 4
Use of intimate partner violence by men in priority population groups
There were no meaningful differences in the use of intimate partner violence by 2013–14 and by 2022 for select priority population groups, except for men with disability (see Figure 1.3). In the 2013–14 data, rates of intimate partner violence use were higher among men with disability (34%) compared to men without disability (21%). By 2022, this difference was no longer observed. Due to a comparatively smaller sample size of men with disability in 2013–14 (N = 82) compared to those without (N = 1,061), this finding must be interpreted with caution. Further, due to limitations in sample size, we were unable to explore an explanation for this finding, such as the effect of age or type of disability (Bowen & Swift, 2019).
Additionally, the increase in prevalence of intimate partner violence use over time is proportionally similar between men in the priority population groups and men who are not in these groups. For example, 20% of culturally or linguistically diverse men reported using intimate partner violence by 2013–14, increasing to 35% by 2022 (around 1.7 times the rate reported by 2013–14). Over the same period, 22% of men who are not culturally and/or linguistically diverse reported using intimate partner violence increasing to 36% by 2022 (around 1.6 times the rate reported by 2013–14). This pattern of results suggests that the prevalence of use of intimate partner violence increased similarly over time, irrespective of priority group membership (except for men with disability as noted earlier). For further comparisons see Figure 1.3.
Figure 1.3: Weighted proportions of ever using intimate partner violence among Australian men by 2013–14 and 2022 for select priority population groups
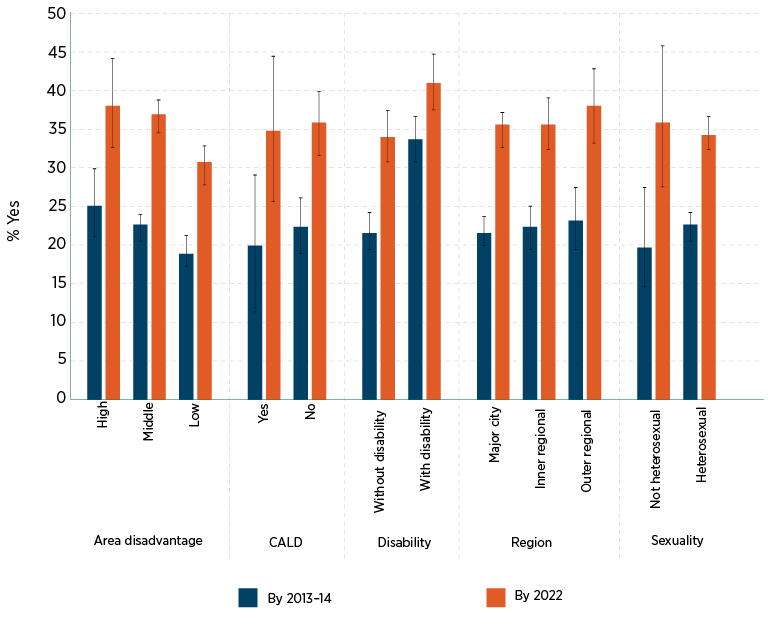
Notes: Sample consists of men who responded to the intimate partner violence questions at both Wave 1 (2013–14) and Wave 4 (2022). See Table S6 in the supplementary materials for unweighted estimates and number of observations. CALD = Culturally and linguistically diverse.
Source: TTM, population weighted, Waves 1 and 4
Association between mental health and wellbeing and the use of intimate partner violence
By 2022, men who earlier reported depressive symptoms or ever having suicide thoughts, plans or attempts were more likely to later report their first use of intimate partner violence (see Table 1.4). When compared to those with no or minimal depressive symptoms in 2013–14, those with mild depressive symptoms had a 32% (95% CI = 1.08, 1.62) increased risk of using intimate partner violence by 2022 and those with moderate or severe depressive symptoms had a 62% (95% CI = 1.21, 2.18) increased risk of using intimate partner violence by 2022. Men who reported ever engaging in any suicide-related behaviours in 2013–14, compared to those who reported no suicide-related behaviours, had a 47% (95% CI = 1.19, 1.81) increased risk of starting to use intimate partner violence by 2022.
The findings also showed that men with more social support in 2013–14, such as those who felt they had social support ‘all of the time’, were less likely to start using intimate partner violence by 2022 (see Table 1.2). Compared to men with less social support, men with the highest levels of social support were 26% (95% CI = 0.55, 0.99) less likely to report intimate partner violence use by 2022.
After accounting for other mental health, wellbeing, economic and psychological factors, our analysis showed no associations between ever receiving an anxiety diagnosis or overall life satisfaction in 2013–14 and men’s first use of intimate partner violence by 2022. The presence of weak multicollinearity between the predictors did not substantially affect the estimated associations (refer to Tables S7 and S8). For further information on how each of the mental health and wellbeing variables are associated with first use of intimate partner violence by 2022 refer to Table S7 in the supplementary materials.
Table 1.2: The relationship between indicators of mental health and wellbeing in 2013–14 and later use of intimate partner violence by 2022 in men who reported no use of intimate partner violence (IPV) by 2013–14
| Any IPV use by 2022, if no use by 2013–14 (ref = no IPV use by 2022; N = 5,036) | ||
|---|---|---|
| iRR [95% CI] | p | |
| Depressive symptoms (ref = no or minimal symptoms) | ||
| Mild depressive symptoms | 1.32 [1.08, 1.62] | 0.007 |
| Moderate/Severe depressive symptoms | 1.62 [1.21, 2.18] | 0.001 |
| Anxiety diagnosis (ref = never been diagnosed) | 1.00 [0.73, 1.37] | 0.987 |
| Suicidal behaviours (ref = never had suicidal behaviours) | 1.47 [1.19, 1.81] | <0.001 |
| Life satisfaction (ref = low) | ||
| Middle | 1.31 [0.94, 1.84] | 0.114 |
| High | 1.25 [0.85, 1.83] | 0.263 |
| Social support (ref = low support) | ||
| Middle support | 1.05 [0.84, 1.31] | 0.665 |
| High support | 0.74 [0.55, 0.99] | 0.043 |
Notes: iRR = incidence risk ratio; 95% CI = 95% confidence interval; p = p value. The model is adjusted for the following indicators at 2013–14: age, region, area-level disadvantage, marital status, sexual identity, masculine norms, drug use, alcohol use and financial stress. See Table S3 in the supplementary materials for further information of the proportion of respondents across each category of the raw exposure variables. N = 3,380.
Source: TTM data, unweighted, Waves 1 and 4
The relationship between paternal affection and use of intimate partner violence
According to our analysis, receiving affection from a father or father figure growing up is associated with a decreased risk of using intimate partner violence in later life (see Table 1.3). The more strongly men agreed that they had received affection from a father or father figure, the less likely they were to report using intimate partner violence. When compared to strongly disagreeing that affection was shown from a father or father figure during childhood, the risk of the later use of intimate partner violence decreased by 29% (95% CI = 0.63, 0.81) for those who ‘neither agree nor disagree’, 42% (95% CI = 0.50, 0.67) for those who ‘agree’, and 48% (95% CI = 0.38, 0.70) for those who ‘strongly agree’. For further information, see Table S9 in supplementary materials.
Table 1.3: Parameter estimates from a Poisson regression model examining the relationship between paternal affection scores and use of intimate partner violence (IPV)
| Any IPV use by 2022, if no use by 2013–14 (ref = no IPV use by 2022; N = 5,036) | ||
|---|---|---|
| iRR [95% CI] | p | |
| Paternal affection score (ref strongly disagree) | ||
| Disagree | 0.90 [0.78, 1.03] | 0.12 |
| Neither agree nor disagree | 0.71 [0.63, 0.81] | <0.001 |
| Agree | 0.58 [0.50, 0.67] | <0.001 |
| Strongly agree | 0.52 [0.38, 0.70] | <0.001 |
Notes: iRR = incidence risk ratio; 95% CI = 95% confidence interval; p = p value. The model is adjusted for the following indicators at 2013–14: age, sexual identity and masculine norms. The model is not adjusted for the mental health exposures considered in Table 1.2 (depression, anxiety, suicidal behaviours, life satisfaction, social support). See Table S3 in the supplementary materials for further information of the proportion of respondents across each category of the raw exposure variable. When paternal affection is coded as a total score (i.e. not categorised), the association with use of intimate partner violence is iRR = 0.83, CI 95% = 0.79, 0.86, p value = <0.001. N = 4,348.
Source: TTM data, unweighted, Waves 1, 2 and 4
Summary
This research aimed to better understand men’s use of intimate partner violence in Australia by analysing the first longitudinal data of such behaviour worldwide. Our findings are intended to inform current efforts to end family, domestic and sexual violence in our communities. This report provides a clearer understanding of how this behaviour changes over time. We have also identified factors that could alter the likelihood of men engaging in intimate partner violence.
Use of intimate partner violence among men
In 2013–14 around 1 in 4 men reported ever having used intimate partner violence, with this number sitting at 1 in 3 men by 2022. At a population level, our findings correspond to around an additional 120,000 Australian men (aged between 18–57 years in 2013–14) per year, over the 9-year study period, starting to use intimate partner violence. There is no other comparable nationally representative Australian data on men’s use of intimate partner violence. Looking internationally, it is difficult to compare our data as estimates of men’s intimate partner violence use vary widely across countries and regions. In the UN Multi-country Study on Men and Violence in Asia and the Pacific (Fulu et al., 2013), on average, 1 in 4 of the 10,000 men surveyed from Bangladesh, Cambodia, China, Indonesia, Sri Lanka and Papua New Guinea, reported using intimate partner violence in their lifetime. In some of these regions up to 80% of men reported use of intimate partner violence emphasising the importance of context to these data. In places like the USA and the UK, estimates of intimate partner violence use are also lacking with most existing data reporting on rates of victimisation (Flood et al., 2022). Our data fill a crucial gap in understanding how widespread intimate partner violence is in Australia and the scale of response required.
The proportion of men who reported both using and experiencing intimate partner violence (18% by 2013 14; 25% by 2022), was more than double the proportion who reported using but not experiencing it (8% by 2013–14; 10% by 2022). This pattern has been found in other studies (Clemens et al., 2023; Schokkenbroek et al., 2022; Varlioglu & Hayes, 2022) and may reflect what is known as mutual or bidirectional couple violence – where both partners in a relationship engage in violent or abusive behaviours (Dokkedahl & Elklit, 2019).
From our data, we are currently unable to explore whether mutual violence took place, as we do not know in which relationship (past or current) the violence and/or abuse was experienced, nor the context in which it occurred. This is an important avenue for future research, particularly in understanding how mutual intimate partner violence unfolds and whether retaliation or self-defence is involved (Flood et al., 2022). Understanding these dynamics is crucial for the development and delivery of appropriate support and interventions for those affected by intimate partner violence (Stith & Spencer, 2024).
Emotional-type abuse was the most common form of intimate partner violence reported by men. In 2022, the proportion of men who reported ever making an intimate partner ‘feel frightened or anxious’ (32%) was around 3 times the proportion who reported ever ‘hitting, slapping, kicking or otherwise physically hurting’ an intimate partner when they were angry (9%). These findings are consistent with other research that had a broader definition of emotional-type abuse but still addressed comparable concepts (ABS, 2023; Palmer et al., 2024; Spencer et al., 2024). Further, our findings align with the evolving societal understandings of intimate partner violence, where there is greater awareness of forms of violence beyond physical violence, such as emotional abuse and coercive control, (for review see Beckwith et al., 2023), that can have at least as many long-term health impacts as physical violence (Oram et al., 2022).
The link between intimate partner violence and mental health
Our findings indicate that men’s mental health could be an important focus area in preventing their use of intimate partner violence. Consistent with past research (Oram et al., 2014; Spencer et al., 2024), we found that men with depressive symptoms were more likely to start using intimate partner violence than men with no depressive symptoms. Further, men with more severe depressive symptoms were at the greatest risk of intimate partner violence initiation. Specifically, after accounting for related mental health and health behaviours, men with moderate or severe depressive symptoms had a 62% increased risk of later using intimate partner violence compared to the 30% risk for men with mild depressive symptoms.
These findings have direct implications for future interventions in health care and service delivery. For instance, screening for depressive symptoms could open referral pathways to psychological support services for at-risk men, providing timely intervention that may help prevent the initiation of intimate partner violence. However, it is essential to acknowledge that only a minority of men experiencing depressive symptoms will later use intimate partner violence, highlighting the importance of individualised assessments.
Further, we were not able to determine if the link between depression and the use of intimate partner violence is bidirectional. That is, we could not test if men who start to use intimate partner violence are likely to later show depressive symptoms. While most previous studies support the temporal link demonstrated in our findings, where depressive symptoms are associated with an increased likelihood of later intimate partner violence use, some studies have demonstrated a potential bidirectional link (Graham et al., 2012; Saunders et al., 2021; Spencer et al., 2022). With the current Ten to Men data, we were not able to explore whether there is a bidirectional link. As new Ten to Men data becomes available, such investigations will be possible. We recommend that future research is conducted to explore the temporal nature of the relationship between depression and intimate partner violence among men. This research could also consider factors, suitable for public interventions such as alcohol use, drug use and masculine norms, that may alter the relationship between mental health and the use of intimate partner violence.
In addition to finding a link between depression and intimate partner violence initiation, we also found that men who ever reported suicidal thoughts, plans or attempts were 47% more likely to subsequently use intimate partner violence compared to those who reported no such suicidal behaviour (accounting for other mental health factors). There is very little research to draw on to help explain our findings, as most research in suicide and intimate partner violence focuses on the increased risk of suicide in those who experience intimate partner violence (White et al., 2024) or suicide within the context of intimate partner homicide (Kim & Merlo, 2023). In a qualitative study of male prisoners in the UK convicted of partner violence offences, the men reported that they used suicidal behaviours as a coping mechanism prior to or around the time they were violent and/or abusive to their intimate partner (Dewar et al., 2022). Further understanding of the relationship between suicidality and use of intimate partner violence will require ongoing research, including detailed longitudinal data, to investigate what underlies this complex association.
Social support and paternal affection as protective factors against using intimate partner violence
The body of research on risk factors for using intimate partner violence far exceeds that on the protective factors that make violence less likely (Flood et al., 2022). Our findings help address this research gap, showing that social support and a good quality relationship with a father or father figure during childhood are 2 factors that reduce the likelihood of using intimate partner violence.
In our sample, men who reported high levels of social support ‘all of the time’ were 27% less likely to report using intimate partner violence. This finding is consistent with most of the limited research on social support and use of intimate partner violence (Capaldi et al., 2012; Spencer et al., 2022). While the exact mechanism through which social support reduces the likelihood of using intimate partner violence is unknown, it has been suggested that social support may provide access to healthy coping mechanisms and reduce emotional distress that can lead to the use of violence (Capaldi et al., 2012).
Men who felt strongly that they had a quality relationship with a father or father figure during childhood, marked with affection, were 57% less likely to report ever having used intimate partner violence. Fathers are typically the earliest role models for boys in demonstrating healthy relationship behaviours and shaping their approach to receiving and giving affection. Indeed, early relational experiences can provide the blueprint for how young people function in their relationships later in life (Eriksson & Mazerolle, 2015; Ha et al., 2023; Li, 2022). Maternal affection is well established as a protective factor that reduces the risk of using intimate partner violence later in life (Dutton et al., 1996). This report presents some of the first evidence suggesting that a quality relationship with a father or father figure offers similar protection.
Although we could not directly test what underpins the relationship between paternal affection and the son’s use of intimate partner violence, there is evidence to suggest that fathers who show affection to their sons provide them with a secure form of attachment (Floyd et al., 2021). Individuals with secure attachment during childhood typically display better interpersonal functioning, emotional regulation and conflict resolution skills during adulthood (Brennan & Shaver, 1995; Chauhan et al., 2014; Thompson et al., 2022).
Further work is needed to better understand the association between paternal affection and the use of intimate partner violence as found in this study. One area for consideration is the role of paternal affection in the context of adverse childhood experiences, such as family violence, and whether the protective effects observed in this study hold in these circumstances. This proposed research would build on the current research to directly serve one of the prevention goals in the National Plan to End Violence Against Women and Children 2022–2032 – to address early factors that can stop violence before it starts.
Data considerations and limitations
When interpreting and applying these findings there are certain data limitations that should be considered. First, our research used men’s self-reported use of intimate partner violence, which can be limited by issues of misreporting due to recall bias, social desirability and misinterpretation. Within the context of intimate partner violence research, misreporting in self-report surveys can lead to both under-reporting and over-reporting of estimates. Some research shows that young men can be more likely to over-report their experience of intimate partner violence or not take the questions seriously (Ackerman, 2016), while other evidence suggests that some people may under-report their experiences due to feelings of shame, judgement or guilt, as well as fear of legal consequences (Chan, 2011). This is an ongoing issue within this research area, with current recommendations emphasising the need for careful survey design and interpretation assistance (Cullen, 2023).
A second consideration of our research is the measure of intimate partner violence used. There are many different conceptualisations and measures of intimate partner violence. We used 3 items of the full COHSAR measure (Donovan & Hester, 2014) to explore intimate partner violence, as the full set of questions were not included in the Ten to Men survey. As such, we captured 3 specific types of intimate partner violence behaviours, and these cannot be generalised more broadly to all intimate partner violence experiences and other contextual issues (e.g. power dynamics among intimate relationships, comparative impact of this abuse). Additional measures of intimate partner violence in future waves of the Ten to Men survey will improve the capacity of the study to investigate intimate partner violence. Additionally, as our measures ask about the experience of intimate partner violence in any intimate partner relationship, at any point in time, we could not examine how intimate partner violence changes across specific relationships over time.
The Ten to Men study is the only longitudinal study on Australian men with data on intimate partner violence use. There is continued need to consider men’s use of intimate partner violence among priority populations of men and consider how the drivers of intimate partner violence use may differ within these groups. In the Ten to Men data used in this study (Waves 1–4 available at time of writing), some of the priority population groups are unrepresented and could not be investigated, such as Aboriginal and/or Torres Strait Islander men, or were small in sample size making interpretation of findings harder, such as men with disability. Future research using the Ten to Men top-up sample (expected release late 2025), an addition specifically recruited to improve representation across priority populations and allow more detailed investigation of key topic areas, is recommended to further investigate the use of intimate partner violence among men.
Key conclusions for policy and practice
The National Plan to End Violence Against Women and Children 2022–2032 emphasises the need for investment in evidence-informed prevention and early intervention to stop these forms of violence from occurring. Our findings provide the following to support this objective:
- Aspects of men’s mental health are associated with their use of intimate partner violence. Aligned with the National Men’s Healthy Strategy 2020–2030 and the National Mental Health and Suicide Prevention Plan, supporting the mental health of men can have meaningful impacts not only for individuals but for their families and communities. Policy and practice changes focused on providing integrated supports for men with mental ill-health and their families could lead to fewer men using intimate partner violence.
- Social support and paternal affection during childhood are also associated with men’s use of intimate partner violence. Our findings show a clear protective link between social support and intimate partner violence. Spaces for men to experience needed social support could be a useful development.
- Our findings highlight the key role of the father–son relationship in reducing the likelihood of later use of intimate partner violence. Programs that support men to develop good quality relationships with their sons based on healthy expressions of affection could contribute to a reduction in men’s use of intimate partner violence.
1In the National Plan to End Violence Against Women and Children (2022), emotional abuse is defined as ‘a pattern of behaviour that aims to control or manipulate another person through repeated actions like insults, belittling, threats, intimidation, isolation, or gaslighting, with the intention to cause emotional harm or fear’. Aligned with this definition, we conceptualise this item as a type of emotional abuse and focus on the experience of the victim-survivor where fear and anxiety are induced.
2This was only asked about in the 2013–14 survey.
3The measures of intimate partner violence used in this study provide an indication about the use of specific behaviours that each relate to a type of emotional abuse, physical violence and sexual abuse. The measures do not capture all violent and/or abusive behaviours that individuals who use intimate partner violence may display. See methods section for further detail.
References
Ackerman, J. M. (2016). Over-reporting intimate partner violence in Australian survey research. British Journal of Criminology, 56(4), 646–667. doi.org/10.1093/bjc/azv066
Akcabozan Kayabol, N. B. (2023). Intimate partner violence: Family background of perpetrators. In Encyclopedia of domestic violence (pp. 1–7). Springer International Publishing.
Australian Bureau of Statistics (ABS). (2023). Causes of death, Australia. ABS. www.abs.gov.au/statistics/health/causes-death/causes-death-australia/2023.
Australian Institute of Health and Welfare (AIHW). (2011). Principles on the use of direct age-standardisation in administrative data collections: For measuring the gap between Indigenous and non-Indigenous Australians. Cat. no. CSI 12. AIHW.
Bandara, D., Howell, L., Silbert, M., & Daraganova, G. (2021). Ten to Men: The Australian Longitudinal Study on Male Health, Release 3 (Waves 1–3). doi.org/10.26193/JDE1TD, ADA Dataverse, V4
Beckwith, S., Lowe, L., Wall, L., Stevens, E., Carson, R., Kaspiew, R., et al. (2023). Coercive control literature review. Australian Institute of Family Studies. aifs.gov.au/research/research-reports/coercive-control-li terature-review
Bowen, E., & Swift, C. (2019). The prevalence and correlates of partner violence used and experienced by adults with intellectual disabilities: A systematic review and call to action. Trauma, Violence, & Abuse, 20(5), 693–705. doi.org/10.1177/1524838017728707
Brennan, K. A., & Shaver, P. R. (1995). Dimensions of adult attachment, affect regulation, and romantic relationship functioning. Personality and Social Psychology Bulletin, 21(3), 267–283. doi.org/10.1177/0146167295213008
Brim, O. G., Baltes, P., Bumpass, L. Cleary, P., Featherman, D., Hazzard, W., Kessler, R. et al. National Survey of Midlife Development in the United States (MIDUS), 1995–1996. Inter-university Consortium for Political and Social Research.
Campbell, E., Fernando, T., Gassner, L., Hill, J., Seidler, Z., & Summers, A. (2024). Unlocking the prevention potential: Accelerating action to end domestic, family, and sexual violence. Australian Government, Department of the Prime Minister and Cabinet. www.pmc.gov.au/resources/unlocking-the-prevention-potential
Capaldi, D. M., Knoble, N. B., Shortt, J. W., & Kim, H. K. (2012). A systematic review of risk factors for intimate partner violence. Partner Abuse, 3(2), 231–280. doi.org/10.1891/1946-6560.3.2.231
Chan, K. L. (2011). Gender differences in self-reports of intimate partner violence: A review. Aggression and Violent Behavior, 16(2), 167–175. doi.org/10.1016/j.avb.2011.02.008
Chauhan, R., Awasthi, P., & Verma, S. (2014). Attachment and psychosocial functioning: An overview. Social Science International, 30(2), 331–344. www.proquest.com/openview/8b6e128d5d72430a4998e213ec3197f8/1?pq-origsite=gscholar&cbl=506333
Chiesa, A. E., Kallechey, L., Harlaar, N., Rashaan Ford, C., Garrido, E. F., Betts, W. R., & Maguire, S. (2018). Intimate partner violence victimization and parenting: A systematic review. Child Abuse & Neglect, 80, 285–300.
doi.org/10.1016/j.chiabu.2018.03.028
Clare, C. A., Velasquez, G., Mujica Martorell, G. M., Fernandez, D., Dinh, J., & Montague, A. (2021). Risk factors for male perpetration of intimate partner violence: A review. Aggression and Violent Behavior, 56, Article 101532. doi.org/10.1016/j.avb.2020.101532
Clemens, V., Fegert, J. M., Kavemann, B., Meysen, T., Ziegenhain, U., Brähler, E. et al. (2023). Epidemiology of intimate partner violence perpetration and victimisation in a representative sample. Epidemiology and Psychiatric Sciences, 32, e25. doi.org/10.1017/S2045796023000069
Conner, K. R., Cerulli, C., & Caine, E. D. (2002). Threatened and attempted suicide by partner-violent male respondents petitioned to family violence court. Violence and Victims, 17(2), 115–125. doi.org/10.1891/vivi.17.2.115.33645
Cullen, C. (2023). Method matters: The underreporting of intimate partner violence. The World Bank Economic Review, 37(1), 49–73. doi.org/10.1093/wber/lhac022
Dalve, K., Ellyson, A. M., Bowen, D., Kafka, J., Rhew, I. C., Rivara, F. et al. (2024). Suicide-related behavior and firearm access among perpetrators of domestic violence subject to domestic violence protection orders. Preventive Medicine Reports, 37, 102560. doi.org/10.1016/j.pmedr.2023.102560
Department of Health and Aged Care (DOHAC). (2019). National Men’s Health Strategy 2020-2030. Australian Government, DOHAC. www.health.gov.au/sites/default/files/documents/2021/05/national-men-s-health-strategy-2020-2030_0.pdf
Department of Social Services (DSS). (2022). National Plan to End Violence Against Women and Children, 2022–2032. Australian Government, DSS. www.dss.gov.au/national-plan-end-gender-based-violence/resource/national-plan-end-violence-against-women-and-children-2022-2032
Department of Social Services. (2023). Theory of change 2022–2032: Under the National Plan to End Violence Against Women and Children. Australian Government, DSS. www.dss.gov.au/system/files/resources/np-theory-change.pdf
Dewar, C., Heggs, D. A., & Davies, J. (2022). Exploring the relationship between domestic violence perpetration and suicidal behavior in male prisoners. Archives of Suicide Research, 26(4), 1831–1846. doi.org/10.1080/13811118.2021.1939207
Dokkedahl, S., & Elklit, A. (2019). Understanding the mutual partner dynamic of intimate partner violence: A review. Partner Abuse, 10(3). psycnet.apa.org/doi/10.1891/1946-6560.10.3.298
Donovan, C., & Hester, M. (2014). How we did the research: the COHSAR research approach. In Domestic Violence and Sexuality (pp. 35–56). Policy Press.
Donovan, C., Holmes, J., McCarry, M., & Fahmy, E. (2005). Comparing heterosexual and same sex abuse in relationships (COHSAR Survey Instrument). Centre for Gender & Violence Research, University of Bristol & Centre for Applied Social Science, University of Sunderland.
Dutton, D. G., Starzomski, A., & Ryan, L. (1996). Antecedents of abusive personality and abusive behavior in wife assaulters. Journal of Family Violence, 11(2), 113–132. doi.org/10.1007/BF02336665
Eriksson, L., & Mazerolle, P. (2015). A cycle of violence? Examining family-of-origin violence, attitudes, and intimate partner violence perpetration. Journal of Interpersonal Violence, 30(6), 945–964. doi.org/10.1177/0886260514539759
Flood, M., Brown, C., Dembele, L., & Mills, K. (2022) Who uses domestic, family, and sexual violence, how, and why? The State of Knowledge Report on Violence Perpetration. Queensland University of Technology.
Floyd, K., Hesse, C., & Generous, M. A. (2021). Affection exchange theory: A bio-evolutionary look at affectionate communication. In Engaging theories in interpersonal communication (pp. 27–38). Routledge.
Fulu, E., Jewkes, R., Roselli, T., & Garcia-Moreno, C. (2013). Prevalence of and factors associated with male perpetration of intimate partner violence: findings from the UN Multi-country Cross-sectional Study on Men and Violence in Asia and the Pacific. The Lancet Global Health, 1(4), e187-e207. doi.org/10.1016/S2214-109X(13)70074-3
Graham, K., Bernards, S., Flynn, A., Tremblay, P. F., & Wells, S. (2012). Does the relationship between depression and intimate partner aggression vary by gender, victim-perpetrator role, and aggression severity? Violence & Victims, 27(5). doi.org/10.1891/0886-6708.27.5.730
Ha, T., Van Ryzin, M. J., & Elam, K. K. (2023). Socialization processes within adolescents’ relationships with parents and peers predicting couples’ intimate partner violence in adulthood: A social learning perspective. Development and Psychopathology, 35(1), 204–217. doi.org/10.1017/S0954579421000602
Hardesty, J. L., & Ogolsky, B. G. (2020). A socioecological perspective on intimate partner violence research: A decade in review. Journal of Marriage and Family, 82(1), 454–477. doi.org/10.1111/jomf.12652
Heyman, R. E., Mitnick, D. M., & Slep, A. M. S. (2022). Intimate partner violence: Terms, forms, and typologies. In R. Geffner, J. W. White, L. K. Hamberger, A. Rosenbaum, V. Vaughan-Eden, & V. I. Vieth (Eds.), Handbook of interpersonal violence and abuse across the lifespan: A project of the National Partnership to End Interpersonal Violence Across the Lifespan (NPEIV) (pp. 2219–2247). Springer Nature Switzerland AG. doi.org/10.1007/978-3-319-89999-2_131
Hulme, S., Morgan, A., & Boxall, H. (2019). Domestic violence offenders, prior offending and reoffending in Australia. Trends and Issues in Crime and Criminal Justice, 580, 1–22. search.informit.org/doi/abs/10.3316/informit.699971903102128
International Wellbeing Group. (2013). Personal Wellbeing Index. Australian Centre on Quality of Life, Deakin University.
Kansky, J., & Diener, E. (2022). NoTable advances in the science of well-being. Positive Psychology: An International Perspective, 43–68. doi.org/10.1002/9781119771418.ch4
Kaufman-Parks, A. M., DeMaris, A., Giordano, P. C., Manning, W. D., & Longmore, M. A. (2018). Intimate partner violence perpetration from adolescence to young adulthood: Trajectories and the role of familial factors. Journal of Family Violence, 33(1), 27–41. doi.org/10.1007/s10896-017-9924-5
Kim, B., & Merlo, A. V. (2023). Domestic homicide: A synthesis of systematic review evidence. Trauma, Violence, & Abuse, 24(2), 776–793. doi.org/10.1177/15248380211043812
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. doi.org/10.1046/j.1525-1497.2001.016009606.x
Li, C. K. W. (2022). The applicability of social structure and social learning theory to explain intimate partner violence perpetration across national contexts. Journal of Interpersonal Violence, 37(23–24).
doi.org/10.1177/08862605211072166
Meyer, S. R., Hardt, S., Brambilla, R., Page, S., & Stöckl, H. (2024). Explaining intimate partner violence through economic theories: A systematic review and narrative synthesis. Aggression and Violent Behavior, 77, 101929.
doi.org/10.1016/j.avb.2024.101929
Oram, S., Fisher, H. L., Minnis, H., Seedat, S., Walby, S., Hegarty, K. et al. (2022). The Lancet Psychiatry Commission on intimate partner violence and mental health: Advancing mental health services, research, and policy. The Lancet Psychiatry, 9(6), 487–524. doi.org/10.1016/S2215-0366(22)00008-6
Oram, S., Trevillion, K., Khalifeh, H., Feder, G., & Howard, L. M. (2014). Systematic review and meta-analysis of psychiatric disorder and the perpetration of partner violence. Epidemiology and Psychiatric Sciences, 23(4), 361–376. doi.org/10.1017/S2045796013000450
Palmer, M. L., Keilholtz, B. M., Vail, S. L., & Spencer, C. M. (2024). The relationship between emotional intimate partner violence and other forms of violence: A meta-analytic review. Family Process, 63(4), 2291–2307.
doi.org/10.1111/famp.12992
Papalia, N., Simmons, M., Trood, M., McEwan, T., & Spivak, B. (2024). Police-reported family violence victimisation or perpetration and mental health-related emergency department presentations: An Australian data-linkage study. BMC Public Health, 24(1), 131. doi.org/10.1186/s12889-023-17570-y
Payne, J., & Morgan, A. (2024). Prevalence of recorded family and domestic violence offending: A birth cohort study. Trends and Issues in Crime and Criminal Justice, 701, 1–18. doi.org/10.52922/ti77598
Saunders, K. R., Landau, S., Howard, L. M., Fisher, H. L., Arseneault, L., McLeod, G. F. et al. (2021). Past-year intimate partner violence perpetration among people with and without depression: An individual participant data (IPD) meta-mediation analysis. Social Psychiatry and Psychiatric Epidemiology, 1–13. doi.org/10.1007/s00127-021-02183-w
Schokkenbroek, J. M., Ouytsel, J. V., Hardyns, W., & Ponnet, K. (2022). Adults’ online and offline psychological intimate partner violence experiences. Journal of interpersonal Violence, 37(15–16), NP14656-NP14671.
doi.org/10.1177/08862605211015217
Sherbourne, C. D., & Stewart, A. L. (1991). The MOS social support survey. Social Science & Medicine, 32(6), 705–714.
doi.org/10.1016/0277-9536(91)90150-B
Spencer, C., Mallory, A. B., Cafferky, B. M., Kimmes, J. G., Beck, A. R., & Stith, S. M. (2019). Mental health factors and intimate partner violence perpetration and victimization: A meta-analysis. Psychology of Violence, 9(1), 1–17. doi.org/10.1037/vio0000156
Spencer, C. M., Stith, S. M., & Cafferky, B. (2022). What puts individuals at risk for physical intimate partner violence perpetration? A meta-analysis examining risk markers for men and women. Trauma, Violence, & Abuse, 23(1), 36–51. doi.org/10.1177/1524838020925776
Spencer, C. M., Keilholtz, B. M., Palmer, M., & Vail, S. L. (2024). Mental and physical health correlates for emotional intimate partner violence perpetration and victimization: A meta-analysis. Trauma, Violence, & Abuse, 25(1), 41–53. doi.org/10.1177/15248380221137686
Stith, S. M., & Spencer, C. (2024). Commentary: 25 years after Johnson’s typology of intimate partner violence the impact of Johnson’s typology on clinical work. Journal of Family Violence, 39(1), 143-148.
doi.org/10.1007/s10896-023-00654-z
Swami, N., Prattley, J., Bandara, D., Howell, L., Silbert, M., Renda., J. et al. (2022). Ten to Men: The Australian Longitudinal Study on Male Health: Waves 1–3. The Australian Economic Review, 55(1), 155–165.
Terhaag, S., Quinn, B., Swami, N., & Daraganova, G. (2020). Mental health of Australian males. In G. Daraganova & B. Quinn (Eds.), Insights #1: Findings from Ten to Men – The Australian Longitudinal Study on Male Health 2013–16. Australian Institute of Family Studies.
Thompson, R. A., Simpson, J. A., & Berlin, L. J. (2022). Taking perspective on attachment theory and research: Nine fundamental questions. Attachment & Human Development, 24(5), 543–560. doi.org/10.1080/14616734.2022.2030132
Varlioglu, R., & Hayes, B. E. (2022). Gender differences in the victim-offender overlap for dating violence: The role of early violent socialization. Child Abuse & Neglect, 123, Article 105428. doi.org/10.1016/j.chiabu.2021.105428
White, S. J., Sin, J., Sweeney, A., Salisbury, T., Wahlich, C., Montesinos Guevara et al. (2024). Global prevalence and mental health outcomes of intimate partner violence among women: A systematic review and meta-analysis. Trauma, Violence & Abuse, 25(1), 494–511. doi.org/10.1177/15248380231155529
Wolford-Clevenger, C., Brem, M. J., Zapor, H., Elmquist, J., & Stuart, G. L. (2017). Prevalence, severity, and correlates of suicidal ideation among men and women in batterer intervention programs. Partner Abuse, 8(2), 190. doi.org/10.1891/1946-6560.8.2.190
Yu, R., Nevado-Holgado, A. J., Molero, Y., D’Onofrio, B. M., Larsson, H., Howard, L. M. et al. (2019). Mental disorders and intimate partner violence perpetrated by men towards women: A Swedish population-based longitudinal study. PLoS Medicine, 16(12), e1002995. doi.org/10.1371/journal.pmed.1002995
About the authors
Karlee O’Donnell, Mulu Woldegiorgis, Constantine Gasser, Katrina Scurrah, Catherine Andersson, Heather McKay, and Sean Martin are from the Australian Institute of Family Studies.
Kelsey Hegarty is from the University of Melbourne.
Zac Seidler works with Movember, Orygen and the University of Melbourne.
Media releases
Acknowledgements
The authors of this chapter are grateful to the many individuals and organisations who contributed to its development and who continue to support and assist in all aspects of the Ten to Men study. The Department of Health and Aged Care commissioned and continues to fund Ten to Men. The study’s Scientific Advisory and Community Reference Groups provide indispensable guidance and expert input. The University of Melbourne coordinated Waves 1 and 2 of Ten to Men and Roy Morgan collected the data at both these time points. The Social Research Centre collected Wave 3 and Wave 4 data. A multitude of AIFS staff members collectively work towards the goal of producing high-quality publications of Ten to Men findings. This publication greatly benefited from the guidance of the AIFS Executive Team (Liz Neville, Catherine Andersson) and Communications Team (Katharine Day, Rachel Evans). Thanks are particularly extended to the survey methodology (Karen Biddiscombe, Aeysha Corrigan, Sarah Carr, Anais Keenan) and data management and linkage (Melissa Suares, Frank Volpe, Michelle Silbert) groups for their efforts in collecting and managing Ten to Men data.
We would especially like to thank every Ten to Men participant and their families who give so generously with their time and energy in completing our study surveys.
Featured image: © GettyImages/golubovy
Suggested citation: O’Donnell, K., Woldegiorgis, M., Gasser, C., Scurrah, K., Andersson, C., McKay, H., Hegarty, K., Seidler, Z., & Martin, S. (2025). The use of intimate partner violence among Australian men. Insights #3, Chapter 1. Melbourne: Australian Institute of Family Studies.
3 June 2025